
Abstract
Intimate partner violence (IPV) is an increasingly prevalent problem in most parts of the world, including Nigeria. Very little is known about why persons who experience IPV sometimes decide to remain in the abusive relationships. In this study, we investigate whether the need for closure (NFC) may play significant roles in the association of IPV and the decision to stay in abusive relationships (traumatic bonding). Specifically, we tested if NFC would mediate the relationship between IPV and traumatic bonding (TB) among victims of IPV in Nigeria. Participants were 345 women, purposively selected from female clients who visited the Sexual Assault Referral Centre (SART) in Awka, Anambra State (n = 145) and the Lagos State Domestic and Sexual Violence Response Team, Lagos (n = 200). Their age ranged from 18–61 years (M = 35.79; SD = 8.6 years). They responded to the Composite Abuse Scale, the Need for Closure Scale, and the Stockholm Syndrome Scale. Results of data analysis using the Hayes regression-based PROCESS macro showed that IPV was not significantly associated with traumatic bonding while NFC was positively associated with increased traumatic bonding. Estimates of indirect effects indicated that NFC mediated the relationship of IPV and TB serving as a pathway through which IPV was linked to dimensions of TB. This shows that NFC may engender tendencies that increase the likelihood of traumatic bonding. The implications of these findings were discussed across policy, research and psychotherapeutic practice.
Introduction
Intimate partner violence (IPV) is becoming a frequent form of violence and a serious public health issue that breaches victims’ fundamental human rights. IPV is defined by the American Psychological Association and the Presidential Task Force on Violence and the Family (1996) as tangible or threatened physical, sexual, psychological, economic, or monitoring abuse perpetrated by present or ex-partners. IPV has continued in the society, and its frequency among couples, particularly female partners, has grown over time (Krug et al., 2002), with a documented spike during the COVID-19 lockdowns (Lyons & Brewer, 2021; Moreira & da Costa, 2020). IPV has also increased dramatically in Sub-Saharan Africa, notably in Nigeria (Lafraniere & Lussier, 2005).
Current Nigerian reports have constantly depicted the unsafe status of women in violent partnerships. For example, informal reports on social media, newspapers, television, and radio programs have repeatedly shown one form of IPV or sexual abuse after another, varying from vicious head trauma (Agbedo et al., 2021; Effiong et al., 2022; Iorfa et al., 2022a, 2022b) to deaths (Agbedo et al., 2021). According to the World Health Organization’s Department of Injuries and Violence Prevention (2005), one out of every four women worldwide experiences sexual violence by her intimate partner, while the CLEEN Foundation (a Nigerian NGO) recently reported that one in every three female respondents in their study accepted being a victim of intimate partner violence and that there has been a nationwide upsurge in violence in the past years, from 21 percent to 30 percent in 2013 (CLEEN Foundation, 2013).
These reports illustrate the prevalence of IPV among Nigerians. Survivors of IPV are frequently presented with a range of choices about abuse and the perpetrator. One of these options is whether to remain in the abusive relationship or quit it (Rakovec-Felser, 2014). However, cultural, societal, and gender norms make it difficult for most IPV victims, particularly women, to make plans to end an intimate relationship, particularly marriage. These characteristics are exacerbated in a mainly patriarchal and religious nation like Nigeria, where the woman may be persuaded to maintain the marriage for the sake of her children, her social position, and religious reasons. Furthermore, research has revealed that intentions to leave or remain in an unhealthy relationship are frequently impacted by a variety of psychological processes, one of which is traumatic bonding (Word Health Organization, 2005).
Traumatic bonding
Traumatic bonding (TB) is an intense affective tie created between an abused individual and his or her perpetrator as a result of the recurrent (and frequently interrupted) cycle of violence (Iorfa et al., 2022a). TB emerges as a result of repeated cycles of assault in which the inconsistent reinforcement of reward and punishment generates strong emotional attachments that are hard to modify (Dutton & Painter, 1981). According to Saunders' (1999) attachment theory, TB is an unsettled form of insecure attachment in which the potential for self-regulation is hindered by an attachment figure’s alternately abusive and protective activities. Other theoretical reasons for TB may be found in the writings of psychodynamic theorists who have used notions like masochism, re-occurring compulsion, and identification with the perpetrator to analyze how TB and other self-destructive relationships emerge (van der Kolk, 1989). It is also reasonable to believe that continuing abusive relationships may influence the victim’s accurate assessment of the abusive circumstances.
Graham et al. (1995) designed a TB scale and discovered that the items were generally characterized by three elements (dimensions): core Stockholm syndrome, psychological damage, and love dependency. In addition, cognitive distortions and interpersonal trauma were characterized as core symptoms of Stockholm syndrome (Graham et al., 1995; Phillip et al., 2020). These included explaining and/or minimizing a violent spouse’s behavior, self-blame, and reporting love in the face of fear. Cognitive distortions and other coping methods are also characteristics of the fundamental Stockholm syndrome component. Depression, low self-esteem, loss of sense of self, and other interpersonal issues are all examples of psychological damage (Effiong et al., 2022; Graham et al., 1995). IPV victims who have suffered psychological damage are continually unhappy and have low self-esteem. Most of the time, because of low self-esteem, they think they are honored to have partners at all and are prepared to stay in violent relationships for the fear of not getting another partner. Psychological damage refers to any emotional disturbances that victims of IPV may face while in an abusive relationship. Love dependence is characterized by a strong sense that one’s entire existence is reliant on a partner’s love, intense idolization, and the feeling that there would be nothing at all to live for without one’ s spouse (Bhat, 2021; Graham et al., 1995). People with a high level of love dependence are more inclined to stay in an abusive relationship despite the apparent disadvantages. For them, leaving their relationships may be identical to leaving life, since they have gotten reliant on their love affairs and the affection they receive from them. People who have a high level of love dependence may assume that their existence is reliant on their partner’s affection. They may adore them in some circumstances. Affection-dependent people also think that their spouse’s affection and security are more essential than whatever suffering the partner may be providing them (Messing et al., 2021).
Given the rising prevalence of IPV and the evidence that TB is used as a maladaptive coping mechanism among victims in Sub-Saharan Africa, particularly Nigeria (Effiong et al., 2022), where facts and data on the true incidence of domestic violence are lacking, it is becoming increasingly important to examine the correlates of TB and the pathways through which it is formed and sustained. This will aid in tailoring appropriate interventions to victims at all levels. As a result, the need for closure was investigated as a mediator of the association between IPV and TB in this study.
Need for closure
Need for closure (NFC) has refers to the “desire for a definite answer on a topic, any answer as opposed to confusion and ambiguity” (Kruglanski, 1989). When faced with ambiguous situations, individuals high in NFC tend to “seize” on an apparent solution (often times, this translates into the first plausible solution they encounter) and “freeze” (i.e., not let subsequent information affect their opinion). According to Webster and Kruglanski (1994), the Need for Closure scale is divided into five domains, including the preference for predictability, closed-mindedness, preference for order, discomfort with ambiguity, and decisiveness. Notably, this sub-division measures an ability component as well as a need component, and this distinction between need and ability has caused serious debates about the structure and validity of the scale (Kruglanski, 1989; Neuberg et al., 1997) as well as its reliability.
That notwithstanding, studies (e.g., Saroglou, 2002; Chirumbolo et al., 2004; etc.) evaluating NFC have linked it to a wide variety of personal and cognitive characteristics. For instance, NFC positively correlates with religious fundamentalism (Saroglou, 2002), cultural conservatism (Van Hiel & Mervielde, 2004), and authoritarianism (Chirumbolo et al., 2004), and negatively correlates with a desire for cognitive complexity (Webster & Kruglanski, 1994), individual and group creativity, and tolerance of multiculturalism (Chirumbolo et al., 2004). Research has examined the role of NFC in satisfaction with jobs (Kosic, 2002), job candidates (Webster & Kruglanski, 1994), and negative evaluations of people whose opinions or behaviors deviate from other people in their social groups (Drigotas et al., 1999; Rusbult & Martz, 1995). However, not much has been done to understand the possible nexus of NFC and IPV-related outcomes such as TB.
Need for closure as a mediator
NFC has been associated with psychological issues, including deviant bias (Schimel et al., 1999). Furthermore, the need for closure is assumed to be a fundamental motivation that is not restricted to the social domain (Kruglanski, 2004). One could argue that dating and forming romantic relationships can be fraught with ambiguity (Drigotas et al., 1999; Tran & Simpson, 2009). Need for closure (NFC) is a personality trait that reflects the desire to have clear and definite answers to ambiguous situations (Webster & Kruglanski, 1994). Previous studies have suggested that NFC may mediate the relationship between intimate partner violence (IPV) and traumatic bonding, which is a psychological attachment to an abusive partner (Dutton & Painter, 1993). IPV may increase the victim’s NFC, as they seek to reduce uncertainty and anxiety in their relationship (Graham-Bermann & Seng, 2005; Mikulincer & Shaver, 2007). High NFC may then facilitate traumatic bonding, as the victim rationalizes the abuse and develops a sense of loyalty and dependence on the perpetrator. Therefore, NFC may explain how IPV leads to traumatic bonding.
There is peripheral support for this idea in the relationship literature, even if the specific phrase “Need for Closure” is not used. Drigotas and Rusbult (1992) proposed a dependency model of breakups that states that some individuals remain in unsatisfying relationships due to their dependence on the other person and the relationship as a whole. The authors framed this dependence as a function of the available alternative relationships, but Johnson and Rusbult (1989) also posit that individuals high in commitment tend to derogate alternative relationships. Thus, even if alternative options are available, individuals seeking predictability may be motivated to derogate those options. In addition, high-NFC individuals are likely to view alternative relationships, no matter how enticing, as having less predictability as compared to established relationships, and this could lead such individuals to place less value on these alternatives.
Finkel and Rusbult (2008) also proposed that, while a desire to make personal sacrifices for the sake of sustaining a relationship is often associated with relationship satisfaction, an excessive desire to do so can lead to neglect of one’s own well-being. Research has produced support for this idea in cases featuring severe consequences (i.e., physical and psychological abuse) as well as those featuring more general dissatisfaction (Fritz & Helgeson, 1998; Rusbult & Martz, 1995).
Finally, although the impact of NFC on traumatic bonding has yet to be studied, several subscales of NFC have been correlated with types of insecure attachment (Mikulincer, 1997), which in turn has been associated with relationship instability later in life (Bartholomew & Horowitz, 1991; Karavasilis et al., 2003). The current research will examine if and how NFC associates with traumatic bonding among victims of IPV.
In intimate relationships therefore, it seems possible that the cognitive tendencies described by NFC could combine to create a situation where one seizes upon the first minimally acceptable dating partner and stays with him or her despite subsequent problems. The high-NFC individual would be motivated to stay in an existing relationship due to his or her high level of decisiveness and due to a discomfort with the ambiguity of starting a new relationship (as opposed to the relative comfort of the familiar one). This is not to say that high-NFC individuals are more likely to become involved in unsatisfying relationships or that their cognitive characteristics lead the relationships to be unsatisfying. It is merely to say that once involved in a relationship, they will be motivated to remain involved, even if the relationship is less than optimal.
This study tests the hypotheses that; 1. IPV will be associated with traumatic bonding 2. NFC will mediate the relationship between IPV and traumatic bonding
Method
Participants
Participants were 345 women, purposively selected from female clients who visited the Sexual Assault Referral Centre (SART) in Awka, Anambra State (n = 145) and the Lagos State Domestic and Sexual Violence Response Team, Lagos (n = 200). Their age ranged from 18–61 years (M = 35.79; SD = 8.6 years). The mean number of years in marriage was 9.8 years (SD = 7.01). All the participants were from Nigeria. In respect to the number of children, most of the respondents 76.2% (263) reported that they had children, while 22.3% (77) of the respondents reported that they had no children. As regards educational qualification, 0.9% (3) of the respondents had a Masters in Business Administration, 9.6% (32) had an Ordinary National Diploma, 55.8% (187) had a Higher National Diploma/Bachelor of Science, 10.4% (35) had either a Master of Science or a Doctor of Philosophy degree, 6.9% (23) had a National Certificate in Education, 15.2% (51) had a Secondary School Certificate in Education, and 1.2% (4) had a First School Leaving Certificate, while 10 people did not indicate their educational qualification. As regards the educational qualification of their spouse, 52.4% (152) had a Higher National Diploma/Bachelor of Science, 15.2% (44) had either a Master of Science or a Doctor of Philosophy Degree, 21.4% (62) had a Secondary School Certificate in Education, 6.2% (18) had an Ordinary National Diploma, 3.4% (10) had a FSLC, and 1.2% (4) had an NCE, while 55 people did not indicate the educational qualification of their spouse. In terms of employment status, most of the respondents 63% (220) reported that they were not employed (Housewife) while 36.2% (125) of the respondents reported that they were employed. As regards socioeconomic status, most of the respondents 59.4% (205) reported that they belong to low socio-economic status, (18%)62 of the respondents reported that they belong to middle socio-economic status while 9.6% (33) of the respondents reported that they have high socio-economic status.
Procedures
The management of the domestic violence response intervention offices gave permission for a research assistant to seek participants for the study. When a visitor to the facility identified herself as a victim of intimate partner abuse to the receptionist, the research assistant contacted the individual, developed rapport, and asked her to engage in the research while outlining their rights to informed consent and confidentiality. The average duration from initial contact to completion and return of the questionnaire form was 20–25 minutes. At both of the two locationss, 360 questionnaires were produced and distributed. However, only 350 were collected, yielding a return rate of 97.2 percent. Out of the 350 copies of the questionnaire form returned, five were eliminated owing to discrepancies or unusual response patterns, yielding a 95.8 percent return rate. Specifically, 150 questionnaire forms were distributed at the SART Awka, Anambra State, and 150 were retrieved, resulting in a 100% return rate, while 205 were distributed at the Lagos State Domestic and Sexual Violence Response Team, Lagos, and 200 were retrieved, resulting in a 97.6% return rate.
Measures
Intimate partner violence
Intimate partner violence (IPV) was measured using the short version of the Composite Abuse Scale (CAS) developed by Hegarty et al. (2005). The short version CAS is a 30-item 6 point Likert Scale containing actions by an intimate partner that constitute emotional or physical abuse and provides data on the prevalence of intimate partner violence experienced by victims. Respondents were required to rate the frequency of abuse in the past year on a scale ranging from 5 = daily, 4 = once per week, 3 = once per month, 2 = several times, 1 = only once, 0 = never). According to MacMillan et al., (2009) an accepted cut-off score of ≥7 is used to indicate the presence of IPV. Sample items include “Locked me in the bedroom,” “Told me that I wasn’t good enough,” “slapped me,” “harassed me at work,” etc. Although the items on the CAS can be grouped into four dimensions of Severe combined abuse, Emotional abuse, Physical abuse and harassment. Hegarty et al. (2005) also permitted summing up all the items to obtain a composite score of IPV. The CAS has recorded good reliability and validity in a number of studies. Hegarty et al. (2005) reported Cronbach’s alpha coefficient for the composite scale to be α = .85.
Need for closure
NFC was measured using the Need for Closure Scale (NFCS) Short Version, (Webster & Krulanski, 1994). It is a 15 items 6-point Likert Scale. Participants are requested to give their ratings on a 6-pointLikert type scale (1 = Strongly Disagree, 2 = Moderately disagree, 3 = Slightly disagree, 4 = Slightly agree, 5 = Moderately agree, 6 = Strongly Agree). Sample items on the NFCS include, “I don’t like situations that are uncertain,” “I dislike questions which will be answered in many different ways,” “I find that a well ordered life with regular hours suits my temperament, “I feel uncomfortable when I don’t understand the reason why an event occurred in my life”, etc. The NFCS has recorded good reliability in previous research. For instance, Pierro et al., (2005) reported Cronbach’s alpha coefficients for the scale to be α = .81.
Traumatic bonding
Summary of reliability and validity fit indices for measures used in the study.
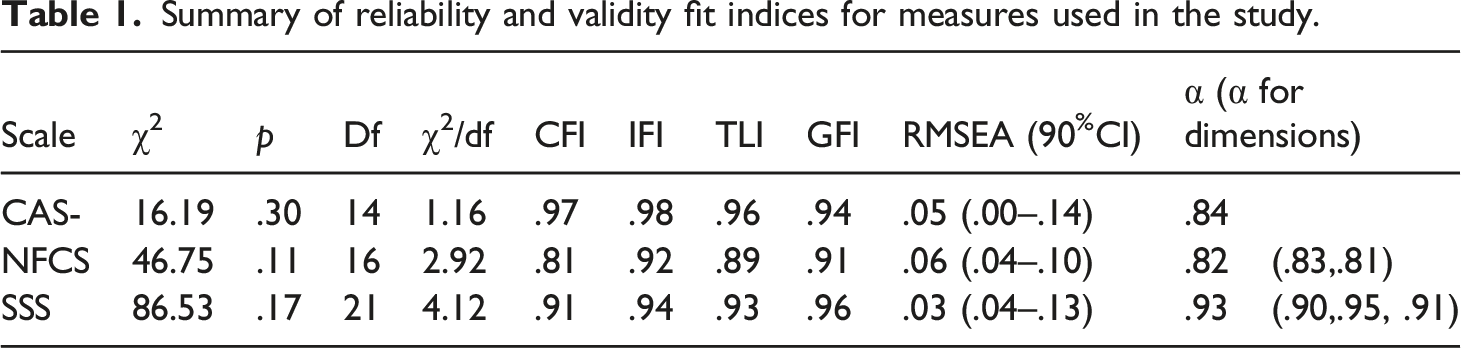
Note: α = Cronbach’s alpha (> 0.6 suggests adequate internal reliability, < 0.6 suggests poor internal reliability; values in brackets represents co-efficient for dimensions) CFI: comparative fit index (> 0.95 suggests good fit, > 0.9 suggests adequate fit, < 0.9 suggests poor fit); TLI: tucker Lewis Index (> 0.95 indicates good fit, > 0.9 suggests adequate fit, < 0.9 suggests poor fit); RMR: root mean residual (< 0.05 suggests good fit, < 0.08 suggests adequate fit, > 0.08 suggests poor fit); GFI: Goodness of fit Index (> 0.95 indicates good fit, > 0.9 suggests adequate fit, < 0.9 suggests poor fit) RMSEA: root mean square error of approximation (< 0.05 is good fit, < 0.08 is adequate fit, > 0.08 is poor fit) CI: confidence interval.
Analysis
A Pearson’s correlation (r) analysis was performed on the demographic factors, predictors, and dependent variables in the research. The correlation was chosen based on Urbina’s (2014) emphasis on its utility as a major tool in demonstrating interconnections between: (a) scores on different tests; (b) test scores and non-test (demographic) variables; (c) scores on parts of tests and whole tests; and (d) scores on various parts of tests and non-test variables. For the mediation analysis, Hayes (2018) PROCESS macro for SPSS Model 4 was used, which employs a regression-based, path-analytical framework which would estimate the path coefficients in the mediator model and generate bias-corrected bootstrapped confidence intervals (CI) for total and particular indirect relationships of IPV on TB dimensions via NFC. Because it outperforms Sobel’s test, the PROCESS module is now the most often used approach in testing mediation theories.
Ethical consideration
Ethical concerns revolve around confidentiality and anonymity of data. These concerns was mitigated as participants were asked for informed consent and the data was handled confidentially using appropriate protocols including anonymization of data and results. The study protocol received ethical approval from the University of Uyo, Department of Psychology Ethics Committee.
Results
Hayes PROCESS macro results of total effects of IPV, Need for closure on dimensions of traumatic bonding with age, years in marriage and educational qualification of participant and spouse as covariates.
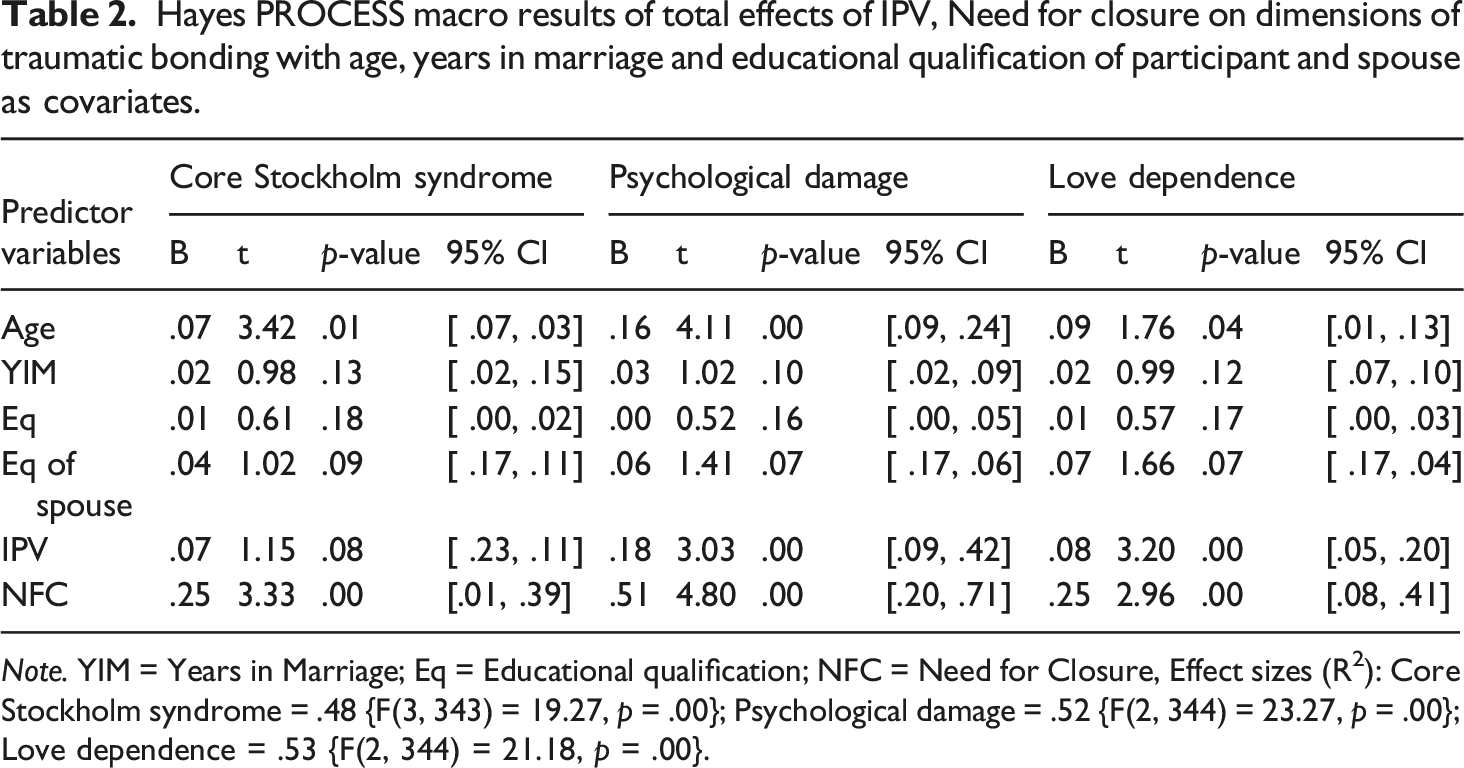
Note. YIM = Years in Marriage; Eq = Educational qualification; NFC = Need for Closure, Effect sizes (R2): Core Stockholm syndrome = .48 {F(3, 343) = 19.27, p = .00}; Psychological damage = .52 {F(2, 344) = 23.27, p = .00}; Love dependence = .53 {F(2, 344) = 21.18, p = .00}.
Completely standardized bootstrap tests of mediating effects of NFC on association of IPV with traumatic bonding.
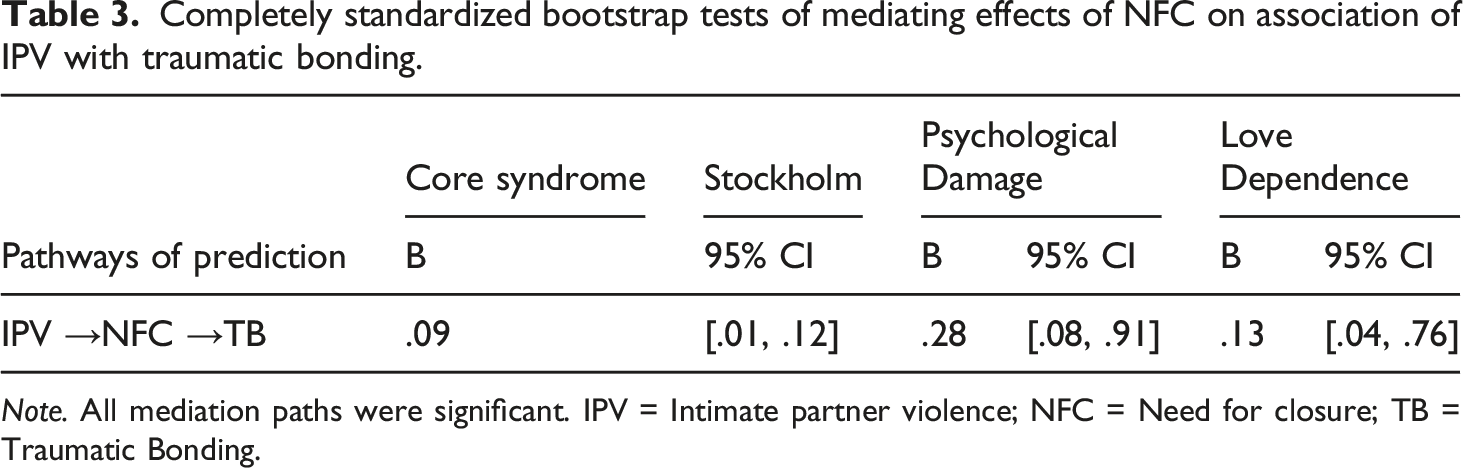
Note. All mediation paths were significant. IPV = Intimate partner violence; NFC = Need for closure; TB = Traumatic Bonding.
Discussion
The purpose of this study was to evaluate the roles of NFC in the association of IPV and TB. As expected, findings indicated that IPV and NFC were positively linked to the dimensions of TB. We also observed evidence that NFC mediated the relationship between IPV and TB, implying that NFC does serve as a pathway to the development of TB in victims of IPV. NFC strengthened IPV’s effect on TB. Despite little research on NFC’s influence on IPV and TB dimensions, there is essentially no evidence that NFC mediates other outcomes (Bartholomew & Horowitz, 1991; Drigotas & Rusbult, 1992; Finkel & Rusbult, 2008; Karavasilis et al., 2003). Of the three components of TB, core Stockholm syndrome was the least influenced by IPV. However, NFC’s mediation of IPV and TB dimensions was strongest for core Stockholm syndrome. This could be because Core Stockholm syndrome predisposes a victimized spouse to excuse violent behavior by their partners while remaining in the abusive relationship (Graham et al., 1995). This means that in the event of IPV, victims with high NFC are more likely to excuse and explain away the abusive actions of their partners. This is possible because the need for closure indicates a desire for a solid solution to any situation, any response, as opposed to ambiguity and uncertainty (Kruglanski, 1989) and therefore victims of IPV who have high NFC would desire to eliminate all possible ambiguities and uncertainties causing IPV and by so doing, may stay longer in an abusive relationship than their counterparts with lower NFC. This finding provides support for Drigotas and Rusbult (1992) dependency model of breakups which posits that some individuals remain in unsatisfying relationships due to their dependence on the other person and the relationship as a whole. Partners with high NFC continue to stay in abusive relationships and view alternative relationships, no matter how enticing they seem, as having less predictability as compared to their already established relationships. Hence, their high NFC may make them choose to remain in an abusive relationship as against trying new ones which may be uncertain.
Being mindful and knowledgeable of IPV perpetrators' and perspectives' mental states may be problematic, leading victims to accept and rationalize violent behaviors by abusive partners. As a result, they may continue to blame themselves (Alix et al., 2020; Effiong et al., 2022; Ullman et al., 2014) and regard themselves as the source of the abuse (Veletsianos et al., 2018). From a holistic standpoint, core Stockholm syndrome suggests justification of the partner’s angry behavior; self-blame for the partner’s angry behavior; allying with the partner against others; and projection of one’s victim status onto the abuser; and will be exacerbated in victims who have a NFC. This is consistent with the findings of Regehr et al., (2002), who investigated the association between NFC and trauma in ambulance paramedics and discovered that paramedics with more capacity to seek closure with patients were more vulnerable to trauma symptoms.
Need for closure (NFC) was also significant in the pathways from IPV to psychological damage, implying that NFC is yet another mechanism by which IPV is translated and escalated into psychological damage. This also suggests that IPV victims with high NFC may experience more psychological damage than those with less NFC. Depression, low self-esteem, loss of identity, and other interpersonal troubles are all manifestations of psychological damage (Effiong et al., 2022). IPV survivors who have experienced psychological trauma may be dissatisfied and have low self-esteem (Péloquin et al., 2011). Based on our findings, it is possible that victims of IPV may be experiencing these feelings more frequently because, rather than leaving an abusive relationship, they seek closure and make excuses for the violent partner’s actions. People with a high NFC and who have experienced IPV may be prone to responding emotionally to their partners’ rage, anguish, and aggression, and rather than leaving the abusive relationship, they may wish to stay and assist, subjecting themselves to further psychological damage. This is consistent with the findings of Lyons and Brewer (2021) as well as Effiong et al. (2022).
The pathways from IPV to love dependency were also mediated by NFC, indicating that NFC again influences IPV victims' love dependency. IPV victims with greater NFC may become more dependent on the love obtained from their abusive relationships than their counterparts who are lower in NFC. Even though there is limited data to back up this claim, similar studies on intimate relationships have revealed a correlation between the need for closure and dyadic partnerships. Finkel and Rusbult (2008), Fritz and Helgeson (1998), Rusbult and Martz (1995), Effiong et al. (2022) and Moreira and da Costa (2020) also suggested that, while a desire to make personal sacrifices for the sake of relationship maintenance is closely correlated with relationship satisfaction, an increased desire to do so can lead to deprivation of one’s own well-being. This notion has been supported by research e.g., (Phillip et al., 2020) in situations with severe effects (i.e., physical and psychological abuse) as well as those with more widespread unhappiness.
Implications of the findings
The NFC’s considerable mediation effects on the correlation between IPV and aspects of TB imply that victims' subjective emotional experiences may play important roles in decisions to leave or remain in an abusive relationship. Because of the ongoing need for conflict resolution, NFC may more readily allow forgiveness, insuring the continuation of the connection with the partner and restoring an active role in the relationship by taking accountability for the perpetrator’s behavior. According to Margherita & Troisi, (2014), this might illustrate why self-blaming and silence are so common in IPV. Research has demonstrated that IPV is more difficult to notice from the victims' perspective (Hirigoyen, 2004), which may be owing to the levels of NFC discovered in our study’s victims.
The findings that NFC mediated the transition from IPV to love dependency have significance for marital counseling. Emotion-Focused Couple Therapy (EFT; Greenberg & Johnson, 1988; Greenberg, 2004), which seeks to reshape the affectional system by discovering partners' closure with one another’s emotional experiences and affectional needs, may be especially beneficial in dealing with love dependency in the context of IPV. It is possible that when partners learn to recognize and embrace the appropriate degrees of need for closure (when to seek closure and when not to), they will reach a level ground where the impact of IPV on love dependency will be refined. As this occurs, different methods of reducing IPV may be implemented in order to build a sense of safety and secure attachment connection in the relationship (Péloquin et al., 2011). It is important to highlight, however, that NFC compels partners to examine unacknowledged attachment needs and feelings, which places them in a vulnerable position and may jeopardize their safety in the setting of extreme IPV. In such cases, Péloquin et al., (2011) advocate that partners work on attachment difficulties and anger management on their own before engaging in couples therapy with their spouse.
As was observed, the mediation by both aspects of NFC was reported to be stronger for psychological damage than for love dependency and core Stockholm syndrome. On the one hand, this may imply that the most common type of TB in our community is psychological damage. On the other hand, this indicates that more focus should be placed on the psychological damage induced by IPV. As our participants were all women, we adopted from earlier research findings (Finkel & Rusbult, 2008; Fritz & Helgeson, 1998; Rusbult & Martz, 1995) that the mediation by NFC on the correlation between violence and romantic relationships may persist only for females but not for men to suggest that TB is still more frequent in women than in men. This has implications for therapeutic goals and strategies. In times of limited resources and personnel, the government and policymakers should pay special attention to women, who make up the majority of TB victims.
Furthermore, by identifying NFC as a conduit or mechanism by which IPV impacts TB, we contribute to theory. We also mention the prospect of NFC being interposed between a previous experience of violence or victimization and an emotional connection with an offender. In this scenario, NFC describes how seeing violence might affect one’s motivation to remain with the offender of violence.
Limitations and suggestions for further studies
The current study was correlational in nature, which limits the ability to establish causality between variables. Future designs would be required to examine the temporal correlations between these factors.
Furthermore, because all variables were measured using self-reported measures, the intensity of the relationship between the research variables may have been overstated due to shared method variation. A multi-method strategy that includes both self-reports and behavioral observations might help researchers better understand the nature of the association between NFC and both IPV and TB. The research also only looked at women. However, as research on victimization among males grows, it will be vital for future research to look at these occurrences in men as well.
A multiplicity of demographic information about individuals may have aided the study further. Future research should collect more detailed demographic information from participants since this might be used as a control variable. This may include sexual orientation, disability, income of respondents etc. Furthermore, because our respondents had already reported to sexual assault referral centers, broad generalizations to those who had not reported IPV are inappropriate. It is critical that future research investigates these issues in a larger group of people who have IPV.
Finally, because we did not collect data on earlier trauma experiences, we could only speculate (Hartman & Morse, 2020) that the association between present IPV and NFC may be due to previous trauma experiences. This is only a suggestion, and we recommend future studies to include data on early trauma or adverse childhood experiences in order to determine exactly how previous trauma exposure may build the relationship between present victimization and NFC.
Conclusion
Need for closure (NFC) mediated the correlation between IPV and TB, demonstrating that NFC is a channel by which IPV is transcribed into TB and that IPV’s impact on TB may be amplified by NFC. NFC may promote behaviors that enhance the chance of traumatic bonding. Our findings demonstrate the effects of NFC in the formation and maintenance of traumatic bonds in IPV victims, as well as how these might be used to free people who are suffering from TB in IPV settings. Furthermore, the findings provide early data for a framework that may aid in broadening existing attachment theories, particularly in the setting of abuse and trauma.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Open research statement
As part of IARR’s encouragement of open research practices, the author(s) have provided the following information: This research was not pre-registered. The data used in the research are available. The data can be obtained by emailing: