
Abstract
In September 2024, a workshop was held, during the EADPH conference in Crete. It aimed to explore what constitutes essential oral healthcare and what are the challenges and solutions in adopting Universal Health Coverage (UHC). It also aimed to raise awareness of the need for oral health to be included in (UHC). The workshop was informed by presentations from five speakers. The attendees then divided into four break-out groups that discussed the topics of,: (1) Which oral health services and which population groups should be publicly funded ? (2) What are the most frequently demanded oral health services at your practice/in your region? (3) What are the most frequently provided services at your practice/in your region? (4) Which of these services are publicly covered and for whom? (5) What are the barriers and enablers for reaching universal health coverage? Each group then considered enablers and challenges to achieving the inclusion of oral health care in UHC and reported their findings and discussions in a plenary session,. during which the implications were discussed. The commentary, which follows, reports the proceedings of the workshop and discusses the implications of its findings.
Summary of the speakers presentations
Globally, oral health conditions and diseases pose a significant burden on populations, health services and wider society. Treatment of oral diseases and conditions is costly, has impacts on oral health quality of life and can result in limited economic productivity, as well as out of pocket payments.
The first speaker, Dr Vujicic, (Senior Economist from the World Economic Forum (WEF), summarised and referenced “ the Economic Rationale for Global Commitment to Invest in Oral Health” report (WEF, 2024). This holistic approach perceives oral health as being critical to overall health and general well-being and oral health is a key driver of economic wellbeing of individuals and populations. The burden of oral diseases is significant globally and amounted to $710 billion in 2019 (Jevdjevic and Listl, 2025). Poor oral health can impact education and academic attainment and employment opportunities. The WEF report, emphasised that productivity losses due to dental conditions surpass those associated with other non-communicable diseases. This burden is more apparent in disadvantaged populations, widening and exacerbating the gaps in oral health inequalities. Therefore, healthcare systems need to adapt and address these challenges. There is no magic solution, but it is necessary to consider the social and commercial determinants of oral health alongside dental care systems that are funded appropriately, driving innovative workforce models with a focus on primary care and integration of oral health into UHC. To achieve the best oral health outcomes. The launch of the WHO Global Oral Health Action Plan for Oral Health has brought oral health into the limelight in the context of the wider Non-Communicable Diseases (NCD) agenda (WHO, 2024). One of the targets is for 70% of the population to have access to UHC by 2030. This ambitious target hopes to gain momentum, and it is important for clinicians, policy makers, and academics to explore what barriers may be posed and what potential solutions can be adopted to advance this agenda.
The workshop then considered the definitions of essential oral health care and the current situation in a variety of regions across Europe. Dr Syngelakis (Chief Dental Officer (CDO) of Greece, explored the South European Region giving examples from Italy, Spain and Greece. Italy provides dental services through a mixed system that includes both public and private sectors, with the private sector being the dominant provider of dental care. It was evident that the Italian National Health Service provided free or subsidised care for children 0–14 year olds and vulnerable populations including those on low-income, people with disabilities and those in need of urgent dental care. However, it was also noted that the majority of the population relied on private dental care with a significant amount of out of pocket payments. Similarly, Spain has a mixed public health system provided through the Spanish National Health System (SNS) and this mainly covers basic and emergency dental care and includes children (up to the of 16 years), and people who are medically compromised. The provision can vary in the 17 autonomous provinces. The majority of adults have to pay for their dental care either through insurance systems or directly to providers. On the other hand, the Greek public healthcare system offers limited dental services, focusing mainly on children (delivering prevention, fluoride varnish and fissure sealant applications and emergency dental care). Typically, adults have to pay out-of-pocket for most treatments, even if they are insured under the public system.
Exploring Eastern Europe, Professor Oancea (Head of Department of Preventive Dentistry and Community Dental Health, Victor Babes University of Medicine and Pharmacy, Timisoara, Romania) explained dental service provision in Romania, the majority is provided in the private sector. There is the Romanian Public Health System that provides care for children, veterans and patients with medical needs.
The view from England demonstrated that it had a mixed health care system. The National Health Service provided dental care for all age groups mixed with private dentistry. Patients who are under the age of 19 years and in full time education, pregnant women and those on government benefits were entitled to free dental care. However, there were challenges in financing dental care and in the dental workforce.
Dr Vassallo (Director Health Promotion and Disease Prevention) described the dental services in Malta, which operate under a dual public-private system. However, Malta has a few distinctions due to its small size and focuses on ensuring there is little unmet need. Public dental care is provided at the dental departments of the two main hospitals, free at the point of access and includes emergency and basic routine care alongside prevention for all the population. It is planned to also provide dental services in a new regional health hub in the south of the island. Children, up to 16 years of age, benefit from comprehensive dental services including restorative and orthodontic treatment under the public system (prevention, fluoride applications and restorative and orthodontic treatment). Adults who have been means tested and diabetic patients are also eligible for comprehensive dental care (including restorative treatment and dentures). All other dental care is subject to out of pocket fees, which can be covered by voluntary health insurance schemes.
Professor Tubert-Jeannin (Professor of Dental Public Health, University of Clermont Auvergne, France) explored the French system which is a comprehensive and accessible dental care system. The health financing system is based on social health insurance (SHI) for all legal residents. Dentists mainly work independently in private offices. For primary dental care and prevention, dentists receive fee-for-service payments according to a list of defined prices for which SHI ensures 60% coverage. As a complement, people (95% of the population) contract private voluntary health insurance (VHI) covering the remaining 40% of costs. An additional public insurance scheme (“CSS”) is offered to people with an annual income lower than a ceiling of resources with 100% coverage of dental care fees. In 2019, a reform known as “100% santé” was implemented, aimed at reducing Out of Pocket Payments on prosthetic treatments through better VHI coverage.
In summary, there were no agreed definitions of essential oral healthcare. Several countries defined this differently and therefore there was no agreed consensus on this concept.
The presentations were then followed by breakout groups to explore the following:
There were varying approaches to this question. Suggested criteria included: • Age-based coverage: children and adolescents and older people should be prioritised • Maternal Care: Pregnant and nursing mothers • Vulnerable populations: (a) Medical vulnerability: patients who are medically compromised with co-morbidities, physical and learning disabilities and oncology patients. (b) Socio-economic disadvantaged patients: Those who are facing socio-economic hardship or social marginalisation.
In terms of clinical care, the services most often identified for public coverage included: • Urgent dental care • Oral health assessments • Preventive care
There was consensus among the different groups that urgent dental care: pain, sepsis and swellings, and dental traumatic injuries were the most prevalent conditions patients sought care for. This was followed by restorative care, aesthetic dentistry and implants. It was noted that patients did not normally demand prevention services preferring curative treatment over prevention.
This was largely dependent on whether dental care is provided through the public or private sector, as well as the availability and distribution of the dental workforce. The majority of dental services that were publicly funded provided urgent dental care, mostly commonly extractions and fillings. Public funded services also provided treatment for specific patient groups including children and young people and those who may be medically compromised or have learning or physical disabilities. Therefore, there wasn’t universal coverage of the whole population.
Where there was availability of private dental services and in those regions with a higher concentration of dental professionals, it was perceived more likely that invasive and complex procedures were more commonly provided.
Core clinical services provided in the private sector frequently include restorative treatments, particularly dental fillings and tooth extractions, alongside root canal therapy (RCT). Dental implants are also increasingly common. However, their availability is largely influenced by country-specific healthcare policies and the balance between public and private sector provision. Funding and provision of orthodontic provision varied, and, in some countries, there was partial or full public coverage and it depended on a number of factors including the funding systems, patient’s age (adults are rarely covered), and orthodontic needs of the patient. For example, in France the public health insurance system partially re-imburses orthodontic care for children under the age of 16 years. In Italy and Spain, children are only covered if they have a serious malocclusion, which is impacting on function and aesthetics. In the UK, this depends on screening patients based on the Index of Orthodontic Treatment Need (IOTN) to assess patients under the age of 16 years.
Similarly, the provision of aesthetic dental procedures (such as tooth whitening or veneers) tends to be more prevalent in the private sector, where demand is driven by patient preferences and the ability to pay out-of-pocket, rather than clinical necessity.
Coverage of different treatment types and population groups varied significantly by region and countries. This suggests differences in national oral health policies and priorities. However, most countries covered dental examinations, radiographs and extractions, reflecting a focus of service being on the provision of urgent dental care.
France provided the most comprehensive coverage under the combination of Social Health Insurance and Voluntary Health Insurance systems, with many oral health services, that are broadly covered for the general population. In contrast, Hungary provided dental examinations, radiographs, and extractions under the public health system and any more complex procedures requires private payment from patients. Belgium operates under a universal coverage model, though certain services may be limited by age eligibility. In Germany, coverage is primarily focused on vulnerable populations, including individuals with low incomes or chronic health conditions. In the UK, all dental services (except implants and aesthetic dentistry) can be provided in a primary care setting by the General Dental Services of the NHS. However, patients are expected to pay a nationally set fee unless they are exempt (children under 19 and in full-time education, pregnant and nursing mothers and those on low income). Outside Europe, in countries such as Iran, publicly funded dental services are stratified based on patient categories, focusing on children, pregnant women, and the elderly.
A range of barriers and enabling factors were reported in achieving UHC for oral health. Reported barriers were: • • • • • • •
On the other hand, several enablers were identified. It was recognised that if the challenges were addressed these would turn into enablers in achieving comprehensive oral healthcare. They included: • • Recognition of Essential oral health care and integration into UHC.
Discussion
The main objectives of this report are to summarise the key discussions from the workshop so that they may support actionable recommendations for EADPH’s future advocacy initiatives.”
UHC has been defined as “access to key promotive, preventive, curative and rehabilitative health interventions for all at an affordable cost, thereby achieving equity in access”. It consists of provision of health services to people with financial difficulties or in situations of social disadvantage. In essence, UHC provides comprehensive care in order for populations to maintain their health and well-being.
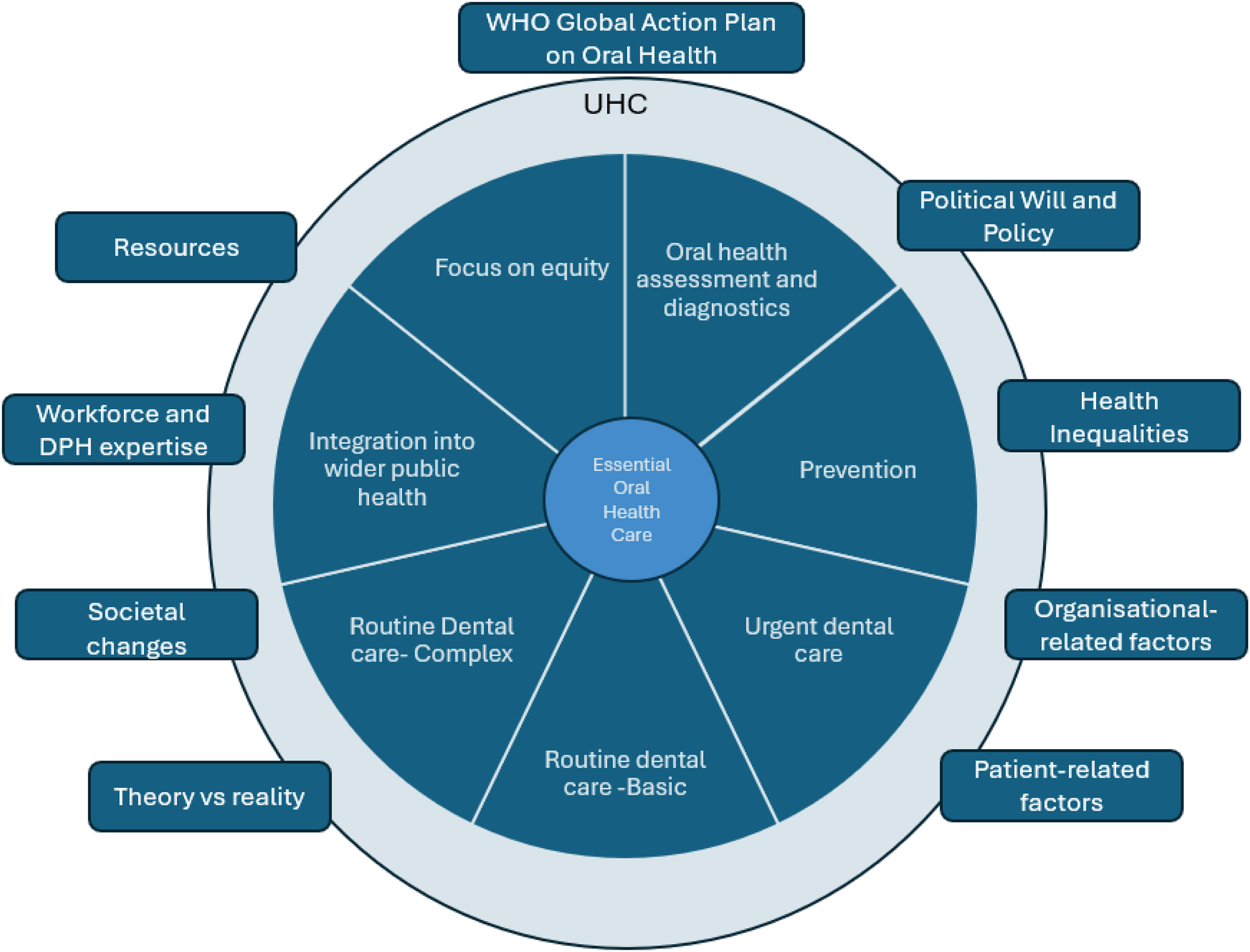
In order to implement UHC, it is necessary to explore what core set of safe and effective oral health care means, namely known as essential oral health care. Previously, essential oral health care has been defined as encompassing ‘’the most prevalent oral health problems through an agreed-on set of safe, quality, and cost-effective interventions at the individual and community level to promote and protect oral health, as well as prevent and treat common oral diseases, including appropriate rehabilitative services”(Benzian et al., 2021). However, the definition of essential oral health care can vary depending on context, resources and population needs.
At the core of this concept is the patient and how oral health is maintained to ensure good oral health function and wellbeing with minimum impacts on oral health related quality of life. well-being. Essential oral healthcare is intended to be affordable, accessible, and effective. It may encompass urgent dental care, routine dental care with a focus on prevention but also rehabilitation of the patient,so that they are able to maintain their oral health. In essence, oral health is no longer a luxury but a fundamental part of oral health. A recent scoping review on integration of oral health into UHC found few studies that included oral health within the UHC, defined by limited oral health services and focusing on particular populations (Marques Dos Santos et al., 2024).
Is it possible to ensure that delivery of oral healthcare targets those who are more likely to be marginalised depending on age, medical and mental health vulnerabilities, socio-economic disadvantage, those experiencing homelessness, refugees and asylum seekers, Gypsy and Roma travellers? How are these vulnerabilities defined? This is subject to interpretation and variation by regions and countries.
In relation to age, there has been a focus on children and limited attention to older people. The global population is undergoing a significant demographic shift, with the number of older adults (aged 60 years and above) increasing to 2.1 billion by 2050. This will have profound impacts on achieving healthy ageing and UHC. There are unique challenges for older people including higher prevalence of cognitive and physical decline, increased prevalence of Alzheimer’s, co-morbidities and poly-pharmacy. All of these factors will increase the risk of oral diseases and conditions and the need for more complex oral healthcare and may compromise healthy ageing.
If inequities in access to services are to be addressed, it may mean that more resources will need to be allocated to the most vulnerable populations, not only because of high unmet needs but also to provide high quality care for these patient groups, to promote improvements and maintenance of oral health.
There have been improvements in dental technologies and digital dentistry alongside societal shifts in expectations and demands and how they can be aligned with limitation in funding and resources.
No clear definition of what is essential oral health emerged from the workshop.
Nevertheless, since the EADPH 2025 workshop, Durvy et al. (2025) have proposed a number of possible essential oral health benefits baskets. When advocating for improvements in oral health, it is necessary to explore what comprehensive oral health care means, in the context of not just focusing on oral healthcare but integrating oral health into the wider public health agenda. Prevention and integration need to be at the centre of all policies to stop siloing oral health from the wider NCD agenda. There is the need to encourage adoption of UHC in alignment with tackling the wider social and commercial determinants of health as clinical care, although important on its own, cannot reduce the overall burden of oral diseases. Aligning UHC with action on social and commercial determinants ensures that oral health policies are proactive and preventive, contributing to health equity and broader sustainable development goals. All those involved in healthcare planning and in its delivery need to be made aware of these considerations. The EADPH could contribute by regularly reviewing oral health policies, to ensure they remain evidence-based and responsive to population needs, while providing clear guidelines to inform decision-making and strengthen oral health interventions. It could also facilitate European consensus on the definition and scope of essential oral health care, monitor progress through standardized indicators assessing access, quality, and equity, and promote collaboration with governments, NGOs, and academic institutions. Such actions would help - clarify the concept of essential oral health care, - support expansion of public funding, particularly for vulnerable populations, - address workforce challenges through the promotion of skill-mix and innovative care models, and integrate oral health into broader public health policies. The workshop has been a first step in this process.
Footnotes
Acknowledgements
The EADPH would like to thank the speakers, the four members who chaired the small group discussions and the four colleagues who acted as rapporteurs. They would also like to thank Dr Aristomenis Syngelakis and Dr Maria Tsantidou the local organisers for the pre-congress and congress.
Author contributions
All the authors planned the pre-congress workshop and this report. HF wrote the draft. KE edited it and ST-J and PV reviewed the draft. All the authors approved the final version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Colgate generously sponsored the workshop.