
Abstract
This paper explored the determinants of well-being, quality of relationships (QOR), and loneliness among people of Botswana before and during the novel COVID-19 pandemic. It also examined whether there were significant differences between participants’ well-being, loneliness, and QOR before and during the COVID-19 pandemic. Factors associated with the well-being, loneliness, and QOR of the Botswana population before and during the COVID-19 pandemic were also explored. A cross-sectional design was used to collect information on the three variables before and during the COVID-19 pandemic using online platforms. Convenience sampling was used to recruit participants (N = 422) using the WHO-5, Three-Item Loneliness Scale, and the Relationship Quality Index (RQI). Data were analyzed using bivariate and multivariate mixed-effects linear models. Age, relationship status, concern about own and family health, difficulty switching on and off media reporting on COVID, change in lifestyle, participation in sports, and resting were significantly associated with well-being (p < .001) and loneliness (p < .05). Sleep was associated with QOR. There were significant differences in the well-being, QOR, and loneliness scores before COVID-19 conditions and during COVID-19 conditions. Stakeholders should take cognizance of the impact of predictor variables on well-being and loneliness to mitigate the impact of current and future pandemics.
Background
Following its outbreak in December 2019 in Wuhan, China (Chodkiewicz et al., 2020), the novel coronavirus disease (COVID-19) quickly spread around the globe (Jebril, 2020). It is now estimated that over two million people worldwide have lost their lives to COVID-19 since its first outbreak (WHO, 2021). On March 11, 2020, the WHO declared COVID-19 a global pandemic (WHO, 2020) as its incident rates were rapidly increasing across the globe. Consequently, many governments were forced to take stringent precautionary measures to mitigate its rapid spread (Jebril, 2020; Zacher & Rudolph, 2020).
The most common of these measures were national lockdowns, social distancing, and quarantines (Chodkiewicz et al., 2020). These restrictions, while helpful, have been linked to an increase in various negative mental health outcomes (Killgore et al., 2021; Rossi et al., 2020). Case in point, in their meta-analysis of articles on the effect of quarantines on mental health, Jin et al. (2021) found that the longer the quarantine duration, the higher the levels of depression, anxiety, and stress. Similarly, lockdowns have been found to have the same effect on levels of depression, anxiety, and stress (Pieh et al., 2021). Like many other countries, Botswana entered a lockdown of its own on April 2nd, 2020, during which people’s movement was highly restricted (Government of Botswana, 2020). Similar to observations made in other countries, these restrictions could have impacted the mental health of the people of Botswana by increasing loneliness and adversely affecting their well-being and quality of relationships.
However, it was unclear from the literature in Botswana how well-being, QOR, and loneliness have been impacted. A search across databases revealed that there have not been any identifiable studies conducted in Botswana to explore the changes in well-being, loneliness, and QOR before and during the COVID-19 pandemic. Previous research on loneliness in the UK (Li & Wang, 2020), Israel (Palgi et al., 2020), and Brazil (Ribeiro et al., 2017) provides evidence of the impact of COVID-19 precautionary measures. The same studies also showed the association between loneliness and poor mental health. The same applies to a systematic review of well-being (Brooks et al., 2020) and research on the quality of relationships (QOR) conducted by Pieh et al. (2020) in Austria and by Biddle et al. (2020) in Australia.
On November 12th, 2021, the Botswana Government reported on its Facebook page that there were 194,129 confirmed cases, 1,095 positive cases, 190,863 recovered cases, 2,416 deceased, and that 17% of the population had been fully vaccinated. Zacher and Rudolph (2020) asserted that while the COVID-19 pandemic is a medical and economic crisis, it also has a psychological dimension that poses a threat to key facets of people’s subjective well-being. Hotopf et al. (2020) posited that the effects of the COVID-19 pandemic on well-being are likely to be profound and long-lasting. In Botswana, lower well-being is highly correlated to poor health and lower resilience, particularly in older people (Mhaka-Mutepfa & Wright, 2022). WHO (2013) reiterated the foregoing finding by stating that there can be no good health without high well-being; individuals’ ability to function productively and to cope with life’s inevitable, stressful, and deleterious situations is determined by their level of well-being. Thus, people might not be able to cope with the impact of the COVID-19 pandemic if their well-being and resilience are compromised (Stieger et al., 2021).
Long-term loneliness is associated with an increased risk of mental health problems (e.g., depression, anxiety, and increased stress), symptomatology, and increased substance use (Horigian et al., 2021; Pieh et al., 2020). Compared to physical health, loneliness has been found to have a larger effect on well-being and mental health (Park et al., 2020). Additionally, the measures implemented to curb the spread of COVID-19 have impacted QOR. For instance, these measures have been associated with conflict in parent-child relationships (Fore, 2020) and gender-based violence (GBV) (John et al., 2021). It was reported that shelters and support centers in Botswana were housing more women and children during the pandemic (UNFPA, 2020) because of the increase in GBV, which could have impacted their well-being. GBV was found to affect QOR in previous studies in Zimbabwe (Mhaka-Mutepfa, 2009) and Iran (Asadi et al., 2017). Additionally, researchers in India reported a disturbing rise in the incidents of GBV during pandemics and epidemics (Mittal & Singh, 2020) which led to a deterioration of family relationships and consequently, poor well-being. However, it should be noted that poor QOR does not always imply GBV.
To fill the gap that exists in the literature for well-being, loneliness, and QOR among people of Botswana, a part of the study investigated these three constructs before and during the novel COVID-19 pandemic. As such, the objectives of the current study were to (1) establish whether there were significant differences between participants’ well-being, loneliness, and QOR before and during the COVID-19 pandemic, and (2) explore associated factors that influenced the well-being, loneliness, and QOR of the participants before and during the COVID-19 pandemic.
Method
A cross-sectional snowballing design was used to collect information on the well-being, QOR, and loneliness of participants before and during the COVID pandemic in July 2020 (about 2 months after the national lockdown was implemented in Botswana). The participants responded to the survey with their recollections of how they felt both before the pandemic arrived in Botswana and after the implementation of the subsequent national lockdown. Using online surveys via social media platforms, the researchers and the respondents had convenience concerning where and when they could participate.
Population and Sample
This study was part of a large research project comprising 12 consortium members in the Global South and was trialed in Rwanda and Uganda. For this paper, the target population was the adult population of Botswana, 18 years and above. Individuals below the age of 18 were excluded as they would have needed parental consent. A questionnaire link, https://www.icpcovid.com/en/form/pfcc, was shared across various media (e.g., email, WhatsApp, and Facebook). Participants were asked to share the link with members of their social circles (snowballing technique).
Instruments
The online questionnaire that was used consisted of 14 sections including informed consent, demographics, different scales, and a personalized feedback section. The instruments used for the current paper included the Three-Item Loneliness Scale (TILS), the Relationship Quality Index (RQI), and the WHO-5 Well-Being Index (WHO-5, 1998 version). The responses on these instruments provided information on the levels of well-being, loneliness, and QOR. Data collected by the different scales included information on COVID-19, coping, well-being, relationships, time spending patterns, social situation, how the COVID-19 pandemic was impacting the social relationships of participants, and others. Participants chose whether to use the English version or the one converted into the local language (Setswana) for this study. The Setswana version was back-translated by a different person to ensure reliability and consistency.
WHO-5 Well-Being Index
The WHO-5 (WHO, 1998) is a five-item scale that measures subjective well-being (Topp et al., 2015). While the WHO-5 assesses respondents’ well-being over the last 2 weeks (Guðmundsdóttir et al., 2014; Topp et al., 2015), the research project on which this paper is based asked the respondents about their well-being before the pandemic and over the last 2 weeks before participating in the study during the pandemic. As a result, the items in the scale were phrased in the present tense and adapted to “I feel cheerful and in good spirits,”“I feel calm and relaxed,”“I feel active and vigorous,”“I wake up feeling refreshed and rested,” and “My day is filled with things that interest me” to allow for the simultaneous measurement of well-being pre-and-during COVID-19 conditions.
The scale uses a six-point Likert-type scale with the response items 0 = “At no time,” 1 = “Some of the time,” 2 = “Less than half of the time,” 3 = “More than half of the time,” 4 = “Most of the time,” and 5 = “All of the time” (Topp et al., 2015). In scoring, the responses were summed to a total raw score ranging from zero (absence of well-being) to 25 (maximal well-being). Previously reported internal consistencies of the scale were good. For instance, .86 (Omani-Samani et al., 2019) and .94 (Ghazisaeedi et al., 2021). Cronbach alpha for the current study was equal to .87, also suggesting good internal consistency.
Three-Item Loneliness Scale (TILS)
The TILS used was adapted from the Revised UCLA Loneliness Scale (see Hughes et al., 2004; Pheko et al., 2023; Russell et al., 1978). Details on the use of the TILS have been given in a paper originating from the same study (Pheko et al., 2023). The scale has the response items 1 = “Hardly ever,” 2 = “Some of the time,” and 3 = “Often” thus the total scores range from three to nine and the higher the score, the greater the level of loneliness (Hughes et al., 2004). The TILS is reliable with an alpha of .75 (Garg et al., 2023) and .82 (Trucharte et al., 2021). For the current study, the Cronbach alpha was .78.
Relationship Quality Index
The RQI, which was previously adapted from the Quality of Marriage Index (QMI) (see Norton, 1983), was used to measure the relationship quality of both married and cohabiting participants. QMI is a reliable measure with the internal consistency of alphas as high as .97 (Heyman et al., 1994). The RQI has the following five items: “We have a good relationship,”“My relationship with my partner is very stable,”“My relationship with my partner is strong,”“My relationship with my partner makes me happy” and “I really feel like part of a team with my partner.” The scale uses a seven-point Likert scale with the response items 1 = “Very strongly disagree,” to 7 = “Very strongly agree” (Norton, 1983). The scores range from five to 35 in the RQI. Similar to the QMI, higher scores indicated greater relationship quality (Norton, 1983). The RQI is a realizable measure revealing an internal consistency of .94 (Day & Sanders, 2018). Similarly, RQI in this study had a good internal consistency as reflected by a Cronbach alpha of .90.
Statistical Analysis
The data collected was analyzed using Stata software (Stata Corp. 2017. Stata Statistical Software: Release 13. College Station, TX: Stata Corp LP). The current study’s outcome variables were subjective well-being; loneliness and QOR. Predictors included socio-demographics, whether people knew people who were infected and/or people who died from the pandemic, and others. Assumptions of normality and homoscedasticity were met for all the outcome variables therefore parametric tests were used for analysis. The variance inflation factors (VIF) were less than 3 for most variables. Descriptive statistics (e.g., frequencies, percentages, mean, and standard deviation [SD]) were used to summarize the characteristics of the sample. Paired samples t-tests were used to establish whether there were significant differences in the mean scores for the WHO-5, TILS, and the RQI before and during the COVID-19 pandemic.
The relationship between the change in the outcome variables due to the COVID-19 pandemic and explanatory factors was evaluated using separate bivariate linear mixed effect models with a restricted maximum likelihood (RMEL). The models included individual-level random effects and considered exchangeable correlation structures. The three final multivariate linear mixed effect models for the three outcome variables included the significant explanatory variables at the 5% level of significance in bivariate models. Each model included random effects, outcome variables, and explanatory variables as the fixed effect of time and their interactions. By using the Bonferroni correction, the adjusted estimates of the outcome variables were compared to the explanatory factors. Statistical significance of the associations was considered for p-values less than .05.
Results
General Information of Participants
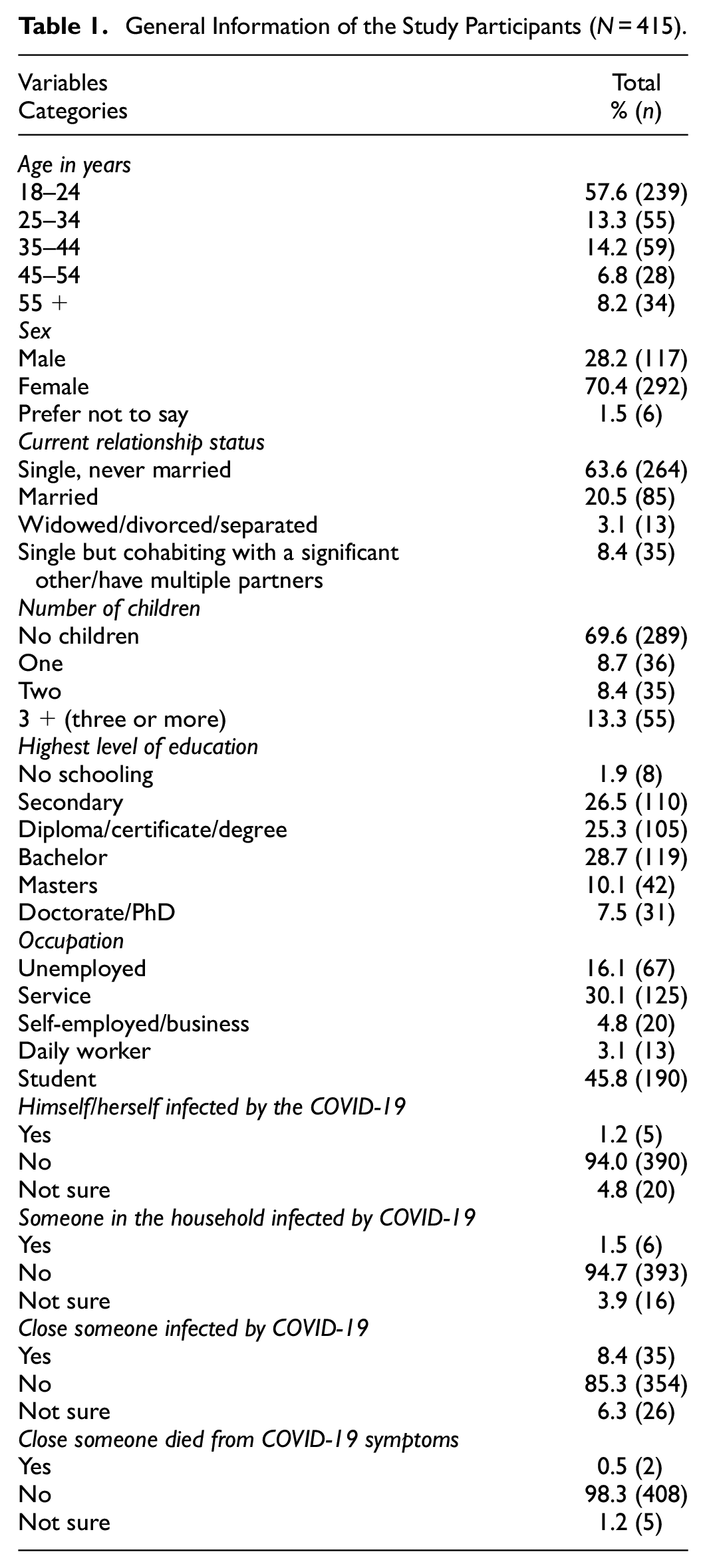
A total of 239 (57.6%) participants in the total sample were aged 18 to 24 years, 292 (70.4%) were female, and 264 (63.6%) were single (see Table 1 for the rest of the demographics). Among all of the study participants, 196 (47.2%) reported they were exceedingly concerned about their health and family health, 151 (36.4%) reported finding it neither easy nor difficult to switch off from media sources, and 191 (46.0%) reported maintaining approximately the same lifestyle since the COVID-19 pandemic started.
General Information of the Study Participants (N = 415).
Well-Being, Loneliness, and Quality of Relationships Before and During COVID-19
Comparisons of mean scores for outcome variables before and during the COVID-19 pandemic are shown in Table 2. The scores indicated lower well-being scores during the COVID-19 pandemic (M = 9.7, SD = 5.4) than before the pandemic (M = 12.9, SD = 5.8). There was also a significant increase in loneliness scores during the COVID-19 pandemic; t(408) = −7.5, p < .001. Additionally, the QOR scores decreased significantly during the pandemic; t(118) = 2.4, p < .001 (see Table 2). Cohen’s d values also showed that there were medium to large effects (0.6) on mean score differences for well-being and small effects for QOR (0.2). Cohen’s d values for loneliness were statistically significant, however, they showed negligible mean score differences (0.1) (see Table 2).
Comparison of Mean Scores for Wellbeing, Loneliness, and QOR Between “Before and During COVID-19.”

Note. ap-value obtained from paired t-test.
Associations of Explanatory Variables with Well-Being, Loneliness, and QOR
Multivariate Mixed effects linear model analysis of well-being, loneliness, and QOR was used to explore associations of explanatory variables with each of the outcome variables (refer to Tables 3 and 4; Supplemental Table 6). Study participants in the age group 18 to 24 years (Mean difference (MD) = 3.5; Confidence Interval (CI) = [2.1, 4.8]), 35 to 44 years (MD = 3.7; CI = [1.0, 6.4]) and more than 55 years (MD = 4.0; CI = [0.1. 7.8]) had significantly lower well-being scores during the COVID-19 pandemic compared to before the pandemic. For current relationship status, the mean difference in well-being score was notably lower for everyone, most notably those that were married (MD = 2.8; CI = [0, 5.5]) amid the COVID-19 pandemic compared to before the pandemic (see Table 3 for the rest of the means). For own and family health concerns, trouble switching off from any media on COVID-19, and other explanatory variables the well-being mean scores were lower than before the COVID-19 pandemic (see Table 3). The lowest mean differences among different categories were statistically significant over the two-time points (see Table 3).
Multivariate Mixed Effects Linear Model Analysis to Explore Adjusted Marginal Effect of Well-Being According to Different Characteristics of the Study Participants.
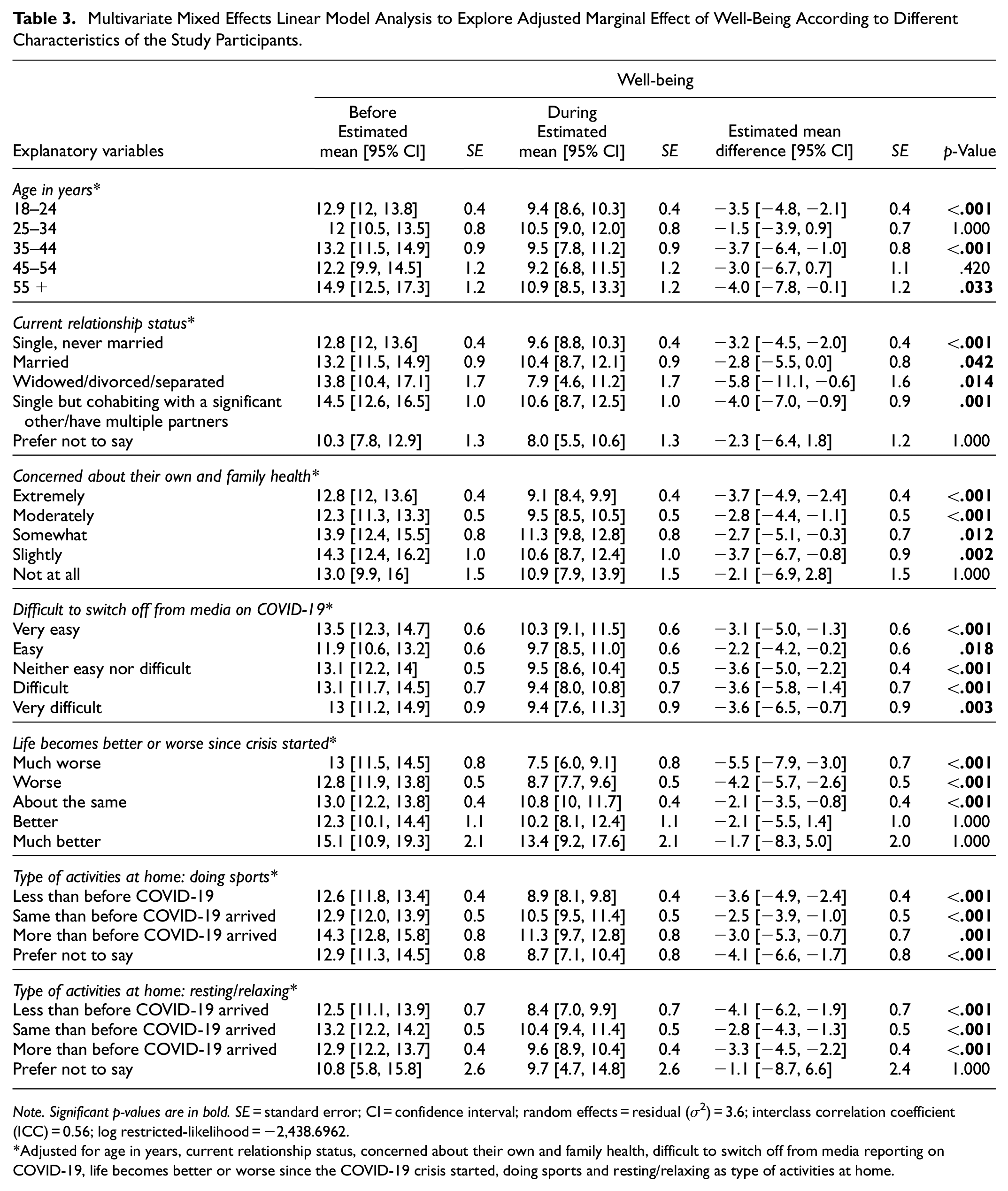
Note. Significant p-values are in bold. SE = standard error; CI = confidence interval; random effects = residual (σ2) = 3.6; interclass correlation coefficient (ICC) = 0.56; log restricted-likelihood = −2,438.6962.
Adjusted for age in years, current relationship status, concerned about their own and family health, difficult to switch off from media reporting on COVID-19, life becomes better or worse since the COVID-19 crisis started, doing sports and resting/relaxing as type of activities at home.
Multivariate Mixed Effects Linear Model Analysis to Explore Adjusted Marginal Effect of Loneliness According to Different Characteristics of the Study Participants.

Note. Significant p-values are in bold. SE = standard error; CI = confidence interval; random effects: residual (σ2) = 1.2; interclass correlation coefficient (ICC) = 0.73; Log restricted-likelihood = −1,669.7823.
Adjusted for age in years, highest level of education, occupation, concerned about their own health and family health, life becomes better or worse since the COVID-19 crisis, sleeping as type of activities at home.
In Table 4, the estimated mean differences for loneliness before the COVID-19 pandemic for 18 to 24-year-olds (MD = 7.1; CI = [6.7, 7.5]), those with secondary education (MD = 7.3; CI = [6.8, 7.8]), those in possession of diplomas and bachelor degrees, the unemployed, and students (MD = 6.8; CI = [6.3, 7.2]) increased during the pandemic but only the 18 to 24-year-olds were significantly associated with loneliness (see Table 4).
The estimated mean differences for loneliness among participants who were extremely and moderately concerned about their own and family health increased significantly during the COVID-19 pandemic (see Table 4). Similarly, estimated mean scores for lifestyle (much worse to about the same) also significantly increased loneliness scores during the COVID-19 pandemic. Table 4 displays that sleeping modes before and during the pandemic were statistically significant (p < .05).
However multivariate mixed-effects linear model analysis between predictors and QOR before and during the COVID-19 pandemic did not show any significant differences and was therefore not included in the current paper (Supplemental Table 6).
Discussion
Wellbeing, Loneliness, and Quality of Relationships Before and During COVID-19
The paired-sample t-test revealed statistically significant decreases in well-being and QOR and a statistically significant increase in loneliness during the COVID-19 pandemic. The findings also indicated that the pandemic harmed these important aspects of mental health among people living in Botswana, which is similar to previous results in New Zealand, the USA, and Sweden (Kivi et al., 2020; Luchetti et al., 2020; Sibley et al., 2020). The change in scores before and during the COVID-19 pandemic will be discussed in detail in the sections that follow.
Well-Being Scores Before and During COVID-19 and the Associations of Explanatory Variables with Well-Being
The multivariate mixed-effect linear model revealed that the difference in well-being scores before and during the COVID-19 pandemic among the participants was statistically significant. The findings that well-being scores decreased during the COVID-19 pandemic are consistent with previous findings (Brooks et al., 2020), showing the deleterious effects of the disease. Life satisfaction might have been lower amongst those who reported that their life became worse during the COVID-19 pandemic, thus lowering their well-being. It is interesting that even those that reported life to be the same as before the COVID-19 pandemic had a reduction in their well-being scores during the pandemic, also suggesting the mental health impact of the disease. The foregoing finding could be further explored in future research.
With regards to associations, age, current relationship status, concern about their own health and family health, difficulty switching off from media, life becoming better or worse since the COVID-19 crisis, sports, and resting/relaxing had a significant effect on well-being. The multivariate mixed-effects linear model analysis also revealed that the 18 to 24, 35 to 44 and over 55 age groups were statistically significant with lower well-being during the COVID-19 pandemic than before the pandemic. This is in tandem with Losada-Baltar et al.’s (2020) findings that younger people in Spain were more likely to be distressed in lockdown as even those that are older had reduced well-being. However, the findings in current study might have been affected by the fact that there were very few older adults who took part in the study. Future studies could look at older people to confirm this finding. However, older people in Botswana were found to have lower well-being even before the pandemic (Mhaka-Mutepfa & Wright, 2022).
Participants who indicated they were concerned about their health and that of their families had significantly lower well-being during the COVID-19 pandemic. This is not surprising as health is a major aspect of quality of life (QOL) and life satisfaction (Dodgee et al., 2012; Mhaka-Mutepfa, 2018; Mhaka-Mutepfa & Wright, 2022). While a majority of the participants had not contracted the virus and did not have loved ones who had died yet, knowledge, uncertainties, and perceptions of the huge health risks might have been enough to negatively impact well-being. Knowledge of the health risks could have been further compounded by the constant media coverage of the pandemic which included statistics of new cases and deaths due to the virus.
While it could be expected that those that found it difficult to switch off from media covering COVID-19 would have significantly lower well-being, everyone had significantly lower well-being. Perhaps this resulted from the fact that even those that could switch off from media coverage of COVID-19 could still have been exposed to information, uncertainties, and panic concerning COVID-19 through their social circles even when they had switched off from media covering the pandemic. Additionally, it was a mammoth task to succeed in switching off from media since a lot of advocacy, promotion, and safety measures information was constantly being disseminated on various platforms.
Loneliness Scores Before and During the COVID-19 Pandemic and Associations of Explanatory Variables with Loneliness
Loneliness scores increased during the COVID-19 pandemic in the current study similar to previous studies (Li & Wang, 2020; Palgi et al., 2020; Ribeiro et al., 2017). Young adults and older adults were the hardest hit, particularly in the previous studies. With regards to associations, age, level of education, occupation, concern about own health and family health, life becoming better or worse since the COVID-19 crisis and sleeping had a significant effect on loneliness. Like findings by Losada-Baltar et al. (2020), the multivariate mixed-effects linear model analysis in the current study on loneliness indicated that the young, who mostly identified as students, those with lower education, and the unemployed had statistically significant increases in loneliness during the pandemic. The students were cut off from fellow scholars during the lockdowns and other forms of movement restrictions thus they felt isolated and lonely. While the business world swiftly initiated remote work, academic institutions in Botswana did not rapidly initiate online learning. Even if they had, there would still have been limited physical contact among students. Therefore, students did not have an opportunity to relate with their peers during the lockdowns as those who were engaged in some form of employment. This could also help to explain why the unemployed also had significant increases in loneliness.
Those that were concerned about their health or that of their family members experienced statistically significant changes in loneliness during the COVID-19 pandemic as did those who reported that their life had become worse or was about the same. The movement restrictions in Botswana, like the rest of the world, were implemented to curb the spread of COVID-19. Thus, if one is concerned for one’s own and family’s health, one is likely to observe movement restrictions which would lead to isolation from other members of their social circles and, in turn, increase loneliness. Associations of predictor variables and QOR will be discussed below.
QOR Scores Before and During the COVID-19 Pandemic and Associations of Explanatory Variables with QOR
QOR scores decreased during the COVID-19 pandemic. However, predictor variables were not associated with QOR (see Supplemental Table 3) except for sleep (p = .043). As displayed in Supplemental Table 6, there was no predictor variable that was significantly associated with QOR. These findings are inconsistent with previous studies that found associations between various predictor variables and QOR (Biddle et al., 2020; Pieh et al., 2020). Other previous findings also revealed that couples who reported poor coping and high levels of conflict experienced reduced ‘satisfaction and adaptive attributions, modestly decreasing already distressed functioning’ (Williamson, 2020, p. 1486). Good QOR was found to be a protective factor and poor QOR was a risk factor (Pieh et al., 2020), even in the current study. However, the lack of significant associations in the current study may be due to a sampling issue. The sample size for participants in relationships was very small, masking the associations. It is also possible that the female participants in the current study may not have been exposed to poor QOR as most of them were single. More research on this issue is required particularly for married people or intimate partners in Botswana.
Lack of participation in activities like sports, exercising, lack of sleep, and others were found to impact loneliness and well-being. Sleep was associated with QOR and loneliness. The impact of physical activity or sport and sleep on loneliness, QOR, and well-being will be discussed below.
Impact of Sport and Sleep on the Three Outcome Variables
Physical activity was associated with loneliness and well-being in the current study. From time immemorial, physical activity has been highly correlated with health and well-being and improvement in mental health (Edwards et al., 2005; Watson & Koontz, 2020). Improvement in mental health suggests a reduction in symptoms of depression, anxiety, pain, and loneliness. Physical activities also improve focus, school performance, sleep, and energy levels (Watson & Koontz, 2020). Edwards et al. (2005) also found that exercise improves all the dimensions of well-being. Like the previous findings, the current study justifies the impact of exercise on well-being as all exercise facilities were closed and people were not allowed to jog or take walks during the lockdowns. Participants who engaged in less sport during the COVID-19 pandemic had less well-being than those who engaged in sports at more or the same level as before the pandemic.
Social cohesion, which contributes to the social and emotional enjoyment of fans and supporters’ identification with sports persons was also interrupted (United Nations, 2020). Sport brings divided communities together even during times of conflict thereby promoting mental health. The complaints raised by tennis players during the Australian open quarantine attest to these findings (BBC Sport News, January 18, 2020). Thus, due to lack of exercise, participants and supporters became more irritable and petulant leading to poor QOR, changes in sleep patterns, higher levels of loneliness, and lower well-being. These attributes have a severe effect on mental health and well-being, hence the need for physical activity even under difficult circumstances.
Sleep was also associated with loneliness and QOR in the current study (Supplemental Table 3), a finding which supports Chow’s (2020) assertions. Lack of sleep is caused by negative thinking and emotional vulnerability (Chow, 2020), which has become synonymous with the pandemic. Cognitive behavioural therapy (CBT) could be used to allay uncertainties and fears as these lead to anxiety and depression (Mhaka-Mutepfa & Wright, 2022). Art therapy can also be effective at improving various aspects of mental health, sleep quality, and psychological well-being.
Limitations
While the online-survey method that the research study used provided the advantage of convenience and flexibility (Evans & Mathur, 2018) as well as safety in these trying times, this method of data collection excluded members of the population who did not have access to the internet from participating in the research and thus they were underrepresented. Therefore, the findings cannot be generalized. In addition, the cross-sectional design of the study does not provide the opportunity to see changes in well-being, loneliness, and QOR as the pandemic continues. Longitudinal research should be conducted in the future, which will include previously excluded members of the population, and identify changes in these variables over time since internet access and use have been growing ever since data collection. The demographics were skewed, particularly age, marital status, gender, and the number of children, this may have affected the associations. Additionally, retrospective questions, those that referred to a time before COVID-19 arrived in the country, are affected by the limitations of human memory. The emotional states of experiencing the impact of the COVID-19 pandemic first-hand may influence the way participants may have envisaged the pandemic. For example, they may think of the past as a much better time due to the pandemic itself, rather than it truly being a better time.
Conclusion
Results revealed statistically significant decreases in well-being, and QOR and a statistically significant increase in loneliness during the COVID-19 pandemic. Age, current relationship status, concern about own health and family health, difficulty switching off from media, life becoming better or worse since the COVID-19 crisis, sports, and resting/relaxing had a significant effect on well-being, and loneliness but not QOR. Only sleep was associated with QOR, maybe due to measurement errors and a small sample size for those in relationships that took part in the study. Stakeholders should take cognizance of the associations’ impact on mental health when effecting restrictions during the pandemic as this influences well-being, QOR, and loneliness in their populace as reported in this paper. Lockdowns lead to mental health struggles especially in low to middle-income countries (LMICs) like Botswana, which impacts QOL and well-being and thus should be debated adequately before implementation. People are social beings and failure to access social networks may have negative repercussions which need to be addressed.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440241251540 – Supplemental material for Well-Being, Loneliness, and Quality of Relationships Before and During the COVID-19 Pandemic in Botswana
Supplemental material, sj-docx-1-sgo-10.1177_21582440241251540 for Well-Being, Loneliness, and Quality of Relationships Before and During the COVID-19 Pandemic in Botswana by Magen Mhaka-Mutepfa, Md Jabuyer Biswas, Leonne M. Mfolwe, Kesego D. Mathoothe and M. Tasdik Hasan in SAGE Open
Supplemental Material
sj-docx-2-sgo-10.1177_21582440241251540 – Supplemental material for Well-Being, Loneliness, and Quality of Relationships Before and During the COVID-19 Pandemic in Botswana
Supplemental material, sj-docx-2-sgo-10.1177_21582440241251540 for Well-Being, Loneliness, and Quality of Relationships Before and During the COVID-19 Pandemic in Botswana by Magen Mhaka-Mutepfa, Md Jabuyer Biswas, Leonne M. Mfolwe, Kesego D. Mathoothe and M. Tasdik Hasan in SAGE Open
Footnotes
Acknowledgements
We would like to acknowledge the Rwanda team for trailing the questionnaire and all the people who took part in the study.
Correction (August 2024):
Article updated to correct the affiliation of M. Tasdik Hasan to “Action Lab, Faculty of Information Technology, Monash University, Melbourne, Australia”
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval to conduct the study was obtained from the Institutional Review Board (IRB) of the University of (redacted) and the local government. All ethical considerations were on the first page of the questionnaire: informed consent was provided with information on the purpose of the study, confidentiality, anonymity, dissemination of results, participants’ rights, and the contact details of the principal investigator and the IRB.
Supplemental Material
Supplemental material for this article is available online.
Data Availability Statement
The data that support the findings of this study are available upon request.