
Abstract
Interprofessional collaboration (IPC) has the potential of improving quality of dental care by integrating dental, medical and social care professionals to deliver high quality comprehensive and patient centered care. The aim of the study was to review current examples of good practice in IPC in selected countries globally followed by exploring the facilitators and barriers in achieving IPC. Barriers included fragmented health care and working in silos, governance and health system challenges, education, professional resistance and lack of integration and data sharing. A roadmap was developed which included the following domains: Governance and legislation, funding and incentives, education, health system public and community engagement, digital data and integration and multidisciplinary research. The findings will inform future development in policy, practice and research in supporting IPC and oral health for the benefit of populations and communities.
Background
At the 2025 EADPH conference, a workshop (sponsored by Colgate) was held in Rome. The theme of the pre-conference workshop ‘How can we bridge the gaps in Inter-Collaborative Practices (IPC) to advance Universal Health Coverage (UHC) and achieve oral health equity’. The workshop commenced with an introduction from Prof. Huda Yusuf, President of EADPH, setting the stage for an insightful exploration of IPC. Manu Mathur, Professor of Global Health at Queen Mary University of London, spoke about the current IPC landscape and the global and regional challenges. Dr Gitana Rederiene, representing the International Federation of Dental Hygienists, then delved into the critical role of skill mix within dental team to drive UHC forward. The discussion gained further momentum as Dr Rakee Patel, Deputy Chief Dental Officer of England and Senior Lecturer at Kings College London showcased real-world examples of successful IPC in oral health, with a focus on aging populations in the UK. Participants were then involved in interactive group discussions. They analysed IPC in their own respective countries, identified key barriers and facilitators, and brainstormed actionable strategies to strengthen IPC in oral health. This manuscript reports the key points which emerged from the workshop and suggests a roadmap for future progress in achieving IPC for oral health.
Definition of inter-professional practice (IPC) and its importance in public health
The World Health Organization (2010) defined Inter-Professional Collaboration (IPC) as a process where “multiple health workers from different professional backgrounds work together with patients, families, carers, and communities to deliver the highest quality of care.” (WHO, 2010) This concept extends to Inter-Professional Education (IPE), “where students from diverse health professions learn with, from, and about each other to improve collaboration and health outcomes. One of the advantages of IPC and IPE is that they bring multi-disciplinary health professionals together to address the significant burden of non-communicable and communicable diseases and associated health inequalities, which pose a threat to public health against a rapid demographic and epidemiological transition. Healthcare systems are struggling to keep populations healthy as treatment becomes more complex and costly. Therefore, IPC facilitates efficiency and quality in relation to service delivery, reduces duplication of efforts in prevention and treatment of diseases and improves mutual trust among different health providers in improving coordinated care and hence resulting positive outcomes for the population (Kaiser et al., 2022). It also boosts job satisfaction among health workers and promotes a preventive, patient-centered approach that considers socio-environmental determinants of health (Carron et al., 2021). In resource-limited settings, IPC is especially valuable, offering a way to maximise impact with constrained workforce and financial resources.
The gap in oral health: Why IPC matters?
Despite its proven benefits, IPC remains underdeveloped in oral health. Globally, Oral Health Professionals (OHPs) dentists and dental teams often operate in isolation, adhering to a traditional, curative, and medical-centric model. This approach leads to working in silos with limited interactions between health, education and social care. The WHO Action Plan for Oral Health calls for integrating oral health into Universal Health Coverage (UHC), ensuring that essential services are accessible and affordable for all. UHC prioritises three pillars: a skilled and equitably distributed workforce, a responsive and high-quality health care system with a focus on equity, and sustainable financing systems.
Globally, the total oral health workforce is compromised of approximately 4 million (3 984 325), oral health professionals of which 2.5 million are dentists, 1.2 million identified as “dental assistants and therapists” and 300,000 “prosthetists/technicians”. Yet, significant barriers persist with workforce shortages and maldistribution in many regions, increased reliance on private dental services, inadequate funding of public services and limited utilisation of skill-mix (Balasubramanian et al., 2021; WHO, 2022). Oral health systems often function separately from broader healthcare systems and there are in many contexts financial barriers, with high out-of-pocket costs making basic oral health services unaffordable especially for socio-economically disadvantaged communities. These challenges are particularly acute in oral health, where the lack of collaboration and integration exacerbates inequities in access and health outcomes (Hung et al., 2025).
Workshop insights: Bridging the gap in IPC for oral health
The pre-conference workshop in Rome brought together public health experts, students and health practitioners to explore how to advance IPC in oral health. Their collective reflections detailed in the following section highlight the barriers, facilitators, and actionable strategies needed to develop IPC in oral health. These insights provide a roadmap for policymakers, educators, and practitioners to drive meaningful change.
The current landscape of inter-professional collaboration in oral health
Participants highlighted a fragmented yet evolving state of IPC in oral health, marked by both persistent challenges coupled with innovative, but isolated, initiatives.
The oral health care system continues to operate largely in isolation, with a highly specialised dental workforce disproportionately concentrated in affluent urban areas. This imbalance leaves rural and underserved regions facing critical workforce shortages, exacerbating disparities in access to oral health care. Despite these challenges, several countries have pioneered targeted IPC interventions, though most remain localised and lack widespread implementation.
How is IPC operationalized in selected countries in relation to clinical practice, policy, education and research?
• In Australia, dental therapists are deployed in rural areas to improve access to dental care. The Australian Government has developed a strategy to develop the rural dental and health workforce due to challenges of the rural populations in accessing oral healthcare (Schwarz, 2006). • Nordic countries prioritise prevention and there is collaboration between dental professionals, schools, public health services, and social care to improve population-wide oral health outcomes. In Norway, public health nurses are recommended to check children’s teeth at the age of 2 years and refer them to the Public Dental Service. However, it was noted that this is not consistently adopted across all regions (Norwegian Health Directorate, 1999). • Malaysia’s National Oral Health Strategic Plan (2022-2030) emphasises “Partnership & Collaboration” as a priority area for inter-professional collaboration (Ministry of Health Malaysia, 2022). Oral health programme is part of the Ministry of Health and this means that they are integrated with other health professionals, Consultants in Dental Public Health (specialists) in each region to support the implementation of the national plan. • In Brazil, there is a national oral health policy and ICP has been achieved through universal health coverage. Dental teams frequently work with other health professionals in primary care (Galvão and Roncalli, 2021). • In Ireland, the Chief Dental Officer works collaboratively with other health departments including public health to realise the ambitions within the oral health plan (Department of Health, 2019) • In Ethiopia: Oral health is integrated into the Ministry of Health. However, the national plan for health is separate from oral health (Federal Democratic Republic of Ethiopia, 2025). • In France, the Service Sanitaire engages health students in health education activities within the community allowing IPE experiences early in the curricula. There are joined up modules in undergraduate dental education in some regions for dentists, GPs, pharmacists and nurses (Chapuis et al., 2025). • Egypt, Greece and Serbia did not have formal national policies on IPC.
In the UK, there are several examples of good practice: • the integration of Extended Duty Dental Nurses (EDDNs-nurses who have been trained to deliver preventive advice apply fluoride varnish on children), dental therapists, and clinical dental technicians (CDTs) to diversify dental care delivery (Gnich et al., 2014). • fluoride interventions in care homes and e-learning programmes (e.g. Stay Smiling) to train carers and social workers on oral health. • cross-disciplinary efforts like GP-dentist collaborative working: screening for diabetes in patients receiving periodontal care in primary dental care, conducting blood pressure checks in dental settings, illustrating the potential for widening the scope of dental teams and facilitating integrated care for patients to improve their oral health and health outcomes. • multi-disciplinary research between pharmacy, nurses and dental teams to improve oral health outcomes (Yonel et al., 2022) • direct access to dental hygiene and dental therapists approved by the UK General Dental Council (GDC, 2025)
Barriers to inter-professional collaboration in oral health
Participants identified multifaceted barriers that hinder the development and scaling of IPC in oral health, spanning systemic, structural, professional, communication, patients and the public challenges:
Structural silos and fragmentation of health care
• Isolated Systems: Oral health operates in silos, with minimal integration into broader healthcare networks. This isolation extends to education, where health professionals (HPs) are trained separately, reinforcing disciplinary boundaries, clinical practice and research. Physical isolation of dental practices from other health and social care providers does not facilitate collaborative working (Gallagher et al., 2024; Prasad et al., 2019). Additionally, there is lack of collaboration between private and publicly funded dental care. • Absence of formal IPC frameworks: There is a lack of standardised guidelines for IPC in both education and practice, making it difficult to establish a common language or shared protocols. This fragmentation contributes to inequities in access and outcomes • Pilot-Only Initiatives: While innovative IPC models exist, they remain localised and unscaled, failing to achieve systemic impact.
Governance and health system challenges
Medical, oral and social care operate separately with limited integration to ensure coordinated and collaborative dental care. • Political barriers and funding Policy Gaps: Decision-makers often lack awareness of IPC’s value in oral health, leading to inadequate funding and support (Harnagea et al., 2017). • Budgetary Isolation: Oral health departments and budgets are frequently separated from Non-Communicable Disease (NCD) programmes within Ministries of Health, undermining integrated planning and resource allocation. Frequently, oral health budgets are separated from general health budgets • Legislative Hurdles: Rigid legislation, regulation, and occupational rights impede task-shifting and role flexibility, limiting collaborative practice (Christian et al., 2023). • Private versus public dental care provision: It is recognised that different funding and provision exists globally with public, private and insurance systems with a dominance of private dental care provision. Some public systems tend to focus on certain groups of the population such as children and vulnerable populations (WHO, 2022). There is a significant gap between the oral health needs of the population, perceived needs and availability, accessibility and affordability for dental services. This is especially apparent for disadvantaged populations, as well those living in rural areas. • Scarcity of Dental Public Health (DPH) leadership within oral health systems further isolates oral health from the wider public health and healthcare systems. Lack of dental public health limits strategic overview, jeopardising capacity to coordinated population based oral care initiatives resulting in fragmented policies and dental care planning. This does not facilitate IPC further restricting integration of oral health into wider healthcare systems.
Education, professional resistance and capacity gaps
• Education: Very few countries have established standardised dental education which is integrated into broader health or interprofessional programmes. Inter-professional education, which involves clinical exposures facilitates health professionals from different backgrounds to learn together to build the foundation for collaboration between dental, medical, pharmacy and midwifery (Haber et al., 2021). Limited oral health literacy among non-dental HPs (e.g., GPs) and lack of integration between different areas of primary care hinders efforts in interdisciplinary working and compromising patient health outcomes and professional satisfaction. • Threats to professional identity and resistance to change: the dental workforce may be protective of their roles and professional identity due to perceived risks to job security. This is coupled with hierarchical structures of the dental professionals which may hinder skill mix within dentistry but also integration into wider primary care. • Workforce Pressures: Oral Health Professionals (OHPs) are often overwhelmed, facing time constraints and financial pressures, which leave little room for collaborative initiatives. * • Communication: Communication can be challenging across health and social care professionals which may hinder collaborative care planning for patients. Health and social care professionals need to work together effectively and achieve an adequate standard of interprofessional communication skills. There are challenges including the dynamics between different professionals and hierarchy, dealing with misunderstanding and conflict, resources and time dedicated to communication and building trust and rapport (Lindqvist, 2015). Poor communication can lead to inefficient information-sharing between hospitals, outpatient, and primary care settings which disrupt continuity and coordination to improve patient outcomes.
Data sharing
Dental care is usually isolated from the rest of the healthcare and social care systems including lack of integration of patient dental and health digital records. Knowledge and data may be interpreted differently depending on setting and context, malalignment in governance structures which may impede data sharing between the institutions and sectors.
It can be conclude that these barriers—systemic, professional, and operational—highlight the need for policy reforms, better workforce training, and cross-sectoral integration to unlock IPC’s full potential in oral health.
Solutions to strengthen IPC in oral health
Who to involve?
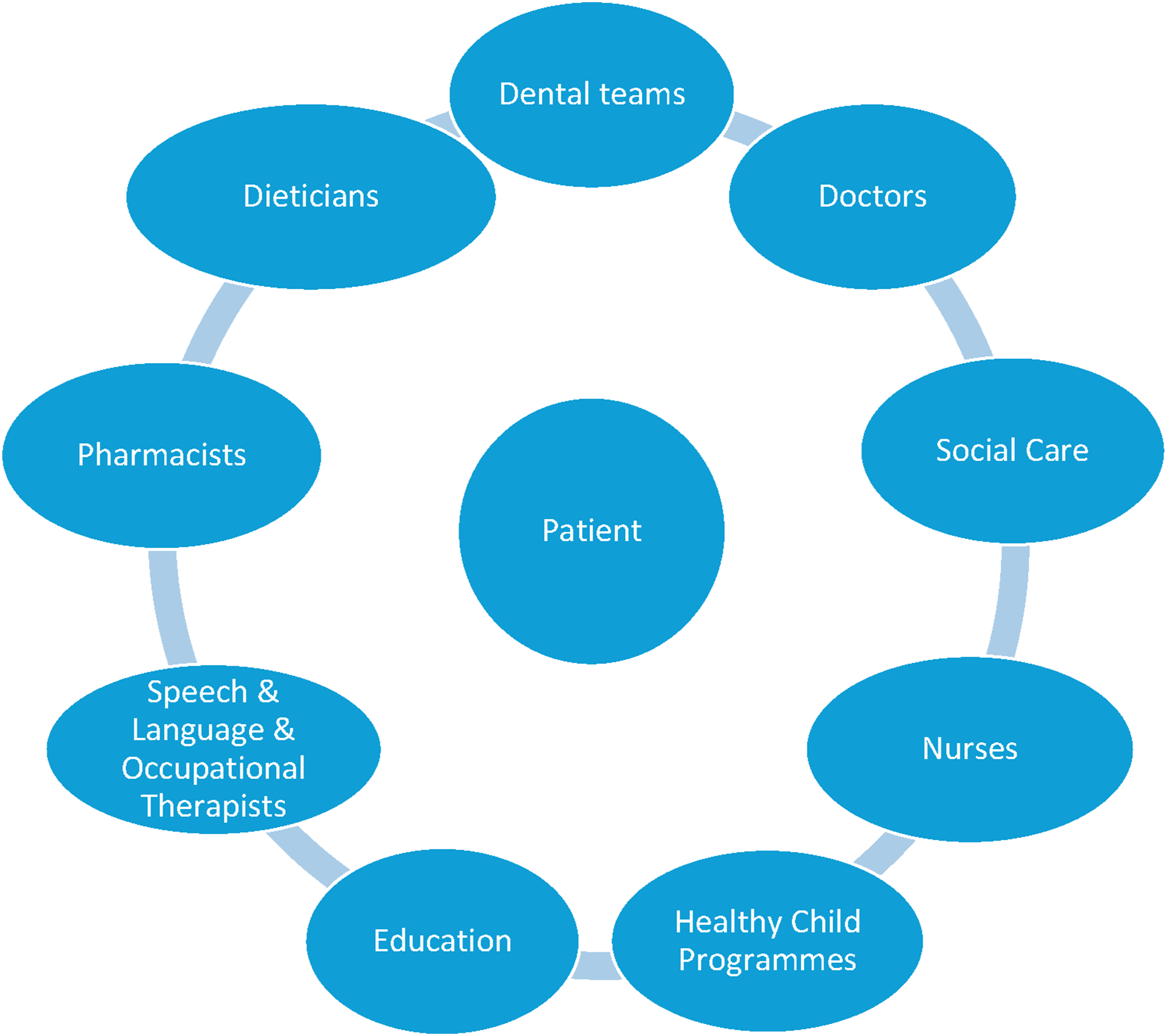
Key actors for Inter-Professional Collaboration in relation to oral health (Figure 1): • Health Professionals: Oral health professionals (OHPs), general practitioners (GPs), nurses, midwives, speech therapists, physiotherapists, occupational therapists, pediatricians, nutritionists/dietitians, geriatricians and health care assistants, pharmacies • Non-Health Professionals: Social care workers, community workers, nursing and care home staff, and staff working in education. • Skill Mix in dental settings: Expand dental teams to include dental hygienists, therapists, and clinical dental technicians. • Focus on vulnerable populations across the life-course: people with additional or special needs, populations with multiple disadvantage including children in care, those experiencing homelessness, refugees and asylum seekers, mental health and older people. Key actors in achieving IPC.
Where to implement IPC?
Strategic Locations for Integrated Care and multi-sectoral collaboration in: • Healthcare Settings: Community health centers, primary care clinics, mixed medical-dental clinics, hospitals, baby clinics, and pharmacies. • Community and Educational Settings: kindergartens, schools, community centres, nursing and care homes. • Local Government Role: Engage cities and municipalities to facilitate access and coordination • Patient, Community and voluntary sector involvement.
How to implement inter-professional practice?
Structural transformation of systems is required in achieving IPC with national governance and leadership. This will be aligned with a paradigm shift from a medical model-centered approaches to holistic approaches to achieving positive oral health outcomes. Such transformation relies on: 1. Governance and legislation: There is a need to create a shared vision and statement to implement national policies in education and clinical practice to facilitate inter-professional practice and provide patient-centered care. This will mean that collaboration between different sectors is prioritised and oral health is integrated into the wider education and health and social care systems. National standards and frameworks need to be developed to guide education, health systems and professional regulation that focus on adoption of oral health into all policies and ensure that multi-sectoral approaches to adoption of IPC. 2. Funding and incentivisation: pooling of budgets and moving away from allocating budgets in silos to oral health to encourage joint working across sectors. Incentivisation of professionals to adopt shared-decision making and ensure that there are collaborative care plans for patients to impact on oral health and health outcomes. 3. Education: Interdisciplinary education should be implemented with the aim of shared training programmes for dental care professionals, medical professionals, and wider health professionals nursing, physiotherapists, psychologists, occupational therapists, speech and language therapists, pharmacists and allied health professionals. This could be facilitated in unifying the curricula and ensuring that students are exposed to lectures and tutorials earlier in the timetable but also in clinical settings to gain experiential experience in team building and working effectively from the start. Skills and competency-based learning should be encouraged rather than siloed technical knowledge. It is also important to foster a common language and mutual understanding of roles and responsibilities (Van Diggele et al., 2020). 4. Health systems and communication: Teams being situated in common physical locations to ensure smooth coordination between different sectors. Include early community outreach for OHPs to build interdisciplinary experience. With universal health coverage becoming more widely available, ICP is a valuable tool for maximizing the effective use of these services. Collaborative working in multi-disciplinary teams ensures a holistic approach to patient-centred care and communication, thereby improving oral health outcomes. This has the advantage of increasing capacity, service reach and efficiency by involving wider health and social care teams and integrating oral health within the primary care systems and achieving UHC and “leaving no one behind” (Reeves et al., 2017). This also ensures that disadvantaged and vulnerable communities are mainstreamed into local health services provision and addressing oral health inequalities. Prevention is at the heart of UHC and therefore through adopting IPC, prevention becomes everybody’s responsibility. Prevention becomes everyone’s responsibility and catastrophic out of pocket payments can be reduced for the population. 5. Workforce transformation and reform: Task Shifting: Delegate tasks to lower-qualified health workers (e.g., hygienists for prevention). The use of skill-mix and IPC will facilitate progress in achieving UHC, however there are significant challenges in achieving this ideal model. There may be inadequate number and distribution of the workforce between low-, middle- and high-income countries and inequity in distribution within countries. High-income countries have a dentist–population ratio of 6.85: 10 000 while low-income countries have a ratio of only 0.57: 10 000, which is 12 times lower, respectively (WHO, 2020). This is further aggravated by reliance on private oral health care systems and under-resourced public oral care services, variation in workforce in rural and disadvantaged populations further widening oral health inequalities (WHO, 2022). Task shifting offers an opportunity to reforming and innovating the distribution of responsibilities in the wider workforce. A systematic review on oral health demonstrated that task shifting (facilitating dental therapist and hygienist to widen the scope of practice can improve access and equitable access to oral healthcare (Dyer et al., 2014). Going one step further is to explore task shifting which is defined as delegating tasks to existing or new health workers with either less training or narrowly tailored training. Evidence has shown that mid-level staff can deliver clinical care safely and effectively, provided they receive adequate training and support. This model of care can enhance capacity and coverage of care especially in underserved areas (Lassi et al., 2013). 6. Public, community and voluntary sector involvement: There have been limited studies exploring patient and public involvement in delivering IPC and this a serious limitation if the aim of IPC is to improve patient outcomes (Morgan et al., 2020). Involvement of patients and communities and co-production should be at the heart of any initiatives that encourage collaboration. Considering the lived experience of patients and communities directly or indirectly through the voluntary sector need to ensure that patient voices are heard and considered in delivery of oral health care. 7. Digital integration and data sharing across sectors: Data Systems: Create integrated health information systems to facilitate data sharing between dental, medical and social professionals. Indeed, digital technologies are rapidly being integrated into a wide range of health fields, with the potential to significantly improve healthcare outcomes (Steinhauser and Raptis, 2023). However, its effective implementation implies that the health workforce has a sufficient level of skills to navigate the digital transformations in health (Wong et al., 2021). Capacity building in this field particularly requires educational frameworks that place an emphasis on interdisciplinary learning. Estonian National Health Information System Sharing data between providers, patients and the state since 2008. The adoption of electronic health data that integrate oral health brings transformative benefits across the healthcare ecosystem. By enhancing accountability and transparency, it fosters trust among citizens, providers, and other stakeholders. Efficient data sharing and improved data quality streamline service provision, while robust data security safeguards sensitive information. The increased usability and impact of health data empower evidence-based policy, drive innovation, and support research—ultimately leading to better health outcomes and more responsive, patient-centred care. In the future, AI will be key in supporting dentists, researchers and other healthcare professionals to work collaboratively by making it easier and safer to share patient data to improve oral health. But to use AI in healthcare, collaboration and strong privacy protections are needed in order to allow the combination of different types of data (radiographs, scans, and patient records) from various places or domains. The use of AI represents an effective tool to reinforce IPC, making diagnoses more accurate, improving treatment plans, and achieving better results for the patients. It is also itself a challenge for the structuring of interprofessional relationships (Brinz et al., 2025). 8. Research: It is important to recognise gaps in research in relation to inter-collaborative practice in achieving oral health and understanding the barriers and facilitators. Health is multi-faceted and therefore IPC needs to be coupled with inter-disciplinary collaboration in research and shift towards integration of public health into clinical research. This could potentially foster information generation, cross-cutting learning across disciplines, concepts and theories which can subsequently improve research quality (Frenken et al., 2025). Dissemination of research findings can be undertaken by different health and social care professionals thereby facilitating pathways to impact. This will in turn improve patient oral health related outcomes. This sharing of concepts, knowledge and skills can elucidate solutions to oral health challenges by integrating it into wider public health, clinical and implementation science research will also support tackling oral health inequalities (Lee et al., 2009).
Best practice example
These eight considerations are summarised in the roadmap (Figure 2). A roadmap to achieving IPC.
Conclusions
IPC is essential in integrating oral health into wider health care systems and achieving universal health coverage in line with the WHO Global Action Plan on oral health. Despite historical fragmentation of oral health and dental care from other non-communicable diseases and healthcare system, there is now growing momentum in collaborative leadership to integrating practice, education and research to ensure equitable, preventive and patient-centred care. This will require transformation and integration of governance, legislation, pooling of funding and incentivisation to transform healthcare systema and education to achieve oral health by 2030.
Footnotes
Acknowledgements
The EADPH would like to thank the speakers (Professor Manu Mathur, Dr Rakhee Patel and Dr Gitana Rederiene, members who chaired the small group discussions and the four colleagues who acted as rapporteurs. They would also like to thank Colgate for sponsoring the workshop and all the attendees for their valuable contributions.
Author contributions
All the authors planned the pre-congress workshop and this report. HY chaired the session and wrote the first draft. KE edited it and ST-J revised and reviewed the manuscript. All three authors approved the final version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Colgate generously sponsored the workshop.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.