
Abstract
Intimate partner violence (IPV) is an increasingly prevalent problem in most parts of the world including sub-Saharan Africa. However, little is known about the bonding patterns of IPV victims who decide to remain with the perpetrator despite the molestation. This study investigated the mediating role of empathy in the relationship between partner molestation and traumatic bonding among victims of IPV in Nigeria. Participants were 345 women purposively selected from female clients who visited the Sexual Assault Referral Centre (SART) Awka, Anambra State (n = 145) and the Lagos State Domestic and Sexual Violence Response Team, Lagos (n = 200). Their age ranged from 18-61 years (M=35.79; SD=8.6 years). They responded to the Composite Abuse Scale, the Basic Empathy Scale, and the Stockholm Syndrome Scale. Results of data analysis using the Hayes regression-based PROCESS macro showed that partner molestation was not significantly associated with traumatic bonding. Affective and cognitive components of empathy were positively associated with increased traumatic bonding. Estimates of indirect effects indicated that affective empathy and cognitive empathy served as pathways through which IPV was linked to dimensions of traumatic bonding. Empathy may engender tendencies that increase the likelihood for traumatic bonding. Findings highlight the dynamics of empathy in building and sustaining traumatic bonding in victims of IPV.
Intimate partner violence (IPV) is now a common type of violence and a major public health problem which violates the fundamental human rights of victims. The American Psychological Association and Presidential Task Force on Violence and the Family (1996) defines IPV as the physical, sexual, psychological, economical or stalking abuse, both concrete and menaced, perpetuated by current or ex-partners. IPV has persisted within the society and its prevalence among couples, especially female partners has increased over the years (Krug et al., 2002) and is reported to have spiked during the COVID-19 lockdowns (Lyons & Brewer, 2021; Moreira & da Costa, 2020). Specifically, IPV has soared across sub-Saharan Africa, particularly in Nigeria (Lafraniere & Lussier, 2005).
Recent reports from Nigeria, have consistently painted the precarious situation of women in abusive relationships. For instance, in Nigeria alone, informal reports on social media, Newspaper, TV and radio stations have repeatedly shown one form of IPV or sexual molestation to the other ranging from brutal injuries (Agbedo et al., 2021; Iorfa, Effiong et al., 2022; Iorfa, Onyishi et al., 2022) to deaths (Sahara Reporters New York, 2022). The World Health Organization, Department of Injuries and Violence Prevention (2005) reported that globally, one in four women experiences sexual violence by her intimate partner while the CLEEN Foundation (an NGO operating in Nigeria) reports that 1 in every 3 female respondents in their study admitted to being a victim of domestic violence and that there has been a nationwide increase in domestic violence in the past years from 21% to 30% in 2013 (CLEEN Foundation, 2013).
These reports show the rate at which IPV is happening among Nigerians. Victims of IPV are often faced with a spectrum of decisions to take regarding abuse and the abuser. One of such decisions is either to stay or to leave the abusive relationship (Rakovec-Felser, 2014). However, dynamics of culture, societal and gender role expectations make the decision to leave an intimate relationship, especially marriage a difficult one for most victims of IPV, especially women. These dynamics are further intensified in a largely patriarchal and religious society like Nigeria, where the woman may be encouraged to endure the marriage because of her children, her status in the society as well as for religious reasons (especially for religions which discourage divorce). Also, research has shown that intentions either to leave or stay in an abusive relationship are often influenced by a wide range of psychological processes one of which is traumatic bonding (Word Health Organization, 2005).
Traumatic bonding
Traumatic bonding (TB) is a strong emotional attachment between an abused person and his or her abuser and is often formed as a result of the repeated (and often times Effiong broken) cycle of violence. TB is developed as the result of ongoing cycles of abuse in which the intermittent reinforcement of reward and punishment creates powerful emotional bonds that are resistant to change (Dutton & Painter, 1981). Saunders’s (1999) attachment theory explains TB as an unresolved form of insecure attachment in which the capacity for self-regulation is impaired by the alternately abusive and protective actions of an attachment figure. Other theoretical explanations to TB are found in the works of psychodynamic theorists who have employed concepts such as masochism, repetition compulsion, and identification with the aggressor (e.g., van der Kolk, 1989) to explain how TB and other self-destructive relationships are formed. It is also logical to think that continued abusive relationships may affect the victim’s correct evaluation of the abusive situation.
Graham et al. (1995) developed a scale to measure TB in which they found that the items were largely represented by three factors (dimensions): core Stockholm syndrome, psychological damage, and love dependency. Core Stockholm syndrome described cognitive distortions and interpersonal trauma (Graham et al., 1995). These included rationalizing and/or minimizing a violent partner’s behaviour, self-blame, and reporting love in the context of fear. The core Stockholm syndrome dimension is also characterized by cognitive distortions and other strategies for coping with abuse. Psychological damage captures depression, low self-esteem, loss of sense of self and other interpersonal difficulties (Graham et al., 1995). Victims of IPV who experience psychological damage are constantly depressed and have developed low self-esteem. Most times due to the low self-esteem, they believe they are even privileged to have partners at all and are willing to keep such abusive relationships for fear of not having another partner. Psychological damage encompasses all possible emotional disruptions that victims of IPV may experience in an abusive relationship. Love dependency typifies a strong belief that one’s very survival is dependent on a partner’s love, extreme idolization, and the belief that without one’s partner there would be nothing for which to live (Graham et al., 1995). Persons high in love dependency are likely to keep up with an abusive relationship no matter the seeming costs. For them, leaving their partners may be synonymous to quitting life, because they have become dependent on the love affair (Kane & Bornstein, 2016) with such partners and the love they get from such. Persons high on love dependency may also believe that their survival is dependent on their partner’s love. In some cases, they may idolize them. Love dependent people also believe that their partner’s love and protection are more important (Messing et al., 2021) than any pain the partner may be causing them.
Since TB has been shown in research to be associated with a wide range of psychosocial processes, it is important that in studying it, researchers incorporate relevant psychological and sociological variables that may be consequent of TB, that may predict it or possibly mediate its relationship with other variables. Looking at the growing rate of IPV and the fact the TB may be prevalent as a maladaptive coping mechanism amongst victim in sub-Saharan Africa and especially Nigeria where facts and data concerning the true occurrence of domestic violence is missing, it becomes increasingly important that correlates of TB be investigated. This will help tailor proper intervention towards the victims at all levels. In this study therefore, empathy was studied as a mediator of the relationship between IPV and TB.
Empathy
Empathy has been defined as predictive accuracy (Dymond, 1949), a vicarious emotional response to the perceived emotional experiences of others (Stotland, 1969) and the capacity to understand or feel what another person is experiencing from within their frame of reference, that is, the capacity to place oneself in another’s position (Bellet & Michael, 1991). A wide range of behaviours may be regarded as being empathic. These include; feeling what someone else feels; caring about someone else; being emotionally affected by someone else’s emotions and experiences, though not necessarily experiencing the same emotions; imagining oneself in another’s situation; imagining being another in that other’s situation; making inferences about another’s mental states; and possibly a combination of two or more of the above examples.
Empathy is an essential part of emotional functioning and interpersonal cognition, making individuals particularly attentive to both the mental states and emotions of other people (Carré, Stefaniak, D'Ambrosio, Bensalah, & Besche-Richard, 2013). Empathy according to Riess (2017) requires an exquisite interplay of neural networks and enables individuals to perceive the emotions of others, resonate with them emotionally and cognitively, to take in the perspective of others, and to distinguish between their emotions and those of others. Empathy is often classified into various subtypes, some of which include affective and cognitive empathy.
Affective (emotional) empathy (AE) refers to the capacity an individual has to respond with an appropriate emotion to another individual’s emotional states (Rogers, Dziobek, Hassenstab, Wolf & Convit, 2007). Davis (1983) opined that affective empathy could be further divided to reflect two subdomains which Rogers et al. (2007) defined as; empathic concern which is sympathy and compassion for others in response to their sufferings; and personal distress which is self-centered feelings of discomfort and anxiety in response to the sufferings of others. These categories have been upheld in other research (see Minio-Paluello, Lombardo, Chakrabarti, Wheelwright, & Baron-Cohen, 2009) and all sum up to a composite measure of affective/emotional empathy. Cognitive empathy (CE) refers to the capacity to understand another person’s perspective or mental states (Gerace, Day, Casey, & Mohr, 2013) and is largely related to the phenomena of theory of mind (Rogers et al., 2007).
A considerable number of recent research (e.g., Kanske, Böckler, Trautwein, Parianen, Lesemann, & Singer, 2016; Kanske, Böckler, Trautwein, & Singer, 2015) have argued that someone who strongly empathizes emotionally may not necessarily be good in understanding other people’s perspective therefore suggesting that affective and cognitive empathy may be very independent from one another. This stand that the two domains of empathy (affective and cognitive) exists and are mutually exclusive has been re-iterated in research as evidenced in the development of instruments to measure empathy (e.g., Spreng et al., 2009; Carré-Perrot et al., 2013).
Empathy as mediator
Research linking empathy to a wide range of psychological outcomes has suggested the validity of empathy as an independent and researchable phenomenon. (Riess, 2017) opined that empathy plays a critical interpersonal and societal role, enabling sharing of experiences, needs, and desires between individuals and providing an emotional bridge that promotes prosocial behavior. Empathy, is an “antecedent to attachment” (Groh et al., 2017) and according to Masten et al. (2005) empathy may have a bi-directional relationship with attachment, i.e., influence bonding/attachment and at the same time be influenced by bonding/attachment. Empathy has also been shown to be influenced by exposure to violence (Hartman & Morse, 2020).
Most research relating empathy and trauma have investigated the effects of trauma on the development of empathy and not the other way around. These studies have found that persons who reported experiencing a traumatic event in childhood had elevated empathy levels compared to those who did not experience a traumatic event (Greenberg, Baron-Cohen, Rosenberg, Fonagy, & Rentfrow, 2018) and that increasing severity of past adversity predicts increased empathy, which in turn, is linked to a stable tendency to feel compassion for others in need (Lim & DeSteno, 2016). Others have highlighted the need for empathy in paramedics and other trauma workers (Moloney & Gair, 2015). Regehr et al. (2002) explored the relationship between empathy and trauma in ambulance paramedics and found that paramedics with higher ability to empathize with patients were more susceptible to developing more complex traumatic conditions. MacRitchie and Leibowitz (2010) observed that empathy was a consistent moderator between previous experience of trauma and a secondary form of trauma similar to traumatic bonding.
The present study therefore also tries to investigate the roles empathy may be playing in traumatic bonding among victims of IPV. In summary, the present research seeks to advance knowledge and add to the available literature on traumatic bonding. Overall, it will help throw light on the mediating roles of empathy (CE and AE) in the relationship of IPV and TB. The findings from this research will help inform therapeutic approaches/strategies as well as policies regarding intimate partner victimization in sub-Saharan Africa. The model shows the direction of the hypotheses which their formulation was guided by studies mentioned above. The hypotheses are; i) IPV will predict dimensions of TB; ii) CE will predict dimensions of TB; iii) AE will predict dimensions of TB; iv) CE will mediate the relationship of IPV and dimensions of TB; and v) AE will mediate the relationship of IPV and dimensions of TB (Figure 1). Conceptual model of the mediating role of empathy on the association of IPV and TB.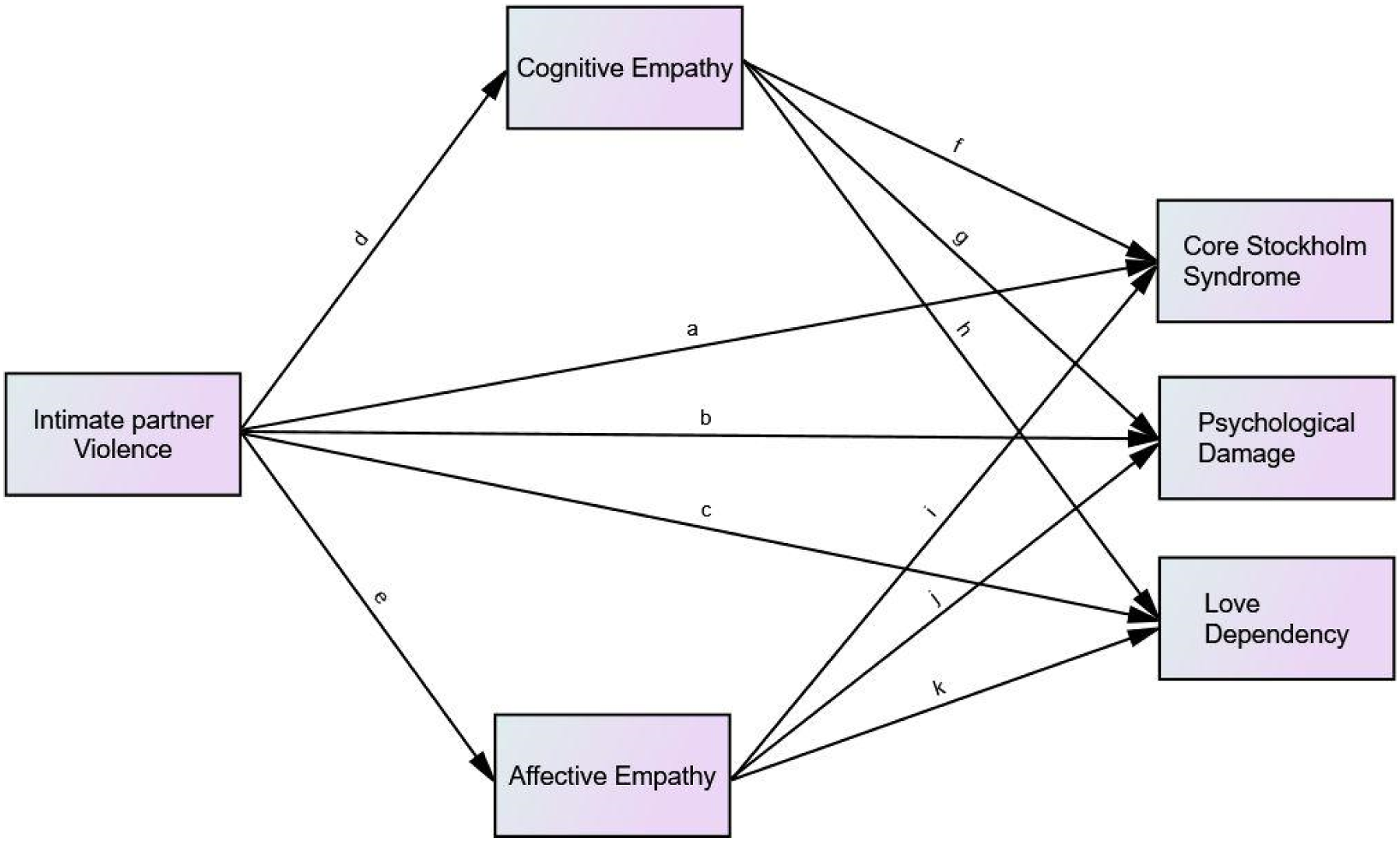
Method
Participants
Participants were 345 women purposively selected from female clients who visited the Sexual Assault Referral Centre (SART) Awka, Anambra State (n = 145) and the Lagos State Domestic and Sexual Violence Response Team, Lagos (n = 200). Their age ranged from 18-61 years (M = 35.79; SD = 8.6 years). The mean number of years in marriage was 9.8 years (SD = 7.01). As regards educational qualification, 0.9% (3) of the respondents had a Masters in Business Administration, 9.6% (32) had an Ordinary National Diploma, 55.8% (187) had an Higher National Diploma/Bachelor of Science, 10.4% (35) had either a Master of Science or a Doctor of Philosophy Degree, 6.9% (23) had an National Certificate in Education, 15.2% (51) had a Secondary School Certificate in Education, 1.2% (4) had a First School Leaving Certificate, while 10 persons did not indicate their educational qualification. As regards educational qualification of spouse, 52.4% (152) had a Higher National Diploma/Bachelor of Science, 15.2% (44) had either a Master of Science or a Doctor of Philosophy Degree, 21.4% (62) had a Secondary School Certificate in Education, 6.2% (18) had an Ordinary National Diploma, 3.4% (10) had a FSLC, 1.2% (4) had an NCE, while 55 persons did not indicate the educational qualification of their spouse.
Procedure
Approval was obtained from the management of the domestic violence response intervention offices to allow a research assistant to recruit participants for the research. Once a visitor to the facility identified to the receptionist that she is a victim of intimate partner violence, the research assistant approached the individual, established rapport and requested her to participate in the research while establishing their rights to informed consent and confidentiality. The average time from establishment of contact to filling and returning of the questionnaire form was within 20–25 minutes. A total of 360 questionnaires were printed and distributed at the two centers. However, only 350 were retrieved giving a return rate of 97.2%. Out of the 350 returned copies of the questionnaires form, 5 were dropped due to either incompleteness or irregular response patterns giving a response rate of 95.8%. Specifically, 150 questionnaires forms were distributed at the SART Awka, Anambra Stateand 150 were retrieved, giving a return rate of 100% while 205 were distributed at the Lagos State Domestic and Sexual Violence Response Team, Lagos and 200 were retrieved, giving a return rate of 97.6%.
Measures
Intimate partner violence
IPV was measured using the short version of the Composite Abuse Scale (CAS) developed by Hegarty et al. (2005). The short version CAS is a 30-item 6 point Likert Scale containing actions by an intimate partner that constitute emotional or physical abuse and provides data on the prevalence of intimate partner violence experienced by victims. Respondents were required to rate the frequency of abuse in the past year on a scale ranging from 5 = daily, 4 = once per week, 3 = once per month, 2 = several times, 1 = only once, 0 = never). According to MacMillan et al. (2009) an accepted cut-off score of ≥7 is used to indicate the presence of IPV. Sample items include “Locked me in the bedroom,” “Told me that I wasn’t good enough,” “slapped me,” “harassed me at work,” etc. Although the items on the CAS can be grouped into four dimensions of Severe combined abuse, Emotional abuse, Physical abuse and harassment. Hegarty et al. (2005) also permitted summing up all the items to obtain a composite score of IPV. The CAS has recorded good reliability and validity in a number of studies. Hegarty et al. (2005) reported Cronbach’s alpha coefficient for the composite scale to be α = .85.
Empathy
Empathy was measured using the Basic Empathy Scale (BES), (Jolliffe & Farrington, 2006) It is a 20 items 5-point Likert Scale. Participants are requested to give their ratings on a 5-pointLikert type scale (1 = Strongly Disagree, 2 = Disagree, 3 = Neither Agree nor Disagree, 4 = Agree, 5 = Strongly Agree). Jolliffe and Farrington (2006), proposed a two-factor model in which nine items assess cognitive empathy (Items 3, 6, 9, 10, 12, 14, 16, 19, 20), and 11 items assess affective empathy (Items 1, 2, 4, 5, 7, 8, 11, 13, 15,17, 18). In the two-factor conceptualization, the BES included seven reversed items and the scores could range from 20 (deficit in empathy) to 100 (high level of empathy). Sample items on the cognitive empathy dimension include, “I can understand my friend’s happiness when she/he does well at something,” “I find it hard to know when my friends are frightened,” “When someone is feeling ‘down’ I can usually understand how they feel,” etc. Sample items on the affective empathy dimension include, “My friends’ emotions don’t affect me much,” “After being with a friend who is sad about something, I usually feel sad,” “I get frightened when I watch characters in a good scary movie,” etc. The BES has recorded good reliability in previous research. For instance, Pechorro et al. (2017) reported Cronbach’s alpha coefficients for the subscales to be α = .81 and α = .86 for the affective and cognitive dimensions respectively.
Traumatic bonding
Traumatic bonding was measured using the Stockholm Syndrome Scale (SSS, Graham et al., 1995). The SSS is a 49 items, 7-Point Likert Scale. Participants are requested to respond to the items on a 7-point Likert type scale ranging from 1(I NEVER feel this way) to 7(I ALWAYS feel this way). The original 49-item SSS (Graham et al., 1995), was later reduced to 24 in subsequent research (George, 2013) to limit participant fatigue and dropout rates (Galesic & Bosnjak, 2009). The items were selected based on how strongly they loaded onto each component of Stockholm syndrome in the original study. Weakly correlated and repetitious items were removed. These items are used to ascertain three dimensions of Stockholm syndrome/traumatic bonding. These are Core aspects of Stockholm syndrome; Psychological Damage and Love dependence. The SSS includes items such as “If I give my partner enough love, s/he will stop getting so angry at me,” “I both love and fear my partner,” “I do not want others to know how angry my partner gets at me,” etc. for the Core Stockholm syndrome dimension, “I do not know who I am,” “I cannot make decisions,” “When others ask me how I feel about something, I do not know” etc. for the Psychological Damage dimension and “My partner’s love and protection are more important than any hurt s/he might cause me,” “Without my partner, I have nothing to live for,” “If my relationship were to break up, I would feel so much pain that I would want to kill myself,” etc. for the Love Dependence dimension. The Cronbach’s alphas for the subscales as reported by the developers are .94 (Core Stockholm Syndrome), .89 (Psychological Damage), and Love Dependence.
Summary of reliability and validity fit indices for measures used in the study.
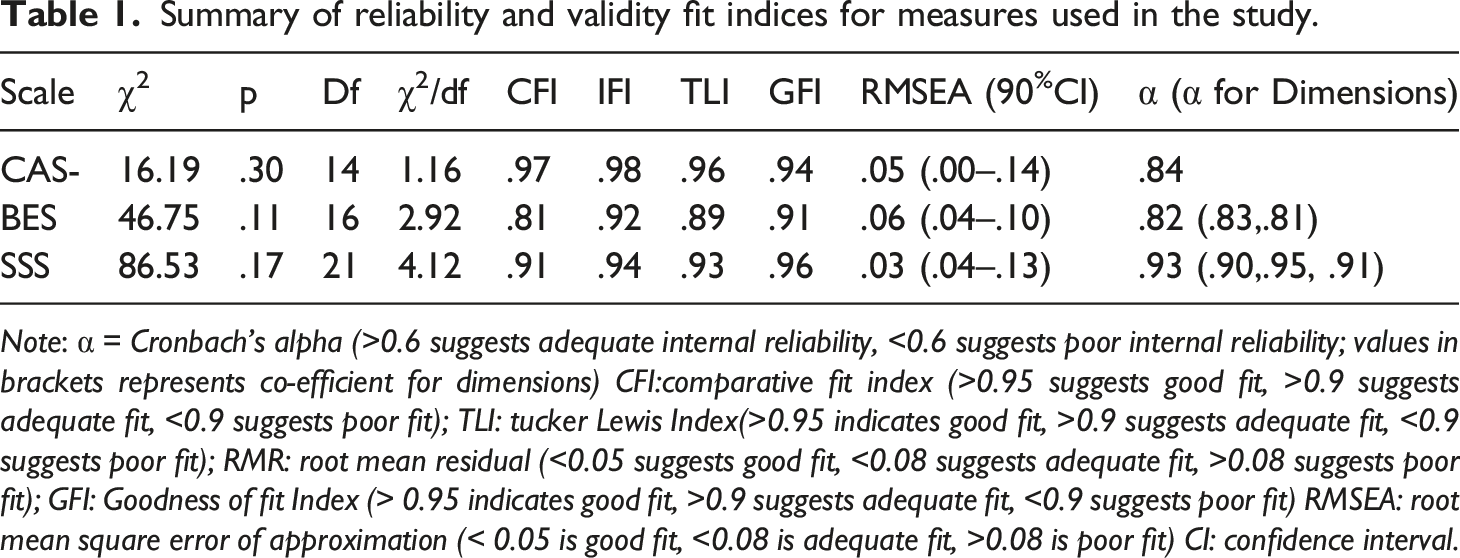
Note: α = Cronbach’s alpha (>0.6 suggests adequate internal reliability, <0.6 suggests poor internal reliability; values in brackets represents co-efficient for dimensions) CFI:comparative fit index (>0.95 suggests good fit, >0.9 suggests adequate fit, <0.9 suggests poor fit); TLI: tucker Lewis Index(>0.95 indicates good fit, >0.9 suggests adequate fit, <0.9 suggests poor fit); RMR: root mean residual (<0.05 suggests good fit, <0.08 suggests adequate fit, >0.08 suggests poor fit); GFI: Goodness of fit Index (> 0.95 indicates good fit, >0.9 suggests adequate fit, <0.9 suggests poor fit) RMSEA: root mean square error of approximation (< 0.05 is good fit, <0.08 is adequate fit, >0.08 is poor fit) CI: confidence interval.
Design/statistics
This is a survey research and cross-sectional design was adopted in the study. Pearson’s correlation (r) analysis was conducted among the study’s demographic variables, predictors and dependent variables. The choice of the correlation was based on Urbina’s emphasis (Urbina, 2014) on its utility as a major tool in demonstrating linkages between: (a) scores on different tests, (b) test scores and non-test (demographic) variables, (c) scores on parts of tests and scores on whole tests, and (d) between scores on different parts of tests (e.g., traumatic bonding subscales) and non-test variables. For the mediation analysis, Model 4 of Hayes (2018) PROCESS macro for SPSS which uses a regression-based, path-analytical framework, was employed to estimate the path coefficients in the mediator model and generate bias-corrected bootstrapped confidence intervals (CI) for total and specific indirect relationships of IPV on dimensions of TB through cognitive and affective empathy. Given its superiority to Sobel’s test, the PROCESS module is currently the commonly used method in tests of mediation hypotheses.
Results
Hayes PROCESS macro results of total effects of IPV, cognitive empathy and affective empathy on dimensions of traumatic bonding with age, years in marriage and educational qualification of participant and spouse as covariates.
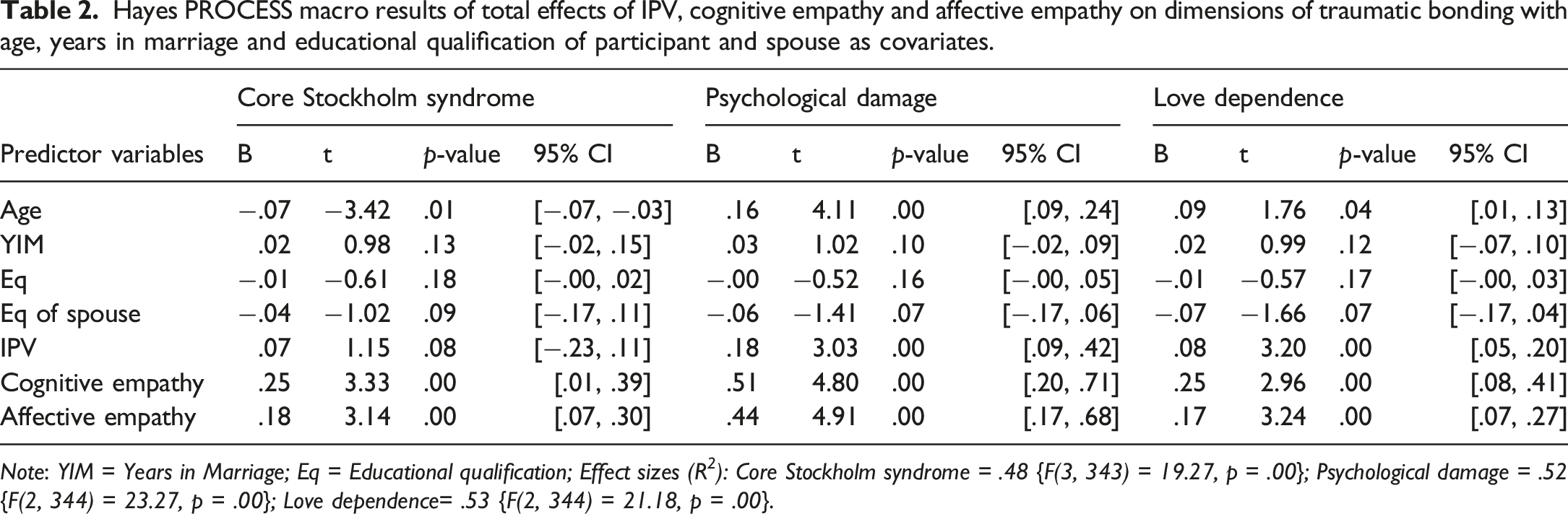
Note: YIM = Years in Marriage; Eq = Educational qualification; Effect sizes (R 2 ): Core Stockholm syndrome = .48 {F(3, 343) = 19.27, p = .00}; Psychological damage = .52 {F(2, 344) = 23.27, p = .00}; Love dependence= .53 {F(2, 344) = 21.18, p = .00}.
Completely standardized bootstrap tests of mediating effects of empathy on association of IPV with traumatic bonding.
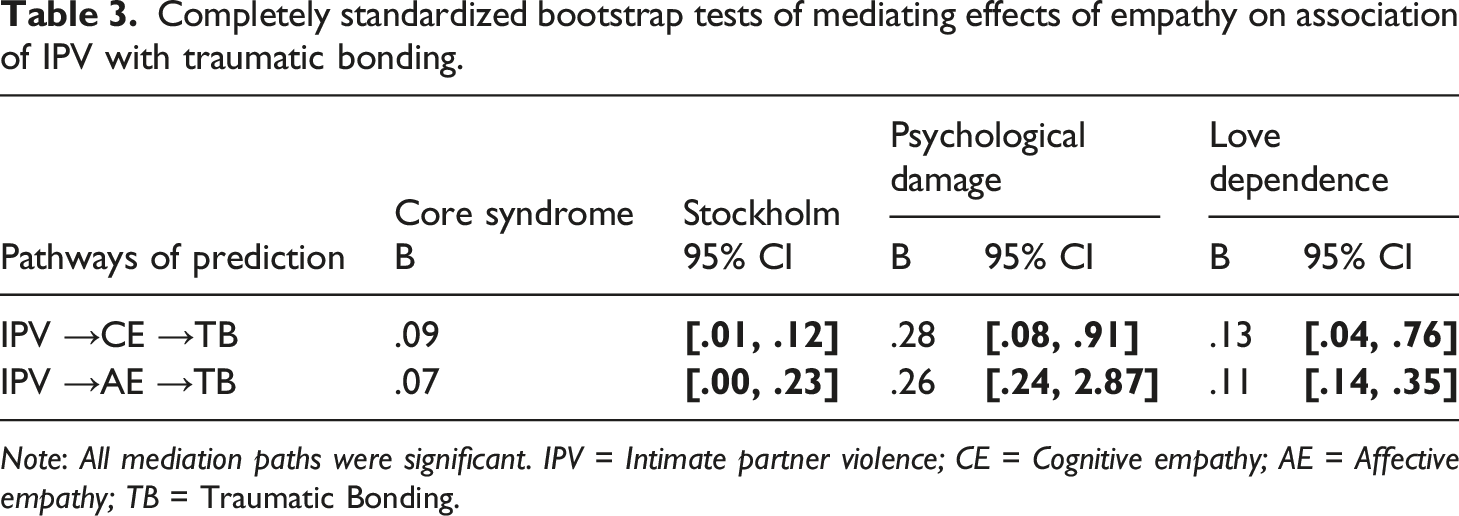
Note: All mediation paths were significant. IPV = Intimate partner violence; CE = Cognitive empathy; AE = Affective empathy; TB = Traumatic Bonding.
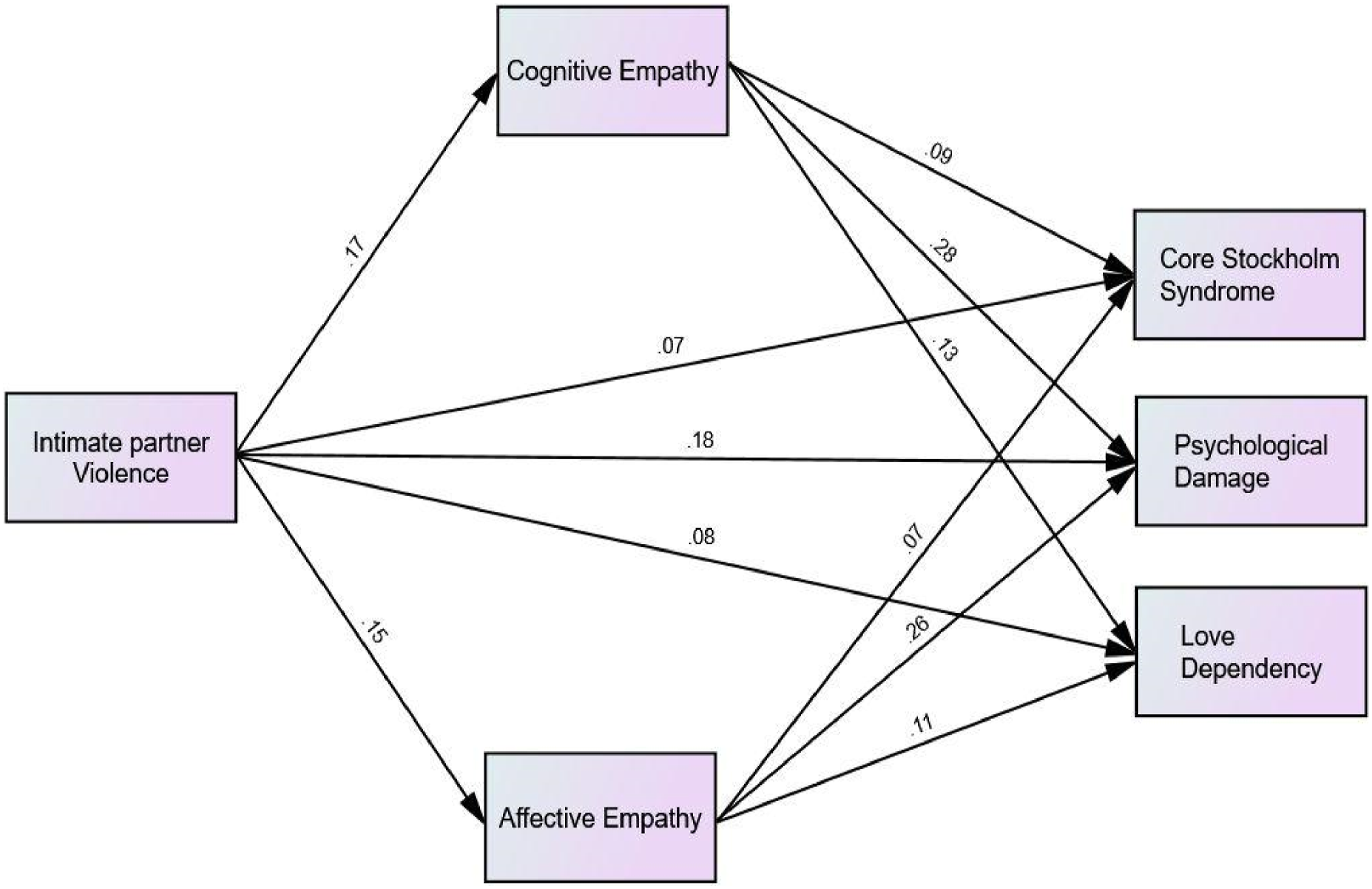
Path diagram showing the mediating role of empathy on the association of IPV and TB.
Discussion
We obtained evidence that empathy mediated the relationship between IPV and TB suggesting that empathy is a pathway through which IPV is translated into TBand that the influence of IPV on TB is intensified via empathy. The dimensions of empathy (i.e. CE and AE) all strengthened the impact of IPV on TB. Specifically, cognitive empathy appeared to be more responsible for higher levels of TB in victims of IPV than affective empathy. Although there is lack of research that has specifically investigated the mediation of IPV and dimensions of TB by CE and AE, there is some evidence that empathy mediates other outcomes (Greenberg et al., 2018; Lim & DeSteno, 2016; MacRitchie & Leibowitz, 2010; Moloney & Gair, 2015; Riess, 2017).
Among the three dimensions of TB, Core Stockholm syndrome was the least influenced directly by IPV and also indirectly through CE and AE. The path through CE accounted for a higher impact on core Stockholm syndrome than the path through AE. This mediation by CE and AE suggests that victims of IPV who are higher in empathy may experience more levels of core Stockholm syndrome than those who are not. Core Stockholm syndrome makes it possible that a victimized partner will explain away violent acts by their partners and still choose to remain in an abusive relationship (Graham et al., 1995) and due to the present findings; we have observed that this may be intensified in the presence of empathy. This is possible because empathy entails the capacity to understand another person’s perspective or mental states (Gerace et al., 2013).
Being thoughtful and understanding with the mental state of IPV perpetrators and perspectives may be maladaptive as it may lead victims to accepting and rationalising violent acts by abusive partners. They may therefore begin to engage in self-blame (Alix et al., 2020; Swannell et al., 2012; Ullman et al., 2014) and see themselves as the cause of the abuse (McElvaney et al., 2014; Veletsianos et al., 2018). Looking at it from a holistic perspective core Stockholm syndrome is suggestive of rationalization of the partner’s angry behaviour, self-blame for the partner’s angry behaviour, siding with partner against others, projection of one’s victim status onto the abuser, and will be intensified in the victims if they have high levels of empathy. This is in support of Regehr et al. (2002) who explored the relationship between empathy and trauma in ambulance paramedics and found that paramedics with higher ability to empathise with patients were more susceptible to trauma symptoms.
CE and AE also mediated the paths from IPV to psychological damage suggesting that empathy is again a pathway through which IPV is translated and intensified into psychological damage. This also means that victims of IPV who are higher in empathy may experience more levels of psychological damage than those who are not. Psychological damage encompasses depression, low self-esteem, loss of sense of self and other interpersonal difficulties. Victims of IPV who experience psychological damage may be depressed and may have developed low self-esteem. Based on our findings, it is explainable that they may be experiencing these feelings much more because, rather than leaving the abusive relationship, they continue to empathise and give reasons why the violent partner acts the way he does. Persons high in empathy and who experience IPV may be predisposed to respond emotionally to the anger, distress and violence of their partners and rather than leave the abusive relationship, may want to stay and help thereby exposing themselves to more psychological damage.
Some closely related research may offer similar perspectives to our current findings. Weiss (1993) and O’Connor, Berry and Weiss (1999) suggested the link between empathy, submission (in other words subservience, tolerance, etc) and depression (an element of psychological damage). In dyadic relationships such as marriage, O’Connor, Berry, Weiss and Gilbert (2002) pointed out the complex relationships that exist between empathy, submission, guilt and depression. Put side by side with our findings, it is logical to think that victims of IPV who are high in empathy may, even in the midst of abuse and violence, submit to an abusive partner, then possibly feel guilty about the abuse and eventually experience depression and other aspects of psychological damage.
The paths from IPV to love dependency was again mediated by CE and AE suggesting that for love dependency also, empathy is a pathway through which IPV is translated and intensified. Victims of IPV who are higher in empathy may become more love dependent on their abusive partners than those who are not. Although there is a paucity of research to support this finding, related studies on attachment have shown a link between empathic cognitions (and acts) and dyadic relationships. For instance, Lafontaine and Lussier (2005), Taft et al. (2006) and Péloquin, Lafontaine and Brassard (2011) revealed that the mediation by empathy on the association of violence and romantic attachment was significant in female participants but not may hold only male participants.
Implications of the findings
The significant mediating effects of the dimensions of empathy on the association of IPV and dimensions of TB mean that the subjective affective experiences of victims of IPV may play relevant roles in the decisions to either leave or stay in an abusive relationship. Empathy through guilt may more easily permit forgiveness, through a reparative gesture, assuring the maintenance of the link with the partner and restoring an active position in the relationship by taking responsibility for the perpetrator’s behaviour. And as opined by Margherita et al. (2014) this could explain why self-blaming and silence are such a widespread phenomena in IPV. Many studies have shown how IPV is more difficult to be recognized from the victims’ perspective (Hirigoyen, 2005; Reale, 2014; ) and this may be due to the levels of empathy in the victims as found in our study.
The finding that empathy also mediated the path from IPV to love dependency has implications for couple therapy. Particularly, Emotion-Focused Couple Therapy (EFT; Greenberg & Johnson, 1988; Johnson, 2004) which aims to restructure the attachment system by exploring partners’ empathic understanding of one another’s emotional experiences and attachment needs may be useful in handling love dependency in the context of IPV. It may be that as partners learn to properly understand and engage the right levels of empathy (when to be empathic and when not to), they may find a level ground where the influence of IPV on love dependence will be nuanced. And as this happens, other ways of putting IPV in check (Johnson & Sims, 2000) may be introduced in order to develop a sense of safety and secure attachment bond (Péloquin et al., 2011) in the relationship. It is worthy to note however that EFT requires partners to explore unspoken attachment needs and emotions, which puts them in a state of great vulnerability and could further endanger their safety in the context of severe IPV. In such circumstances, Péloquin et al. (2011) have recommended that partners work on attachment issues and anger control management on an individual basis before undergoing couples’ therapy with their partner.
As was observed, the mediation by both dimensions of empathy was stronger for psychological damage than for love dependency and core Stockholm syndrome. This may mean on the one hand that the most prevalent form of TB in our population is psychological damage. On the other hand, this also suggests that emphasis need to be placed on the psychological damage caused by TB. As our participants were all women, we have borrowed from the findings of previous studies (Lafontaine & Lussier, 2005; Taft et al., 2006; Péloquin et al., 2011) that the mediation by empathy on the association of violence and romantic attachment may hold only for females but not men to state that TB is still more common in women than men. This has implication for intervention targets and approaches. Government and other stakeholders should, in times of scarce resources and manpower, focus more attention on women as they form the larger percentage of persons experiencing TB.
Also, by highlighting empathy as a pathway or mechanism through which IPV influences TB, we provide an extension to theory. Specifically, we state the possibility of empathy being sandwiched between an earlier experience of violence/victimization and an attachment/bond that is born with a perpetrator. In this case, empathy explains how experiencing violence may influence the motivation to stay with the perpetrator of violence.
Limitations and suggestions for further research
The present research was correlational in nature and this places some restrictions on inferring causation between variables. Prospective designs would be needed to determine the temporal relationships between these variables.
Also, it is possible that the strength of the association between the study variables may have been inflated due to shared method variance because all variables were assessed using self-report measures. A multi-method approach, which may include both self-reports and behavioural observations may further inform the nature of the relationship between empathy and both IPV and TB. The study also focused only on women, however, as evidence for victimization among men is also rising, it will be important for future studies to investigate these phenomena among men.
The study could have benefitted more from a plethora of demographic information regarding participants. Future studies should obtain more robust data regarding participants’ demographics as this could serve as control variables. Also, because our participants were those who had already reported at sexual assault referral centers, generalizations may not be made to persons experiencing IPV who have not reported. It is important that future studies explore these concepts among a more general population of persons who experience IPV.
Finally, because we did not obtain data regarding previous trauma experiences, we could only explain based on previous findings (Hartman & Morse, 2020) that the relationship between current IPV and empathy may be as a result of previous trauma experiences. This however is a speculation and we urge future research to incorporate data on childhood trauma or adverse childhood experiences in order to uncover exactly how earlier exposure to trauma may establish the link between current victimization and empathy.
Conclusions
Empathy mediated the relationship between IPV and TB suggesting that empathy is a pathway through which IPV is translated into TB and that the influence of IPV on TB may be intensified through empathy. The dimensions of empathy (i.e., CE and AE) all strengthened the impact of IPV on TB. Specifically, CE appeared to be more responsible for higher levels of TB in victims of IPV than AE. Empathy may engender tendencies that increase the likelihood for traumatic bonding. Our findings highlight the dynamics of empathy in building and sustaining traumatic bonding in victims of IPV and how these may be explored to liberate persons who are experiencing TB in IPV situations. Further, the findings offer preliminary findings for a framework that may serve to expand existing theories of attachment specifically in the context of abuse and trauma.
Footnotes
Authors Note
The data from this research formed part of the PhD work for
Open research statement
As part of IARR’s encouragement of open research practices, the author(s) have provided the following information: This research was not pre-registered. The data used in the research are available. The data can be obtained at: ![]() . The materials used in the research are available. The materials can be obtained at: https://www.icpsr.umich.edu/web/ICPSR/series/203.
. The materials used in the research are available. The materials can be obtained at: https://www.icpsr.umich.edu/web/ICPSR/series/203.