
Abstract
Adolescents in the care of the state have complex developmental needs that include low academic attainment. The aim of this study was to describe the language and literacy profiles of adolescents (aged 13–19) in out-of-home care (‘looked after children’). Mental health status, biopsychosocial history, and education and employment histories were also documented. Twenty-six adolescents were assessed by a speech and language therapist. Ninety-two percent had oral language skills below the average range on the Clinical Evaluation of Language Fundamentals: 4th edition, with 62% scoring two or more standard deviations below the mean. Ninety-two percent of participants scored below the average range on two or more subtests of the Test of Language Competence: Expanded edition. On the York Assessment of Reading Comprehension, 92% scored in the very low range and 65% were below-average on single-word reading. Fifty percent of participants reported a diagnosis/symptoms of depression and 54% reported a diagnosis/symptoms of anxiety. The correlation between oral language and literacy was modest but significant (r = 0.502; p ⩽ 0.05); no significant correlations were found between oral language, literacy and mental health status, suggesting that mental health problems are a comorbidity rather than a correlate of language and literacy difficulties. Language and literacy difficulties are highly prevalent in this population. Language disorders are likely to be undiagnosed in the context of significant mental health problems, and disrupted schooling and accommodation. Speech-language therapy scope of practice needs to include out-of-home care populations in order to foster developmentally appropriate language and literacy skills that maximize school success, both academically and socially.
I Introduction
In the UK, children in the care of the state are referred to as ‘looked after children’, and it was estimated in 2016–17 that there were 96,000 such children, with increases occurring in recent years in England, Northern Ireland and Wales, against a decrease in Scotland (National Society for the Prevention of Cruelty to Children, 2019). In Australia, out-of-home care (OoHC) refers to short-, medium- or long-term living arrangements made for minors aged 0–17 years who cannot, according to the assessment of human services personnel, safely remain living in their family home. OoHC is typically statutory, i.e. a legally-ordered arrangement made due to substantiated instances of various combinations of abuse, neglect and/or family violence (Australian Institute of Family Studies, 2019a), collectively known as maltreatment. In the state of Victoria, the Department of Health and Human Services (DHHS) provides oversight for OoHC, and various community and not-for-profit service providers coordinate the provision of care. Care types include foster care, kinship care, permanent care and residential care 1 (Australian Institute of Health and Welfare, 2018). In June 2017, 47,915 Australian children were living in OoHC (8.7 per 1,000), which is an increase from 7.4 per 1,000 children in June 2011 (Australian Institute of Family Studies, 2019a). This rate is similar to that in England (6.6 per 1,000; Department for Education, 2017). Young people from Aboriginal and Torres Strait Islander backgrounds are overrepresented in OoHC at a rate of 16:1 (Australian Institute of Family Studies, 2019b). The reasons for this are complex and multifactorial, relating to Australia’s history of colonization, inequitable government support policies, poverty, and ongoing intergenerational trauma (Titterton, 2017).
1 Background
Young people in OoHC have long been known to be highly developmentally vulnerable, by virtue of their unsafe and/or chaotic family backgrounds, lack of stable adult carers and role models, disrupted education, and exposure to adverse childhood experiences (ACEs; Jamora et al., 2009). ACEs include various forms of childhood maltreatment, as well as exposure to traumatic incidents, such as family violence and the sudden loss of a key attachment figure. A key point about ACEs is that they are cumulative and their effects are likely to persist into adolescence (Appleyard et al., 2005) and often manifest as chronic physical and/or mental health problems, risky health behaviours, and compromised potential across the life-span (Hughes et al., 2017).
Maltreated children and adolescents experience lower secondary school graduation rates (Lemkin et al., 2018), higher rates of school absenteeism, and poorer mental health outcomes than their non-maltreated peers (Hagborg et al., 2018; Tarren-Sweeney and Hazell, 2006). Further, many young people in OoHC experience multiple placements (Delfabbro et al., 2010), resulting in numerous changes of school. Disrupted schooling can contribute to an exacerbation of problem behaviour, risk of school disengagement, and criminal conviction (Fine et al., 2018). In 2017, the Australian Institute of Health and Welfare reported on the (Australian) National Assessment Programme Literacy and Numeracy (NAPLAN) scores of 3,583 children (aged 7–17 years) in OoHC in 2013 and identified them as an academically disadvantaged group. Notably, however, NAPLAN does not measure oral language skills and these have not yet been documented in Australian adolescents in OoHC. NAPLAN also does not measure the decoding component of reading, as conceptualized in the Simple View of Reading (Gough and Tunmer, 1986), and so does not provide a complete picture about the skill profiles of students. These Australian Institute of Health and Welfare findings are consistent with a review of 29 studies concerning academic outcomes of children in OoHC (Trout et al., 2008), indicating that children in all types of OoHC performed in the low to low-average range on academic measures, including reading comprehension, though studies that specifically assessed receptive and expressive language skills were not identified.
2 Language skills in vulnerable children and adolescents
In community samples, it is estimated that approximately 7–10% of children have a Developmental Language Disorder (DLD; Tomblin et al., 1997), 2 and in recent years, there has been a growing interest in the extent to which language development is compromised by a child’s experience of maltreatment. A recent meta-analysis by Lum et al. (2015) showed a reliable relationship between early experience of maltreatment and adverse outcomes for language development. This has important implications for both the development of prosocial interpersonal skills and for making the transition to literacy in the first three years of school (Snow, 2016). Notably, the Royal Australasian College of Physicians (2006) reported that the speech language and communication needs (SLCN) of children in OoHC are likely to be overlooked by service providers; there is little reason to believe that this has changed in the ensuing 14 years.
Victorian data collected via an OoHC commissioned study (Frederico et al., 2014) identified that 77% of children for whom maltreatment had been substantiated and who human service practitioners reported did not have SLCN needs were subsequently identified by a speech and language therapist to in fact have such needs. Frederico et al. recruited 65 participants (aged 4–8 years) from community service organizations and an Aboriginal organization in Victoria. Eleven were living at home and 54 were in out-of-home care. None of the children had been previously assessed with respect to their communication needs, yet 57 (88%) required referral for SP intervention, with the majority having deficits in two or more communication domains. Ninety-four percent (n = 61) of participants completed formal standardized assessment, of which 44% had global language scores one or more standard deviations below the mean.
There is significant overlap between child protection and youth justice (YJ) populations (Snow, 2019), and the prevalence of DLD/LD is also high in YJ samples, ranging between 38% and 70%, depending on study inclusion criteria and assessment tools (Snow, 2019). In a related population of young people, Snow et al. (2019) recently identified that 72% of adolescents attending flexible education programs had oral language skills that placed them in an at-risk range, and nearly half (47.5%) had reading comprehension ages of less than 12 years. Notably, when examining the language skills of young people in custody, Snow and Powell (2011) reported that DLD rates were higher amongst those who had a history of living in OoHC, suggesting a compounding risk phenomenon, and a need to pay closer heed to the needs of young people in care, addressing these before they are in trouble with the law. There appears to be less research on adolescents in care than younger children, however, in their investigation into the language skills of adolescents entering a residential care program, Trout et al. (2011) reported that the group mean Core Language Score on the CELF-4 (Semel et al., 2003) was in the borderline/mildly impaired range (M = 78.48, SD = 15.53), with nearly three-quarters of the sample showing some degree of overall risk with respect to language skills. With the exception of this study however, estimates of the prevalence of DLD/LD in adolescents, as opposed to children in OoHC appear to be lacking.
3 Aim and research questions
The aim of this study was to describe the receptive and expressive oral language abilities and reading (decoding and comprehension) skills of a sample of adolescents living in OoHC in Victoria, Australia. We hypothesized that the prevalence of language difficulties would be significantly higher than those seen in community samples, consistent with data collected on maltreated children and adolescents in youth justice and flexible education, and that there would be a positive correlation between oral language skills and measures of reading ability. We also examined the prevalence of mental health problems in the sample and explored the relationship between language skills and mental health functioning, and reading comprehension and mental health, hypothesizing that rates of high-prevalence mental health problems (anxiety and depression) would be significantly associated with more problematic language and literacy profiles. The study was approved by the La Trobe University Human Research Ethics Committee, the Victorian Department of Health and Human Services, and Anglicare Victoria.
II Method
1 Participants
A convenience sample of 26 young people living in OoHC in Victoria, Australia, was recruited over a 12-month period. Recruitment occurred across three services, in metropolitan and regional Victoria. Inclusion criteria were as follows: stable mental state (not suffering from acute mental illness, e.g. psychosis; not acutely agitated or distressed), not substance affected, and having completed the majority of schooling in an English-speaking country. Young people from Aboriginal and Torres Strait Islander (ATSI) backgrounds were only recruited if they reported having grown up in metropolitan areas or regional centres and identified Standard Australian English (SAE) as their first language. A structured biographical interview, which has been used in previous studies of at-risk young people, was used to elicit self-report information regarding neurobiological diagnoses, type of OoHC, time spent living in OoHC, receipt of additional supports at school, and post-school vocational training and/or employment.
The sample included 12 females and 14 males. The mean age was 15.2 (SD 1.7; range 13–19 years). All participants had English as their first language. Seven (27%) were Aboriginal or Torres Strait Islander with none from other cultural or linguistic backgrounds. Nineteen participants (73%) were still attending school, although not necessarily mainstream secondary school settings. The remaining seven participants were not attending school, and on average they had been disengaged from education for seven or more months. The mode for the highest year level attained was Year 7 (the first year of secondary school in Victoria 3 ). Sixty-two percent of participants reported a history of exclusion (suspension and/or expulsion) because of behaviour problems; 31% reported attending an alternative/flexible education setting, and 15% reported attending a specialist school setting.
Six participants (23%) reported at least one neurodevelopmental diagnosis. These included foetal alcohol spectrum disorder (n = 1), autism spectrum disorder (n = 2), intellectual disability (n = 3), and traumatic brain injury (n = 2). Only one participant reported an SLCN diagnosis. Twelve participants (46%) reported this was an area of difficulty for them and 13 (50%) reported no SLCNs. Nine participants (35%) reported receiving at least one form of additional assistance at school: support from an integration aide/teacher’s assistant (n = 5), Reading Recovery® (n = 6), speech-language therapy (n = 3) and ‘other’ support (sessions with the school counsellor; n = 1).
Five participants (19%) reported engaging in vocational education and training – community or Technical and Further Education (TAFE) 4 based – with the median being four courses commenced and none completed. Five participants (19%) reported being in open employment, most commonly for a duration of 0–6 months.
Age of first OoHC placement was self-reported. This was at 12 years or younger for 18 (69%) participants, including two aged 2 years or below, five aged 2–5 years, and 11 aged 6–12 years. The remaining eight participants (31%) reported being aged over 12 years when first placed in OoHC. Most participants were in foster care (38.5%) or residential care (34.6%) with the remainder in kinship care (19.2%) and permanent care (7.7%).
Seven participants (27%) reported contact with youth justice (YJ), with three being current YJ clients and four being past YJ clients. All of these seven reported having Community Based Orders (CBO), which are flexible orders allowing a court-imposed sentence to be served within the community (Sentencing Advisory Council, 2019).
2 Measures and procedure
a Expressive and receptive language
The Core Language Score (CLS) was derived from four subtests of the Clinical Evaluation of Language Fundamentals: 4th edition, Australian standardization (CELF-4; Semel et al., 2003). These are: Recalling Sentences, Formulated Sentences, Word Classes (Receptive and Expressive) and Word Definitions. The CELF-4 provides detailed, norm-referenced data and is widely used in Australia and overseas, in both clinical and research contexts, as an accepted measure to determine the presence of a language disorder and entitlement to specialist services (e.g. speech-language therapy services in schools).
Three subtests of the Test of Language Competence: Expanded edition (TLC-E) 5 were included as measures of figurative and idiomatic use of language, in contrast to the CELF-4, which is commonly regarded as a measure of ‘structural’ aspects of language (e.g. vocabulary and syntax use and understanding). The test’s psychometric properties are outlined in the technical manual (Wiig and Secord, 1989).
Subtest 1 (Ambiguous Sentences) requires the interpretation of sentences with lexical, surface structural and underlying structural ambiguities for which two alternative meanings are identified and explained by the participant; e.g. ‘John was looking up the street’: he was either standing on the street and physically looking up to the other end or he was looking up the street in a map. Subtest 2 (Listening Comprehension: Making Inferences) requires the drawing of inferences based on incomplete information, which is presented as an event chain by choosing two plausible story outcomes from four choices. Subtest 4 (Figurative Language) requires the interpretation of metaphoric expressions, through selection of an alternative from four options; e.g. recognizing that the phrase ‘There is rough sailing ahead of us’ has a non-literal meaning concerning difficult times. In each of these subtests, the participant both heard and saw the printed stimuli, which were placed in clear view and read aloud by the examiner.
b Discourse and pragmatic language skills
The La Trobe Communication Questionnaire (LCQ; Douglas et al., 2000, 2007a, 2007b) was used to ascertain participants’ own views about their everyday discourse/pragmatic language abilities. This tool is derived from Grice’s (1975) Cooperative Principle of Conversation, which is built around four key maxims pertaining to quality (speakers should say only that which they believe to be true), quantity (speakers should say neither more nor less than what is required to convey meaning to their listener), relation (speakers should keep their contributions relevant) and manner (speakers should converse in an orderly, easy to follow way). In addition to representing these maxims, the LCQ contains items pertaining to communication behaviours that are influenced by cognitive function; e.g. losing track of conversations in noisy places and difficulty thinking of things to say to keep a conversation going. LCQ items are self-rated on a 1–4 ordinal scale pertaining to the perceived frequency with which difficulties are experienced (1 = never; 4 = always). Scores can range from 30–120; except for items that are reversed-scored: the higher the score, the greater the perceived difficulty. Six items are reverse scored, in order to guard against a response-set pattern. The LCQ has been shown to have strong validity and reliability, as well as a robust factor structure (Douglas et al., 2000, 2007a, 2007b). An example of an LCQ manner item is: ‘When talking to others do you use a lot of vague or empty words such as “you know what I mean” instead of the right word?’ In order to be confident that responses were not adversely influenced by poor reading skills, participants were given the option of reading items silently themselves, reading them aloud with scaffolded support by the research assistant (a speech and language therapist), and/or having the research assistant read them aloud.
c Reading
The York Assessment of Reading for Comprehension Secondary: Australian edition (YARC; Snowling et al., 2012) was used to assess reading. This comprises a test of single word reading and the reading of two passages, one fiction and one non-fiction. The test of single word reading measures reading accuracy (decoding skills), while passage reading is used to assess reading rate, fluency, comprehension and summarization. Standard scores map to percentile ranks and age-equivalents of between 7;01 years and 18;07 years (Snowling et al., 2012).
YARC scores can be aligned with the Simple View of Reading in which Gough and Tunmer (1986) proposed that reading is the product of decoding ability and language comprehension ability, where scores on each of two dimensions can range from zero (nullity) through to one (perfection). Reading ability is therefore measured via both decoding skills and language comprehension skills. The test affords classification of participants as having a typical reading profile, a decoding difficulty only, a language comprehension difficulty only, or a mixed decoding-language comprehension difficulty.
d Social emotional functioning
The Strengths and Difficulties Questionnaire (SDQ; Goodman, 2001) was used to gauge participants’ self-assessment regarding their everyday functioning. Participants rated themselves across 25 attribute statements (e.g. ‘I worry a lot’) across the domains of Emotional Symptoms, Conduct Problems, Hyperactivity/Inattention, Peer Relationship Problems and Prosocial Behaviours. Scores from Emotional Symptoms, Conduct Problems, Hyperactivity/Inattention and Peer Relationship Problems were tallied to determine a Total Difficulties Score. We also obtained an Emotional Symptoms Score, Conduct Problems Score, Hyperactivity Score, Peer Problems Score and Prosocial Behaviour Score, which can all be rated as ‘normal’, ‘borderline’ or ‘abnormal’. An Impact Score was also generated based on participants’ rating of total distress experienced as a consequence of their difficulties, as well as the impact they felt their difficulties had on home life, friendships, classroom learning, and leisure activities respectively. As per administration of the LCQ (see above), participants were provided with scaffolded support to read and understand the SDQ items.
3 Data analysis
Results are reported categorically and as frequencies with respect to test scores, and associations between language, literacy, and mental health variables are reported as Pearson’s r correlations. Inter-rater reliability and scoring accuracy checks were conducted on a random sample of 20% of standardized test scores before data entry and data analyses were undertaken. These checks were conducted by a speech and language therapist not involved in data collection. The two speech and language therapists scored independently and then met to compare outcomes. Scaled scores of any subtest that differed by more than one point were re-scored by both parties independently then discussed. If subtest scores differed by only one point, the original subtest score was retained. There was perfect agreement for 19/30 subtests checked and 8/30 checked subtest scores differed by one point only, so the original was retained. Ten percent of subtest scores had differences of 1 or more scaled score points and consensus was achieved on all of these prior to analysis.
III Results
1 Language
The CELF-4 CLS mean for the sample was 67 (SD = 15; range = 40–100), more than two standard deviations below the test mean of 100 (SD = 15). Most participants (92.3%) scored below the average range, with 61.5% scoring in the very low range. Scores are summarized in Table 1.
CELF-4 core language scores: Severity breakdown.
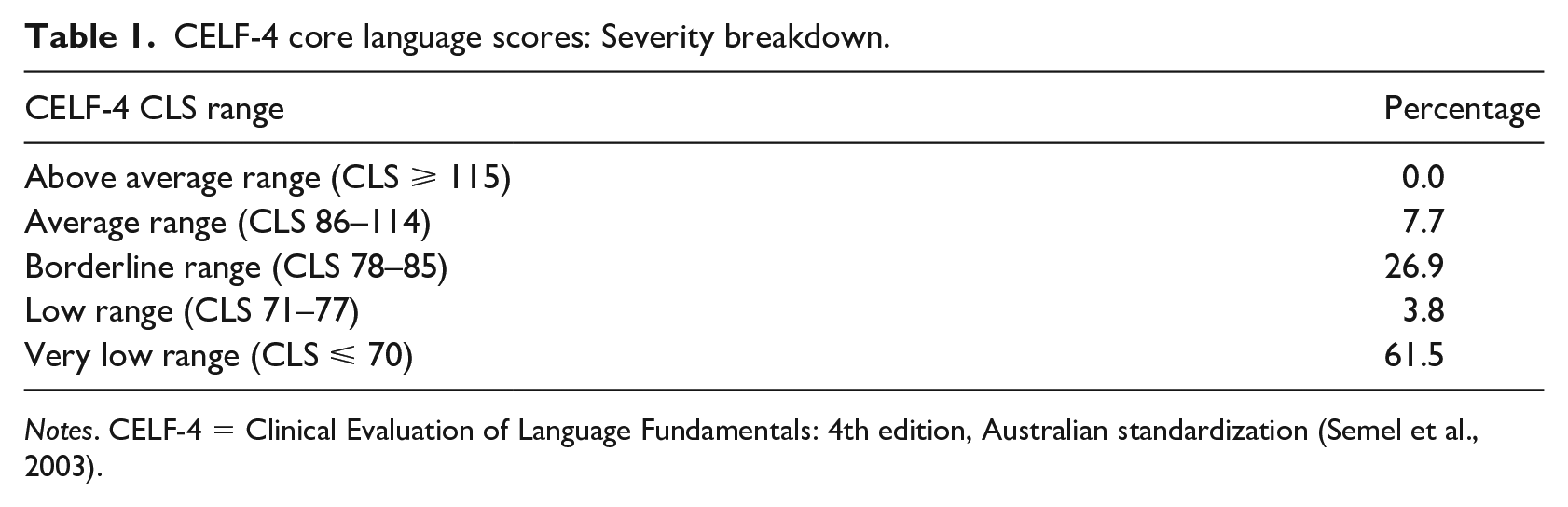
Notes. CELF-4 = Clinical Evaluation of Language Fundamentals: 4th edition, Australian standardization (Semel et al., 2003).
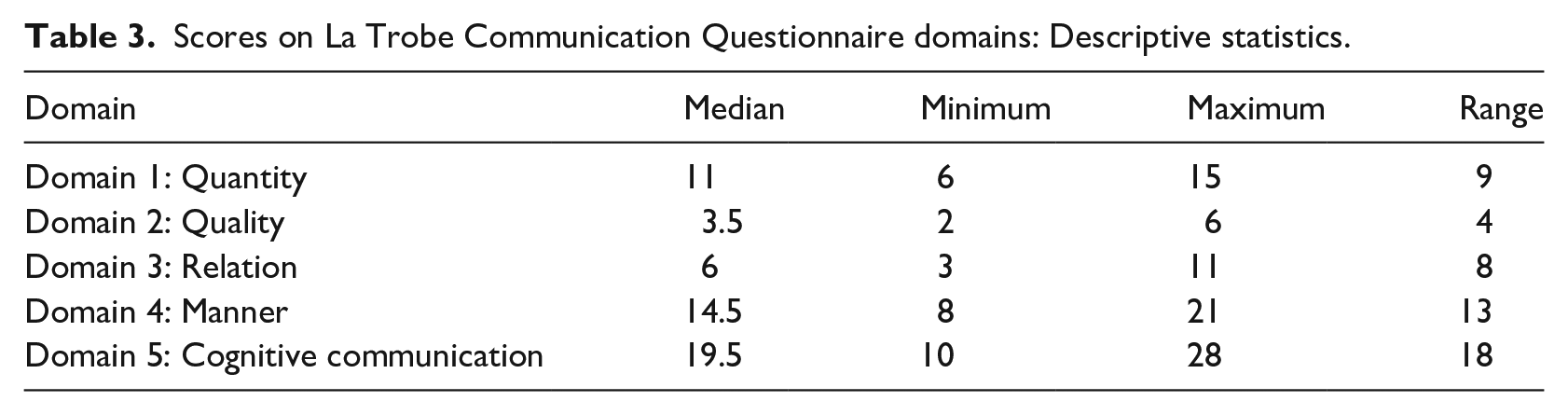
On all three TLC-E subtests, the sample mean fell well below the test mean of 10 (SD = 3), with all means falling between one and two standard deviations below the test mean. Ninety-two percent of participants scored below the average range on two or more subtests. Details are recorded in Table 2. Table 3 summarizes the scores across the five LCQ discourse domains. The median score for the sample was 65 (range 40–92). Quantity, manner, and cognitive communication were rated as the areas of greatest difficulty.
Test of language competence-expanded edition subtest scaled scores: Descriptive statistics.
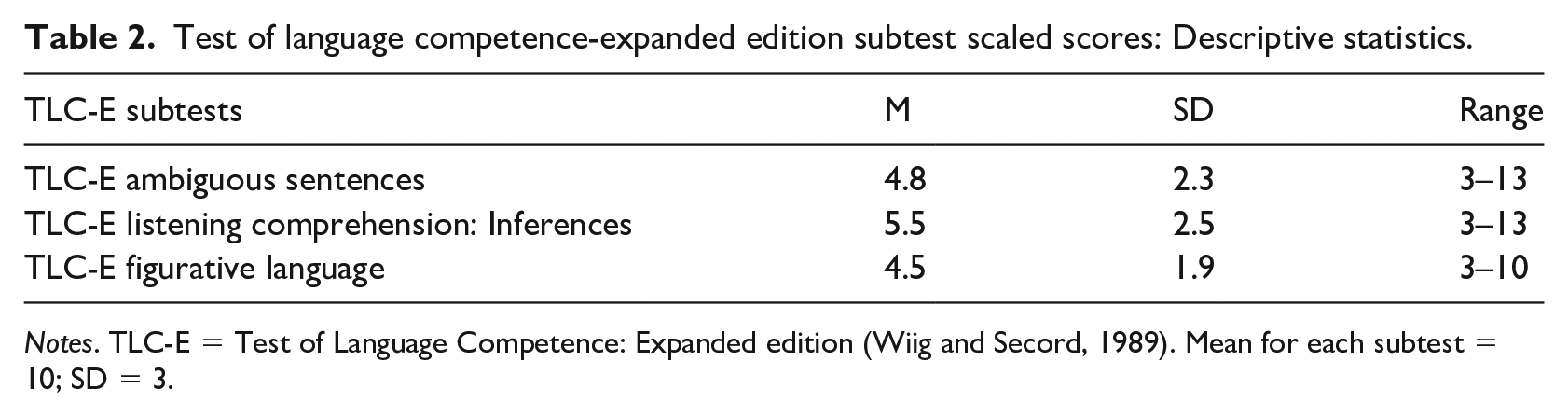
Notes. TLC-E = Test of Language Competence: Expanded edition (Wiig and Secord, 1989). Mean for each subtest = 10; SD = 3.
Scores on La Trobe Communication Questionnaire domains: Descriptive statistics.
2 Reading
The mean standard score for single word reading was 80.7 (SD = 13), which is more than one standard deviation below the test mean of 100 (SD = 15). The median age equivalent was 12.2 years (against a mean age for the sample of 15 years). The majority of the sample (65.4%) scored below the average range, with 42.3% scoring in the very low range, as summarized in Table 4, which also displays group scores for rate, fluency, and comprehension. Notably, 100% performed below the average range on reading comprehension.
YARC reading scores × reading domains: Descriptive statistics and score breakdown (percentages).
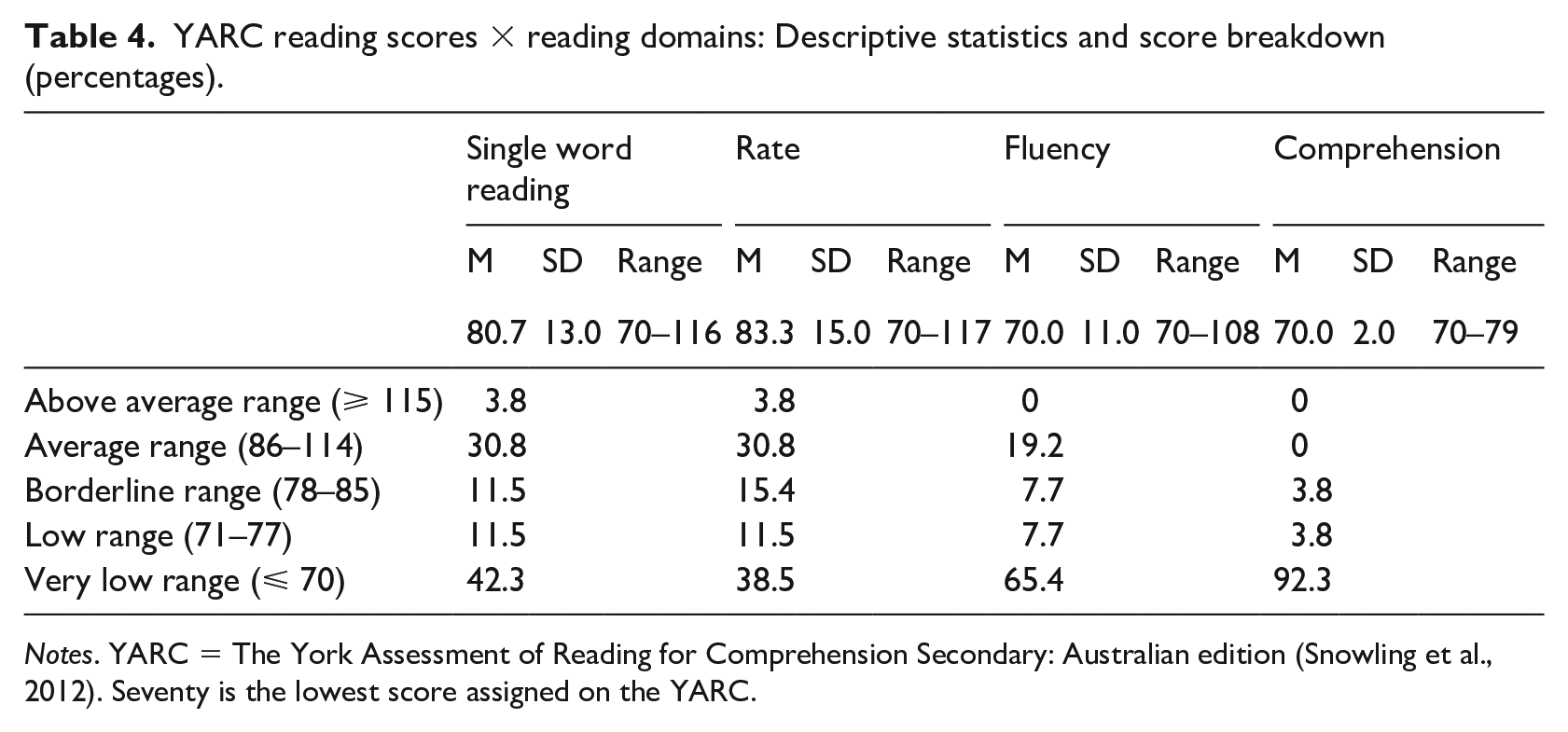
Notes. YARC = The York Assessment of Reading for Comprehension Secondary: Australian edition (Snowling et al., 2012). Seventy is the lowest score assigned on the YARC.
In terms of the Simple View of Reading (Gough and Tunmer, 1986), no participant had a typical reader profile and no participant had a pure decoding problem. Ten participants (38.5%) had difficulty with comprehension only, while the remaining 16 participants (61.5%) had a mixed decoding-comprehension difficulty. Decoding was an area of difficulty for the majority, with 65.3% scoring below the average range. Comprehension ability was two or more standard deviations below the mean for all but two participants. 92.3% of participants scored in the very low range for reading comprehension, and no participant scored within the average range.
3 Psychosocial functioning
Ten participants (38%) reported one or more formal mental health diagnoses. Of these, five reported two diagnoses and one reported three. Depression and anxiety diagnoses were equally most common. Ten participants (38%) reported no symptoms of mental ill health. On the Strengths and Difficulties Questionnaire, the mean total difficulties score (out of 40) was 14.5 (range 3–28), compared to the Australian community norm of 9.1 for 14–17-year-olds (Mellor, 2005). Thirteen participants had scores within the normal range, five had scores in the borderline range, and eight had a score in the abnormal range. Scores across the domains of Emotions, Conduct, Hyperactivity, Peer Problems, Prosocial and Impact are displayed in Table 5. Difficulties for this sample far exceeded rates in community samples for 14–17 year olds for Emotions, Conduct, Hyperactivity and Peer Problems, while for Prosocial this sample scored below that of the community norm.
Scores across Strengths and Difficulties Questionnaire domains (percentages).
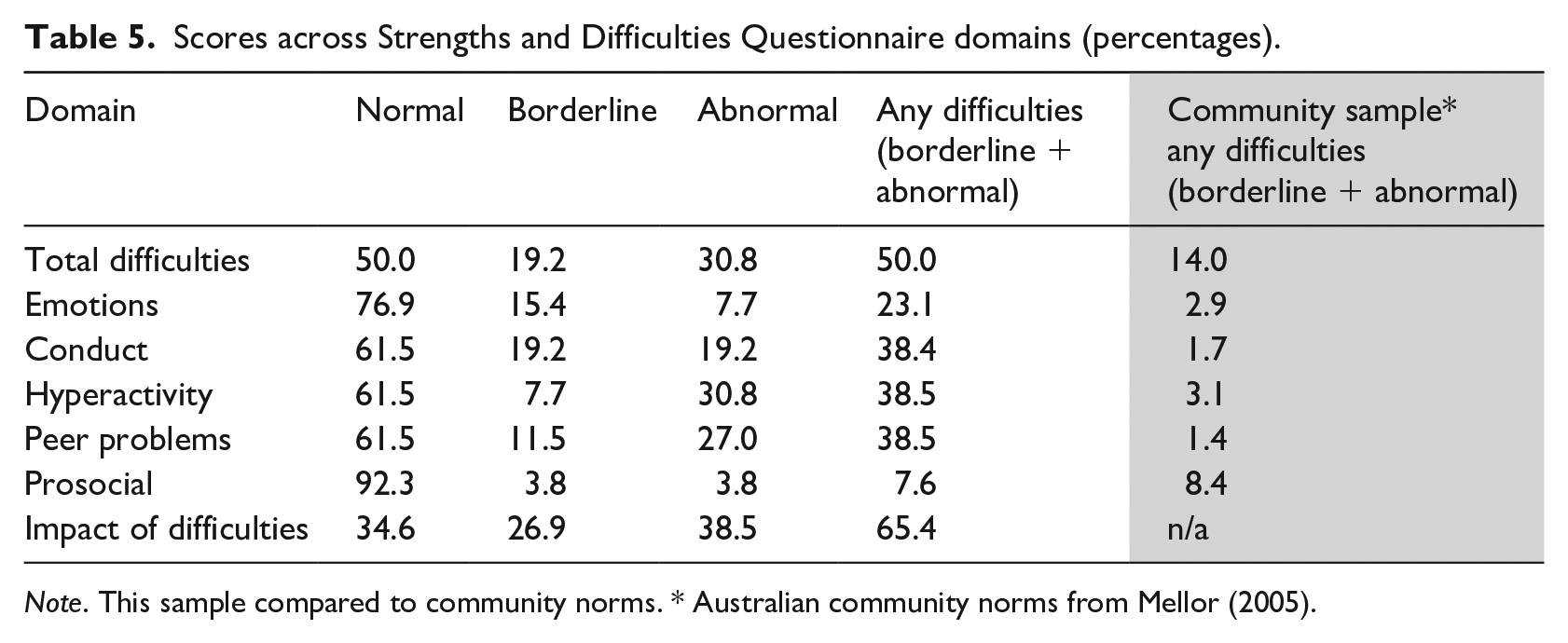
Note. This sample compared to community norms. * Australian community norms from Mellor (2005).
4 Correlations
Examination of the relationship between oral language and literacy, using the composite language score from the CELF-4 CLS and TLC-E subtest scores and the YARC Comprehension scaled score revealed a moderate, significant positive relationship (r = 0.502; p = 0.009). There was no relationship between composite language scores and mental health (SDQ total difficulties; r = .366, p = 0.06) or literacy (YARC comprehension scores) and mental health (r = .252, p = 0.21). It is noted, however that 24 of the 26 participants had the same, lowest possible standard score (70) on the YARC Reading Comprehension measure, which is likely to have created a floor effect.
IV Discussion
Our findings indicate that language disorders are so common in this population as to be almost normative; 92% scored below average on the CELF-4 CLS and mean scores on all TLC-E subtests were between one and two SD below the test mean. This suggests that structural and idiomatic use of language are equally and severely impacted for this population. Notably, participants seemed to have some awareness of difficulties with pragmatic (discourse-level) communication abilities, as reflected in their LCQ self-ratings, which highlighted difficulties in the quantity, manner, and cognitive-communication aspects of everyday discourse in particular. In addition to their highly impoverished oral language skills, this group displayed extremely marked difficulties with reading, at both the decoding and comprehension levels. Two thirds of the sample performed below average on single word reading, and 100% performed below average on reading comprehension, with the vast majority being in the very low range. As hypothesized, there was a significant association between composite oral language scores and reading comprehension. This is line with findings derived from a related sample, adolescents in flexible education settings (Snow et al., 2019), and underscores the importance of oral language skills for reading success (Snow, 2016). Notably, 24 of the 26 participants had the lowest-possible standard score (70), which is equivalent to a reading age of 7;01. It is not possible, however, to determine how many participants had reading abilities below this level.
Our findings suggest that neurodevelopmental disorders are strongly over-represented in the OoHC population, with nearly a quarter of the sample self-reporting diagnoses such as autism, intellectual disability, and traumatic brain injury. This is consistent with evidence that such diagnoses are over-represented in high-risk adolescents (for review, see Snow, 2019) and further strengthens the case for access to specialist services such as speech-language therapy for this population, given the implications of such diagnoses, even without maltreatment histories, for the development of language and literacy skills.
Although the sample as a whole reported high levels of distress with respect to their mental health and wellbeing, we did not find a significant association between this dimension and either oral language skills or reading comprehension. With respect to reading comprehension, this is likely to reflect the floor-effect described above. Although not necessarily correlated, it is important for clinicians to understand the levels of comorbidity in these dimensions, as anxiety and depression require specialist services alongside speech-language therapy services. Teacher aides may be effective in supporting the learning needs of struggling students, but only where certain pre-conditions are met with respect to their training, support and monitoring (Farrell et al., 2010). Children and adolescents with language and literacy difficulties and backgrounds of complex trauma histories are likely to require highly focused interventions, based on diagnostic data derived from specialist assessments. Generic classroom approaches are unlikely to be high-impact in the face of severe and complex disorders.
Histories of school exclusion were common in this sample, consistent with the fact that co-occurring behaviour disturbance and DLD/LD can compromise social and academic success (Lum et al., 2018; Romano et al., 2015). Social and academic engagement are critical to the prevention of entry to the so-called ‘school-to-prison-pipeline’ (Christle et al., 2005), bearing in mind, however, that life-long social marginalization is also a form of imprisonment, albeit one that is not time-limited (Snow and Douglas, 2017). Pleasingly, there is a growing body of evidence indicating that speech-language therapy interventions can be effective for struggling adolescents, both in the mainstream (Lowe et al., 2018) and in youth custodial settings (for review, see Snow, 2019). It remains to be seen, however, whether such interventions can be delivered effectively to the OoHC population, and this needs to be a focus of future research.
While most children and adolescents with a history of living in OoHC do not have contact with the justice system, the risk of criminal conviction is significantly greater for those who have had child protection notifications made on their behalf, maltreatment substantiated by child protection services, and/or have lived in OoHC (Malvaso et al., 2017). Of note, a young person convicted of a criminal offence is likely to have experienced maltreatment (Malvaso et al., 2017), and rates of language disorder in youth offenders have been reported as higher in those who come via child protection (Snow and Powell, 2011). The 2019 Cross-over Kids Report (Sentencing Advisory Council, 2019), about Victorian children who are engaged with both the child protection and youth justice sectors, indicated that 38% of young people sentenced or diverted in the Children’s Court were known to Child Protection. The significant cross-over between child protection and youth justice systems highlights the level of psychosocial, academic, and vocational risks to which this population is exposed and the need for ‘joined-up’ services to prevent further psychosocial disadvantage accruing as a result of disjointed and inefficient service-delivery systems (Mendes et al., 2014).
A number of limitations need to be considered in relation to our sample, which was small in size, and non-random. Data were collected in only one state (Victoria, Australia) and in only two services, and were cross-sectional rather than longitudinal. Our reliance on self-report for information about care histories means that some inaccuracies will be inevitable.
V Conclusions
Our findings lend support to the limited extant literature regarding the oral language and reading skills of adolescents in out-of-home care, and are consistent with, but even more concerning than those reported by Trout et al. (2011). The findings reported here suggest that adolescents in out-of-home care are highly vulnerable with respect to their ability to use and access everyday spoken and written language. Given the importance of spoken communication skills and at least functional literacy for vocational training and employment, it is vital that these young people have access to intensive speech-language therapy services from an early age, to maximize educational outcomes and social-emotional wellbeing. This needs to be a matter of policy and service-delivery priority in pre-school and school-aged prevention and intervention frameworks and settings. Such services need to be provided within the context of an interdisciplinary team, so that children’s complex biopsychosocial needs are anticipated and met by appropriately qualified professionals.
Footnotes
Acknowledgements
We would like to thank our partner agency (Anglicare Victoria) and their staff for their assistance in conducting this study. We also thank the Victorian Government Department of Health and Human Services (DHHS), the Centre for Evaluation and Research Evidence (CERE) for their continuing generous support of the Language and Literacy Skills of Adolescents in Out-of-Home Care Project.
The opinions in this report reflect the views of the authors and do not necessarily reflect those of Anglicare Victoria or DHHS.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by an internal La Trobe University Transforming Human Society Research Focus Area (RFA) Grant.