
Abstract
This study was conducted to determine the prevalence and predictors of intimate partner violence (IPV) among female youth in an urban low-income neighborhood in Ibadan, Nigeria. Data for 298 female youth (15-24 years) were analyzed. The respondents’ mean age was 20.8 ± 2.2 years and 21% had suffered IPV within 12 months of the study. Predictors of 12-month IPV were circumstances surrounding sexual debut: coerced (odds ratio [OR] = 4.18; confidence interval [CI] = [1.49, 11.75]) or forced (OR = 4.76; CI = [1.67, 13.59]) compared with consensual sex, history of partner involvement in fights (OR = 2.78; CI = [1.02, 7.54]), and history of partners’ father beating mother (OR = 41.82; CI = [5.03, 347.80]). IPV is common among female youth in Idikan community and interventions need to target these youth and their partners.
Introduction
Intimate partner violence (IPV) comprises, “any behaviour within an intimate relationship that causes physical, sexual or psychological harm, including acts of physical aggression, sexual coercion, psychological abuse and controlling behaviours” (Heise & Garcia-Moreno, 2002, p. 89). It has been recognized as a major medical, psychological, social, and public health problem (Banyard & Cross, 2008; Exner-Cortens, Eckenrode, & Rothman, 2013; Silverman, Gupta, Decker, Kapur, & Raj, 2007; World Health Organization [WHO], 2002). Findings from the WHO multi-country study on women’s health and domestic violence revealed that about 15% to 71% of women aged 15 to 49 years had experienced physical and/or sexual violence by an intimate partner at least once in their lifetime (Garcia-Moreno, Jansen, Ellsberg, Heise, & Watts, 2006). A review of data from Demographic and Health Surveys (DHS) conducted in 10 countries also revealed that the lifetime prevalence of physical or sexual violence among currently married or cohabiting women aged 20 to 44 years ranged from 16% to 75% (Hindin, Kishor, & Ansara, 2008). Findings from some studies conducted in Nigeria similarly indicate that IPV is common among women. For example, Mapayi, Makanjuola, Fatusi, and Afolabi (2011) reported that about 37.0% of women aged 18 to 37 years attending the antenatal clinic and welfare units of a primary health center in Ile-Ife, South-West Nigeria, had experienced IPV in the 12-month period preceding their survey (Mapayi et al., 2011). Balogun, Owoaje, and Fawole (2012) reported a lifetime IPV prevalence of up to 70% among women aged 15 to 49 years in South-Western Nigeria. The discrepancies in prevalence rates across studies have been attributed to factors such as differences in methodology, definitions of violence, study population as well as willingness of study participants to disclose this information especially if privacy is not ascertained during the data collection process (Krug, Mercy, Dahlberg, & Zwi, 2002). Generally also, reporting of IPV is still a problem in many countries (Krug et al., 2002).
IPV can take many forms such as physical violence, sexual abuse, and psychological abuse (Heise & Garcia-Moreno, 2002; Watts & Zimmerman, 2002). A number of problems have been associated with IPV and these include physical injuries (Antai, 2011; Esere, Idowu, Durosaro, & Omotosho, 2009), substance use problems (Decker et al., 2014; Exner-Cortens et al., 2013), and sexual and reproductive health problems such as unintended pregnancy, nonuse of condoms, sexually transmitted diseases including HIV/AIDS (Decker et al., 2014; Hindin et al., 2008; Silverman et al., 2007), and adverse pregnancy outcome (Silverman et al., 2007).
Violence within an intimate relationship is not restricted to adults but is similarly pervasive among young people (Bruce, 2011; Stöckl, March, Pallitto, & Garcia-Moreno, 2014). Although, males also experience violence from their intimate partners, females are more likely to be victims and to suffer from the attendant effects of IPV (Gass, Stein, Williams, & Seedat, 2011; Heise & Garcia-Moreno, 2002; Krug et al., 2002). A number of studies have also documented that young age is associated with being a victim of IPV (Abramsky et al., 2011; Heise & Garcia-Moreno, 2002; Mapayi et al., 2011). Findings from studies among young females have documented IPV rates as high as 66%. For example, Stöckl et al. (2014), in their analysis of IPV among adolescents and young women aged 15 to 24 years in nine countries, found a lifetime prevalence of IPV that ranged from 19% to 66%. Decker et al. (2014), in a study among adolescents residing in vulnerable urban communities in five global cities, revealed that among ever-partnered women, past-year IPV prevalence ranged from 10.2% to 36.6%. Young females who experience IPV are exposed to similar consequences as older adult women; however, an additional challenge for them is the fact that experiencing IPV during this stage in their development is an established risk factor for violence within future intimate relationships (Bruce, 2011). Exner-Cortens et al. (2013), in their study on the “longitudinal associations between teen dating violence victimization and adverse health outcomes,” demonstrated that teenage respondents who experienced teen dating violence had a higher incidence of various adverse health outcomes such as substance abuse, suicidal ideation, and IPV victimization. These highlight the immediate and long-term negative consequences of IPV on young females. In addition, young females residing in low-income settings within cities are at increased risk of violence and several other negative health outcomes (United Nations Children’s Fund, 2012).
The Ecological Model for Understanding IPV
This article utilized the ecological model to explore the factors that predispose female youth, that is, females aged 15 to 24 years (United Nations Department of Economic and Social Affairs [UNDESA]) to IPV victimization. According to the WHO World Report on violence and health, the ecological model “explores the relationship between individual and contextual factors and considers violence as the product of multiple levels of influence on behavior” (Krug et al., 2002). The ecological model has been utilized by various researchers to explain the factors influencing violence which operate at individual, relationship, community, and societal levels (Figure 1; Krug et al., 2002).

Ecological model for understanding violence.
Individual factors are personal factors within the individual that increase the likelihood of being a victim or a perpetrator of violence. Examples of these include female gender, age, low level of education, substance abuse, previous experience to violence, and so on. Female youth residing within low-income communities are more likely to have low levels of education, be unemployed or engaged in menial jobs, and have a history of witnessing parental violence compared with their counterparts residing in higher income communities (Krug et al., 2002; Stöckl et al., 2014). Within the ecological model, relationship-level factors are those which involve close social interactions between the individual and people in his or her family or immediate environment and the influence of these relationships on violence perpetration or victimization. Relationship-level factors predisposing female youth in low-income communities to IPV include discord within their intimate relationships, being in relationships with men who have lower levels of education, are unemployed, have multiple partners, exhibit controlling behavior, use substances, and who experienced violence when growing up (Krug et al., 2002; Uthman, Lawoko, & Moradi, 2010). Community-level factors refer to the community contexts, for example, neighborhoods, workplaces, and schools within which social relationships are domiciled. Within the community, factors such as low levels of education among the community members, high levels of poverty and unemployment, and low socioeconomic status of women influence the rates of IPV (Heise & Garcia-Moreno, 2002; United Nations Children’s Fund, 2012). The societal level includes factors within the society at large such as institutional, community, and public policies and laws that regulate or support healthy actions and practices. Other societal-level factors promoting IPV within low-income communities include weak legal sanctions against IPV, sociocultural values and norms that view IPV as acceptable, and norms that associate manhood with dominance and aggression (Heise & Garcia-Moreno, 2002; Krug et al., 2002; McLeroy, Bibeau, Steckler, & Glanz, 1988; U.S. Department of Health and Human Services, 2005). The ecological model when applied to violence is also useful in the development of interventions that target key actors or institutions at the different levels of influence.
In spite of the fact that young females are at higher risk for IPV compared with their older counterparts, there is a paucity of published research on IPV among them (Russell et al., 2014) especially in developing countries like Nigeria. Furthermore, available studies among this vulnerable category of women are usually school-based (Russell et al., 2014; Swart, Seedat, Stevens, & Ricardo, 2002) and/or health-facility based (Mapayi et al., 2011). These would miss out on a significant proportion of females residing in these poor communities, because many of them already have limited access to amenities such as education and health care (United Nations Children’s Fund, 2012). The focus of this article was therefore to determine the prevalence and predictors of IPV among female youth aged 15 to 24 years residing in Idikan community, a densely populated, low-income urban community in Ibadan North-West Local Government Area (LGA), Oyo state, Nigeria. Our findings would add to the existing body of knowledge on IPV among female youth in developing countries like Nigeria and also provide data required to develop interventions targeting this category of females. Data for this article were from a larger cross-sectional study on IPV among women of reproductive age in married/current relationships residing in a low-income community (Idikan) in southwestern Nigeria.
Method
This was a cross-sectional community-based study and we analyzed data for young women aged 15 to 24 years residing in Idikan community, Oyo state, Nigeria.
Study Area
Idikan community is an inner core community in Ibadan North–West LGA, Oyo state, Nigeria (Lawoyin et al., 2004). It is a densely populated area comprising mainly of people of Yoruba ethnicity. Most families are polygamous with large family sizes comprising grandfathers, uncles and aunts, and grandchildren residing in smaller apartments or rooms all located within the family compound (also called “agbole”). There are established health facilities within the community providing primary care and referral services (Osamor & Owumi, 2010).
Study Participants
The study participants comprised female youth (aged 15-24 years) in current relationships. The definition of youth used in this article is in line with the United Nations’s definition which specifies that a youth is an individual aged 15 to 24 years of age (UNDESA).
Sampling Technique
Respondents were selected using a cluster sampling technique. The Idikan community is located within the inner core of the Ibadan North-West LGA. The community is composed of smaller units—compounds—and within each compound are two or more houses. Two or more extended families reside in each house. A major road runs through the community and divides it into two approximately equal and largely homogeneous neighborhoods. For this study, one half of the community was selected by balloting. All the houses within the selected neighborhood were visited and every eligible woman residing in these houses who provided informed consent was interviewed (Owoaje & OlaOlorun, 2012).
Instrument and Data Collection
Data were collected over a period of 4 months. The information was obtained from the respondents using questions from the WHO Multi-Country Study on Women’s Health and Life Events questionnaire (version 9.9) used for the WHO Multi-Country Study on Women’s Health and Domestic Violence (WHO, 2000, 2005). The data collection procedures were further informed by the safety recommendations for conducting research in domestic violence outlined in the WHO manual: “WHO Multicountry Study on Women’s Health and Domestic Violence Against Women” (WHO, 2005) and in the WHO and PATHS manual on “Researching Violence Against Women: A Practical Guide for Researchers and Activists” (Ellsberg & Heise, 2005). The Department of Community Medicine runs a community clinic within the Idikan community and the clinic home visitors assisted the research team with community entry and navigating within the community. On arrival in the family compound, the research staff introduced themselves to the household head or other adult in the household, and explained that the study was about women’s health issues. As suggested in the WHO guidelines, the research staff did not mention that questions on violence would be asked. Within each household, all women aged 15 to 45 years who were married or had been in an intimate relationship were approached to participate in the study. Each eligible respondent suggested a convenient and private location within the household/family compound where the questionnaires could be administered without interruption by her partner/husband or other family members. This was often on the porch, in the sitting room, or on the corridor or in a section within the family compound were the respondent could be free to answer the questions. The interviewers had been trained to change the topic or discontinue the interview if other people came into the room, approached the section of the home environment where the interview was being conducted, or if they had a sense that the respondent’s privacy might be breached. A few women requested to have the interviews in their workplaces which were not very far from their homes for better privacy. Information obtained included respondents’ sociodemographic characteristics, sexual history, experience of violence as a child, and history of physical and sexual violence experienced within 12 months of the study. Information on selected partner characteristics was also obtained. The response rate for the larger study among the 15- to 45-year-old married or ever-partnered women was approximately 98.6%. The current article is based on information obtained from the female youth aged 15 to 24 years.
Measures
Outcome variable
Experience of IPV victimization within 12 months of the study
Experience of at least one form of violence (physical or sexual) from an intimate partner at least once in the 12-month preceding the study.
Information on physical IPV victimization was obtained by asking respondents if their current husband/partner or any other partner had done any of the following to them within 12 months prior to the study: slapped or thrown something at respondent that could hurt the respondent; pushed or shoved respondent or pulled respondent’s hair; hit respondent with fist or something else that could hurt her; kicked, dragged, or beaten respondent up; choked or burned respondent on purpose; or threatened to use or actually used a gun, knife, or weapon against respondent.
For sexual IPV, respondents were asked if their current husband/partner or any other partner had ever done any of the following to them within 12 months prior to the study: physically forced respondent to have sexual intercourse when she did not want to, or forced respondent to do something sexual that they found degrading/humiliating. Respondents were also asked if they had sexual intercourse when they did not want to with their current husband/partner or any other partner because they were afraid of what he might do.
Explanatory/independent variables
Our choice of explanatory variables was guided by the ecological model and information from previous literature which had identified some factors associated with IPV among women (Abramsky et al., 2011; WHO, 2002). Variables were limited to selected factors at the individual and relationship levels of the ecological model. Individual-level factors studied were as follows:
Sociodemographic characteristics: respondent’s age, current relationship status (i.e., if respondent was currently married or in an intimate relationship), highest level of education, and occupation;
Sexual history: age at first sexual intercourse, number of sexual partners ever had, circumstances surrounding first sexual intercourse (consensual or forced);
History of violence: experience/witness of childhood violence by respondent;
Experience of violence by the respondent’s mother.
Relationship-level factors: These were limited to selected partner characteristics and included the following:
Partners’ sociodemographic characteristics such as age, education, employment status, type of work;
Relationship of partner to respondent (spouse or partner);
Type of marriage (monogamous or polygamous marriage);
History of partner witnessing violence as a child (whether or not his father used to beat up his mother);
History of partner being involved in physical fights; and
Use of alcohol by intimate partner
Analysis
Data were analyzed using SPSS version 20.0 software. The associations between the outcome variable (IPV in the last 12 months) and the selected characteristics were first explored using bivariate analysis (chi-square test). Following the bivariate analysis, individual and partner variables that were associated with experience of IPV within 12 months of the study at p < .1 were entered into the multiple logistic regression model (using a stepwise approach) to determine factors predicting IPV among the female youth.
Ethical approval for the study was obtained from the Oyo State Ministry of Health Ethical Review Committee. The trained research staff obtained verbal informed consent from all respondents and they were informed that they were free to refuse to participate and would not suffer any consequences if they chose not to participate. The research staff administered the questionnaires to the respondents, and confidentiality was maintained.
Results
Respondents’ Characteristics
A total of 298 female youth with a mean age of 20.8 ± 2.2 years were interviewed. More than two thirds of them, (68.1%) were currently married, 73.8% were Muslims, 66.4% had at most primary education, and 70.5% were currently working (Table 1). More than three quarters (76.2%) of the females had sexual debut when they were aged 15 to 19 years, 87.9% had ever had at most one to two sexual partners;78.2% stated that their first sexual intercourse was consensual while, 9.7% said it was forced (Table 1). Twenty-nine (9.7%) reported that their mothers had been victims of partner violence.
Respondents’ Sociodemographic and Other Characteristics.

Partner Characteristics
Information on the characteristics of the respondents’ partners is presented in Table 2. The mean age of the respondents’ partners was 26.5 ± 4.8 years, ranging from 16 to 50 years. Approximately 60% had at most secondary education and 267 (89.6%) were employed at the time of the survey. About two thirds, 106 (66.7%), of the female youth stated that their current partner was in an intimate relationship with another woman/women. Forty-seven (15.9%) women stated that their partners were currently using alcohol or other psychoactive substances, and 8.8% were frequently involved in physical fights. As many as 71.8% were aware that their partners’ fathers used to beat up their mothers.
Selected Partner Characteristics.

Denominator varies across variables because of missing data.
Only one unmarried respondent reported her partner may have relationship with other women.
Prevalence of IPV Among the Female Youth
Sixty-two (20.8%) of the female youth had experienced at least an episode of physical and/or sexual IPV in the 12 months preceding the survey; of these, 43 females had been victims of physical violence while 27 were victims of sexual violence. Of those who experienced physical violence, 43 (100%) were slapped or had something thrown at them, 18 (41.9%) were kicked/dragged/beaten up, and 17 (39.5%) were hit with a fist or something that could hurt. Twenty-four (88.9%) victims of sexual violence had sexual intercourse when they did not want to, 11 (40.7%) were physically forced to have sex, and one person was forced to do degrading sexual things (Table 3).
Prevalence and Types of IPV Experienced in the Last 12 Months.

Note. IPV = intimate partner violence.
Multiple responses.
Factors Associated With Experience of IPV in the Last 12 Months
Individual factors associated with experience of IPV in the last 12 months
About a quarter of the female youth who had their first sexual intercourse when they were aged 15 to 19 years had experienced IPV compared with their counterparts who had their first sexual intercourse when they were aged 11 to 14 years (6.5%) or 20 to 24 years old (15.0%). Circumstances surrounding sexual debut was significantly associated with IPV victimization as 37.9% of respondents who reported that their first sexual experience was forced had experienced IPV in the 12 months preceding the survey compared with 27.8% who said their first sexual intercourse was coerced and 17.6% who said their first sex was consensual (p = .021; Table 4).
Selected Respondent Characteristics Associated With IPV in the Last 12 Months.
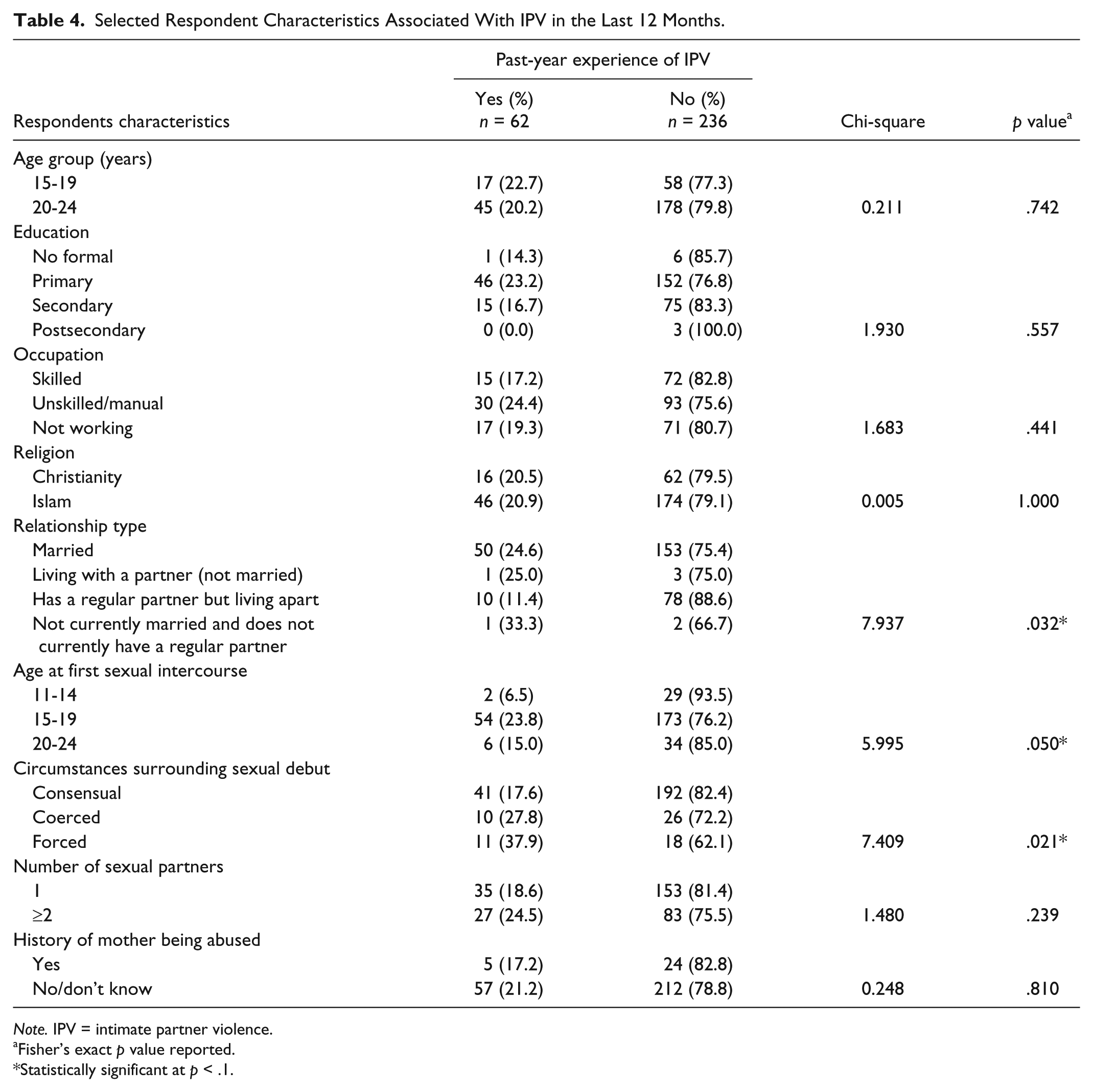
Note. IPV = intimate partner violence.
Fisher’s exact p value reported.
Statistically significant at p < .1.
Partner-related factors associated with experience of IPV in the last 12 months
Findings on the association between partner characteristics and experience of IPV in the last 12 months are presented in Table 5. A higher proportion of female youth whose partners were engaged in unskilled/manual employment (29.5%) and in semiskilled employment (16.4%) had experienced IPV in the last 12 months (p = .031). None of the two female youth whose partners were in professional occupations had experienced IPV. A significantly higher proportion of female youth (25.7%) who reported that their partners’ fathers beat their mothers experienced IPV compared with those whose partners’ fathers never beat their mothers (8.3%; p = .001). Approximately 35% of female youth whose partners had been involved in a physical fight compared with those whose partners had never been involved in a fight (19.6%) had experienced IPV (p = .081).
Association Between Partner Attributes and Experience of IPV in the Last 12 Months.

Note. IPV = intimate partner violence.
Fisher’s exact p value reported.
Statistically significant at p < .1.
Predictors of IPV in the last 12 months
Individual-level factors predicting IPV victimization in the last 12 months were age at first experience of sexual intercourse and circumstances surrounding sexual debut (i.e., whether first sexual intercourse was consensual, coerced, or forced) Table 6. Respondents who had their first sexual experience when they were aged 15 to 19 years had a significantly higher odds of IPV victimization compared with those aged 11 to 14 years (odds ratio [OR] = 8.19, confidence interval [CI] = [1.62, 41.43], p = .011). Respondents whose first experience of sexual intercourse was nonconsensual (coerced or forced) were greater than 4 times more likely to have experienced IPV compared with those whose first sexual experience was consensual.
Logistic Regression Analysis of IPV Victimization in the Last 12 Months.

Note. IPV = intimate partner violence; CI = confidence interval.
Reference category.
Only two partners were professionals and neither of their partners reported a history of IPV.
Statistically significant at p < .05.
Partner factors that were significant predictors of IPV victimization in the last 12 months were partners’ involvement in a physical fight and history of partner’s father beating his mother. Respondents who reported that their partners had been involved in physical fights were greater than 2.5 times more likely to have experienced IPV than their counterparts whose partners had not been involved in physical fights (OR = 2.78; CI = [1.02, 7.54], p = .045). Furthermore, respondents who stated that partners’ fathers used to beat their mothers were also more likely to have experienced IPV in the last 12 months compared with their counterparts whose partners’ fathers did not beat up their mothers (OR = 41.82; CI = [5.03, 347.80], p = .001).
Discussion
This study assessed the prevalence and predictors of IPV among female youth from a low-income urban community.
Prevalence of IPV
Our findings revealed that many female youth in the study area were experiencing IPV as more than a fifth (21%) reported 12-month experience of IPV. This is comparable with findings from some other studies; for instance, O’Donnell, Agronick, Duran, Myint-U, & Stueve (2009) reported a 12-month prevalence of IPV of 29% among economically disadvantaged young adult women aged 22 to 25 years in New York. Some other researchers have reported higher prevalence rates of IPV among young females; for instance, Russell et al. (2014) reported a 3-month prevalence of 39% among in-school girls in the eighth grade in Cape town, South Africa. On the whole, our findings confirm the wide range in IPV prevalence often reported within and between countries. This wide variation was also highlighted in the WHO multi-country study on IPV among adolescents and young women aged 15 to 24 years which reported a lifetime prevalence of IPV that ranged from 19% to 66% (Stöckl et al., 2014).
In the current study, we found 12-month prevalence rates of physical and sexual IPV of 14.4% and 9.1%, respectively. These are higher than corresponding values reported by Umana, Fawole, and Adeoye (2014) who found lifetime prevalence of physical and sexual IPV of 7.9% and 6.6%, respectively, among postgraduate students (aged < 20 and 35 years) in Ibadan. Our higher prevalence rates could be because, compared with the sample studied by Umana et al., our respondents were slightly younger overall, had lower levels of education, and resided in vulnerable communities. These characteristics (younger age and low levels of education) have been identified as factors that confer increased vulnerability for IPV (WHO, 2002).
Predictors of 12-Month IPV Victimization
Our study revealed a number of individual and partner-related factors that were associated with 12-month IPV. Individual factors associated with IPV (after logistic regression analysis) were (a) age at first sexual intercourse (those who had first sexual intercourse when they were 15 to 19 years old compared with those aged 11 to 14 years at first sex and (b) circumstances surrounding sexual debut—Young women who reported that their first sexual experience was not consensual or forced were more likely to have experienced IPV. Stöckl et al. (2014) similarly found that a history of nonconsensual sexual debut was significantly associated with IPV victimization. The incident of forced or unwanted sexual debut might have occurred within the 12-month period under investigation and could thus explain this finding. Another possible explanation could be that the female had remained in this abusive relationship and the violence had continued.
Partner-related factors significantly associated with 12-month IPV were history of partner being involved in a fight and partner’s father beating his mother. Other studies have similarly reported that women whose partners have a history of being involved in aggressive behavior including physical fights were more likely to be victims of IPV. O’Donnell et al. (2009), in their longitudinal study on IPV among economically disadvantaged young adult women, found that those who had a history of aggressive behavior in their middle school years were likely to perpetrate IPV as young adults. Female youth in our study who reported that their partner’s father used to beat his mother were more likely to report a history of IPV than their counterparts who did not have a similar history. Findings from existing literature have documented that a positive history of IPV between partner’s parents is an established risk for women to experience violence from their partners (Hindin et al., 2008). This phenomenon has been referred to as “inter-generational cycling of violence,” described as the effect of witnessing violence in the family as a child (Seedat, Van Niekerk, Jewkes, Suffla, & Ratele, 2009). Possible reasons which have been adduced for this include the fact that men who witnessed their fathers beating up their mothers might have grown up with the impression that this behavior is part of a relationship/marital role that gives a man the right to abuse his partner as a means of correction or discipline (Umana et al., 2014). Hence these men behave in a similar manner toward their own partners/spouses. Children who grow up witnessing violence within the family may also be wrongly socialized to thinking that this is a normal “disciplinary measure.” This finding highlights the need to target individuals who report a history of violence between their parents with appropriate interventions so that these affected children do not grow up to continue the cycle of violence within their own homes. In addition, some cultures in Africa support beating of wives as an “appropriate disciplinary measure” (Uthman et al., 2010). This fuels IPV; hence, urgent steps need to be taken to discourage this view.
Conclusion
Our findings confirm that IPV is a problem among female youth residing in low-income communities. Past experience of violence was a major factor associated with IPV among our study population as the female youth who reported a history of IPV between their own or their partners’ parents and a history of their partners being involved in physical fights were at higher risk of being victims of IPV victimization. These findings highlight the urgent need for comprehensive intervention programs to target vulnerable females as well as men within our study area. It is important to invest in primary prevention intervention efforts to prevent IPV among female youth in our study area. Our findings supported “inter-generational cycling of violence.” We thus recommend that, psychological interventions that target women and men with a history of IPV in their parents could be useful in reducing the prevalence of IPV in our study area.
Limitations
Our study has a few limitations. First, we obtained self-reported history of IPV, and the prevalence could be lower than expected as a result of information and recall bias. Some of the respondents could have withheld information regarding their personal experiences due to a general culture of silence regarding IPV in our society. We however tried to minimize this by encouraging the respondents to be open about their experiences and emphasizing that the information they provided would be useful in advocating for appropriate interventions. We made efforts to reduce recall bias by obtaining information on past-year experience of IPV in addition to a history of any past experience of IPV. Finally, our study was cross-sectional in nature; hence, we report on factors associated with IPV and these do not imply a causal relationship. However, these factors are consistent with results from other studies. Our findings thus contribute to the existing body of knowledge on IPV among female youth in socially disadvantaged communities and would be useful in developing interventions to target them.
Implications of Study Findings
Our findings emphasize the need for existing interventions to reach young females in disadvantaged neighborhoods to reduce the occurrence of IPV among them. One of the ways to reach these women could be through routine screening for violence at any point when they encounter a health professional.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.