
Abstract
Loneliness is a complex and multifaceted experience resulting from a person’s subjective assessment of the gap between their desired and actual social connections. This study presents an analysis of prevalence rates and correlates of loneliness amongst Maltese individuals aged 11 years and older (n = 658). Data collected in 2022 allowed for a follow up on a first ever study investigating loneliness in Malta in 2019 (n = 1,009) and makes comparisons to understand how loneliness prevalence rates have changed over time and in view of the COVID-19 pandemic. Results show that in 2022, 54.6% of the sample reported some degree of loneliness. The sociodemographic characteristics that were significantly associated with the highest levels of loneliness were age (11–19 years and 55+), lower levels of education, being widowed, retired, low household income, decreased sense of neighborhood belonging, poor general health, poor coping abilities and not feeling positive about life. Compared to 2019, mean overall loneliness scores were significantly higher in 2022. The most marked increases were observed amongst the youngest groups (11–19 years and 20–34 years), those with the lowest and the highest educational levels, those with a weaker sense of neighborhood belonging and those with poorer coping abilities. The paper makes some recommendations for further research, policy and practice in view of the findings.
Introduction
Humans are by nature, social animals and possess deeply ingrained mechanisms designed to assist in navigating social connections which are crucial to the maintenance of good health (Cacioppo et al., 2014). The felt experience of loneliness developed as an evolutionary function to reduce social isolation and increase chances of survival by motivating individuals to form connections with others. In this sense, experiencing a transient sense of loneliness may be an adaptive experience since it encourages the person to create and maintain social relations (Cacioppo et al., 2014). However, when loneliness persists into a chronic state, and the individual experiences a lack of satisfying relationships or connections, this results in the activation of behavioral and neural mechanisms which lead to negative health outcomes (Cacioppo & Hawkley, 2009; McDade et al., 2006). The term ‘loneliness’ refers to a person’s subjective assessment of the gap between their desired and actual social connections. It is similar yet distinctively different to social isolation (Holt-Lunstad et al., 2015; Perissinotto & Covinsky, 2014). Social isolation pertains to the number of an individual’s social connections, whereas loneliness focuses on the quality of those relationships. Loneliness is subjectively experienced and negative (De Jong Gierveld & Van Tilburg, 1999). Research has shown that loneliness greatly affects a person’s overall wellbeing, whilst also posing a significant health and societal challenge (Klinenberg, 2018; Nowland et al., 2018). A growing body of empirical evidence continues to demonstrate the serious concern for public health which is posed by chronic loneliness (Holt-Lunstad et al., 2015). More and more data reveal that young people’s health is significantly impacted by loneliness. Qualter et al. (2013) revealed that moderate or high levels of loneliness in young people were correlated with lower subjective health ratings and more frequent visits to the doctor. Loneliness is also an economic concern, including considerable costs to public healthcare systems, and loss of productivity and profitability to employers and the economy (Kung et al., 2021; Mihalopoulos et al., 2020). Meisters et al. (2021) report that loneliness is associated with higher primary care and mental healthcare spending.
In the Maltese context the first national survey of loneliness amongst the Maltese population was conducted in 2019 (Clark et al., 2019, 2021). This was the first comprehensive attempt to measure loneliness across different age groups on the Maltese Islands. In Malta, research on loneliness had primarily focused on university students and older individuals in institutional settings. While empirical evidence on the prevalence of loneliness in Malta was limited, there were indications that loneliness was increasing, evidenced by the rising number of calls to the national support line from individuals experiencing loneliness (Clark et al., 2019). In 2018, the Faculty for Social Wellbeing produced a research documentary, University of Malta, Faculty for Social Well Being (2018) (The Wound of Loneliness) which uncovered the phenomenon. The 2019 initial study aimed to: assess the prevalence of loneliness among the Maltese population; explore relationships between loneliness and various socio-demographic and structural variables; and contribute to the existing body of empirical research on loneliness.
The social context of the Maltese islands is characterized by a blend of traditional values and modern influences, shaped by Malta’s colonial background, strong family and community ties, religious heritage, and recent socio-economic transformations due, in part, to EU membership since 2004 (Mitchell, 2002). While Malta, the southernmost nation state in the EU, experienced slower economic development, in the early 21st century, Malta embraced a neoliberal agenda promoting individualism, significantly altering its societal fabric (Visanich, 2020). Traditionally, Malta boasted close-knit communities. Villages and towns had a strong sense of identity, reinforced by local feasts (festas) and other community events (Boissevain, 2001). Modernity’s influence in Malta is particularly visible in its fast-changing urban areas, marked by numerous construction projects and changes in the population (Cuff et al., 2024), with their impact on how one experiences community. Loneliness has implications for both physical (Nowland et al., 2018) and mental health (Meisters et al., 2021) and understanding its prevalence and impact can help in crafting public health, family and community development interventions. Generating data from standardised tools that is comparable to that of other countries allows for examination of how varying social structures and cultural elements impact individuals' sense of connection. In Malta, the family has historically been a key provider of social support. However, its role has been evolving in recent years. Changes include shifting gender roles within families, a redistribution of power between men and women, and the introduction of divorce and civil partnerships. Additionally, there has been a rise in the age of marriage, a decline in fertility rates, and an increase in the number of children born outside of marriage, all contributing to the growing diversity of the Maltese family (Abela, 2016). By understanding the extent and correlates of loneliness in different contexts, targeted policies to reduce loneliness and improve social integration can be developed with context in mind. The measurement of loneliness in Malta can inform polices relating to its aging population (Formosa, 2021) given loneliness is particularly prevalent among the elderly, with comparative studies helping identify best practices for supporting older adults across different cultural contexts. Malta has also experienced drastic increases in levels of urbanization, as well as migration, perhaps making social isolation more pronounced. Understanding these trends, in comparison to those in other countries, can help in designing interventions that take into account how cultural, social, and economic factors foster connected and resilient communities.
The current study compares 2022 data on loneliness with data collected in 2019, when the initial survey of loneliness amongst the Maltese population was conducted. Those findings indicated that Maltese individuals are more prone to severe loneliness if they have low subjective wellbeing, rate their coping ability poorly, live alone, or are widowed. Additional factors linked to severe loneliness included having a disability, a low level of education, financial insecurity—reflected in the perceived adequacy of household income—and residing in a home with an unpaid mortgage.
The present study examines the following research questions. RQ1: What is the prevalence of loneliness in Malta in 2022 and what sociodemographic variables are associated with loneliness? RQ2: Are there any significant differences in loneliness levels between data collected in 2019 and 2022 and are these associated with specific sociodemographic variables?
Literature review
The connection between mental health, wellbeing and loneliness has been extensively studied. Loneliness is considered to be a transdiagnostic construct (Käll et al., 2020) which can be experienced alongside, as well as exacerbating or predicting mental health conditions (Cacioppo & Cacioppo, 2018; Hawkley & Cacioppo, 2010) such as depression (Vanhalst et al., 2013), eating disorders (Levine, 2012), social anxiety (Lim et al., 2016), and suicidal action or ideation (Mezuk et al., 2014; Stickley & Koyanagi, 2016). International research shows that several sociodemographic variables are linked to the likelihood of experiencing and reporting loneliness. These variables include gender, age, socioeconomic status, employment status, and community factors, among others, factors investigated in the first Maltese national study in 2021. Regardless of age, females have been more likely than males to report feelings of loneliness (Barreto et al., 2022; Pinquart & Sörensen, 2001; Rokach, 2018) although more recent research is failing to find consistent patterns of gender differences in loneliness amongst the general population (Pagan, 2020). The earlier gender differences might be explained by societal gender roles (which are rapidly changing) and the extent to which the different genders are willing to report the phenomenon. The stigma associated with the reporting of loneliness is also more present for males (Barreto et al., 2022). With regards to age, loneliness rates exhibit a non-linear complex relationship when viewed across the lifespan (Clark et al., 2021). The 2019 Maltese study on loneliness also found that loneliness was significantly associated with age group, with higher rates among older persons (Clark et al., 2021). However, a nationally representative cross-sectional study (Hawkley et al., 2022) failed to provide sufficient evidence for loneliness predictors which were specific to certain age groups. In this study, the predictors of loneliness were household size and income, marital status, health, and frequency of socializing. Qualter et al. (2021) revealed consistent findings with regards to sociodemographic associations; loneliness was more prevalent amongst those with lower socioeconomic status (SES), poorer academic achievement and unemployment (Qualter et al., 2021). The literature also indicates that individuals with low SES (Macdonald, Nixon, & Deacon, 2018), living in deprived communities with inadequate services and transportation (Kearns et al., 2015) are at heightened risk of experiencing loneliness. Socially disorganized communities are often characterized by a high rate in change of residents, which makes establishing and maintaining permanent friendships difficult (Kearns et al., 2015). Stable and healthy relationships as well as marriage are protective factors against loneliness, especially in later life (Stokes, 2017; Fokkema, de Jong Gierveld & Dykstra, 2012). However, this is mediated by the quality of the relationship (Ayalon et al., 2013) and a poor relationship may actually lead to isolation (Dykstra et al., 2005; Lehmann et al., 2015). These same sociodemographic factors emerged as significant to the experience of loneliness in the Maltese 2019 survey mentioned above. Higher loneliness rates were observed among individuals with lower educational levels, those who are unemployed, widowed, separated, or divorced, those living alone, those with an unpaid mortgage, and those who perceive their household income as inadequate. Loneliness was also more prevalent among individuals who rate their physical health, coping ability, and subjective well-being poorly, as well as among those with a disability. Conversely, participants who engage in active citizenship exhibited significantly lower loneliness rates compared to those who do not participate in such activities (Clark et al., 2021). People’s mental health and well-being have been significantly and widely impacted by COVID-19, including an increase in loneliness and social isolation across gender and age groups (Ernst et al., 2022) as well as increases in anxiety brought about by the disruption in daily life and the wide-ranging economic impact (Azzopardi et al., 2023).
The literature review highlights that loneliness is a significant predictor and exacerbator of various mental health conditions, with demographic factors such as gender, age and socioeconomic status influencing its prevalence. The 2019 Maltese study corroborated these findings, noting higher loneliness rates among older adults, individuals with lower socioeconomic status, and those experiencing poor health. The current study will explore changes in loneliness levels between 2019 and 2022 and how these are associated with specific sociodemographic variables as well as how COVID-19 may have further amplified these issues across different demographic groups.
Methods
A cross-sectional design was used to collect data on loneliness prevalence and associated sociodemographic characteristics. Data collection took place during July 2022 when Maltese authorities removed social distancing measures. The target population consisted of all persons aged 11 years and over living in private households in the Maltese Islands. The same random sampling process used in 2019 was once again adopted in order to allow for comparability of findings and to ensure a uniform and adequate representation of respondents’ gender, residential district and age group. Participants were then selected through the use of a random number generator which identified local telephone and mobile numbers. In both study periods, survey data were weighted to correct for any biases present in the final sample of participants, arising from different rates of responses observed in different categories. During data collection, the sample proportions of participants grouped by gender, age and district were comparable to the corresponding population proportions. A sample of 1009 participants collected in 2019 and another sample of 658 participants collected in 2022 guaranteed a maximum margin of error of 3.1% in 2019 and 3.8% in 2022, assuming a 95% confidence level.
The survey was available to participants in Maltese or English. Ethical approval was obtained from the Faculty Research Ethics Committee of the Faculty for Social Wellbeing at the University of Malta (Ref. SWB-2021-00091). Participants were verbally advised of the purpose of the study, voluntary participation, the right to refuse to answer any questions, and the guarantee of anonymity. In the case of minor participants aged less than 18 years old, parental guardians’ verbal informed consent was obtained prior to gaining participants' informed assent. The 11-item De Jong Gierveld Loneliness Scale (DJGLS) was used (De Jong-Gierveld & Kamphuls, 1985). This standardized scale consists of five items which measure social loneliness (Questions 1,4,7,8,11) and six items which measure emotional loneliness (Questions 2,3,5,6,9,10), including both positively- and negatively- worded statements on which participants are asked to rate their agreement. Social loneliness is assessed by neutral or negative responses to items such as, “I can call on my friends whenever I need them,” while emotional loneliness is indicated by neutral or positive responses to items such as, “I often feel rejected”. Response options are: “Yes,” “More or less,” or “No”. Each scale item is subsequently scored, giving a social loneliness score and an emotional loneliness score, both of which are combined to provide a total loneliness score ranging between 0-11. A score of 0–2 indicates that the individual is not lonely, whilst a score of 3–8 indicates a moderate degree of loneliness, and a score of 9–11 indicating severe or very severe loneliness. To ensure correct interpretation among the adolescent population and in the Maltese version of the scale, one additional qualifying question was also added to the original 11-item DJGLS. The question “Do you have a really close friend?” (Yes or No) was posed to the participants after the first question of the original scale. This additional question was not included in the analysis for the current paper and for the original research report in 2019.
The DJGLS was chosen for the present study because it was the tool used in the 2019 study on loneliness in Malta, thereby allowing for a comparison of loneliness prevalence and correlates in two time periods and following the occurrence of a pandemic. The instrument has undergone considerable validation for use with various age groups (Grygiel et al., 2019; Penning et al., 2014) and has proven to provide consistent results across cultural groups (Van Tilburg et al., 2004). The DJGLS has good psychometric properties, with De Jong Gierveld and Van Tilburg (1999) reporting internal consistency coefficients that range between .80 and .90. In the current study, reliability was adequate at the full-scale level in both 2019 (Cronbach´s α = 0.738) and 2022 (Cronbach´s α = 0.789). The final questionnaire package consisted of 32 items. 20 items assessed health and sociodemographic factors. These items were developed in collaboration with the Maltese National Statistics Office in 2019 during the development of the original instrument. Minors were not asked to respond to all the sociodemographic items - for example, they were omitted from questions about occupational status (automatically marked as “student”) and marital status (automatically marked as “single”). Translation of the questionnaire was done according to respective guidelines, whereby an independent researcher who is a native Maltese speaker translated the DJGLS into Maltese, following which the questionnaire was back-translated from Maltese to English. Loneliness scores were computed according to author instructions. While it is recognized that the use of the same sample participants would have allowed for better comparability of the two data sets, the anonymous nature of data collection in both surveys did not allow for this.
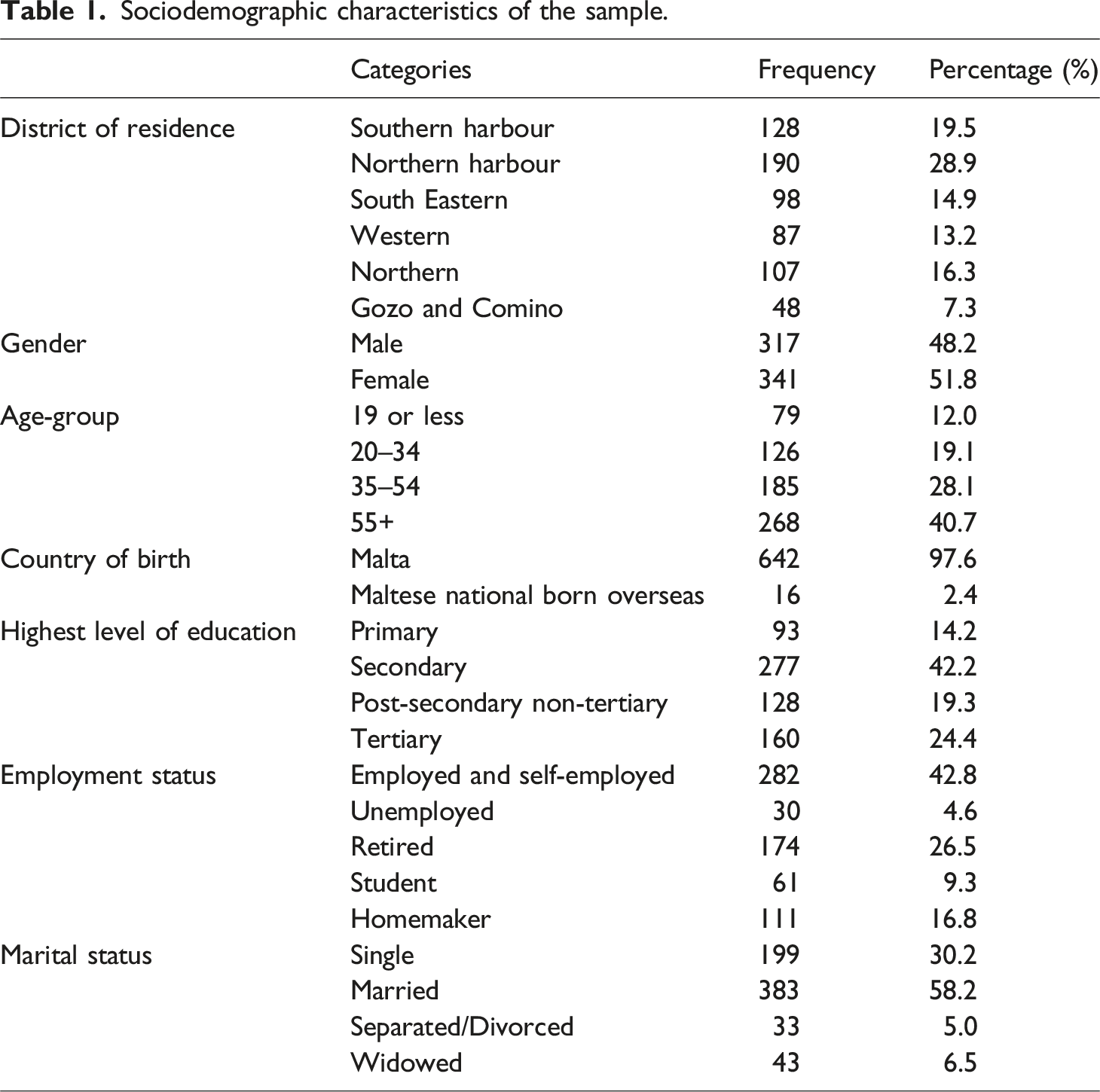
Sociodemographic characteristics of the sample.
Data analysis
The data was analyzed utilizing the IBM Statistical Package for the Social Sciences (version 29). Analysis was undertaken in order to make comparisons between the current (IBM, 2022) dataset and the data collected in 2019, when the initial representative survey of loneliness amongst the Maltese population was conducted. Descriptive statistics tables showing means and standard deviations were used to analyze the prevalence of loneliness in 2022. The Independent Samples t test was used to compare mean loneliness scores between 2022 and 2019. The One-Way ANOVA was used to compare mean loneliness scores in 2022 between groups of participants clustered by a number of socio-demographic variables. Moreover, the same test was used to compare differences in mean loneliness scores between 2022 and 2019 for groups of participants across the same socio-demographic characteristics of the participants. A 0.05 level of significance was used for all statistical tests and any p value >.05 indicates no statistical significance while p values of <.05 indicate statistical significance. In the current study, due to the word count limit, only findings with a p value of <.05 are presented in the tables and only those with a p value of <.001 are discussed in text.
Results
The results below commence with a presentation of the percentage of individuals who reported feeling not lonely, moderately lonely, severely and very severely lonely in 2022. Differences in mean loneliness scores are then presented, compared to those from 2019 and further analyzed according to a number of socio-demographic characteristics.
Levels of loneliness in 2022
A total of 54.6% of the sample reported experiencing some form of loneliness, whilst 45.4% were not lonely. From the group who were classified as lonely, 49.2% were experiencing moderate loneliness and 5.2% severe and very severe loneliness.
Significant differences in mean loneliness scores in 2022 according to socio-demographic characteristics
Differences in mean loneliness scores by sociodemographic characteristics (95% confidence interval)ª.
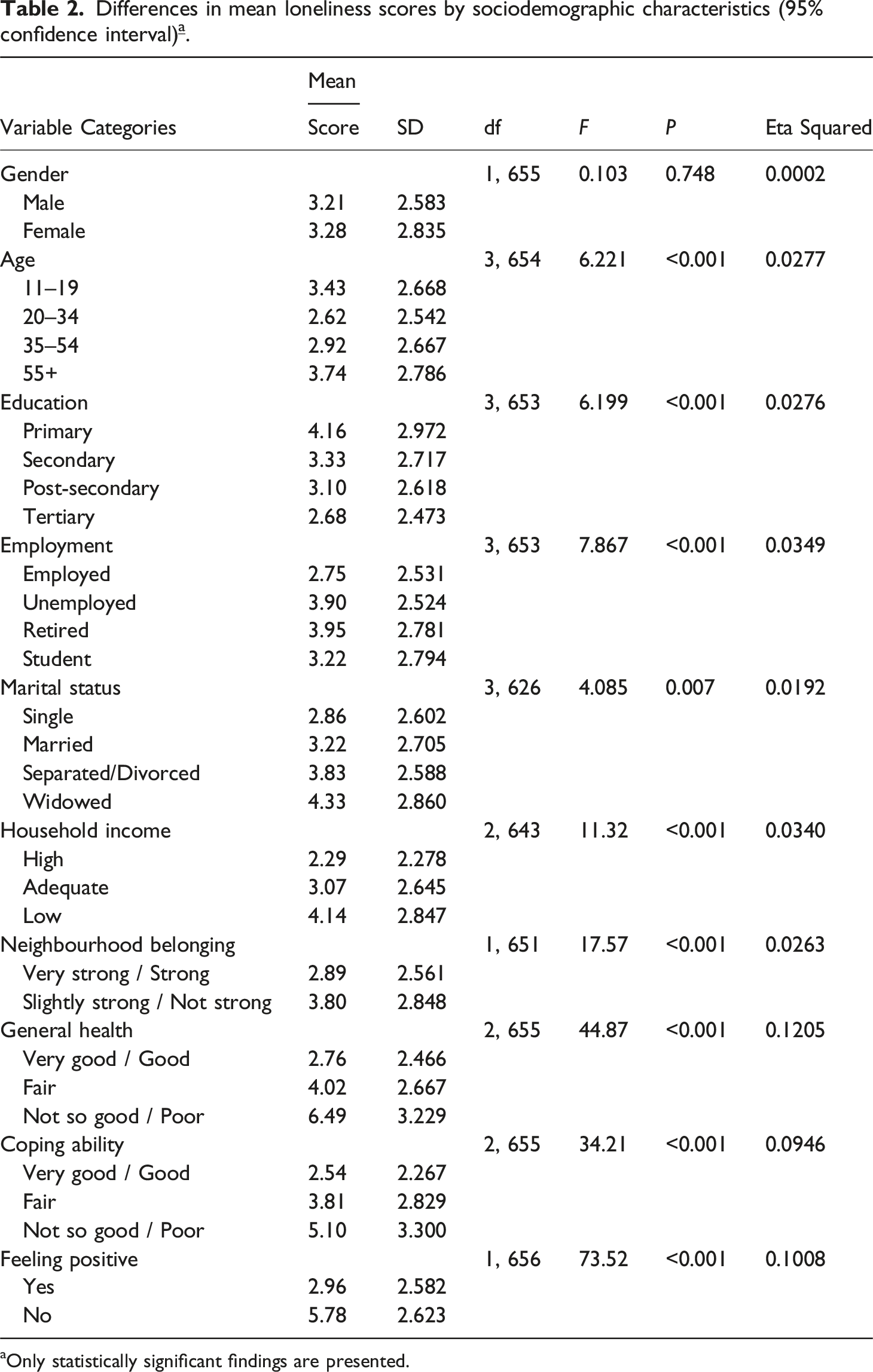
aOnly statistically significant findings are presented.
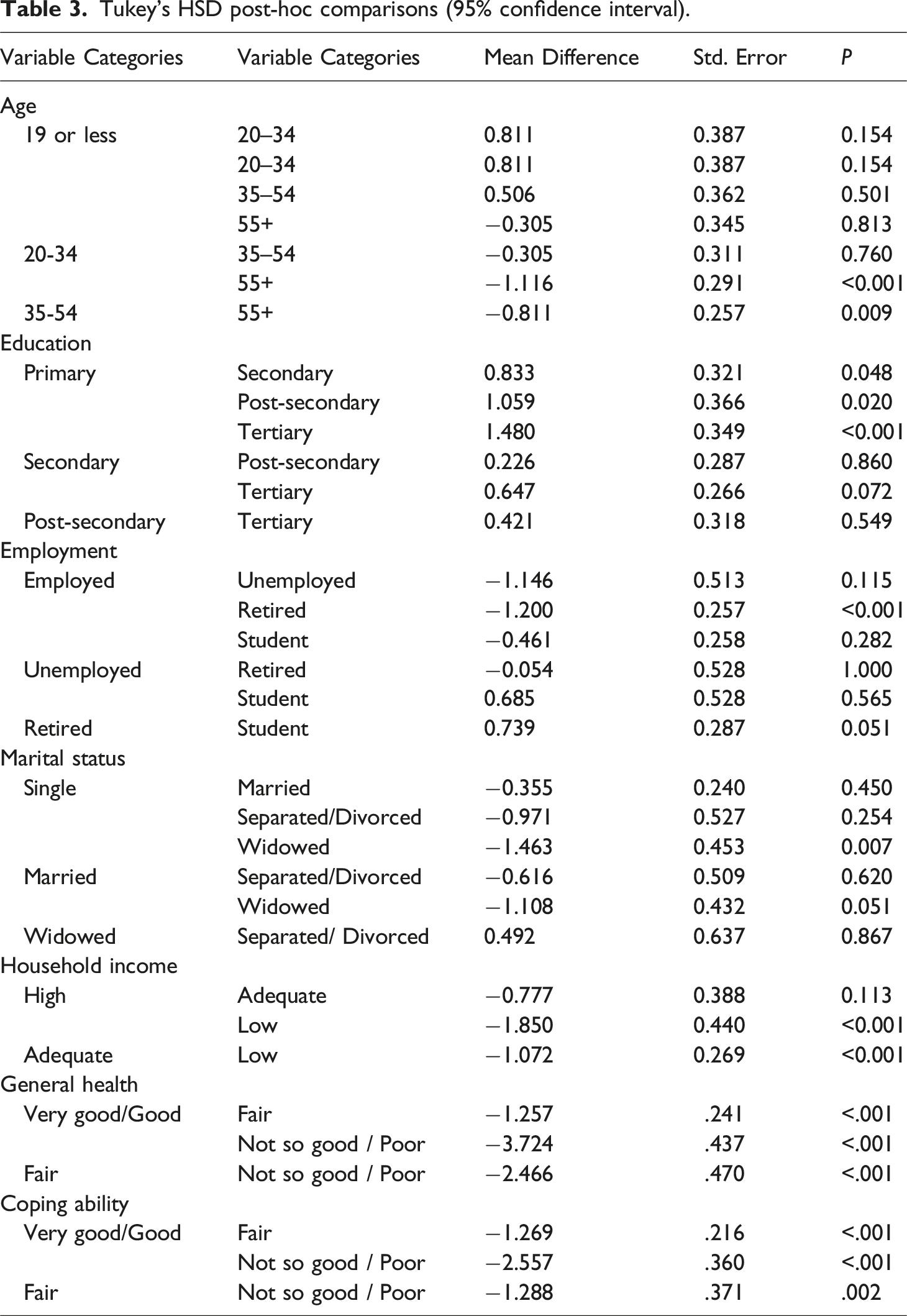
Tukey’s HSD post-hoc comparisons (95% confidence interval).
A Two-Way ANOVA regression model including an interaction effect was fitted to relate the loneliness score to two predictors (age and marital status). The p-value for age (0.068) is much lower than the p-value for marital status (0.750) or the p-value of their interaction effect (0.460). These findings indicate that there was more variation in the mean loneliness scores between the age groups than the marital status groups and consequently the higher rates of loneliness among widows could be partially attributed to their older age. Finally, the mean loneliness score of those reporting to be in good health was significantly lower than those reporting fair health, who in turn had a significantly lower mean loneliness score than those reporting poor health. Similarly, the mean loneliness score of those with good coping ability was significantly lower than those with fair coping ability, who in turn had a significantly lower mean loneliness score than those with poor coping ability.
Changes in loneliness scores from 2019 to 2022
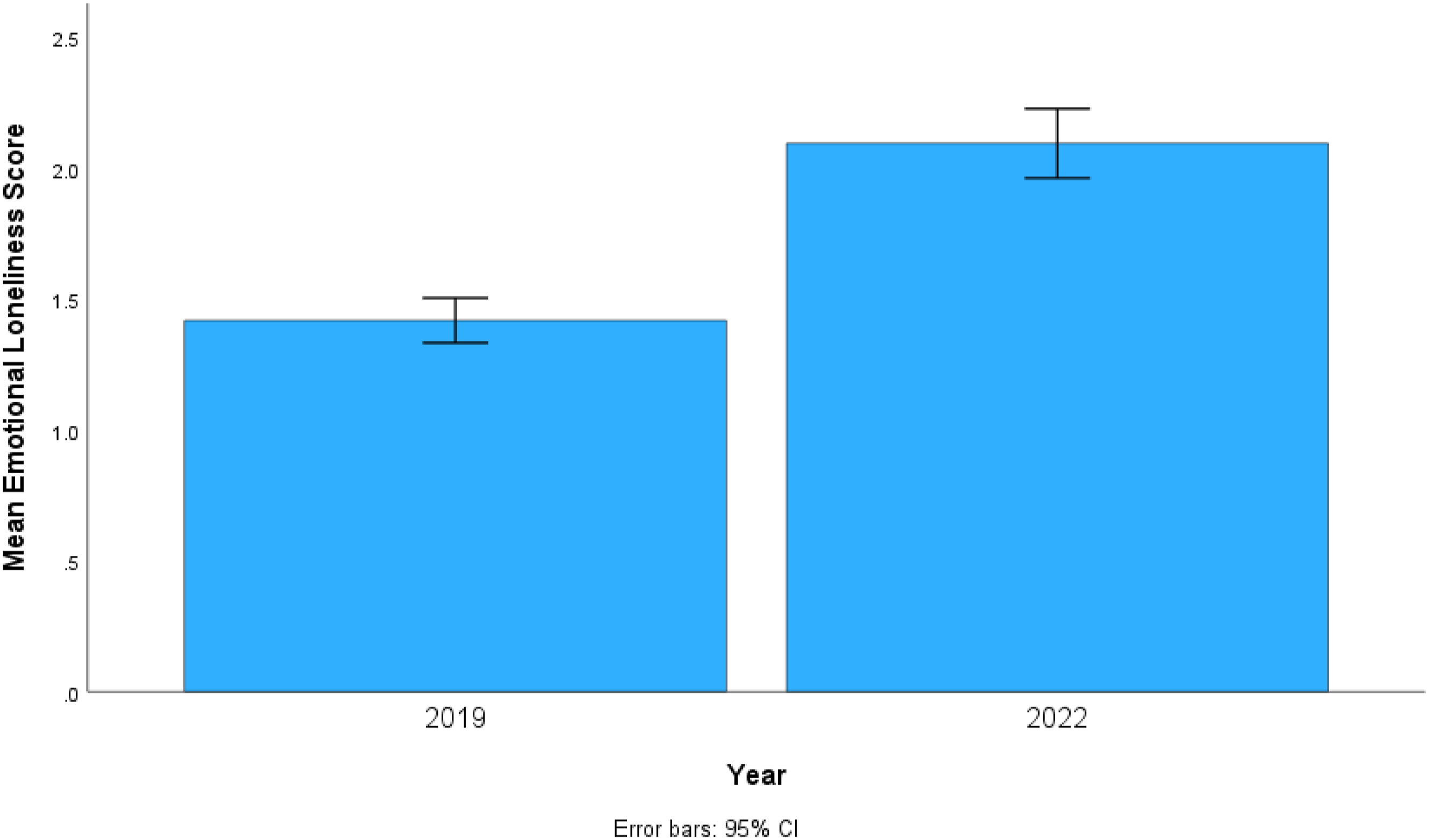
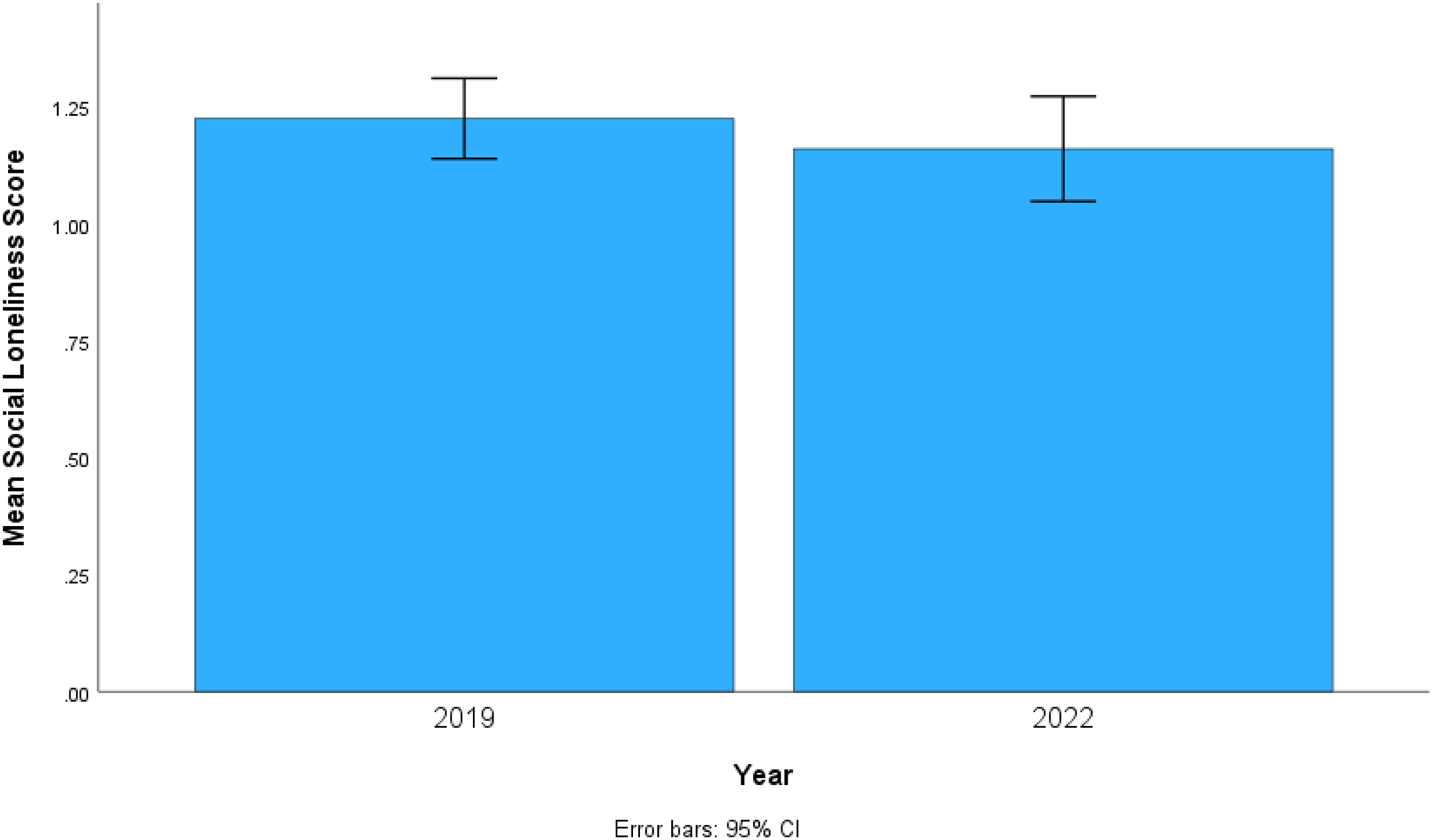
The first part of this section of the analysis compares mean emotional loneliness scores (ranging from 0-6), mean social loneliness scores (ranging from 0-5) and mean loneliness scores (the sum of the former and the latter, ranging from 0-11) between 2019 and 2022. The analyses revealed that between 2019 and 2022 the mean loneliness score increased significantly from 2.65 (SD = 2.33) to 3.26 (SD = 2.73), t(1665) = -8.81, p <. 001 and the mean emotional loneliness score, from 1.42 (SD = 1.39) to 2.10 (SD = 1.73), t(1665) = -4.10, p < .001. The mean social loneliness score, on the other hand, was slightly lower in 2022, 1.16 (SD = 1.47) compared to 2019, 1.23 (SD = 1.39), however this difference is minimal and not significant, t(1665) = .911, p = .232 . The error graphs (Figures 1–3) display the 95% confidence interval of the mean total, mean emotional and mean social loneliness scores respectively. The two confidence intervals for the mean total loneliness scores (Figure 1) and the mean emotional loneliness scores (Figure 2) do not overlap, indicating statistically significant increments between study period 2019 and study period 2022. Differences in mean total loneliness scores 2019 and 2022. Differences in mean emotional loneliness scores 2019 and 2022. Differences in mean social loneliness scores 2019 and 2022.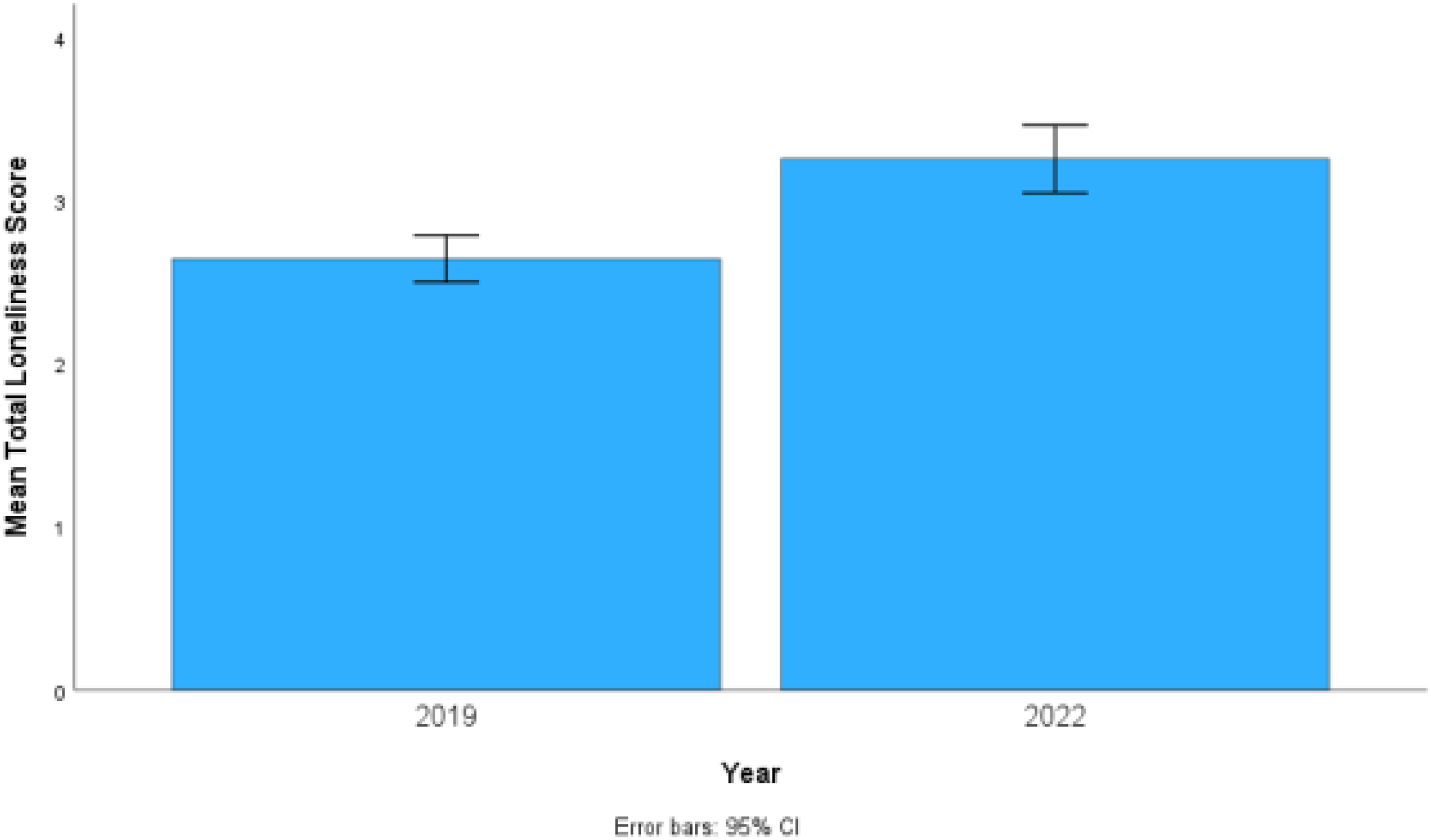
Mean total loneliness scores: Comparison between 2019 and 2022 according to sociodemographic and other characteristics
Differences in mean total loneliness scores between 2019 and 2022 by sociodemographic characteristics (95% confidence interval).
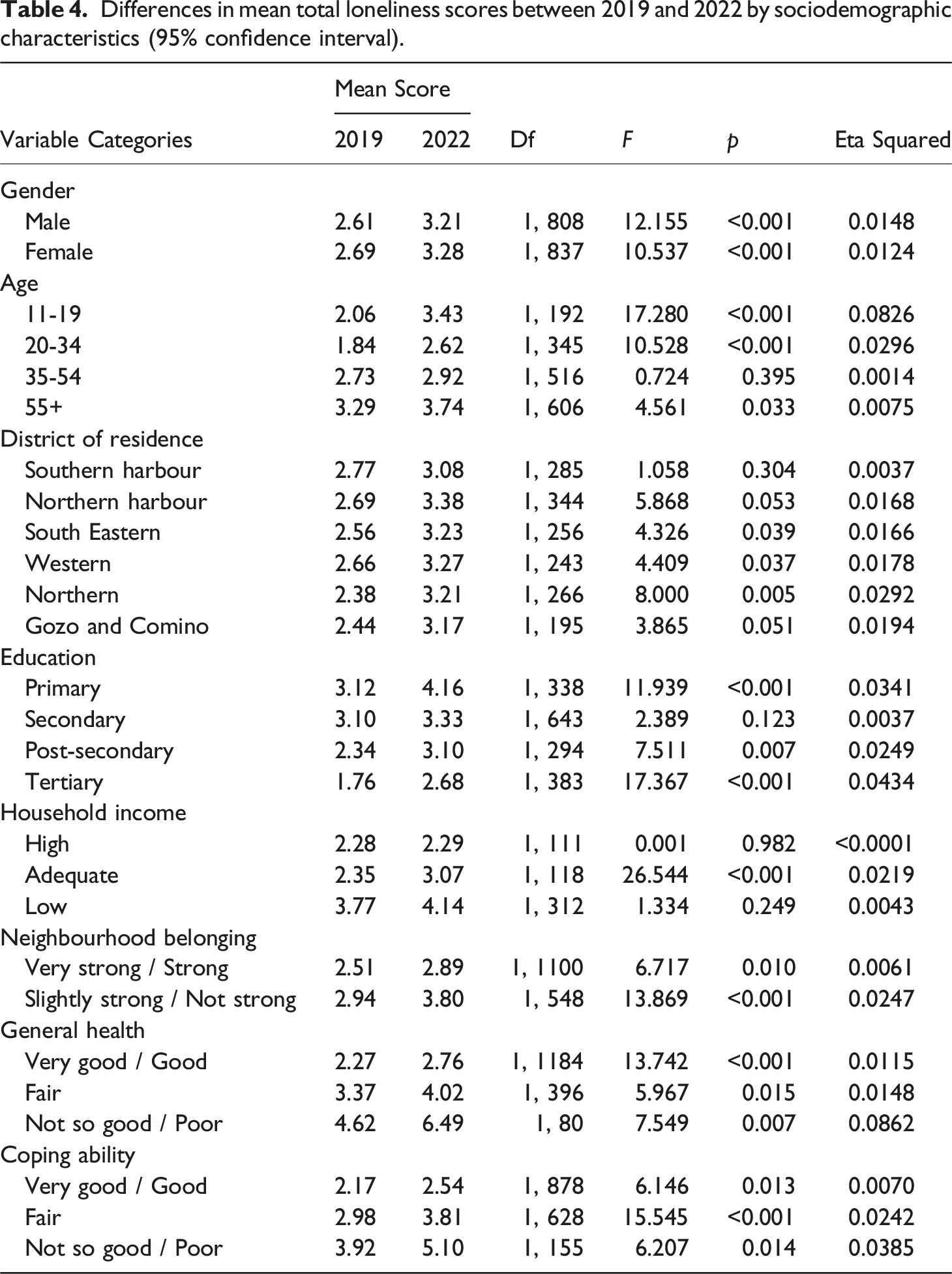
Several Two-Way ANOVA models with interaction were fitted to investigate the interaction effect between the two study periods (2019, 2022) and each of the various sociodemographic explanatory variables. One of the models revealed a significant interaction effect between phase and age-group, F(3, 1659) = 2.921, p = .033. The increment in mean loneliness scores between 2019 and 2022 was considerably larger for younger participants, compared to their older counterparts. Scores increased by 1.370 for the younger group (19 years or less) and this increment was significant, t = −4.157, p < .001. The mean loneliness score increased by 0.447 for the older group (55 years or more) and this increment was significant, t = −2.136, p = .033. Another model revealed a significant interaction effect between phase and health condition, F(2, 1660) = 3.191, p = .041. The increment in the mean loneliness score between 2019 and 2022 was considerably larger for participants reporting poor general health compared to their healthier counterparts. The mean loneliness score increased by 3.400 for participants who reported to be in poor/not so good general health and this increment was significant (t = −2.564, p = .020). On the other hand, mean loneliness scores decreased by 0.375 for participants who reported to be in good health, however this reduction was not significant (t = 1.461, p = .145). Other interaction effects were not found to be significant at the 0.05 level of significance.
Discussion
In the first wave of loneliness research in Malta in 2019, 41.3% of respondents were classified as moderately lonely, with 2.1% of participants classified as severely or very severely lonely. In 2022 the rate of loneliness rose to 54.6% with 5.2% reporting severe or very severe loneliness. These statistically significant changes may reflect increasing social fragmentation. A number of explanations may possibly account for this, including recent urbanization and the changing fabric of Maltese society (ERA, nd; Farrugia, 2010) and changes in family dynamics (Abela, 2016). From 2019 to 2022, COVID-19 and the containment measures were both in full swing. The COVID-19 pandemic increased loneliness among people all across the world (Ernst et al., 2022). In Malta between 2019 and 2022 loneliness increased across most of the socio demographic variables. The interaction effects do however point to some interesting observations.
The increase in total loneliness scores between 2019 and 2022 was statistically significant for both males and females. Gender differences were minimal across all loneliness categories in both 2019 and 2022 and these differences were not statistically significant. The findings are consistent with existing literature which has recently been reported as failing to find consistent patterns of gender differences in loneliness amongst the general population (Pagan, 2020).
This study again identifies periods in the life course that place young people and older people (55+) as being at risk of heightened loneliness when compared with other age groups. The COVID-19 pandemic may have affected these age groups disproportionately, perhaps because elder care facilities were closed to visitors during the pandemic. The lack of visits from family and friends led to increased feelings of isolation among residents. Social interactions are crucial for emotional well-being, and their absence can exacerbate depression and anxiety (Previtali et al., 2020).
It has long been known that marriage is associated with lower experiences of loneliness (Stack, 1998) and while this was confirmed in the current study, it must be noted that the mean loneliness scores varied more throughout age groups than amongst marital status groups; as a result, widows' greater rates of loneliness may be partly explained by their advanced age.
Higher proportions of young people also reported loneliness in the second data collection period than in the first, underscoring the need for social connectedness during this critical juncture in development. Social connections are a key indicator of young people’s emotional state (Sabato et al., 2021).
Increases in loneliness scores between 2019 and 2022 were observed amongst those who had moderate concerns about household income. COVID-19 led to widespread job losses and heightened uncertainty about future employment, particularly impacting the Maltese economy, which relies heavily on tourism. A survey by the National Statistics Office (NSO) in April 2020 revealed that 62% of employed individuals reported their jobs being affected by the pandemic (NSO, 2020, cited in Borg, 2021). Early lockdown measures resulted in a reduction of working hours for three out of ten workers, dropping from an average of 37 hours per week in 2019 to 29 hours in April 2020. The pandemic-induced global economic downturn forced many businesses to downsize, temporarily close, or shut down permanently. It remains unclear why it was those who perceive their income to be moderate who experienced statistically significant increases in loneliness, and not those who perceived their income to be poor. Income inequality has been cited as one condition that contributes to social deprivation and loneliness in 11 European countries (Aartsen et al., 2020). While the relationship between unemployment and loneliness is well established in the literature (Morrish & Medina-Lara, 2021), the direction of the relationship remains unclear (Morrish et al., 2022). Our study found no significant differences between those who were employed and not, albeit the unemployed scoring higher on loneliness and the employed scoring lower. According to data from a British study, lonely young adults were more likely to be unemployed, underprepared for the workforce, and more pessimistic about their employment prospects at age 18 (Matthews et al., 2019). The research on employment and loneliness emphasises the necessity of comprehending the reciprocal relationships between unemployment and loneliness (Matthews et al., 2019). It also underscores the need for policy makers to properly address inequities in individuals' social circumstances, especially in time of emergency as that brought about by the pandemic.
In 2022 loneliness was related to poorer coping ability and decreased positivity about life. Significant increases in total loneliness scores between 2019 and 2022 were primarily observed amongst those with said they coped ‘fairly’. Poor stress management may be exacerbated by loneliness. People who experience social isolation or relationship dissatisfaction may lack the social support that has been shown to be effective in reducing stress (Hostinar et al., 2014).
In 2022 loneliness was also higher amongst those who said their general health was poor or not so good. For people with pre-existing medical issues, COVID-19 has added an additional layer of difficulties (David et al., 2022). During COVID-19, social distancing practices, isolation, and restricted connections with others may have exacerbated feelings of loneliness, particularly for those already suffering with health-related restrictions on their activities and social interactions.
While the increase in loneliness between 2019 and 2022 is small, it could nonetheless have a long-term impact on people’s general wellbeing as well as physical and mental health on the Maltese Islands given that loneliness may result in several adverse physical (Hawkley et al., 2010; Caspi et al., 2006; Luanaigh & Lawlor, 2008), psychological (Cacioppo et al., 2010; Vanhalst et al., 2013) and social outcomes (Victor et al., 2000). The slight increase identified in this study has implications for the planning and implementation of public health policy. While COVID-19 has certainly impacted the experience of social isolation, this increase might also be explained by the rapid social change currently occurring in Maltese communities, leading to shifts in lifestyles, values, and behaviors. According to Cuff et al. (2024), a number of communities in Malta are under increasing pressure due to a range of dynamics emerging from technological growth, globalization, migration, changing family structures and urban development. Hammoud et al. (2021) found an association between the experience of loneliness and environmental variables, including crowdedness, population density, social inclusivity, and contact with nature. In 2022 loneliness was related to weaker sense of neighborhood belonging, reflecting the importance of community.
Limitations
Due to the cross-sectional research design used in this study, no causal connections between loneliness and the sociodemographic variables can be claimed from the data. The study is therefore limited in that it only examines associations between variables without examining the underlying mechanisms for those variables. Additionally, even though the research tool had previously shown to be valid, the current study did not further validate it for usage with the local community. While the sample was stratified based on gender, districts and age, it was not stratified based on income, educational level and health status. People from low socioeconomic groups and people with poor health are less likely to participate in survey research (Korkeila et al., 2001). Household income was not based on income registries but rather participant perception and therefore may be construed as subjectively experienced rather than objectively measured. The study also noted some findings that are inconsistent with previous studies. For example, in the 2022 study single people experienced the least loneliness. Being married has consistently been found to protect against loneliness (Beutel et al., 2017; Diener et al., 2009). This was not borne out in this current study and may be because of the strains COVID-19 placed on marital relationships (Reizer et al., 2020). Research indicates that the quality of one’s marriage is more important than being married, when attempting to explain individual variations in loneliness rates (Hawkley et al., 2008).
Recommendations for further research
Given the significance of age in the experience of loneliness, future loneliness research should try to establish agreed-upon age categories, as variations in the current age classifications prevented in-depth comparison with other studies. Further research is needed to assess the long-term impact of the COVID-19 pandemic on a digitally-connected westernized world that was already experiencing higher levels of social isolation and disconnectedness. Research investigating the value of interventions targeting the interaction of the psychological and social factors that contribute to chronic loneliness is also warranted. Studying loneliness using qualitative research methods can provide valuable insights into the experiences, perceptions, and factors that contribute to loneliness in individuals and to examine the subjective and context-dependent nature of loneliness. Mixed methods designs may also be appropriate in evaluating possible interventions addressing loneliness in Malta and elsewhere. The study omitted questions about sexual orientation, disability, and gender identity, which are significant sociodemographic factors that should be explored in future research.
Recommendations for policy and practice
The findings mentioned above shed light on several social policy-relevant issues. Authorities would be wise to take into account the greater prevalence of loneliness among those who are financially insecure, as well as the negative effects this has on health. This shows that initiatives to address affordable housing and the cost of living may be able to reduce the need for social support and medical care among the population. Given the connections between loneliness and sociodemographic characteristics found in the current study, policy should address the social epidemiology of loneliness, rather than viewing loneliness as an individual issue, addressed by individual solutions. Investing in stronger communities is a valuable approach to combating loneliness and promoting overall well-being through fostering social connections, a sense of belonging, and support systems that can help prevent or alleviate feelings of loneliness. Local government may promote community engagement by encouraging community events and gatherings that facilitate interactions among residents and promote a sense of unity. The social infrastructure, such as, community centers, parks, and public spaces may be further developed to encourage social interactions and provide opportunities for people to come together. Social inclusion programs specifically targeting vulnerable and marginalized populations would foster a culture of acceptance and respect for diversity. The role of family doctors who are closely knit to the Maltese family system are also a contributing factor to supporting people navigating loneliness.
Conclusion
The findings from this study contribute to the understanding of the prevalence and correlates of loneliness as well as to the expanding body of research on the psychological and social repercussions of loneliness. The increase in the prevalence of loneliness from 43.4 % in 2019 to 54.6% in 2022 deserves further in depth investigation. Firstly, the socio-demographic variables where the increases are most marked shed light on certain personal, social and economic conditions that co-exist with increased feelings of loneliness. These factors include the adolescent years and older age, low education levels, being widowed, household income concerns, poor coping skills and weaker sense of neighborhood belonging, Secondly, placed in the context of the COVID-19 pandemic, one needs to understand the impact that the pandemic may have had in exacerbating the feeling of loneliness amongst groups that were possibly more vulnerable and susceptible to the negative psycho-social effects of the lockdowns and social distancing measures.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Open research statement
As part of IARR's encouragement of open research practices, the author(s) have provided the following information: This research was/was not pre-registered. The data used in the research cannot be publicly shared but are available upon request.