
Abstract
Keys messages
Children with DLD enter kindergarten less prepared than typically developing children and are at greater risk of academic, social, and behavioral problems. Early intervention services are essential to supporting school readiness of children with DLD. A response to intervention approach could optimize school readiness for these children while building on existing strengths. Priorities to optimize school entry for children with DLD are maximizing community initiatives, training, and communicating with partners, supporting change in practice, offering flexible services adapted to children's needs, and implementing mechanisms to ensure service continuity and information transfer between agencies to ensure service continuity and information transfer.
Introduction
School readiness is a broad concept that includes individual characteristics, school-related factors, and environmental influences (Justice et al., 2009; Reid and Strobino, 2019). Upon entering school, children must have attained a minimum level of development, including physical, social, behavioral, cognitive, and language abilities, in order to be able to adapt to school requirements (Justice et al., 2009). It also includes the quality of the transition from daycare or home to school, the opportunities for both children and parents to prepare for this transition, and school resources to support children with disabilities (Reid and Strobino, 2019; Williams and Lerner, 2019).
Finally, school readiness is characterized by family and community support in order to provide a healthy environment involving health care services and access to good daycare services (Reid and Strobino, 2019; Williams and Lerner, 2019).
Nearly 10% of kindergarten children have language difficulties and 7% present a developmental language disorder (DLD) (Norbury et al., 2016; Simard et al., 2018; Tomblin et al., 1997). This neurodevelopmental disorder, present at birth, is characterized by significant and persistent difficulties in various receptive and expressive spheres of language that are sufficiently severe to lead to functional impacts (Bishop et al., 2016). As communication is central to the child's participation, children with (DLD) are expected to experience limitations and challenges on a daily basis (Bishop et al., 2017; Forrest et al., 2021; Justice et al., 2009; McKean et al., 2017). As a result, children with DLD begin school less prepared than typically developing children which demonstrates the importance of language skills in school readiness. Indeed, children with DLD are at greater risk than typically developing children of experiencing academic, social, and behavioral challenges, as assessed in kindergarten (Justice et al., 2009; Pentimonti et al., 2016). These children are also likely to have important participation and socialization limitations, motor skills disorders, low level of autonomy, and employment challenges later in life (McCormack et al., 2009).
To support language development, early family-centered services are recommended (Ebbels et al., 2019; Guralnick, 2011; Institut national d’excellence en santé et en services sociaux (INESSS), 2017; Law et al., 2017; National Research Council and Institute of Medicine, 2000). This approach is associated with greater parent satisfaction in services received and favorable child development (Dempsey and Dunst, 2004; Law et al., 2003; O'Neil et al., 2001; Reich et al., 2004). It is based on three principles i.e., the respect for the child and family, the appreciation of the family's impact on the child's well-being, and the collaboration between the professional and family and it encourage parent involvement (Almasri et al., 2018; King and Chiarello, 2014). To improve access to effective early family-centered care and to better meet the needs of children with DLD, a Response to Intervention (RTI) model adapted to speech-language pathology has also been proposed (Ebbels et al., 2019; Law et al., 2013). This type of model promotes early identification of at-risk children and aims to coordinate available resources in order to reduce the risk of long-term difficulties. RTI design often includes three tiers of intervention: universal (Tier 1), targeted (Tier 2), and specific (Tier 3) (Graner et al., 2005; Jimerson et al., 2007; Justice, 2006; Snow et al., 2015). The child's progress is measured regularly to adjust services and move from one tier of intervention to another. Universal intervention refers to quality teaching for all children, e.g., scientifically validated effective teaching methods, adjusted feedback and reinforcement. Targeted intervention is offered to small groups and focuses on specific objectives and explicit teaching. It provides more models to the child, increases instructional time, and allows the child more time to acquire a skill. Specialized intervention is individualized and targets a child's needs and learning style. It can be offered by a speech language pathologist (direct intervention) or by a supervised assistant (indirect intervention) (Graner et al., 2005; Jimerson et al., 2007). Based on this approach, optimal support for language development should include the following: in Tier 1, all children would attend daycare settings where quality education and language stimulation are offered; in Tier 2, children below age expectations or at risk of persistent difficulties would participate in a language program group intervention led by a trained assistant or education professional; finally, in tier 3, children with a confirmed DLD would receive individualized intervention (Ebbels et al., 2019). RTI encourages indirect intervention by an assistant, or a parent supervised by a speech-language pathologist as well as group intervention, known to play a role in the optimization of health care services and in preparing children with DLD for school (American Speech-Language-Hearing Association, 2008; Boyle et al., 2007, 2009; Guralnick, 2011, 2017; Klatte et al., 2020; Law et al., 2003; Ross-Lévesque et al., 2021).
It is clear that language skills play a key role in school readiness because communication is crucial in the child's participation (Bishop et al., 2017; Forrest et al., 2021; Justice et al., 2009; McKean et al., 2017). So, children with DLD need optimal support to prepare them for school (Ebbels et al., 2019; Justice et al., 2009). The aim of this phenomenological study (Creswell, 2014) is to explore the opinions of professionals and managers providing services to preschool children with DLD about how to better support school readiness. More specifically, it targets the reported facilitators and barriers to school readiness in children with LD, as well as reported strategies to better prepare them for school entry. This examination of facilitators, barriers, and strategies is anchored in an RTI model to better understand how it may offer a framework for preschool services to children with language difficulties.
Methods
Design and methodology
The study was approved by the research ethics committees of the two collaborating institutions (CIUSSS-CN; #2018-596). A qualitative research design using focus groups was deemed most appropriate given the objective of collecting the opinions of specific groups of people, while engaging in a collective reflective process. This method also encourages interaction between the various individuals involved in the service provision and allows them to take part in the research itself (Creswell, 2014; Kivits et al., 2016; Liamputtong, 2011; Pope and Mays, 2020). The methods and results are based on the Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups (Tong et al., 2007).
Context of the study
The study was conducted by a doctoral student in speech-language pathology (first author) and supervised by researchers specialized qualitative research (second author) or in developmental language disorder (third author). The first author has knowledge of RTI model and services for children with DLD and realized this study in the context of her thesis. She knew some of the participants from past collaboration in clinical work with them. The second and third authors had no relationship with the participants.
The study was conducted in the province of Québec, Canada, where services for children with DLD are offered through three ministries, i.e., Education, Health and Social Services, and Family. Services can thus be offered in their community, in health center or in schools. According to the most recent government data (INESSS, 2017), the penetration rate (number of children receiving services on the estimated number of children between 2 and 9) in services for children aged between 0 to 10 years old is 2,5%, which is lower than the estimated 7% prevalence rate in the general population. In addition, there is a waiting time of more than 5 months between the assignment of a case to a provider and the first service offered. The average length of a service episode would be 20 months. Children would receive an average of 10 h of service delivery (INESSS, 2017). In the recent years, Quebec government has implemented a program to enhance the provision of services in the 0–5 age group by identifying children with developmental delays as early as possible and providing services that are appropriate to the child's needs (Ministère de la santé et des services sociaux, 2021). Services are not explicitly based on an RTI model, although the recent program implemented in province of Quebec is inspired by RTI. This context lends itself well to a discussion about the organization of services offered in an RTI approach, based on the evidence in the field.
Recruitment
Participants were recruited by the first author. The inclusion criteria were: 1) working directly or indirectly with children with LD, 2) being an expert in the services available for children with DLD, as confirmed by the number of years of service, and 3) being located in one of the two targeted administrative regions: a rural region or an urban region, to maximize the representativeness of the sample. Participants were recruited by email using convenience sampling and networking strategies. Managers and professionals from the region's healthcare main organization and from the school services center were directly invited to participate in the project or selected on the basis of referrals from already recruited participants. Six participants declined to take part to the study by lack of time or dropped out because of a schedule conflict.
Participants
Fifteen participants took part in one of two focus groups. All participants worked in the public sector financed by one of the Quebec three ministries involved—education sector, health sector, or family support sector and had at least ten years of experience in their field at that time. All participants had knowledge of the RTI model, but not all worked in an organization where it was implemented.
Data collection
Prior to the focus group meetings, participants received the questions to be addressed (see Appendix A) and were invited to begin individual reflection. Two groups were created, one for each administrative region. The first group was composed of six participants from a rural region: one speech-language pathologist and one manager from a rehabilitation center, a speech-language pathologist in a public school, two specialized educators working with children aged between 0 and 5, and a community counselor working in the development of community program to help children's transition to school. The second group included nine participants from an urban region: two speech-language pathologists from local Community Service Centers, one speech-language pathologist from a rehabilitation center, three speech-language pathologists in public schools, one specialized educator from a rehabilitation center, one project manager, and one clinical coordinator in a rehabilitation center.
The approximately two hour-long focus groups were conducted remotely via Microsoft Teams videoconferencing platform, in French. All participants were viewable to each other and to the researchers via web cameras. Participants used inboard or external microphones and headsets at their convenience to ensure audio quality. Participants were asked about the audio quality at the beginning of the meeting and invited to mention any technical problems if necessary. Audio quality during the focus group was satisfactory for the participants. Both focus-group were moderated by the first author who also asked the questions to the participants. A research assistant who is also a master's student in speech-language pathology participated in the meetings to control the audio recordings and to take notes on emerging themes. The audio recordings were taken directly on the computer of the research assistant. The moderator used a semi-structured interview protocol developed by the authors to ensure that the objectives of the study were met while also allowing for spontaneous questions to be raised in order to clarify or expand on certain points (Creswell, 2014) (see Appendix A). The participants discussed their opinions about the services currently offered and possible changes thereto. The discussion with participants was explicitly structured around the RTI model, i.e., possible solutions were discussed for each of the three tiers: universal, targeted, and specialized (Ebbels et al., 2019; Graner et al., 2005; National Center on Response to Intervention, 2010; Troia, 2005).
Data analysis
The interviews were analyzed using a three-step analytical questioning strategy (Clarke et al., 2015; Leavy, 2017; Paillé and Mucchielli, 2016). This strategy allows the research questions to be answered directly through deductive and inductive processes. It is also time- and resource-efficient insofar as it does not require a verbatim transcription. In step 1 of the analysis, the first author listened to the audio recordings and listed all relevant verbatim of the participants’ statements about facilitators and barriers to school readiness, as well as strategies to better support it, without distinction between group, in an Excel file. In step 2, the analysis model was created in a deductive manner based on the three tiers of the RTI model; participants’ statements from step 1 were therefore classified according to relevance under tiers 1, 2, or 3. The remaining statements were categorized inductively based on the additional topics identified. In step 3, the final step of the analysis, the first author identified the main themes emerging from the participants’ statements. To ensure validity of the results, two steps were taken, i.e., peer-debriefing and seeking participant feedback. First, results were discussed by the three authors to reduce researcher bias. Second, results were sent to all participants to obtain their judgment of accuracy and credibility (Creswell, 2014). In this article, we have selected quotes, freely translated from French by the first author, to illustrate the opinions of participants.
Results
The first step of the analysis yielded 17 reported facilitators and 16 reported barriers to school readiness as well as six strategies to support readiness in children with DLD. In the second step, these facilitators, barriers, and strategies were categorized by tiers of the RTI model and are presented in Table 1. In the third step of analysis, five main themes were identified: (1) maximizing community initiatives, (2) training and support for partners, (3) supporting change in practice, (4) offering flexible services adapted to children's needs, and (5) implementing mechanisms to ensure service continuity and information transfer between agencies. These five themes summarize the content of all the participants’ statements and are therefore used to present the results of this analysis.
Reported facilitators, barriers, and strategies to support school readiness in children with LD.
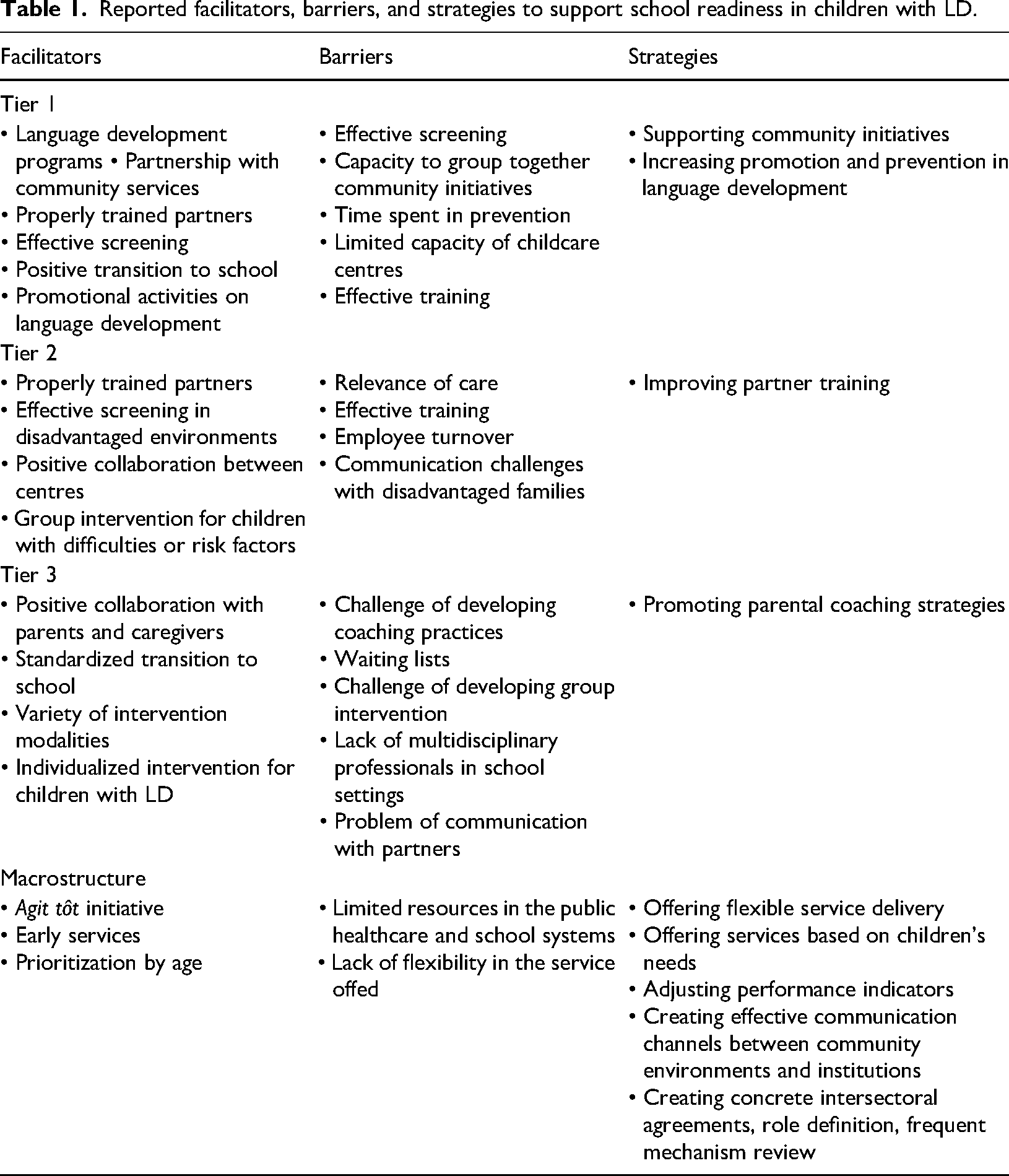
Reported facilitators, barriers, and strategies to support school readiness in children with LD.
Participants highlighted the impact of community initiatives on language development and described these as a facilitator to establishing effective universal services for children. Examples of such community initiatives are partnership between local services center, community organization, and educators in daycare to promote strategies to help language development or workshop offer to parents by community organization. Participants nonetheless emphasized the barriers associated with listing and grouping these initiatives together because there are many of them and they change quickly. They also mentioned the importance of their contribution to enhancing these initiatives and of obtaining recognition for the time invested. “The links with the community, there are so many initiatives taking place everywhere; how do we bring them together in an integrated way […] How do we connect all these initiatives, how do we enhance the potential of the community?”
To encourage community initiatives, participants suggested creating accessible communication channels between community environments and institutions. In addition, participants indicated that the performance indicators currently used in practice settings are quantitative, i.e., number of minutes of therapy per client. Interventions in the community, as such are not taken into consideration and, as a result, not valued by managers. Performance indicators should therefore be set up to include the time invested in the community. “For universal services, really taking advantage of every opportunity in our region and encouraging the small initiatives that are being launched is to create links with these small initiatives. I think that would be a win-win situation. The more channels we create, the more able we are to reach out to our vulnerable clientele […]; encouraging as much as possible all community opportunities.”
Theme 2: Training and supporting partners
Participants believed that collaboration between speech-language pathologists and stakeholders is an important factor in promoting school readiness of children with DLD. This includes collaborating with parents, as well as other significant adults in the child's life such as early childhood educators and teachers. However, they brought up a number of challenges to establishing collaboration and effective partner training, especially due to stakeholder availability and lack of resources. They also pointed out that education employee turnover creates additional workload for speech-language pathologists, especially in socially and economically disadvantaged environments. Participants also mentioned some community resistance from early childhood educator to collaborate with speech-language pathologist, particularly in daycares and in families with children with special needs. “It's good to provide training, which we do a lot, but we’ve realized over the years that training alone is not enough to improve teachers’ skills, that we need to develop know-how, which requires support, it requires self-assessment on the part of the teachers […] You really have to support and create ties with them, get them to think, give them very concrete solutions […]. This still requires continuous work with each intervener and adapting to the objectives of each one of them; it's still a lot when you are a speech therapist, and you have seven schools and interveners to support and train […].”
“There's a lot of staff turnover too. We often have to start over, particularly in disadvantaged environments, there is even more staff turnover, and this is where interveners need to be better trained, better equipped […].”
“Speaking of childcare settings, we have this service offer, but maybe our interventions are not as intense as we would like because there is still resistance […] It's kind of up to each person.”
To help speech-language pathologists improve their training skills with stakeholders, participants wish to be better equipped to develop these skills, for example, with programs and pre-designed materials. They specified a need to optimize resources for partner training. They also encouraged knowledge transfer between professionals and asked for concerted action to promote training for partners. Finally, they suggested fostering relationships with daycare centers and, to this end, rapidly reaching out them.
Theme 3: Supporting change in practice
Participants listed various services that support school readiness, covering universal, targeted, and specialized tiers within the RTI model, as well as early services and prioritizing children entering kindergarten as contributing factors. Multidisciplinary follow-up (involving speech-language pathologist, social worker, occupational therapist, or specialized educator services) provided to families of children with DLD also helps to prepare them for school. There are obstacles, however, to implementing change in practice. Participants find it difficult, for example, to apply certain practices that are recognized as effective, such as parental coaching and group intervention. They point out that actualization of these practices varies from one region to another and from one center to another. A lack of financial and human resources also hamper the implementation of these practices. “It is not easy to deploy a group service offering, it's all the complexity related to group offering in a vast area.”
“This whole aspect of change in practice, we talk a lot about parental coaching, the importance of involving significant persons in the child's life, how to succeed in actualizing this change in practice, which is still complex. I think that everyone agrees on this but updating practices in order to create a better partnership with people who are close to the child is not as easy as it seems.”
To support practice change, participants raised the importance of involving managers in the development of new practices and clinical decisions. Providing training to professionals, implementing participatory action research in order to develop projects that are in line with these changes, and collaborating with the communities where these changes are already in place are needed. Additional resources are also necessary in order to implement these changes.
Theme 4: Offering flexible services adapted to children's needs
To promote better school readiness, early identification of children at risk of experiencing difficulties is crucial. To identify those children and provide them the services they need, it is essential to have effective screening. Participants mentioned the contribution of a new program in the Province of Quebec which facilitates holistic screening of children and makes it possible to rapidly identify their developmental needs. However, screening continues to be an issue. On the one hand, professionals have observed an over-screening of children with very few risk factors in recent years, leading to system overload. On the other hand, some families, in particular vulnerable families with more risk factors to a low school readiness, are hard to reach. Participants also stressed the importance of offering services based on children's needs instead of diagnosis to promote school readiness. Currently, the lack of flexibility in service delivery based on diagnosis, long waiting lists, and shortage of human and financial resources impede the effectiveness of services for children with DLD. “Many of the children in our continuum of services continue to be monitored because they are a little fragile, and I have the feeling that all these children overload our continuum of services. How can we create a safety net for these children [….]? How can we better serve them so that we can direct intense intervention toward children with real needs. It's the issue of relevance of care, use of care, misuse or overuse of the care we provide.”
“Waiting lists and lack of resources is the bottom line. Access to services is a real problem, but there is also a lack of resources, both financial and human. Sometimes there's a little bit of money but we don't have anyone and sometimes we have people and there's no money.”
To make services more flexible, participants discussed the possibility of making changes to the performance indicators currently used in the public system that are judged on the amount of direct or indirect follow-up with a specific client. In line with the RTI model, performance indicators used in clinical settings should take into account all types of services, provided to specific children and his parents and educators, but also services in the community to promote prevention and use of stimulation strategies in home and daycare indirectly to parents, caregivers, or educators. The quality and diversification of services should be considered along with the volume of users served. In addition, participants noted the importance of making service delivery for children with mild difficulties more flexible in order to tailor services according to the child's needs and the relevance of care. “To integrate such a model [RTI model], we have to think in terms of continuum of service with all the people involved, all stakeholders, regardless of resources, and in terms of focusing on clinical appropriateness and timing of service for the child.”
Theme 5: Implementing mechanisms to ensure service continuity and information transfer between agencies
The transition to school entry was also an important topic discussed. The mechanisms in place to support the transition to school entry appear to be crucial in ensuring child readiness. Examples of such mechanisms are the school integration programs before kindergarten, multidisciplinary follow-up offered to families of children with LD, and initiatives such as transition protocol put in place by some school boards, which facilitates information transfer between the preschool and school environments. Poor communication and information exchange between the two environments can indeed hinder the transition to school process. “Information transfer is not always easy, social services, readaptation center, school environment. Whether it is reports, observations, we need to talk to each other, we have to take the time to keep each other in the loop. Sometimes the evaluation report arrives at the school, but it doesn’t get to the speech therapist who covers 7 schools […] we still have communication problems between services.”
To support the sustainability of initiatives and promote information transfer between involved parties, participants called for the creation of concrete intersectoral agreements to better define the role of each party and committees to regularly review the mechanisms in place. In their opinion, the information transfer process must be made more systematic. Transition protocol put in place by some school boards seems to be a good way of the systematization of information transfer.
Discussion
The purpose of this phenomenological study was to explore the opinions of school and health care professionals and managers regarding the services offered to children with DLD in order to better support school readiness within an RTI model. Five themes emerged from discussions about facilitators and barriers to school readiness and strategies to support it: (1) maximizing community initiatives, (2) training and supporting partners, (3) supporting a change in practice, (4) offering flexible services adapted to children's needs, and (5) implementing mechanisms to ensure service continuity and information transfer between agencies. These themes are key elements of speech-language pathology services to support children with DLD and are in line with recommendations about optimal delivery services based on an RTI framework. Indeed, service delivery reorganization following an RTI model can make it possible to address some of the gaps observed while building on existing facilitators. This model hinges on a needs-based, flexible service offer, and complementarity of services rather than organizational silos (Ebbels et al., 2019; Institut national d’excellence en santé et en services sociaux (INESSS), 2017). Consequently, to implement an RTI model, the five key elements discussed could be taken into account. Figure 1 presents an integration of these key elements in the RTI framework proposed by Ebbels et al. (2019).
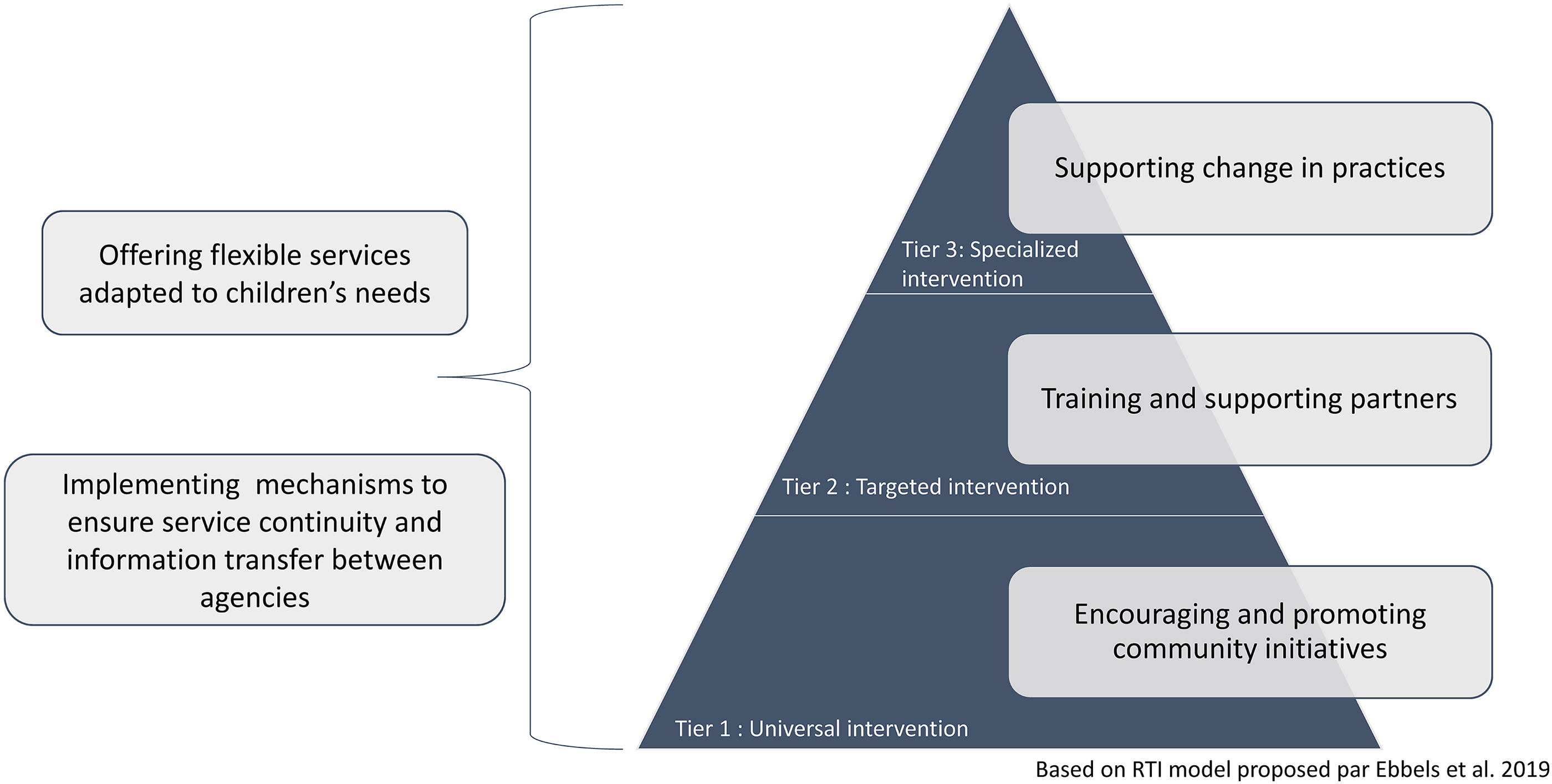
Key elements integrated in an RTI model.
First, as previously mentioned, this model encourages collaboration among partners. It highlights the value of indirect intervention by a parent or non-SLT professional in all tiers of the model (Boyle et al., 2007, 2009; Klatte et al., 2020; Law et al., 2003). For the purpose of training partners, professionals stressed the importance of being a trained trainer. A program such as Train-the-trainer can be a way to improve training skills among speech and language pathologists (Byington et al., 2020; Leung et al., 2020; Summerside et al., 2018). Second, it promotes a needs-based service offer. One of the strengths of this model is that it aims to add services based on children's needs and their response to intervention, which is in line with flexible services (Ebbels et al., 2019; Snow et al., 2015). This model also implies some changes in practice. Change in practice implementation should begin with introducing more parental coaching techniques by SLP as well as group interventions. It is recognized that early intervention is effective in supporting child language development, especially if the intervention is oriented toward parent-child interaction (Guralnick, 2011, 2017). It has also been shown that indirect language intervention, i.e., intervention by an assistant supervised by a speech-language pathologist, is just as effective as direct intervention practiced by the speech-language pathologist (Boyle et al., 2007, 2009; Klatte et al., 2020).
Regarding the RTI model, this study also highlights maximizing community potential. This idea is discussed by various authors in the field of child development (Grindal et al., 2016; Murphy et al., 2011; Williams and Lerner, 2019). However, the role of SLP and other child development professionals in community service promotion and collaboration must be further defined and encouraged by the health care system (Ebbels et al., 2019; Law and Pagnamenta, 2017). This study also highlights the importance of making standard use of the transition to school procedure in order to ensure a smooth transition for children with DLD. This entails close collaboration and communication with daycare centers and parents, as well as proper assessment of children's needs (Janus et al., 2008; Janus et al., 2007; Rosenkoetter et al., 2007).
Nevertheless, some challenges and limitations to the implementation of this model remain. First, to be effective, the RTI model requires that all three tiers are available within an integrated continuum of services (Ebbels et al., 2019). Language development needs must be promoted to positively influence services for children with DLD in the 0–5 age group, and SLT roles in each tier have to be better defined and encouraged (Bishop et al., 2016; Ebbels et al., 2019; Law et al., 2003; Snow et al., 2015). Second, in order to implement this approach, it is crucial to place emphasis on indirect intervention. Consequently, research about the effectiveness of group interventions and interventions via an assistant, educator, or teacher should be supported. This approach does yield positive results, yet it continues to be viewed by some as an affordable option that does not provide quality intervention (American Speech-Language-Hearing Association, 2008; Boyle et al., 2007, 2009; Klatte et al., 2020). That said, speech-language pathologist must keep in mind that for children to benefit from these interventions, those involved must be well trained and supported, which in turn requires significant resources (Parsons, 2019). Finally, context can be a limiting factor to implementation. Limited resources, lack of locally available and consistent services, long waiting lists, and age cut-off for eligibility are raised by parents and professionals as barriers to optimal service delivery (Liptak et al., 2006; Ruggero et al., 2012). These challenges and constraints illustrate the discrepancy between what we know and what we do (Theobald et al., 2018). To help organizations implement the RTI model and its various components, strategies should be discussed, including identifying facilitators and barriers to implementation, sharing local knowledge, conducting ongoing training, etc. (Powell et al., 2015; Waltz et al., 2015).
Given the exploratory nature of this study, the conclusions must be interpreted with caution while their transferability is limited by the small sample of participants and geographical areas including only two Quebec regions. In addition, participants who responded to the invitation to participate likely did so based on their commitment to improve service delivery. Their opinions may not reflect all professionals’ views. However, we made sure to involve professionals and managers from different backgrounds who are all committed to meeting children's needs. It is also important to mention that the classification according to the relevance is indicative of a possible researcher bias. It is therefore reasonable to expect that these results can guide actors in making changes with a view to optimizing services and improving school readiness of young children with DLD.
Conclusion
This study supports the relevance of a response to the intervention model in planning services for preschool children with DLD. It further highlights the importance of maximizing community initiatives, training and supporting partners, supporting change in practice, offering flexible services adapted to children's needs, and implementing mechanisms to ensure service continuity and information transfer between agencies of promoting community initiatives, training and communicating with partners, and changes in practice to better respond to children's needs. These key elements could be considered as recommendations for improving service delivery to better support school readiness for children with DLD.
Footnotes
Acknowledgments
This research was supported by the Centre for interdisciplinary research in rehabilitation and social integration (CIRRIS) and by Université Laval. We thank the participants and Emma DeChamplain, the research assistant.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Université Laval and the Cirris.