
Abstract
Children and young people living in care (aka looked-after children and young people) are at a high risk of language development delays. This scoping review aimed to identify and synthesise research published between 1989 and 2024 that examines the prevalence, nature and key areas of language difficulties among children and young people in care. It also aimed to report associated risk and protective factors and to identify existing intervention strategies relevant to supporting their language development. An iterative search strategy resulted in the inclusion of 38 studies, with the majority conducted in the United States (n = 12). Studies varied widely in terms of methodological factors, and most were single research projects that had not been replicated. A range of language screening tools were used which included well-known and less-known measures that had different clinical thresholds. The results indicated that children and young people in care are at a greater risk of experiencing difficulties in all areas of language. This topic thus warrants more attention and further investigation. This research has the potential to significantly influence both policy and practice by highlighting the critical need for early identification and support for language difficulties among children in care, particularly those who have experienced maltreatment.
Keywords
Introduction
The development of language in children is complex and multifaceted, beginning in infancy and continuing through early childhood and into adolescence (Asmussen et al., 2018; Johnson et al., 2010; Kennison, 2014). However, there is considerable variation in the rate and extent of language development among children. Several factors contribute to these variations, including socioeconomic status, exposure to language-rich environments (Harrison and McLeod, 2010; Hart and Risley, 1995), and being born in deprivation (Vernon-Feagans et al., 2012). One group which exhibits much variability in the development of language are children and young people living in care.
Background
In the UK, children and young people in care are those under the age of 18 who have been looked after by local authorities for more than 24 hours (DfE, 2018). The terminology used to define children in care differs across countries. For example, the USA, Sweden, Canada and Australia use the term ‘children in out-of-home care’ (OHC or OoHC) and the United Nations International Children's Emergency Fund (UNICEF) uses ‘children in alternative care’. Despite differences in terminology, a common trend is that children and young people are frequently placed in care due to exposure to adverse childhood experiences (ACEs) such as maltreatment, neglect and other forms of trauma (DfE, 2022; Krier et al., 2018; Stacks et al., 2011). The presence of multiple ACEs significantly heightens risk of developmental delays and long-term challenges in areas such as educational attainment, social and emotional development, mental health and behavioural issues (Frederico et al., 2018; Lorio et al., 2022; Pears and Fisher, 2005). Children and young people in care are placed in various out-of-home care (OHC) environments when they can no longer safely remain in their family homes (e.g. Coman and Devaney, 2011; Jones et al., 2011). These OHC arrangements encompass a wide range of living environments, including institutions, foster care, residential care, and kinship care (Berger et al., 2009; McGrath-Lone et al., 2017). While most children in care report that their experiences are positive and that entering care was the right decision for them (Biehal et al., 2014), the circumstances leading to a child to be taken into care are often complex and multifaceted. These complexities frequently involve a disruption in the parent–child relationship due to ACEs with subsequent placement instability further compounding developmental delays, particularly in the area of language (Raby et al., 2018).
Language development is profoundly influenced by early, stable and responsive interactions with caregivers, which are essential for emotional regulation and social competence (Palazón-Carrión and Sala-Roca, 2020). However, children exposed to ACEs, such as maltreatment, often lack these critical experiences, which may hinder language acquisition (Sylvestre et al., 2016). Research consistently links exposure to ACEs with poorer language outcomes. Maltreated children often exhibit significantly weaker language skills compared to non-maltreated peers (Pears and Fisher, 2005), with a meta-analysis revealing that they score on average, one standard deviation below their peers in expressive language (Lum et al., 2015). Pragmatic language refers to the use of language in social contexts, encompassing the ability to adjust language according to the listener's needs, follow conversational rules and interpret non-literal language such as jokes and sarcasm. Pragmatics appears especially vulnerable due to its reliance on early social interactions that maltreated children often miss (Di Sante et al., 2019; Sylvestre et al., 2016). Despite the previous investigtions, language development and difficulties, within the children in care population, remain under researched. This scoping review aims to examine the literature on language development in children and young people in care by exploring the prevalence and nature of language difficulties, the associated risk and protective factors, particularly those related to care experiences and ACEs, and the intervention strategies used to support this population.
Methods
The scoping review was guided by Arksey and O’Malley's (2005) framework, which has several stages: (a) identifying the research question, (b) identifying relevant studies, (c) selecting studies, (d) charting the data, (e) collating, summarising and reporting the results and (f) an optional consultation stage. Since the topics related to language difficulties in children and young people in care remain underrepresented in the literature, the scoping review methodology enabled a preliminary mapping of the evidence. The optional stage (f) of consultation was not undertaken.
Identifying the research questions
In line with the aims of the review, the following research questions were formulated:
RQ1: What is the rate/prevalence of language difficulties in children and young people in care?
RQ2: What aspects of language development are affected in children and young people in care?
RQ3: What protective and risk factors for language difficulties are connected to OHC settings or the ACEs leading to being taken into care?
RQ4: What are the types of intervention strategies used to support language difficulties in children and young people in care?
Identifying relevant studies
The reviewers adopted a three-step search process: database searches, reference list screening, and grey literature searches (Joanna Briggs Institute, 2015). Search terms were developed utilising the Population–Concept–Context (PCC) Framework (Joanna Briggs Institute, 2015). A comprehensive search of Medline, CINAHL, Embase, PsycINFO, PubMed, NICE, and Web of Science was conducted to identify English-language publications from November 1989 to October 2024. The complete list of search terms used in the databases can be found in Appendix A, Table A1. The searches were undertaken in two stages: (a) Medical Subject Headings (MeSH) and (b) keyword search. Search terms reflecting the same concepts were combined with ‘or’, and search terms reflecting different concepts were combined with ‘and’. Subsequently, a search of reference lists and grey literature was performed to identify both published and unpublished studies. The use of a three-step search strategy, combined with the removal of duplicate entries, resulted in a total of 397 research articles. Examples of electronic database search strategies are presented in Table 1.
Examples of search concepts and keywords.
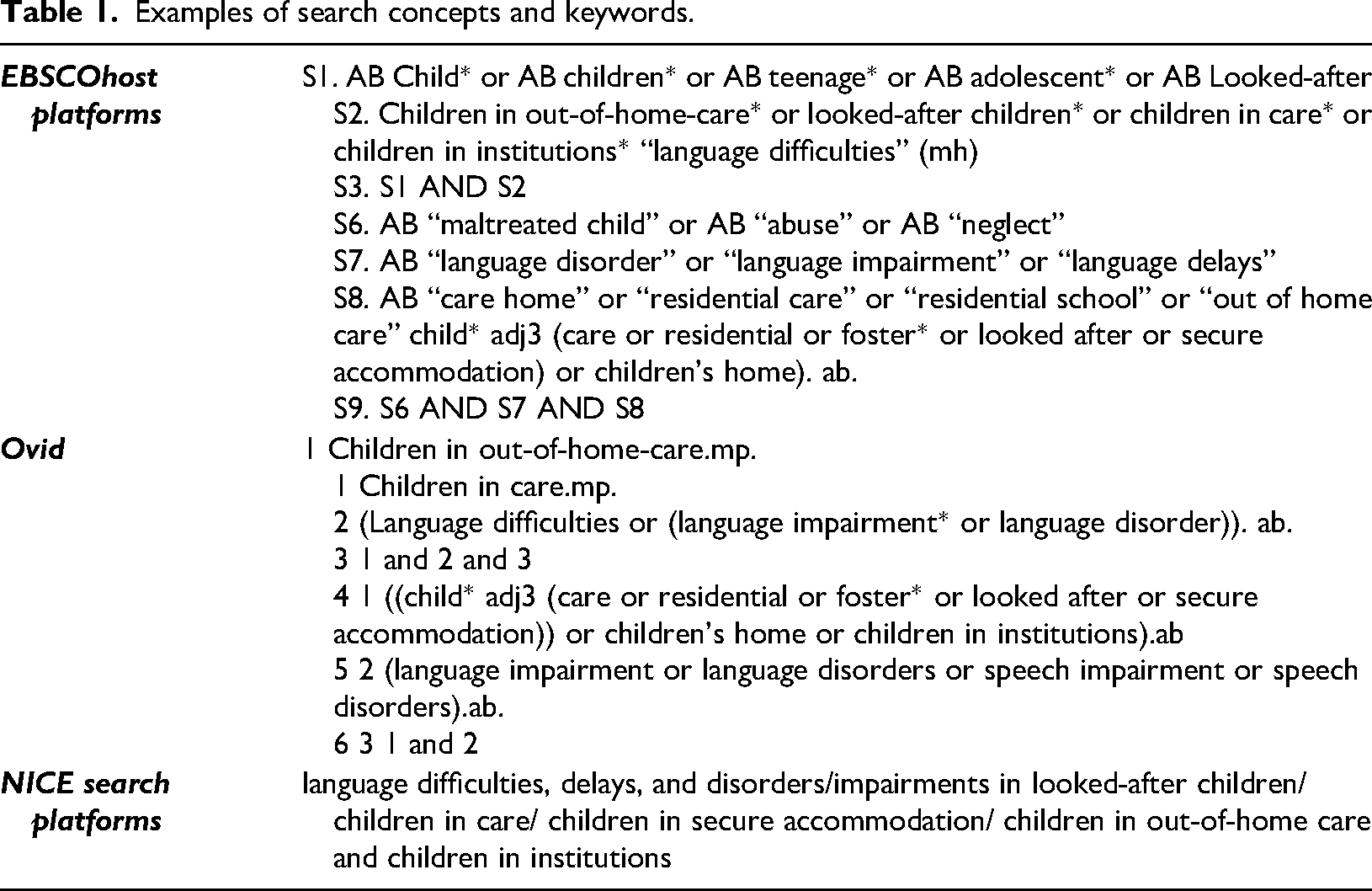
Examples of search concepts and keywords.
The scoping review focused on the period between December 1989 and October 2024 as there was a significant increase in interest in language abilities in children and young people in care, following the adoption of the United Nations Convention on the Rights of the Child in 1989. The included studies were not limited to a specific country or location. A summary of the inclusion criteria is outlined in Table 2.
Summary of inclusion criteria.
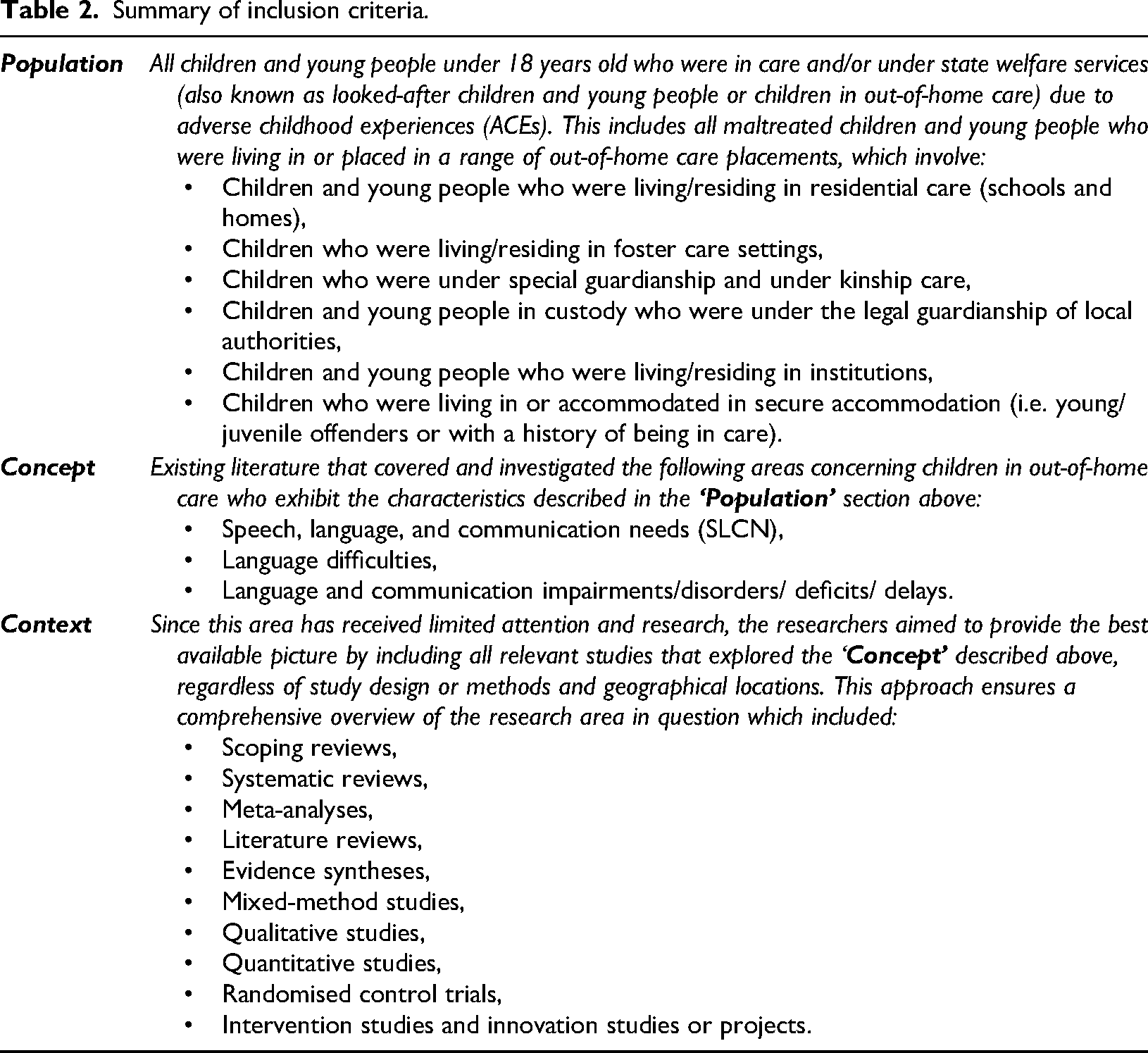
Summary of inclusion criteria.
The study selection process consisted of two phases: (a) title and abstract screening and (b) full-text review. The PRISMA flowchart shows that the three-step search yielded n = 413 records. Following the removal of duplicates (n = 16), n = 397 records remained for screening. Title-abstract and full-text screening led to the exclusion of 359 records that did not meet inclusion criteria. Studies were excluded if they lacked empirical data, did not focus on language development, or were commentaries, editorials, performance reviews, or book chapters without data. Studies involving children not in out-of-home care or published outside the December 1989 to and October 2024 time-frame were also excluded. Further details are provided in Table A1. The use of a two-phase selection process resulted in 38 articles meeting the eligibility criteria and was included in the study. The authors developed draft inclusion criteria based on the research questions. To ensure the reliability of the review findings, two reviewers independently screened 40 of the 397 articles at the title and abstract stage and 35 of the 179 articles at the full-text stage. Kappa statistics were used to assess the inter-rater reliability of the final papers included in the review, and no discrepancies were found (Cohen, 1960). An overview of the study selection process is presented in Figure 1. Note that despite comprehensive search trials, a high number of papers were sourced through reference checking. This is due to the wide range of different, sometimes unique, terms being used in this field of research and will be discussed in following sections.
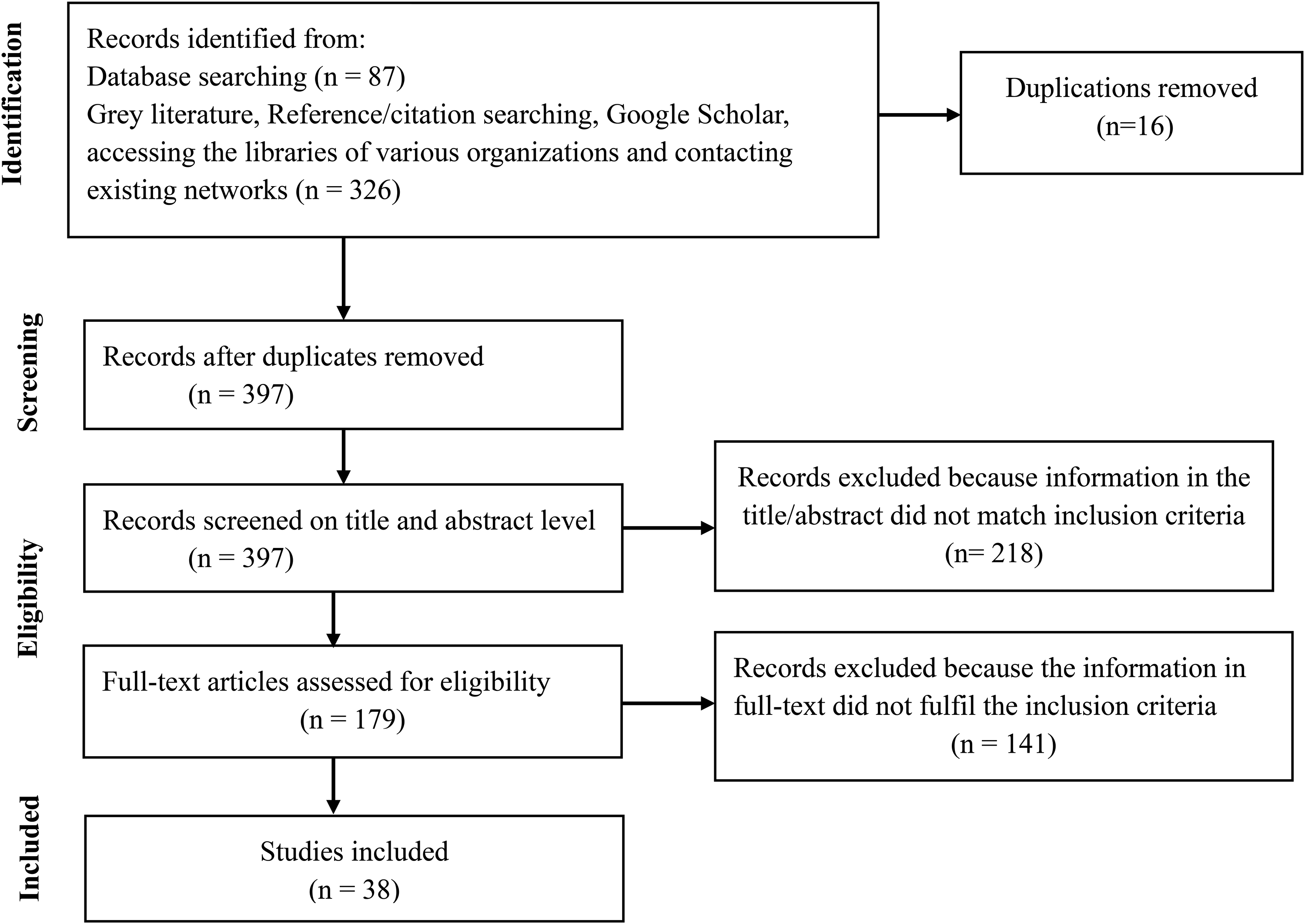
Flow chart of the study selection process.
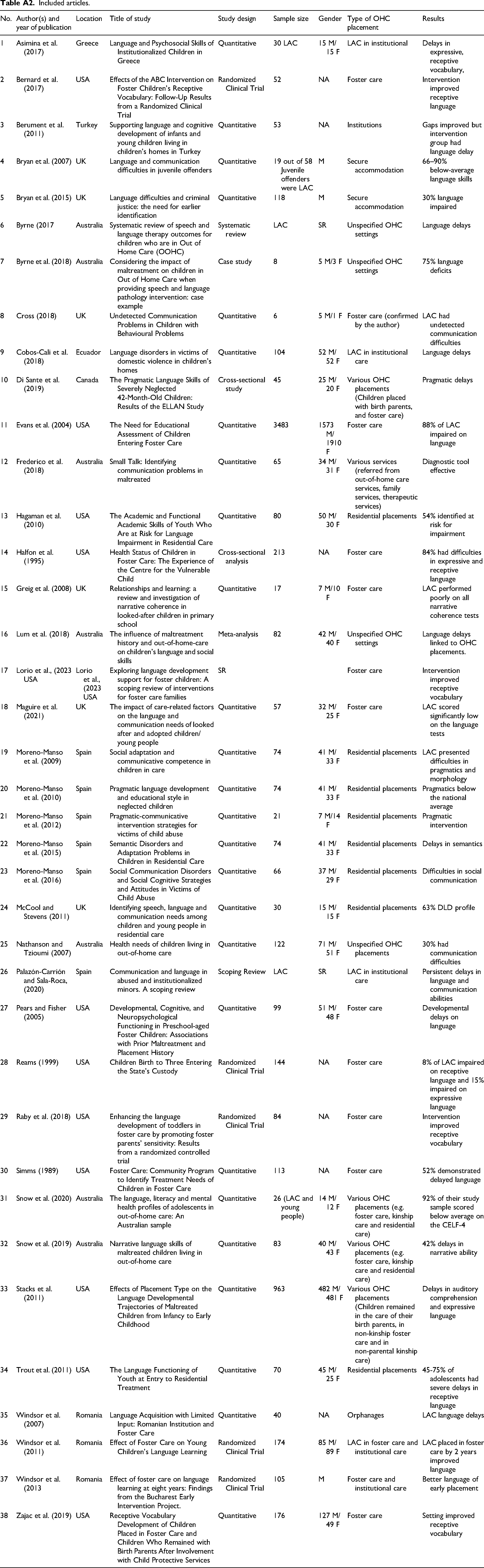
To assist the data extraction process, a data charting table was created to record key information which included: authors, year of publication, country of origin, title of the study, study design, sample size, gender, types of OHC placement and results. An overview of the included studies and key information are recorded systematically in Table A2 of Appendix A.
Results
Scope of the papers
The included studies mostly have not been replicated. The types of language assessments used, varied across the studies with few, and in some cases, a single measure carried out for the language assessment. The age ranges varied from early childhood to later adolescence (i.e. aged 1 month to 18 years), though most studies focused on younger (e.g. ≤12 years) children. Demographic information, including children's gender and age, was clearly outlined in each study. However, some details related to their pre-care histories were missing, for example reasons for entry in care, SEN status, age of first placement and previous diagnosis of language difficulties. The included studies were conducted across 9 countries, and 12 out of the 38 studies were conducted in the USA (Table 3).
Characteristics of included studies (n = 38).
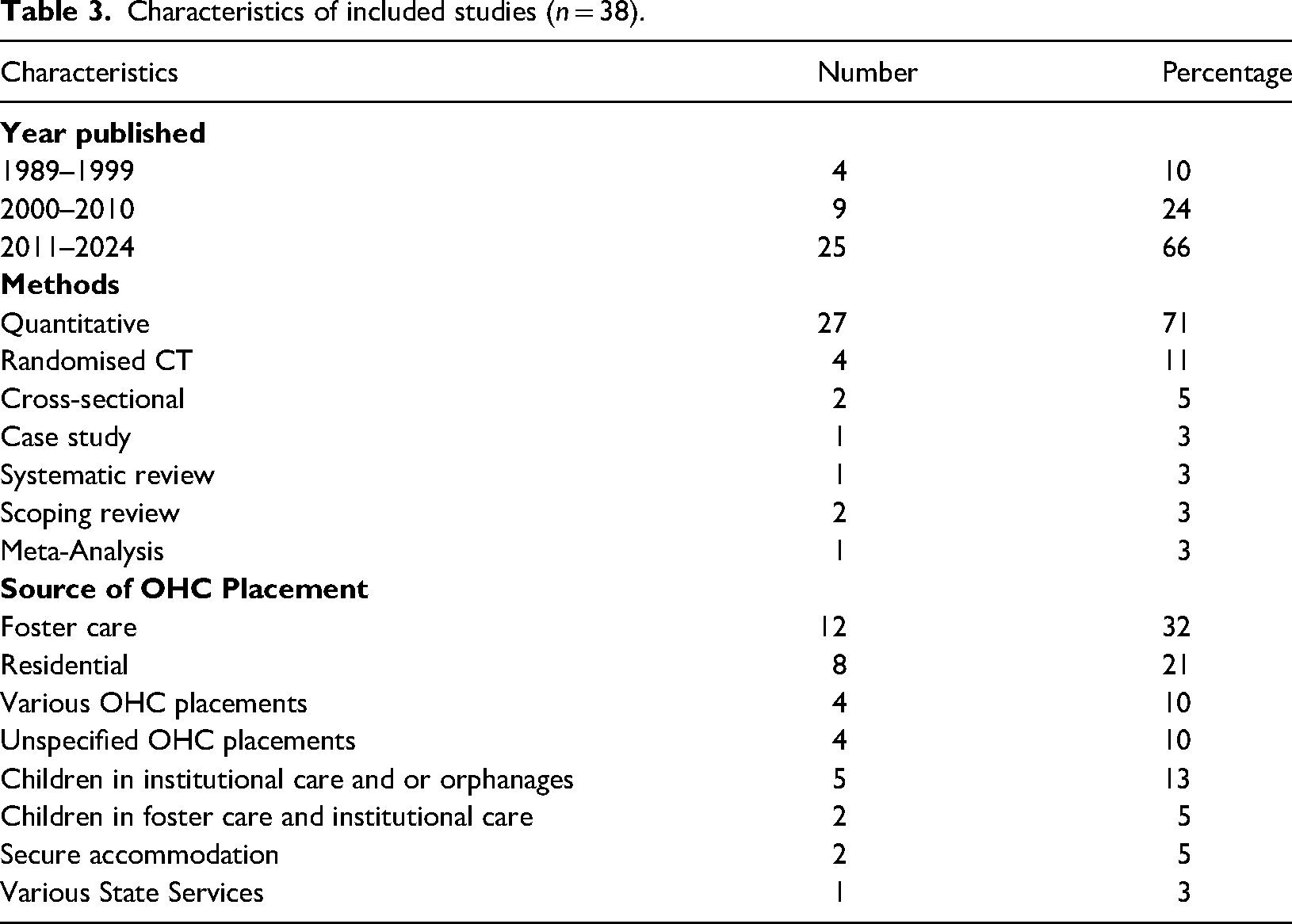
Characteristics of included studies (n = 38).
In addition to the characteristics outlined above, the review yielded four types of papers: (a) studies utilising general health and language development screens (n = 10); (b) studies using standardised language tests and comparison of results with test norms (n = 12); (c) studies that compared children and young people in care with a matched control group (n = 10); and (d) studies investigating interventions aimed at the language needs of this population (n = 6). When addressing each research question, we have described results with reference to each type of study. A more detailed overview of the reviewed articles is presented in Table A2 in Appendix A.
RQ1: What is the rate/prevalence of language difficulties in children and young people in care?
Of the 38 studies reviewed, 10 assessed language skills as part of broader evaluations of general health and development with screening tools. These studies reported that between 30% and 85% of children and young people in care experienced language difficulties. Such difficulties were observed across a range of OHC settings and difficulties were seen in all aspects of language (vocabulary, grammar, etc.), including pragmatics. For instance, Nathanson and Tzioumi (2007) found that 33% of children who had experienced more than one OHC placement demonstrated speech delays. Similarly, Simms (1989) reported that 53% of young children attending a weekly foster care clinic exhibited significant delays in language development, making it the most commonly affected developmental domain on the screening – a result supported by other studies (e.g. Reams, 1999).
The 12 studies that used standardised test measures to compare children in young people in care against normative data, assessed varying aspects of language. Prevalence rates for these papers indicated that between 30% and 92% of children and young people in care experienced what the researchers called language difficulties. For example, Snow et al. (2020) used the CELF-4 (Semel et al., 2003) to assess structural language, and the TLC-E (Wiig and Secord, 2014) to evaluate figurative and idiomatic language in children and young people in care. They found that 92% scored below average on the CELF-4, with TLC-E scores falling one to two standard deviations below the mean. These results were interpreted by the authors as evidence of significant impairments in both structural and idiomatic language among this population. Using other measures, Evans et al. (2004) found that 52% of children demonstrated language underachievement, while McCool and Stevens (2011) identified social communication impairments or broader language needs in 27% to 37% of their sample. In residential care settings, Hagaman et al. (2010) and Trout et al. (2011) reported that 54% and 73% of adolescents, respectively, were at risk of language impairment, particularly in expressive and receptive domains, again using the CELF.
Two papers that compared children in care with peers also reported higher prevalence rates for communication needs: Di Sante et al. (2019) found that neglected children (22 children residing in foster care and 23 living with their biological parents) were 10 times (44%) more likely to experience difficulties in their early pragmatic development compared to their non-neglected peers. Another study based on UK norms indicated that a substantial proportion (68%) of looked-after and adopted children/young people experience language and communication difficulties (Maguire et al., 2021). An explanation offered for these differences was the protective effect of early placement in a permanent home with responsive parents or carers from an early age.
RQ2: What aspects of language development are affected in children and young people in care?
In 4 of the 12 studies conducted by the same research group, difficulties were observed in syntactic, morphological and semantic abilities, with pragmatic language emerging as the most consistently and profoundly affected domain (Moreno-Manso et al., 2009, 2010, 2015, 2016). Two further studies from other groups, reported that children exposed to maltreatment were at heightened risk for both expressive language delays (Stacks et al., 2011) and broader communication difficulties, including difficulties with speech, fluency and non-verbal communication (Frederico et al., 2018). These issues were observed in up to 85% of the sample, compared to peers with similar demographic characteristics who had not experienced maltreatment (Frederico et al., 2018). Other general screening studies highlighted a clear association between their language difficulties and other areas of development, such as academic, social, cognition and emotional difficulties (e.g. Halfon et al., 1995).
Seven of the 12 studies that used standardised tests compared with norms, employed the CELF (Semel et al., 1987), while 7 used alternative standardised measures (Cross, 2018; Bryan et al., 2015; Hagaman et al., 2010; Lum et al., 2018; Snow et al., 2019, 2020; Trout et al., 2011). All studies consistently identified structural language difficulties – including receptive, expressive and narrative skills – among children and young people in care. For instance, multiple studies reported that participants consistently scored below one standard deviation cut-off indicating clinical concern (e.g. Bryan et al., 2007, 2015; Cross, 2018). In one study, 30% of children exhibited structural language delays, and 42% struggled with narrative tasks, suggesting real-world communication difficulties (Snow et al., 2019).
RQ3: What protective and risk factors for language difficulties are connected to OHC settings or the ACEs leading to being taken into care?
Several studies emphasised that children and young people residing in various OHC settings are at a heightened risk of experiencing language difficulties. Notably, 9 of the 38 studies reviewed, highlighted the complex interplay of contributing factors (e.g. inadequate OHC environments) that exacerbate these difficulties. In contrast, one of the studies proposed that early exposure to foster care could be a protective factor for children's language skills; this included maltreated children placed in foster care compared to those who remained with their birth families (e.g. Byrne et al., 2018).
The 10 studies in this review that compared the language development of children in care with age- and SES-matched groups revealed that delays in receptive, expressive, and social-pragmatic language skills were often associated with early adversity. For example, the Bucharest Early Intervention Project (Windsor et al., 2007, 2011, 2013) found that children placed in foster care before 24 months developed language skills comparable to their non-institutionalised peers, whereas those placed later exhibited persistent delays. This finding is supported by 3 studies, which reported language delays among institutionalised children (e.g. Asimina et al., 2017; Berument et al., 2011; Cobos-Cali et al., 2018). Pears and Fisher (2005) reported lower language scores among maltreated children in foster care compared to matched peers, with a negative correlation between the severity of maltreatment and language ability – contrasting with the findings of (Byrne et al., 2018). Similarly, Greig et al. (2008) attributed weaker narrative skills among children in care to disrupted attachment and trauma. Furthermore, a scoping review of studies on maltreated institutionalised children revealed that persistent delays in their language and communication skills often remain unidentified or unrecognised (Palazón-Carrión and Sala-Roca, 2020).
RQ4: What are the types of intervention strategies used to support language difficulties in children and young people in care?
A total of 6 out of the 38 published papers focused on intervention strategies and methods used to support the language development of children and young people in care. One of the papers was a systematic review of 45 intervention studies (Byrne et al., 2018), while another was a recent scoping review involving 24 studies that examined intervention strategies in foster families (Lorio et al., 2022). Both reviews concluded that only a few studies focus specifically on strategies for promoting children's language development. Among the limited number of studies, two suggested that interventions aimed at enhancing parent–child interactions (e.g. Attachment and Biobehavioural Catch-up for Toddlers (ABC-T); Dozier and Bernard, 2017) can positively influence broader aspects of children's language development, particularly in relation to receptive language abilities (e.g. Bernard et al., 2017; Raby et al., 2018). One study reported the positive effects of intervention in foster care placements on children and young people's language skills (e.g. Byrne et al., 2018) while one study reported notable improvements in children's pragmatic skills following the implementation of a pragmatic-communicative intervention programme (Moreno-Manso et al., 2012).
Across the 38 studies reviewed, children and young people in care are described as having over-representative levels of language difficulties. These delays occur in all areas of language development and from comparisons using standardised assessments these delays are diagnosed as constituting a developmental language disorder (DLD; e.g. Evans et al., 2004; McCool and Stevens, 2011). Several other studies did not suggest this diagnosis, despite children and young people in care having scores beyond clinical cut-off levels (e.g. Cross, 2018; Greig et al., 2008; Windsor et al., 2007).
Systematic comparisons of language development across different OHC settings remain scarce. Early placement in foster care and the presence of supportive families appear to serve as protective factors, whereas institutional and custodial settings may increase risk. Additionally, maltreatment has been identified as a significant risk factor for language difficulties. These findings are discussed in further detail below.
RQ1: What is the reported prevalence of language difficulties among children and young people in care?
This scoping review found that 30% to 92% of children and young people in care exhibited language difficulties, highlighting their elevated risk compared to age-matched peers. Across studies, children in care consistently demonstrated delays in expressive, receptive, and pragmatic language skills. These findings align with studies reporting high rates of language difficulties among other at-risk groups (40–56%), including those from socially disadvantaged and deprived backgrounds (e.g. Law et al., 2011; Locke et al., 2002). The high levels of language difficulties reported in the scoping review for children in care can be attributed to the cumulative impact of ACEs, which are prevalent among this population.
ACEs commonly include maltreatment, traumatic events, and disrupted caregiving relationships, both prior to and during placement in care (e.g. Lorio et al., 2022; Maguire et al., 2021). Such experiences often involve negative parent–child interactions (Raby et al., 2018), separation from birth parents, frequent placement changes (Maguire et al., 2021), and adjustment to unfamiliar environments with new carers such as foster or residential placements (Trout et al., 2011; Lorio et al., 2022). Language development is critically shaped by early interactions with responsive caregivers and within stable attachment relationships (Maguire et al., 2021). When these are absent or inconsistent, as is frequently the case for children in care, the development of receptive and expressive language skills can be disrupted (e.g. Pears and Fisher, 2005; Stock and Fisher, 2006). The quality and quantity of language input in child–caregiver interactions, along with the availability of age-appropriate learning materials in both the home and OHC settings, are essential for fostering language development (e.g. Byrne et al., 2018; Hart and Risley, 1995; Raby et al., 2018). Children in care often lack access to such enriching experiences. Studies comparing maltreated children in foster care with those living in more stable environments (Bernard et al., 2017; Byrne et at al., 2018; Moreno-Manso et al., 2010; Raby et al., 2018) highlight the negative impact of ACEs on language development. These early disruptions not only hinder immediate communication skills but also increase the risk of persistent language difficulties extending into adolescence. A recent study confirmed that, without early and effective intervention, language problems in this population often endure or worsen during adolescence and beyond (Clegg et al., 2021).
RQ2: Which specific areas of language development are most frequently affected?
The review highlights that children and young people in care, much like those with DLD and other at-risk groups, experience difficulties across all areas of language, social pragmatics and extended uses of language in school. Studies consistently reported that children in care have an average performance at below age expectations on a range of language measures. These included expressive and receptive skills, including semantic and morphosyntactic abilities. This equates to delays in understanding grammatical and word relationships, as well as higher abstract concepts (Byrne et al., 2018; Cobos-Cali et al., 2018; Eigsti and Cicchetti, 2004; Maguire et al., 2021; Moreno-Manso et al., 2009; Stacks et al., 2011). Trout et al. (2011) and, Moreno-Manso et al. (2009) identified difficulties in word meaning, syntax and morphology, with prevalence rates ranging from 23% to 73%. Asimina et al. (2017) and Eigsti and Cicchetti (2004) documented delays in vocabulary development and difficulties in producing syntactically accurate sentences. These lead to difficulties with everyday communication and learning the foundational skills of academic success such as written language (Eigsti and Cicchetti, 2004; Palazón-Carrión and Sala-Roca, 2020; Snow et al., 2020).
The review also confirms widespread social pragmatic difficulties within this population (e.g. Di Sante et al., 2019; Snow et al., 2019). Social pragmatic difficulties in this group include various domains, including interpreting others’ intentions, initiating and maintaining conversations, taking turns, seeking clarification, and adapting communication to suit different social contexts (e.g. Moreno-Manso et al., 2009; Snow et al., 2019). As with their language skills, this population's social pragmatic delays are explained by authors of the studies to be shaped by their ACEs, distressing life circumstances, social disadvantages and the complexities of growing up within care systems (e.g. Coster et al., 1989; Sylvestre et al., 2016). Language is fundamental to emotional regulation and social competence (Palazón-Carrión and Sala-Roca, 2020; Stacks et al., 2011). However, children exposed to ACEs often miss out on critical relational interactions, hindering their ability to develop essential social-pragmatic skills such as turn-taking, topic maintenance, and adapting language to different contexts (Lum et al., 2018; Sylvestre et al., 2016). Traumatic life experiences may impair their ability to engage in reciprocal exchanges by affecting trust, emotional regulation, and the interpretation of social cues (Lanais et al., 2024; Maguire et al., 2021). Exposure to a wide range of language registers is also likely to be limited, as caregivers may be emotionally unavailable, inconsistent, or preoccupied with their own stress, thereby reducing opportunities for rich, responsive dialogue (Culp et al., 1991; Eigsti and Cicchetti, 2004; Sylvestre et al., 2016). Furthermore, caregivers themselves affected by trauma or mental health difficulties may struggle to adjust their communication to the child's developmental level, making it more difficult for children to practise key social language skills (Eigsti and Cicchetti, 2004; Lorio et al., 2022). These cumulative disruptions can have long-term consequences for pragmatic competence. Some caution is needed, however, in interpreting results from the standardised test measures and normative statistical cut-off criteria. The unique life experiences of this population, particularly their exposure to ACEs such as abuse, neglect and trauma, introduce qualitative differences that may not align with samples of children with normative or non-care experience (e.g. Norbury et al., 2016). These contextual factors should be considered when evaluating and supporting language development in children in care.
RQ3: What risk and protective factors are associated with language difficulties in this population, including those linked to care experiences and adverse childhood experiences (ACEs)?
This review highlights a consistent pattern of delayed language development among children in OHC, particularly those in institutional settings (e.g. Windsor et al., 2007, 2011). Understanding the causes of elevated language difficulties is critical for informing prevention and intervention strategies tailored to the complex needs of children in care. Notably, some evidence suggests that family-like placements, such as foster care, may serve as a protective factor in children's language development (e.g. Healey and Fisher, 2011; Jones et al., 2011), as being in care can sometimes offer a positive alternative to an abusive home environment (Biehal et al., 2014; Coman and Devaney, 2011). Consistent with these findings, early placement in foster care has been shown to act as a protective factor, even for children with a history of maltreatment (Byrne et al., 2018; Windsor et al., 2011). However, a more nuanced understanding of foster care is needed. This review identified a negative association between age at placement and language ability: children placed at older ages were more likely to experience language delays (e.g. Windsor et al., 2011, 2013). This highlights the importance of early and stable placements in supporting optimal developmental outcomes. Early placement aligns with sensitive periods in brain development, enabling children to benefit from developmental plasticity – the brain's ability to adapt and reorganise in response to enriched environmental input (Lanais et al., 2024; Loiro et al., 2022). By reducing exposure to ACEs and increasing access to nurturing, developmentally rich experiences, early and stable placements can serve as a protective factor. Environmental factors such as inconsistent caregiving, overcrowding, and understaffing may compromise the provision of responsive interactions (Bakermans-Kranenburg et al., 2011), which are essential for meeting children's physical, emotional, and social needs (e.g. Halfon et al., 1995; Eigsti and Cicchetti, 2004; Pears and Fisher). The advantage of early foster care likely stems from timely exposure to a responsive, family-like caregiving environment and enriched language input, both of which can foster secure attachments and cognitive growth (Asmussen et al., 2018; Lanais et al., 2024; Loiro et al., 2022). In contrast, delayed placement or prolonged institutionalisation often results in reduced access to these enriching experiences, increasing the likelihood of language difficulties (e.g. Windsor et al., 2011, 2013). Although improvements have been observed following foster placement, variability in children's ages and the unique circumstances under which children enter in care, make it challenging to generalise outcomes across different OHC environments.
The second part of this research question considered the various ACEs on this population's language development. Children are often placed in care when they can no longer live with their birth parents, due to range of factors, for example maltreatment (DfE, 2022; Jones et al., 2011). This complexity makes it challenging to disentangle the effects on a child's overall development from the effects on their language growth, with respect to these circumstances (e.g. Eigsti and Cicchetti, 2004). Nonetheless, our scoping review findings indicated that maltreatment, in particular neglect and abuse, significantly impacts this population's language abilities, including social pragmatics.
RQ4: What are the types of intervention strategies used to support language difficulties in children and young people in care?
The results of this scoping review reveal a significant gap in research on strategies specifically designed to promote language development in children and young people in care. Some interventions, particularly those involving foster parent–child interactions, demonstrate potential to positively influence language outcomes. A number of studies have revealed that early identification of language difficulties, followed by timely intervention, can offer significant benefits, potentially preventing or reducing associated difficulties (Bryan et al., 2015; Raby et al., 2018; Snow et al., 2020). For instance, studies by Bernard et al. (2017) and Raby et al. (2018) suggested that the use of the ABC-T intervention led to improvements in the receptive vocabulary abilities of preschool-aged children placed in foster care, while other studies highlighted the benefits of foster care placements more broadly (e.g. Byrne et al., 2018). However, the lack of targeted research on effective intervention methods for this group highlights the need for further investigation. Given their elevated risk for language delays, developing evidence-based language interventions at the clinical level is essential (Lorio et al., 2022). Furthermore, the absence of comprehensive intervention strategies limits SLTs’ capacity to provide effective, responsive care which is aligned with the complex needs of children and young people in care. This gap continues to disadvantage this population, restricting their access to language support that meets their specific developmental needs (Byrne, 2017).
Limitations
The studies included in this systematic review contained several limitations and variability across papers make it difficult to understand their findings completly. The studies vary in their assessment methods, sample populations, research aims, and the specific aspects of language difficulties they address. Additionally, it is far from consistent what researchers label as language difficulties and/or impairment. Studies use ‘delay’, ‘disorder’, ‘poor’ or ‘low’ language skills interchangeably. Also, the variability in how language is tested, combined with the lack of replicated studies, further complicates the findings. While some researchers rely on single tests, others use broader health and education assessments. These inconsistencies may have affected the results, which makes a comprehensive understanding of language difficulties in children in care more difficult to achieve. Future research and practice should prioritise the use of standardised language measures, and more complete records of the children’s environment and history to more accurately identify language difficulties in this population. A wider issue is that there are some challenges in defining search terms in research on LAC. General terms like ‘care’ are widely used across different contexts and disciplines. Moreover, the variability in terminology across publications posed challenges for a comprehensive search. As a result, despite rigorous efforts, a substantial number of relevant studies were identified through grey literature and reference checking, reflecting the diverse and often inconsistent language used within this field.
Implications for wider practice
This review addressed a set of research questions with the potential to significantly impact practice, policy, and language outcomes for children and young people in care. It highlights that language assessments and interventions for this population are often overlooked (e.g. Bryan et al., 2015; Frederico et al., 2018; Hagaman et al., 2010). It summarises the prevalence of language difficulties, the most affected areas of language development, and the lack of tailored intervention strategies for this group, which. Study provides several insights for both clinicians and policymakers. These findings emphasised the importance of equipping professionals with the tools to address the complex language needs of this population, thereby improving their long-term outcomes. Additionally, by exploring risk and protective factors, the review provides valuable pointers for policymakers to design targeted, trauma-informed, and developmentally appropriate interventions. Future research and practice should prioritise the use of standardised language measures to more accurately identify language difficulties in this population.
Summary and future directions
This systematic scoping review analysed 38 studies on language difficulties among children in care. The results highlight the heightened vulnerability of children in care to language-related difficulties, including pragmatics. It raises the urgent need for specialised support and intervention strategies. Further research is needed to better understand the risk and protective factors contributing to language difficulties in children in care, as well as those leading to positive outcomes.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Appendix A. List of tables
Included articles.
| No. | Author(s) and year of publication | Location | Title of study | Study design | Sample size | Gender | Type of OHC placement | Results |
|---|---|---|---|---|---|---|---|---|
| 1 | Asimina et al. (2017) | Greece | Language and Psychosocial Skills of Institutionalized Children in Greece | Quantitative | 30 LAC | 15 M/15 F | LAC in institutional | Delays in expressive, receptive vocabulary, |
| 2 | Bernard et al. (2017) | USA | Effects of the ABC Intervention on Foster Children's Receptive Vocabulary: Follow-Up Results from a Randomized Clinical Trial | Randomized Clinical Trial | 52 | NA | Foster care | Intervention improved receptive language |
| 3 | Berument et al. (2011) | Turkey | Supporting language and cognitive development of infants and young children living in children's homes in Turkey | Quantitative | 53 | NA | Institutions | Gaps improved but intervention group had language delay |
| 4 | Bryan et al. (2007) | UK | Language and communication difficulties in juvenile offenders | Quantitative | 19 out of 58 Juvenile offenders were LAC | M | Secure accommodation | 66–90% below-average language skills |
| 5 | Bryan et al. (2015) | UK | Language difficulties and criminal justice: the need for earlier identification | Quantitative | 118 | M | Secure accommodation | 30% language impaired |
| 6 | Byrne (2017 | Australia | Systematic review of speech and language therapy outcomes for children who are in Out of Home Care (OOHC) | Systematic review | LAC | SR | Unspecified OHC settings | Language delays |
| 7 | Byrne et al. (2018) | Australia | Considering the impact of maltreatment on children in Out of Home Care when providing speech and language pathology intervention: case example | Case study | 8 | 5 M/3 F | Unspecified OHC settings | 75% language deficits |
| 8 | Cross (2018) | UK | Undetected Communication Problems in Children with Behavioural Problems | Quantitative | 6 | 5 M/1 F | Foster care (confirmed by the author) | LAC had undetected communication difficulties |
| 9 | Cobos-Cali et al. (2018) | Ecuador | Language disorders in victims of domestic violence in children's homes | Quantitative | 104 | 52 M/52 F | LAC in institutional care | Language delays |
| 10 | Di Sante et al. (2019) | Canada | The Pragmatic Language Skills of Severely Neglected 42-Month-Old Children: Results of the ELLAN Study | Cross-sectional study | 45 | 25 M/20 F | Various OHC placements (Children placed with birth parents, and foster care) | Pragmatic delays |
| 11 | Evans et al. (2004) | USA | The Need for Educational Assessment of Children Entering Foster Care | Quantitative | 3483 | 1573 M/1910 F | Foster care | 88% of LAC impaired on language |
| 12 | Frederico et al. (2018) | Australia | Small Talk: Identifying communication problems in maltreated | Quantitative | 65 | 34 M/31 F | Various services (referred from out-of-home care services, family services, therapeutic services) | Diagnostic tool effective |
| 13 | Hagaman et al. (2010) | USA | The Academic and Functional Academic Skills of Youth Who Are at Risk for Language Impairment in Residential Care | Quantitative | 80 | 50 M/30 F | Residential placements | 54% identified at risk for impairment |
| 14 | Halfon et al. (1995) | USA | Health Status of Children in Foster Care: The Experience of the Centre for the Vulnerable Child | Cross-sectional analysis | 213 | NA | Foster care | 84% had difficulties in expressive and receptive language |
| 15 | Greig et al. (2008) | UK | Relationships and learning: a review and investigation of narrative coherence in looked-after children in primary school | Quantitative | 17 | 7 M/10 F | Foster care | LAC performed poorly on all narrative coherence tests |
| 16 | Lum et al. (2018) | Australia | The influence of maltreatment history and out-of-home-care on children's language and social skills | Meta-analysis | 82 | 42 M/40 F | Unspecified OHC settings | Language delays linked to OHC placements. |
| 17 | Lorio et al., (2023 USA | Lorio et al., (2023 USA | Exploring language development support for foster children: A scoping review of interventions for foster care families | SR | Foster care | Intervention improved receptive vocabulary | ||
| 18 | Maguire et al. (2021) | UK | The impact of care-related factors on the language and communication needs of looked after and adopted children/young people | Quantitative | 57 | 32 M/25 F | Foster care | LAC scored significantly low on the language tests |
| 19 | Moreno-Manso et al. (2009) | Spain | Social adaptation and communicative competence in children in care | Quantitative | 74 | 41 M/33 F | Residential placements | LAC presented difficulties in pragmatics and morphology |
| 20 | Moreno-Manso et al. (2010) | Spain | Pragmatic language development and educational style in neglected children | Quantitative | 74 | 41 M/33 F | Residential placements | Pragmatics below the national average |
| 21 | Moreno-Manso et al. (2012) | Spain | Pragmatic-communicative intervention strategies for victims of child abuse | Quantitative | 21 | 7 M/14 F | Residential placements | Pragmatic intervention |
| 22 | Moreno-Manso et al. (2015) | Spain | Semantic Disorders and Adaptation Problems in Children in Residential Care | Quantitative | 74 | 41 M/33 F | Residential placements | Delays in semantics |
| 23 | Moreno-Manso et al. (2016) | Spain | Social Communication Disorders and Social Cognitive Strategies and Attitudes in Victims of Child Abuse | Quantitative | 66 | 37 M/29 F | Residential placements | Difficulties in social communication |
| 24 | McCool and Stevens (2011) | UK | Identifying speech, language and communication needs among children and young people in residential care | Quantitative | 30 | 15 M/15 F | Residential placements | 63% DLD profile |
| 25 | Nathanson and Tzioumi (2007) | Australia | Health needs of children living in out-of-home care | Quantitative | 122 | 71 M/51 F | Unspecified OHC placements | 30% had communication difficulties |
| 26 | Palazón-Carrión and Sala-Roca, (2020) | Spain | Communication and language in abused and institutionalized minors. A scoping review | Scoping Review | LAC | SR | LAC in institutional care | Persistent delays in language and communication abilities |
| 27 | Pears and Fisher (2005) | USA | Developmental, Cognitive, and Neuropsychological Functioning in Preschool-aged Foster Children: Associations with Prior Maltreatment and Placement History | Quantitative | 99 | 51 M/48 F | Foster care | Developmental delays on language |
| 28 | Reams (1999) | USA | Children Birth to Three Entering the State's Custody | Randomized Clinical Trial | 144 | NA | Foster care | 8% of LAC impaired on receptive language and 15% impaired on expressive language |
| 29 | Raby et al. (2018) | USA | Enhancing the language development of toddlers in foster care by promoting foster parents’ sensitivity: Results from a randomized controlled trial | Randomized Clinical Trial | 84 | NA | Foster care | Intervention improved receptive vocabulary |
| 30 | Simms (1989) | USA | Foster Care: Community Program to Identify Treatment Needs of Children in Foster Care | Quantitative | 113 | NA | Foster care | 52% demonstrated delayed language |
| 31 | Snow et al. (2020) | Australia | The language, literacy and mental health profiles of adolescents in out-of-home care: An Australian sample | Quantitative | 26 (LAC and young people) | 14 M/12 F | Various OHC placements (e.g. foster care, kinship care and residential care) | 92% of their study sample scored below average on the CELF-4 |
| 32 | Snow et al. (2019) | Australia | Narrative language skills of maltreated children living in out-of-home care | Quantitative | 83 | 40 M/43 F | Various OHC placements (e.g. foster care, kinship care and residential care) | 42% delays in narrative ability |
| 33 | Stacks et al. (2011) | USA | Effects of Placement Type on the Language Developmental Trajectories of Maltreated Children from Infancy to Early Childhood | Quantitative | 963 | 482 M/481 F | Various OHC placements (Children remained in the care of their birth parents, in non-kinship foster care and in non-parental kinship care) | Delays in auditory comprehension and expressive language |
| 34 | Trout et al. (2011) | USA | The Language Functioning of Youth at Entry to Residential Treatment | Quantitative | 70 | 45 M/25 F | Residential placements | 45-75% of adolescents had severe delays in receptive language |
| 35 | Windsor et al. (2007) | Romania | Language Acquisition with Limited Input: Romanian Institution and Foster Care | Quantitative | 40 | NA | Orphanages | LAC language delays |
| 36 | Windsor et al. (2011) | Romania | Effect of Foster Care on Young Children's Language Learning | Randomized Clinical Trial | 174 | 85 M/89 F | LAC in foster care and institutional care | LAC placed in foster care by 2 years improved language |
| 37 | Windsor et al. (2013 | Romania | Effect of foster care on language learning at eight years: Findings from the Bucharest Early Intervention Project. | Randomized Clinical Trial | 105 | M | Foster care and institutional care | Better language of early placement |
| 38 | Zajac et al. (2019) | USA | Receptive Vocabulary Development of Children Placed in Foster Care and Children Who Remained with Birth Parents After Involvement with Child Protective Services | Quantitative | 176 | 127 M/49 F | Foster care | Setting improved receptive vocabulary |