
Abstract
Sexuality education (SE) can be acquired through different sources. In a cross-sectional online study with Spanish and Portuguese participants (N = 595), we examined differences between formal traditional sources (i.e., mandatory SE received in schools), formal modern sources (e.g., SE received in courses), informal traditional sources (e.g., talks with friends and family), and informal modern sources (e.g., pornography and online content) and their contribution to sexual health and well-being outcomes. Results showed that sexual and reproductive health were among the most addressed topics across all sources. Nearly all participants received SE from informal sources, whereas more than two-thirds received SE from formal traditional sources. Results of a linear regression model showed that participants who perceived more influence from formal traditional sources reported using condoms more often, were more focused on disease prevention, and enacted more sexual health communication, but were also less sex-positive. Participants who perceived more influence from both types of informal sources attributed more importance to SE topics but reported having condomless sex more frequently and were more focused on pleasure promotion. Still, participants who perceived more influence from informal traditional sources also endorsed more internal/external consent, were more sexually satisfied, were more sex-positive, and enacted more sexual health practices. Lastly, participants who perceived more influence from informal modern sources were also more likely to have been diagnosed with a sexually transmitted infection. Only a small proportion of participants received SE from formal modern sources and had to be excluded from this analysis. Some differences between Spain and Portugal are discussed. Taken together, our findings highlight the need to consider different sources for a more comprehensive and inclusive SE, in articulation with sociocultural and political contexts.
Keywords
Introduction
The World Health Organization (2006) defines sexual health as a state of physical, emotional, mental, and social well-being related to sexuality beyond the absence of diseases, dysfunctions, or infirmities. Sexual health and well-being are intrinsically linked to a positive and respectful approach to sexuality and sexual relationships, and pleasurable and safer sexual experiences. Hence, access to accurate and comprehensive sexuality education (SE) is crucial for any strategy aimed at improving sexual health and well-being (Braeken & Cardinal, 2008; Mullinax et al., 2017; Vanwesenbeeck, 2020). SE should focus on behavioral, emotional, and relational aspects of sexuality, sexual pleasure, relationship dynamics, and sexual rights (Cacciatore et al., 2019; Ford et al., 2019; Hirst, 2013; Mitchell et al., 2021; Sladden et al., 2021). This comprehensive approach aims to equip people (particularly children and younger people) with the proper knowledge and tools to make informed choices, value themselves and their dignity, have respectful relationships with others, and understand the consequences of their sexual decisions and behaviors (European Expert Group on Sexuality Education, 2016; Michielsen & Ivanova, 2022; UNFPA, 2018).
Evidence from different countries has consistently shown that taking part in SE programs increases sexual literacy and sexual empowerment, facilitates sexual decision-making, and helps people to be more attentive to, and respectful of, their sexual partners (for reviews, see Goldfarb & Lieberman, 2021; Montgomery & Knerr, 2018; Patton et al., 2016). However, differences in education policies between (and within) countries can have distinct impacts on sexual health and well-being outcomes (Ketting et al., 2021; Mullinax et al., 2017; Parker et al., 2009). For example, Weaver and colleagues (2005) found that countries with more (vs. less) inclusive and comprehensive approaches to SE (e.g., the Netherlands) tend to have higher rates of condom use at first intercourse and lower rates of sexually transmitted infections (STIs). Still, young people consider that SE during mandatory school years fails to offer a sex-positive approach or address topics related to sexual consent and pleasure (Mark et al., 2021; Waling et al., 2021; Willis et al., 2019). Hence, people often rely on their peers, family, social media, and other readily available sources to retrieve this knowledge (Bouclaous et al., 2021; Richmond & Peterson, 2020).
The current cross-sectional study aimed to understand whether different SE sources are associated with distinct outcomes pertaining to sexual health practices (e.g., condomless sex), sexual well-being outcomes (e.g., sexual satisfaction), and sexual rights (e.g., endorsement of sexual consent). We further explored differences between Spain and Portugal, two countries largely underrepresented in the international scientific community.
Formal sexuality education in schools
Similar political regimes have influenced the development of SE over the years in Spain and Portugal. Both countries faced periods of dictatorship and repression characterized by limited freedom and rights, in which conservative views were predominant (for reviews, see Cunha-Oliveira et al., 2021; Martínez et al., 2012; Matos et al., 2014; Picken, 2020). In Spain, the government approved the right to education in 1978 and the legal framework regulating SE in 1990. Legislation changes have forced both advancements and setbacks over the years, often influenced by the political ideology of the governing bodies. Control over education was transferred to regional governments in 2000. The reform that occurred in 2013 to improve the quality of education, however, did not include SE as mandatory or optional in schools, nor was it explicitly part of the basic competencies that students should acquire. Faced with this, some autonomous communities in Spain took advantage of their competencies in education and included SE in schools. In these cases, SE is regulated by local authorities and schools. In other communities, SE can be taught in short-term workshops together with other topics offered by public or private organizations.
The Portuguese Constitution established the foundation for sexual health promotion and education in 1976 and presented the first official document on SE and family planning in schools in 1984. This document emphasized the inclusion of scientific knowledge related to human anatomy, physiology, genetics, and sexuality for different educational levels. SE was included as part of personal and social development in 1986, and the government offered practical measures for implementing the law in 1998. The government established the objectives, curriculum, and organizational framework of SE for all children over the age of 6 in 2009, affirming the mandatory nature of SE. In recent years, there has been a significant emphasis on affirming citizens’ rights to education and health, and increasing SE awareness. For example, Portugal was the first country in the world to legally recognize September 4th as the National Sexual Health Day in 2021.
SE curricula in Spain and Portugal emphasize a biological-hygienist approach primarily centered around biology and the potential risks of sexual behavior, similar to other countries (Alvarez & Pinto, 2012; Picken, 2020; Schmidt et al., 2015). For example, mandatory SE in Portuguese schools mainly addresses topics such as the risk of pregnancies, contraceptive usage, STIs, bodily changes in adolescence, and biological differences between men and women, and tends to overlook topics such as romantic relationships, sexual and gender identity, or violence and abuse (Ferreira et al., 2022). This can have several consequences. Firstly, formal SE is failing to meet the objective of addressing topics that have become a priority in recent years (European Expert Group on Sexuality Education, 2016; Lameiras-Fernández et al., 2021), including sexual identity, sexual self-knowledge, sexism, sexual exploitation, homophobia, gender norms and inequalities, power dynamics in sex, the role of pleasure and sexual consent, the challenge of heteronormativity, and the acknowledgment of a wider and realistic repertoire of sexual practices. Secondly, formal SE is failing to adequately address the needs and concerns of younger people, as shown by perceptions that curricula have a very limited scope and fail to discuss other topics that are relevant to their lives and experiences (Cense et al., 2020; Sieg, 2003; York et al., 2021). Possibly related to this, health reports and research have shown high incidences of STIs, including HIV, and low incidence of contraception use at last intercourse across different age groups worldwide (e.g., CDC, 2023; Du et al., 2022; UK Health Security Agency, 2023), including in Spain and Portugal (Ballester-Arnal et al., 2022; de Irala et al., 2008; ECDC, 2022; Reis et al., 2019; Rodrigues et al., 2020).
Message framing used by current formal SE curricula can also foster differences in sexual behaviors and decisions. Research has shown that health communication is more efficient when the message frame aligns with people’s predominant motives in health (Fridman & Higgins, 2017; Ludolph & Schulz, 2015). Drawing from regulatory focus theory (Higgins, 2015), single people predominantly focused on prevention are driven by safety motives and tend to prioritize sexual health (e.g., use condoms more often), whereas single people predominantly focused on promotion are driven by nurturance motives and tend to prioritize sexual well-being (e.g., pursue sexual pleasure; Rodrigues et al., 2020, 2022). As SE curricula typically adopt a preventive framework, contents are more likely to resonate with people focused on disease prevention. In contrast, people focused on pleasure promotion may be less attentive to formal SE topics, given the overall lack of pleasure-related topics.
The current state of affairs in Spain and Portugal highlights a commitment toward a comprehensive SE (Michielsen & Ivanova, 2022; Picken, 2020). However, the implementation and effectiveness of formal SE are less convincing given a heavier focus on biology and hygiene, lack of inclusiveness of different topics (e.g., gender and sexual diversity), and lack of adjustment to what some younger people feel they need to explore (e.g., sexual pleasure and consent). As such, other sources of SE must be considered (see also European Expert Group on Sexuality Education, 2016).
Alternative sources of sexuality education
Beyond the mandatory school environment, people learn about sexuality and sexual behavior and seek advice from other sources (Harris, 2011). Adolescents and young adults learn about sexuality by talking to their parents, friends, sexual partners, teachers, or health professionals, or by looking for information on the Internet, watching movies and TV shows, or reading magazines and brochures (e.g., Perenc & Pęczkowski, 2022; Scharmanski & Hessling, 2022). These informal sources of SE can provide invaluable information and skills not addressed at school (sometimes allowing for a more inclusive and sex-positive approach), and drive people to actively search for sex-related information and learn ways to pursue more pleasurable sexual activities. For example, Nuttall and colleagues (2022) found that adolescents who attended sexual and reproductive health education programs provided by peer educators (i.e., healthcare students) improved their knowledge about contraception and sexual pleasure. Also, young people who report higher levels of general communication with their parents, and for whom their parents were a source of SE, are more likely to talk about sexual health with their partners (Hicks et al., 2013). And yet, people seem to rely on specific sources depending on the topic they are interested in. For example, Ferreira and colleagues (2022) found that Portuguese adolescents and young adults tend to talk to their friends and romantic partners about a larger number of topics (e.g., pregnancy risks, contraceptive methods, romantic relationships, sexual initiation, or violence in relationships), followed by their mothers (e.g., changes in adolescence, romantic relationships). In contrast, they tend to acquire information about STIs from their teachers. Interestingly, information about consultations and services related to sexuality, contraception, and family planning is sometimes acquired from health professionals, or searched for alone on the Internet.
Resources such as the Internet and social media provide easy and affordable tools that facilitate exposure to sex-related content (Cormier & O’Sullivan, 2021; Olamijuwon & Odimegwu, 2022). However, these sources are not a guarantee of comprehensive or accurate SE. For example, Kalke and colleagues (2018) analyzed 2,693 mobile apps related to SE and found that only 25% actually addressed sexual health, and only 1% met the criteria for comprehensive SE. Of these, most apps covered topics related to anatomy, STIs, and pregnancy prevention. Examining SE content on TikTok, Dolev-Cohen and colleagues (2023) found that most videos conveyed positive views of sex and sexuality, and highlighted the importance of sexual pleasure. These benefits notwithstanding, content creators tended to address topics superficially, given the short duration of the videos. In another study, Fowler and colleagues (2022) analyzed a sample of 100 TikTok videos with the hashtags #sexeducation and #healthclass. Most videos addressed topics related to anatomy (37%, particularly female anatomy) and sexual pleasure (23%). The remaining videos addressed topics related to contraception (13%) and, to a smaller extent, sexual health (5%) and communication (4%). Interestingly, a large number of the videos (18%) discussed negative experiences with formal SE in schools (e.g., the limited scope of topics) and the importance of addressing a more comprehensive list of topics (see also Cense et al., 2020; Goldfarb & Lieberman, 2021). This shows a disconnect between the SE offered in formal contexts (particularly at schools) and people’s needs.
Alternatively, sources such as movies and TV shows can facilitate exposure to new realities and groups and help to normalize public discourse (e.g., changing the narrative associated with transexual people). Some people also use pornography to learn about sexuality and experiment sexually (Grubbs et al., 2019; Litsou et al., 2021; Löfgren-Mårtenson & Månsson, 2010; Wright et al., 2018). However, these SE sources can convey traditional sex norms (e.g., sexual double standard) or unrealistic expectations about sex and relationships, and can facilitate the objectification of others, aggressive behaviors, and riskier sexual behaviors (Clancy et al., 2021; Endendijk et al., 2022; Román García et al., 2021; Willis et al., 2022).
Overall, the potential of informal SE sources as adequate tools is still far from understood. Leaving people to be informed about sex and sexuality through some of these sources can contribute to misinformation, the development of negative myths, and harmful practices.
Current study
The overall goal of this study was to better understand if and how SE received from different sources relates to people’s current needs, motives, and behaviors, particularly examining the Spanish and Portuguese contexts. We organized these sources into innovative categories according to their formality and modernity. Specifically, formal traditional sources included SE received during mandatory school years, and formal modern sources included SE received through optional education courses and higher education. These sources were differentiated based on the reasoning that traditional sources refer to SE curricula mandated by government-issued guidelines, whereas modern sources refer to SE curricula offered outside the mandatory school environment. Moreover, informal traditional sources included SE received by talking to family, friends, or romantic partners, and informal modern sources included SE received by watching movies, TV shows, and online pornography, or looking at online content and social media. In a cross-sectional study, we examined how sources of SE were perceived in terms of importance, if topics addressed in each source of SE differed, and whether the perceived influence of each SE source on current thoughts and behaviors in sex was uniquely associated with sexual health and well-being outcomes (i.e., condom use, predominant motives in sex, sexual health communication, sexual consent, sexual satisfaction, sex positivity, and sexual health practices).
We also explored whether differences between Spain and Portugal emerged. Not only is there a generalized lack of studies comparing both countries from the Iberian Peninsula, but there are also differences in the way both countries approach SE during mandatory school years. This raises questions as to whether these approaches (even during school years) have different implications for the way sexual health and well-being topics are addressed with other people (e.g., parents) or searched for (e.g., on social media), as well as to the way people think about sexuality and behave in sex. The current study was part of the Prevent2Protect project, and our hypotheses were pre-registered (https://osf.io/5hfw6).
Method
Participants
Demographic characteristics and country comparisons.
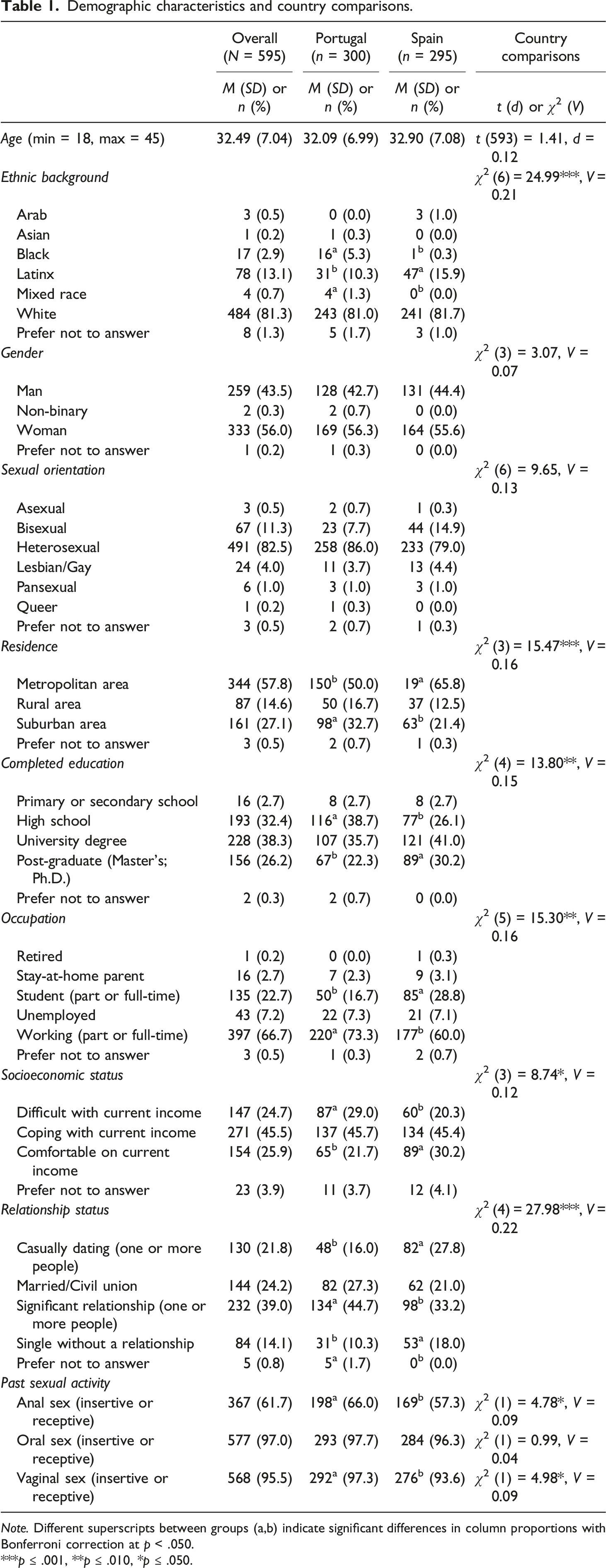
Note. Different superscripts between groups (a,b) indicate significant differences in column proportions with Bonferroni correction at p < .050.
***p ≤ .001, **p ≤ .010, *p ≤ .050.
Country comparisons revealed differences in ethnic background, p < .001, residence, p = .001, education, p = .008, occupation, p = .009, socioeconomic status, p = .033, relationship status, p < .001, past anal sex, p = .029, and past vaginal sex, p = .027. More specifically, a higher proportion of Portuguese participants identified as Black or mixed-race, lived in suburban areas, completed high school, were working, were having difficulties with their current income, had a significant relationship with one or more people (or preferred not to answer), and had engaged in anal or vaginal sex in the past. A higher proportion of Spanish participants identified as Latinx, lived in metropolitan areas, were post-graduates, were studying, were comfortable with their current income, were casually dating one or more people, or were single without a relationship.
Measures
We computed Confirmatory Factor Analyses (CFA) with robust maximum likelihood estimation (Yuan & Bentler, 2000) using Mplus 7 (Muthén & Muthén, 2012) on our outcome measures. We considered recommendations for adequate model fit (Byrne, 2012) and examined absolute fit (χ2; SRMR), relative fit (TLI), and non-centrality indices (CFI; RMSEA), as well as standardized regressions paths (λ) between items and their respective factor. We also examined reliability using McDonald’s omega (ω; Hayes & Coutts, 2020).
Sources of sexuality education
Formal traditional sources
We asked participants to indicate if they received SE classes during their mandatory school years (1 = No, 2 = Yes), more specifically “During your first to fourth years”, “During your fifth or sixth years”, “During your seventh to ninth years”, and “During your 10th to 12th years”. Participants were categorized as having received formal traditional SE if they indicated “Yes” to either of the items.
Formal modern sources
We asked participants to indicate if they attended (or were attending) optional SE courses after their mandatory school years (1 = No, 2 = Yes), more specifically, “Courses for adults”, “In post-graduate education”, “In higher education”, and “Other (please specify)”. Participants were categorized as having received formal modern SE if they indicated “Yes” to either of the items.
Informal traditional sources
We asked participants “Throughout your life, did you engage in conversations about sex with some of the following people?” and provided them with the items “Your parents”, “Your friends”, “Your romantic partners”, “Your casual partners”, and “With teachers” (responses to each item: 1 = No, 2 = Yes). Participants were categorized as having received informal traditional SE if they indicated “Yes” to either of the items.
Informal modern sources
We asked participants “Throughout your life, did you look for or retrieve sex-related information in some of the following places?” and provided them with the items “Movies or TV shows”, “Pornography”, “Webpages (please indicate which)”, and “Social media (please indicate which)” (responses to each item: 1 = No, 2 = Yes). Participants were categorized as having received informal traditional SE if they indicated “Yes” to either of the items.
Sexuality education topics
When selecting “Yes” in each of the items above, participants were then presented with a list included eight topics retrieved from the International Planned Parenthood Federation (IPPF, 2011): (1) Sexual and reproductive health (e.g., use and access to contraceptives); (2) Sexual knowledge (e.g., ways to explore sex and your body); (3) Sexual pleasure and difficulties (e.g., ways to achieve sexual pleasure and overcome sexual difficulties); (4) Sexual diversity and sexual orientation (e.g., the meaning of gender identity); (5) Sexual and reproductive rights (e.g., puberty, menstruation, sexuality, and reproduction); (6) Feelings and emotions in sex (e.g., feelings and emotions as part of sexuality); (7) Gender violence (e.g., forms of physical violence against women); (8) Sexual abuse (e.g., forms of non-consented sexual activity). For each source of SE, participants were asked to indicate which topics were addressed and how much each topic has influenced how they think and behave in sex now. Responses to each topic were given in 8-point rating scales (0 = Not applicable, I did not address this topic; 1 = I addressed this topic, but it had no influence to 7 = I addressed this topic and influenced a lot). After all sources of SE were assessed, participants were again shown the list of eight topics and asked to rate the importance of each topic for high-quality and comprehensive SE (1 = Not at all important at all to 7 = Extremely important).
Sexual behaviors
As part of the inclusion criteria, participants were asked to indicate if they had ever engaged in vaginal sex, anal sex, or oral sex (for each item, 1 = No and 2 = Yes) at the beginning of the survey. Depending on the type of sexual activity they enacted, participants were then asked to think about their sexual activity in the last six months and indicate “How often did you have vaginal sex without using condoms?” (1 = Never to 7 = I always had condomless sex), “How often did you have anal sex without using condoms?” (1 = Never to 7 = I always had condomless sex), and “How often did you have oral sex without using condoms?” (1 = Never to 7 = I always had condomless sex). Items were analyzed separately, with higher scores indicating a higher frequency of condomless sex. As a control measure, we additionally asked participants “Compared to your typical behavior before the COVID-19 pandemic, how similar or different was the frequency of your sexual activity (penetrative and/or oral sex) in the last 6 months?”. Responses were given in 7-point rating scales (−3 = I had sex less often than before to zero = I experienced no significant changes to 3 = I had sex more often than before).
Regulatory focus in sexuality
We used the Regulatory Focus in Sexuality scale developed by Rodrigues and colleagues (2019) to assess individual motives for prevention (three items; e.g., “Not being careful enough in my sex life has gotten me into trouble at times” [reverse-coded]) and promotion in sexuality (six items; e.g., “I am typically striving to fulfill my desires with my sex life”). Responses were given on 7-point rating scales (1 = Not at all true of me to 7 = Very true of me). CFA results showed good fit indices to our data, χ2 (25) = 90.80, SRMR = .04, TLI = .93, CFI = .95, and RMSEA = .07, with moderate to high standardized regression paths for the prevention [.45; .83] and promotion subscales [.62; .79]. Responses were mean averaged on each subscale, with higher scores indicating a greater focus on prevention (ω = .74) or promotion in sexuality (ω = .85). Both subscales were modestly correlated, ϕ = −.18, p < .001. We computed an index of regulatory focus by subtracting promotion from prevention scores (see Rodrigues et al., 2019), with more positive (vs. negative) scores indicating a greater focus on prevention (vs. promotion) in sexuality.
Sexual health communication
We used an adapted version of the Health Protective Sexual Communication Scale (Catania, 2020) to be more diverse and inclusive. Specifically, we rephrased “homosexual experiences” to “sex with more than one partner at the same time” and removed the item “Talked to a new sex partner about birth control before having sex for the first time” from the analysis. The final scale included nine items and assessed how often participants discuss health-related topics before having sex (e.g., “Ask your partners how they feel about using condoms before having sex”). Responses were given on 4-point rating scales (1 = Never to 4 = Always). CFA results showed good fit indices to our data, χ2 (26) = 114.68, SRMR = .05, TLI = .91, CFI = .94, and RMSEA = .08, with moderate to high standardized regression paths [.38; .80]. Responses were mean averaged, with higher scores indicating more sexual health communication (ω = .82).
Sexual consent
We used an adapted version of the Dual Measures of Consent (Jozkowski et al., 2014). Specifically, we selected and adapted the two items with the highest factor loading on each of the original factors, and asked participants to think about their typical sexual behaviors. Participants then indicated how often they experience internal sexual consent feelings (10 items; e.g., “During my typical sexual behaviors, I feel secure”; 1 = I never have this experience to 4 = I always have this experience), and how often they endorse external sexual consent communication (10 items; e.g., “In sex, I typically initiate behavior and check to see if my partner reciprocates”; 1 = I never behave like this to 4 = I always behave like this). CFA results indicated the removal of two items: one item from the internal consent scale that had a non-significant standardized factor loading, p = .156 (“During my typical sexual behaviors, I feel flushed”), and one item from the external consent scale that was negatively correlated with its factor, p < .001 (“During my typical sexual behaviors, I do not do anything”). The model with the remaining 18 items presented good fit indices to our data, χ2 (124) = 281.34, SRMR = .05, TLI = .93, CFI = .94, and RMSEA = .05, with moderate to high standardized regression paths [.11; .64]. Responses were mean averaged for each factor, with higher scores indicating more internal (ω = .80) and external consent (ω = .62).
Sexual satisfaction
We used the short version of the New Sexual Satisfaction Scale (Štulhofer et al., 2010) to assess how sexually satisfied participants are with their sex partners. We assessed sexual satisfaction with oneself (six items, e.g., “The quality of my orgasms”) and others (six items, e.g., “The variety of my sexual activities”). Responses were given on 5-point rating scales (1 = Not at all satisfied to 5 = Extremely satisfied). CFA results showed good fit indices to our data, χ2 (50) = 177.68, SRMR = .05, TLI = .93, CFI = .94, and RMSEA = .07, with moderate to high standardized regression paths for the ego [.58; .80] and activity subscales [.50; .77]. Responses were mean averaged on each subscale, with higher scores indicating more ego (ω = .87) and activity sexual satisfaction (ω = .84). Both subscales were correlated, ϕ = .86, p < .001, and therefore we mean averaged both scales into a single sexual satisfaction score.
Positivity and negativity in sex
We used the short version of the Sex Positivity-Negativity Scale (Hangen & Rogge, 2022) to assess positive (four items; e.g., “In general, I feel that sex and sexuality are fun”) and negative feelings about sex and sexuality (four items; e.g., “In general, I feel that sex and sexuality are miserable”). Responses were given on 6-point rating scales (1 = Not at all to 6 = Extremely). CFA results showed good fit indices to our data, χ2 (19) = 44.00, SRMR = .03, TLI = .97, CFI = .98, and RMSEA = .05, with high standardized regression paths for the positivity [.65; .88] and negativity [.79; .92]. Responses were mean averaged within subscales, with higher scores indicating more positive (ω = .86) and negative feelings about sex and sexuality (ω = .91). Subscales were treated separately in our analyses.
Health check-ups
We asked participants “How frequently do you go on routine sexual health check-ups?” (1 = I never went to one, 2 = Less than once a year, 3 = About once a year, 4 = More than once a year). Participants were also asked, “How frequently are you tested for STIs? (e.g., HIV, chlamydia, gonorrhea, syphilis)” (1 = I have never been tested, 2 = Less than once a year, 3 = About once a year, 4 = About twice a year, 5 = About once a month, 6 = More than once a month) and “Have you ever been diagnosed with an STI?” (1 = No, 2 = Yes).
Procedure
This study was approved by the Ethics Council at Iscte-Instituto Universitário de Lisboa (Ref.: 70/2021). Data were collected by recruiting prospective participants on the Clickworker platform and inviting them for an anonymous online survey about sexuality education and sexual behavior. To be eligible, participants were required to give their consent, be between 18 and 45 years of age (to account for social changes surrounding social and political discussions about SE), have already engaged in any type of sexual activity (i.e., oral, vaginal, or anal sex), and live either in Spain or Portugal. People who failed to meet any of these inclusion criteria were automatically redirected to the end of the survey. Eligible participants received €3 on their user account upon survey completion.
We started by asking participants to provide preliminary information (i.e., inclusion criteria), followed by standard demographic questions (e.g., gender, sexual orientation, education). We then defined SE according to the European Union guidelines (Picken, 2020) to our participants and presented participants with the remaining measures. We used two attention check items throughout the survey (e.g., “Please select the option “Extremely”. This is not a trick question”). Before the end of the survey, we also assessed participants’ attentiveness by asking “How much attention did you pay to this questionnaire while you were completing it?” (1 = No attention, 2 = Very little attention, 3 = Moderate amount of attention, 4 = Very close attention), and asked whether they wanted to retain or withdraw their responses (1 = I want to maintain my responses or 2 = I want to remove my responses and prevent them from being analyzed). Participants who failed at least one of the attention checks, who were not attentive to the survey (responses ≤2), and who asked to withdraw their responses were excluded from the final sample. At the end of the survey, participants were thanked, debriefed about the overall goals of the study, provided with information about SE, and provided with the contact of the research team.
Analytic plan
We conducted descriptive analyses to examine which of the eight topics of SE were considered the most and least important for a high-quality and comprehensive SE, using a repeated-measures ANOVA. Post-hoc comparisons were computed with Bonferroni correction. We then computed overall descriptive statistics and overall correlations. Following our pre-registration, we compared participants according to SE sources. Specifically, we computed the percentage of participants who received SE from any formal and informal sources. We also compared the average number of topics addressed in each source and the perceived influence of topics addressed in formal (vs. informal) sources of SE.
To have a finer analysis, we conducted exploratory analyses to examine the percentage of participants who addressed each topic on each of the four SE sources and the perceived influence of each topic within each SE source. Given that most participants received informal SE, we were unable to compare participants according to whether they received SE. Specifically, only two of our participants did not receive any type of SE, and of the participants who received formal SE, only three did not receive any informal SE. Hence, we had to revise our pre-registered analytic plan. To avoid confounds with the type of SE received by participants, we used the perceived influence of each SE source as our main predictor variables. However, given the low percentage of participants who received SE from formal modern sources (12.6%), we decided to discard this variable from the analysis. This allowed us to examine the relative contribution of each predictor variable on all sexual health and well-being outcomes with a subsample of 340 participants. We computed a linear regression using Mplus 7 (Muthén & Muthén, 2012) with mean-adjusted weighted least square (WLSM) as our estimator, given that past STI diagnosis was a dichotomous variable (Yuan & Bentler, 2000). We then examined if the results of the regression remained unchanged after controlling for age, gender, relationship status, and changes in sexual activity frequency since the pandemic (M = −0.10, SD = 1.67). Lastly, we explored the differences between Spain and Portugal. Study materials and anonymized data supporting the results herein reported are available (https://osf.io/5sd3h/).
Results
Descriptive analysis
Overall descriptive statistics and correlations.
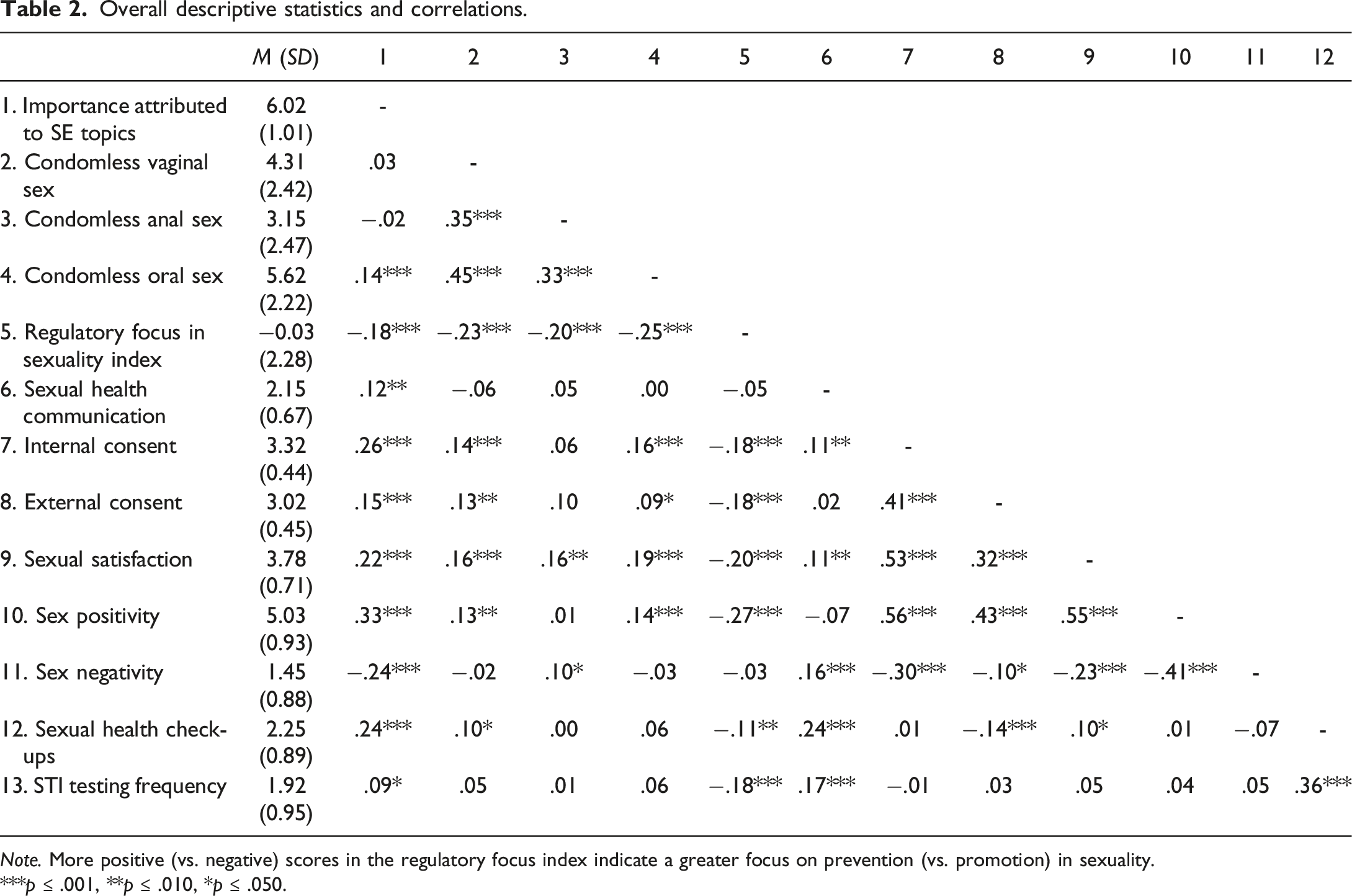
Note. More positive (vs. negative) scores in the regulatory focus index indicate a greater focus on prevention (vs. promotion) in sexuality.
***p ≤ .001, **p ≤ .010, *p ≤ .050.
Sources of sexuality education
Pre-registered comparisons between formal and informal sources
More than half of our participants received SE from any formal source (69.1%) and addressed, on average, five topics (M = 5.40, SD = 2.38). In contrast, nearly all participants received SE from informal sources (99.2%) and addressed, on average, seven topics (M = 7.34, SD = 1.25). The difference between the average number of topics addressed in each source was significant, t (407) = 16.63, p < .001, d = 0.82. Overall, participants perceived topics addressed in informal sources to have had more influence on their current thoughts and behaviors in sex (M = 4.67, SD = 1.14) than topics addressed in formal sources (M = 4.24, SD = 1.47), t (405) = 6.47, p < .001, d = 0.32.
Exploratory comparisons between all sources and topics
Most participants received SE from informal traditional sources (98.8%) or informal modern sources (84.0%) and addressed an average of seven topics on each source (M = 7.40, SD = 1.52, and M = 7.13, SD = 1.74, respectively). To a lesser extent, participants received SE from formal traditional sources (66.9%) and addressed an average of five topics (M = 5.33, SD = 2.43). Only a small subset of the participants received SE from formal modern sources (12.6%), although they addressed an average of seven topics (M = 6.67, SD = 2.41).
Percentage Of Participants Who Addressed Each Topic on Each Source of Sexuality Education and its Perceived Influence.
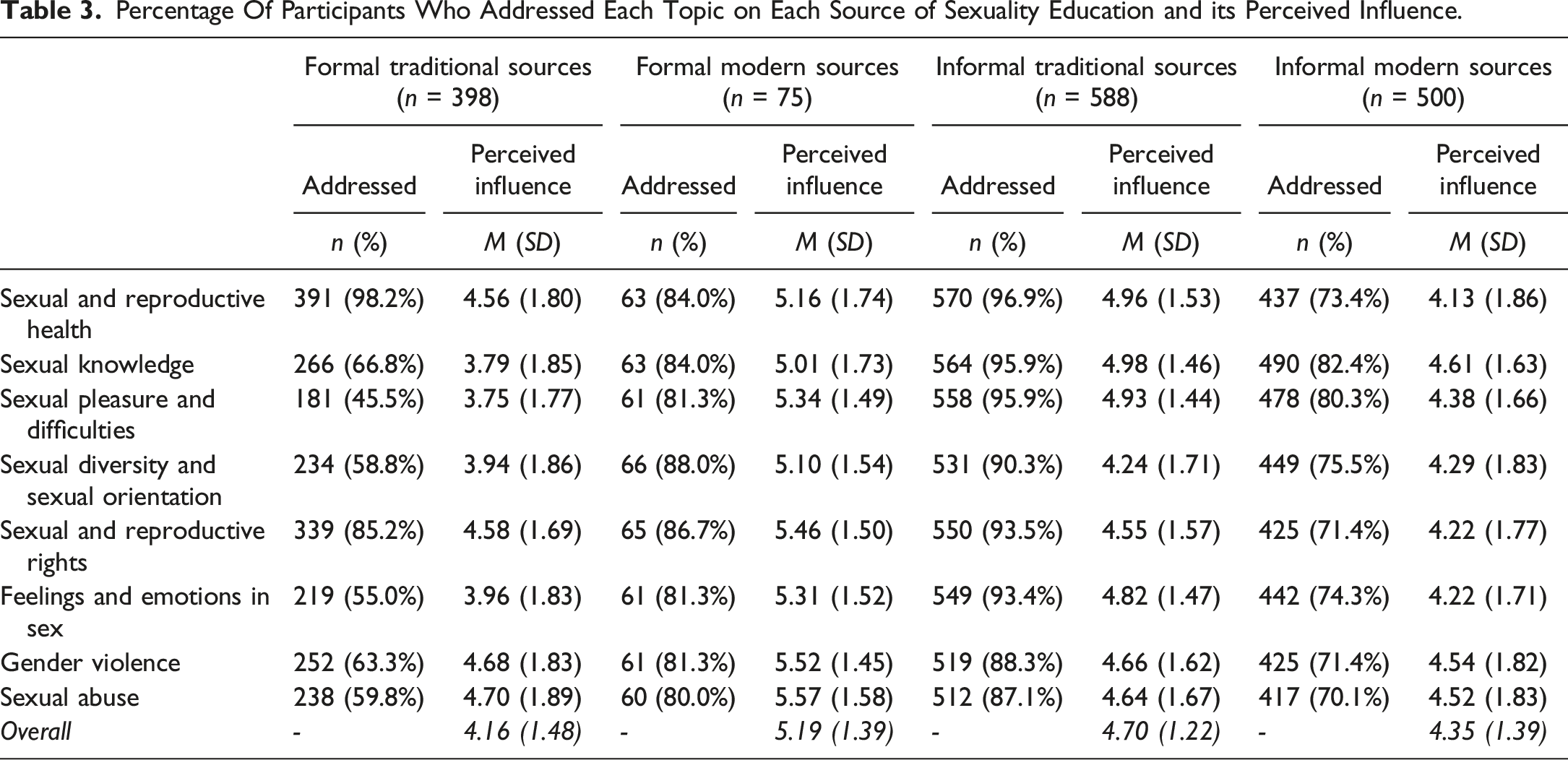
Lastly, participants perceived that most topics had some influence on their current thoughts and behaviors in sex. This was particularly evident among participants who received SE from formal modern sources (all M ≥ 5.01) and informal traditional sources (all M ≥ 4.24), and less evident among participants who received SE from formal traditional sources (all M ≥ 3.75).
Exploratory associations with sexual health and well-being outcomes
As depicted in Figure 1, participants who perceived more influence from formal traditional sources had condomless vaginal sex less frequently, β = −.17, SE = .06, p = .007, were more focused on prevention in sexuality, β = .17, SE = .06, p = .004, enacted more sexual health communication, β = .13, SE = .06, p = .030, and were less sex-positive, β = −.15, SE = .07, p = .031. Participants who perceived more influence from informal traditional sources attributed more importance to SE topics, β = .37, SE = .04, p < .001, had condomless vaginal sex more frequently, β = .14, SE = .07, p = .039, were more focused on promotion in sexuality, β = −.26, SE = .05, p < .001, experienced more internal consent, β = .32, SE = .06, p < .001, endorsed more external consent, β = .28, SE = .06, p < .001, were more sexually satisfied, β = .31, SE = .06, p < .001, were more sex-positive, β = .31, SE = .06, p < .001, went more frequently to routine sexual health check-ups, β = .21, SE = .06, p = .001, and got tested for STIs more often, β = .15, SE = .06, p = .016. Lastly, participants who perceived more influence from informal modern sources also attributed more importance to SE topics, β = .20, SE = .05, p < .001, had more frequent condomless vaginal sex, β = .14, SE = .07, p = .038, and anal sex, β = .21, SE = .09, p = .017, were more focused on promotion in sexuality, β = −.17, SE = .05, p = .001, and were more likely to have been diagnosed with an STI, β = .29, SE = .13, p = .033
1
. The results of this analysis remained unchanged after controlling for age, gender, relationship status, and changes in sexual activity frequency since the COVID-19 pandemic. Associations of Perceived Importance of Sexuality Education Sources with Sexual Health and Well-Being Outcomes. Note. SE = Sexuality education. STI = Sexually transmitted infection. More positive (vs. negative) scores in the regulatory focus index indicate a greater focus on prevention (vs. promotion) in sexuality. Only significant paths are depicted for clarity. Full lines indicate positive associations. Dashed lines indicate negative associations.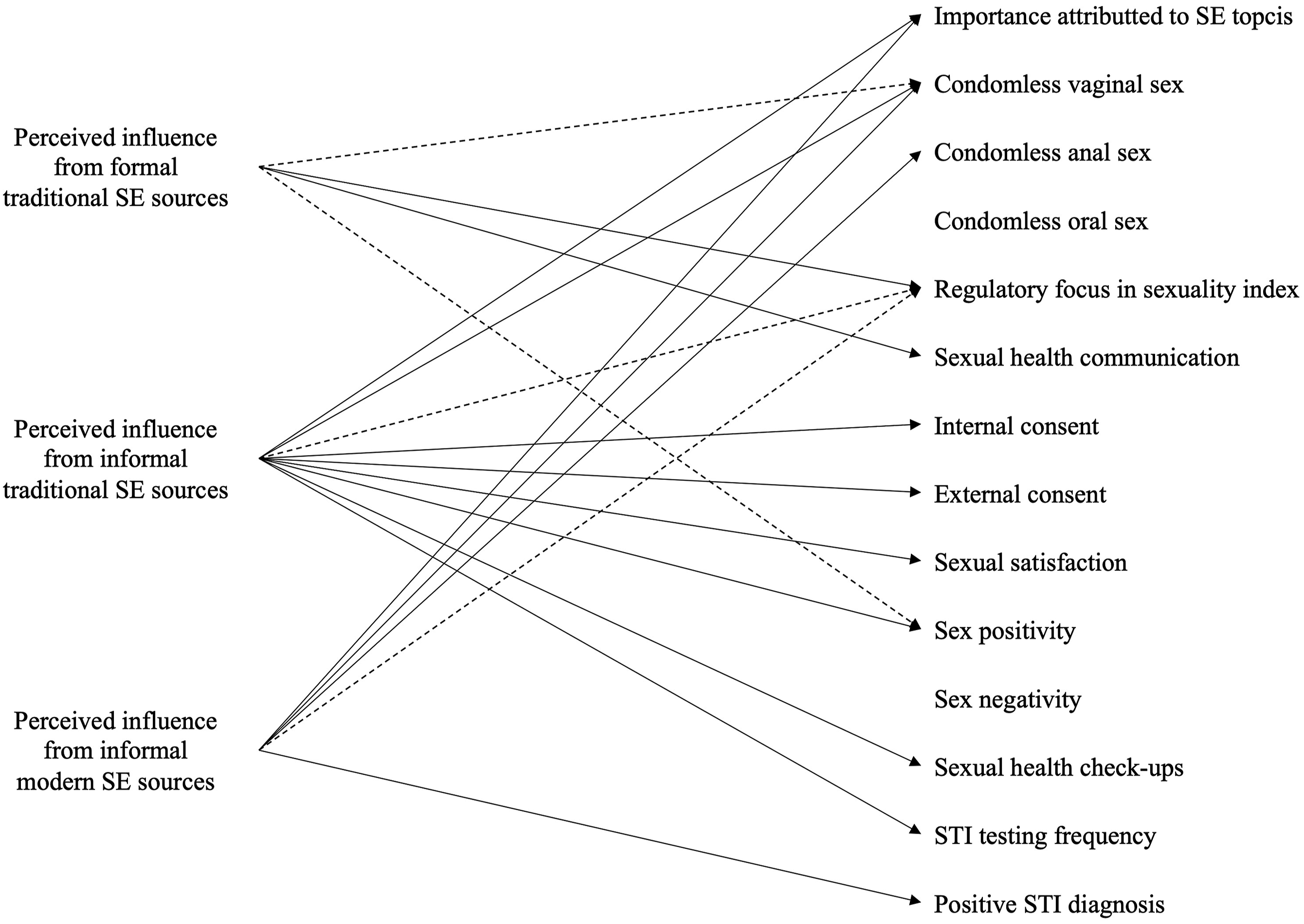
Country comparisons
Some differences emerged when comparing Spain and Portugal (see Supplemental Materials and https://rb.gy/gztwv). As shown in Table S1, Portuguese participants had condomless vaginal sex more frequently, p < .001, experienced more internal consent, p < .001, endorsed more external consent, p = .017, were more sexually satisfied, p < .001, and were more sex-positive, p = .015. In contrast, Spanish participants were more sex-negative, p = .002. Also, we found a similar pattern of correlations in both countries, albeit with a few exceptions. For example, attributing more importance to SE topics was correlated with more sexual health communication and more external consent endorsement only for Spanish participants, and with higher STI testing frequency only for Portuguese participants (see Table S2).
Comparisons between SE sources and topics (see Table S3) showed that Spanish and Portuguese participants were equally likely to have received SE from informal traditional sources, p = .245, and addressed a similar number of topics, p = .281. Although no country differences emerged in the percentage of participants who received SE from informal modern sources, p = .122, Portuguese participants addressed, on average, a higher number of topics when compared to Spanish participants, p = .047. Results also showed that more Spanish than Portuguese participants received SE through formal traditional sources, p = .011, although Portuguese participants addressed, on average, a higher number of topics than Spanish participants, p = .011. Lastly, more Spanish than Portuguese participants received SE through formal modern sources, p < .001, but no country differences in the number of topics addressed emerged, p = .122.
As shown in Table S4, Spanish participants were more likely to have addressed topics such as sexual pleasure and difficulties, p = .029, sexual diversity and sexual orientation, p = .037, and feelings and emotions in sex, p = .029, in formal modern sources. In contrast, Portuguese participants were more likely to have addressed topics such as sexual and reproductive rights, p < .001, gender violence, p < .001, and sexual abuse, p < .001, in formal traditional sources. Portuguese participants were also more likely to have addressed topics related to sexual and reproductive health, p = .048, and sexual and reproductive rights, p = .015, in informal traditional sources, as well as topics such as sexual and reproductive rights, p = .027, gender violence, p = .014, and sexual abuse, p = .008, in informal modern sources. Examining the perceived influence of each SE topic (see Table S5), Portuguese participants perceived more influence of sexual and reproductive health topics received through formal traditional sources, p = .043, and sexual knowledge topics received through informal modern sources, p = .031. Despite these differences, the results of the linear regression were largely unchanged after adding country as an additional covariate.
Discussion
The current study aimed to examine whether different sources of SE were uniquely related to multiple indicators of sexual health and well-being, and to explore differences between Spain and Portugal. Overall, participants acknowledged the importance of different topics to a high-quality and comprehensive SE, validating their importance to improve sexual literacy. Topics related to sexual and reproductive health were perceived as the most important, which resonates with how frequently this topic was addressed in all SE sources, particularly in formal traditional (Alvarez & Pinto, 2012; Picken, 2020; Schmidt et al., 2015) and informal traditional sources (Ferreira et al., 2022; Perenc & Pęczkowski, 2022; Scharmanski & Hessling, 2022). Participants who attributed more overall importance to SE topics were also more focused on prevention in sexuality (i.e., more likely to avoid risks and pursue safety maintenance), communicated more about sexual health with their partners, reported more internal and external sexual consent, were more sexually satisfied, had more positive and less negative attitudes toward sex, and enacted more sexual health practices (i.e., routine check-ups and STI testing). In other words, acknowledging the relevance and importance of the information received through SE sources can have benefits for multiple sexual health and well-being outcomes, and ultimately contribute to healthier and respectful relationships, and better informed and more responsible sexual practices. Surprisingly, attributing more overall importance to SE topics was also associated with more frequent condomless oral sex. This suggests that sometimes people make conscious decisions to enact condomless sex practices, which may be particularly evident when these behaviors are believed to have (or known objectively to have) lower risks for health (e.g., oral sex vs. penetrative sexual practices; Hawkins, 2001). This may explain why some people decide to forgo condom use or STI testing in certain situations (e.g., when in a committed relationship). Aligning with this reasoning, recent research has shown that people who are more focused on prevention in sexuality tend to be more lenient with their condom use intentions with casual partners, but only when contextual cues indicate lower health risks (Rodrigues, 2023).
Our results further showed that each source of SE has benefits and consequences for sexual health and well-being, and should be considered complementary to a comprehensive and inclusive SE. Nearly all participants received SE from informal traditional sources (e.g., talks with parents and friends) and informal modern sources (e.g., movies and social media), addressed most of the topics in both cases, and perceived all topics to have influenced their current thoughts and behaviors in sex. Perceived influence from both sources was also associated with the attribution of more importance to SE topics, echoing the argument that informal sources of SE, particularly informal traditional sources, have added value over formal traditional ones. This may be related to differences in the type of message used by informal sources (e.g., sex-positive approach) compared to formal traditional sources (e.g., risk-based approach). Participants who perceived more influence from informal traditional sources also reported more benefits for their sexual health and well-being, including more sexual consent, sexual satisfaction, sex-positivity, and sexual health practices. And yet, this perceived influence was also associated with potential health consequences. Indeed, these participants reported having condomless sexual activity more often and were more focused on promotion in sexuality (i.e., more likely to pursue sexual pleasure), and participants who perceived more influence from informal modern sources were more likely to have been diagnosed with an STI. Arguably, factors related to peer pressure and condomless sex practices often conveyed in online content (e.g., pornography) might contribute to more lenient decisions regarding condom use (Clancy et al., 2021; Wright et al., 2018).
Around two-thirds of our participants received SE from formal traditional sources (i.e., in mandatory school), although around half did not address topics related to sexual pleasure and difficulties, feelings and emotions in sex, sexual diversity and sexual orientation, or sexual abuse. This suggests that comprehensive discussions around the importance of exploring oneself sexually and having respectful relationships with others may be lacking from current SE curricula in schools. Perceiving more influence from formal traditional sources was associated with benefits for sexual health and well-being, such that participants reported having condomless less often, were more focused on prevention in sexuality, and were more likely to enact sexual health communication with their partners. This indicates that formal traditional sources of SE are crucial to offering fundamental knowledge concerning sexual and reproductive health, and rights and knowledge, to inform the decision-making process in sexuality. Participants who perceived more influence from formal traditional sources were also less sex-positive. This may be a byproduct of formal traditional sources being mostly centered around risk mitigation, and SE curricula not being completely aligned with adolescents’ needs, which might inadvertently determine how comfortable and open people are to embrace and explore their sexuality.
We also found that most participants addressed all topics when receiving SE from formal modern sources (e.g., courses) and perceived them to be most influential to their current thoughts and behaviors in sex. This shows the importance of having courses dedicated to SE made available to young adults (most of whom are already outside their mandatory school years), offered in more private contexts (e.g., at home), and in some cases offered in higher education (e.g., as part of university courses). This is particularly relevant considering the low proportion of participants who received SE through this source, suggesting greater adequacy for young adults’ needs and expectations. These sources of SE may allow people to delve deeper into the intricacies of sexuality and sexual identity, explore the emotional and psychological dimensions of sexual intimacy, and learn about sexual pleasure and difficulties in specific stages of development (e.g., emerging adulthood).
Lastly, we need to highlight some differences that emerged between Spain and Portugal. Both countries are aligned with the European Union directives and committed to providing comprehensive SE to all people (European Expert Group on Sexuality Education, 2016; Ketting et al., 2021; Picken, 2020). However, differences exist in the implementation and integration of SE curricula in the formal education system (Cunha-Oliveira et al., 2021; Martínez et al., 2012; Matos et al., 2014). We found that more Spanish participants received SE through both formal traditional sources and formal modern sources. We also found that topics related to sexual pleasure and difficulties and feelings and emotions in sex were addressed in formal modern sources by more Spanish participants. Spanish autonomous communities were given control over education (including SE) in 2000. This decentralization likely allowed local governments in Spain to offer SE contents in schools for a longer period and through alternative formats (e.g., courses; Espada et al., 2015). Alternatively, Spanish people who did not receive SE in schools might feel the need to receive SE when they leave mandatory schools. In contrast, the establishment of nationwide Portuguese guidelines to govern SE in 2009 might have facilitated specific topics to be addressed in schools. Indeed, we found that Portuguese participants perceived sexual and reproductive health topics addressed in formal traditional sources to be more influential, indicating the importance of mandatory SE in the school context. We also found that more Portuguese participants addressed topics related to sexual and reproductive health, gender violence, and sexual abuse in formal traditional sources. These topics were addressed by more Portuguese participants in informal traditional sources (i.e., sexual and reproductive health) and informal modern sources (i.e., sexual and reproductive health, gender violence, and sexual abuse). This suggests the particular importance of informal sources to address certain topics of SE by Portuguese adolescents and young adults.
Limitations and future studies
The sociocultural and political contexts of both Iberian Peninsula countries are likely to limit the generalizability of our findings to other contexts. Also, our findings rely on cross-sectional data, and we are unable to establish causal associations between the perceived influence of SE sources and sexual health and well-being outcomes. In addition, we did not assess the type of SE messages received (e.g., how or under which conditions were the SE topics addressed) and we were unable to conduct further comparisons within each SE source (e.g., talks parents vs. friends within informal traditional sources). Hence, we could not determine whether the quality or framing of the information addressed in each SE source (e.g., messages focused on abstinence vs. condom use) had distinct implications for their perceived influence on current thoughts and behaviors and, consequently, sexual health and well-being outcomes (e.g., quality of parent-child SE communication; Astle & Anders, 2023). Likewise, we were unable to conduct finer analyses on the perceived importance (or influence) of specific topics within SE sources for sex-related perceptions, behaviors, and experiences. Hence, the specific contributions of our work must be considered in light of important additional variables. For example, our results showed that people who perceived more influence from formal traditional sources used condoms more frequently. However, we must acknowledge that condom use decision-making is complex and informed by multiple variables (e.g., de Visser & Smith, 2004; Rinaldi-Miles et al., 2014). These limitations notwithstanding, our study offers a new perspective on SE sources and can inform new research. For example, future studies could consider replicating our study in diverse geographical and cultural settings, and integrate qualitative approaches to have a deeper understanding of the implications of different SE sources and topics, and longitudinal approaches to determine the temporal effects of SE received through different sources and the unique contribution and intersection between (and within) SE sources. Moreover, future studies could examine the type of messages conveyed by different sources to sexual health and well-being outcomes. Such an approach would also allow researchers to extend our knowledge and examine whether SE sources influence other outcomes over time, including sexual communication skills, emotional well-being, and mental health. Lastly, future studies could consider qualitative approaches to understand better how people think about each source of SE, whether people are more likely to benefit from specific SE sources at different stages of their development, and if addressing topics with some people (e.g., teachers vs. parents) or engaging with certain materials (e.g., social media vs. SE apps) are more influential to sexual behaviors.
Implications
This study has implications for social policies and public health interventions. Our results emphasize the need to guarantee the comprehensiveness of SE by assuring that all topics are addressed equally in formal traditional sources. This applies particularly to topics related to sexual pleasure and difficulties, shown to improve sexual health and well-being outcomes (Zaneva et al., 2022), but also to most of the other topics (except those related to sexual and reproductive health; Picken, 2020). Hence, policymakers should work to ensure equitable and adequate coverage of different topics in SE curricula offered at schools, and consider developing SE curricula and courses to be offered outside the mandatory school environment (e.g., lectures or workshops held in universities). Lastly, policymakers should consider developing high-quality materials to help train sexuality educators (Walker et al., 2021) and to be shared through other SE sources (e.g., self-paced SE platforms).
Our study also emphasized the importance of informal sources to SE, which should be considered by sexuality educators in schools and worked as an advantage. Indeed, formal traditional sources of SE tend to overlook the potential advantages that other sources can have. Acknowledging and taking advantage of these sources can offer opportunities for younger people in schools to address their needs, expectations, and concerns from different perspectives, and have informed discussions around certain aspects that may have been unintentionally learned. For example, researchers have suggested the importance of improving pornography literacy among younger people and including discussions around the implications of pornography use on SE curricula (Crabbe & Flood, 2021; Dawson et al., 2020). These informal modern sources are more dependent upon individual needs, and knowledge acquisition is likely to be guided by curiosity and material availability. Interlocutors who have scientific and communication training could help increase awareness of the misinformation and biased depictions of sexual activities typically conveyed in these sources. Likewise, sex educators in schools could take advantage of digital media to improve sexual literacy and offer younger people the tools to critically assess the contents available in informal modern sources of SE. Lastly, policymakers could also contemplate the benefits of working with family life educators, and work to develop parent education programs and community engagement programs. These informal traditional sources are more dependent upon interpersonal dynamics and may be restricted by social norms, expectations, and pressures. Hence, these programs should strive to improve shared knowledge, and foster open and informed conversations that can have benefits to sexual health and well-being.
Conclusion
The results of this study suggest that sexual well-being seems to be overlooked in favor of sexual health in formal traditional sources of SE. In contrast, sexual well-being seems to be prioritized relative to sexual health in informal sources of SE. Comparing Spain and Portugal, a stronger balance between established directives and allowed autonomies, and between mandatory and modern approaches still needs to be achieved. Such balance should aim to enhance the comprehensiveness of SE topics and adjust them to the needs, questions, and interests of younger people.
Supplemental Material
Supplemental Material - Do different sources of sexuality education contribute differently to sexual health and well-being outcomes? Examining sexuality education in Spain and Portugal
Supplemental Material for Do different sources of sexuality education contribute differently to sexual health and well-being outcomes? Examining sexuality education in Spain and Portugal by David L. Rodrigues, A. Catarina Carvalho, Richard de Visser, Diniz Lopes, and Maria-João Alvarez in Journal of Social and Personal Relationships
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grants from the International Association for Relationship Research (IARR 2022 Geographical Diversity Research Grants) and the Social Observatory of the “la Caixa” Foundation (Ref.: CF/PR/SR20/52550001) awarded to DLR, and from the Fundação para a Ciência e a Tecnologia awarded to DLR (Ref.: 2020.00523. CEECIND) and ACC (Ref.: 2023.01784.BD).
Ethical statement
Open research statement
As part of IARR’s encouragement of open research practices, the author(s) have provided the following information: This research was pre-registered. The aspects of the research that were pre-registered were the hypotheses, materials, procedures, and data analytic plan. The registration was submitted to https://osf.io/5hfw6. The data and materials used in the research are publicly available. The data and materials can be obtained at: ![]() or by emailing:
or by emailing:
Supplemental Material
Supplemental material for this article is available online.
Note
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.