
Abstract
The present study investigated how caregivers in Finland and the US recount learning and teaching care within the family, drawing on a new educational-psychological framework for care. This study applied thematic analysis to seven focus groups in the US and five focus groups in Finland composed of caregivers (N = 45). The results suggest one main theme for learning, Imperfect Mirroring of Past Parenting and Present Parenting Practice, and two themes for teaching: Actions Tell More Than Words (US) and Teaching Them To be Independent and Caring Citizens (Finland). For learning, the findings indicate that childhood experiences are transformed into an informal guide for how care should (or should not) be practiced, highlighting how the lack of systematization in learning care contributes to caregivers’ need for self-teaching and unlearning what they experienced. In addition, caregivers tend to reproduce their learning experiences in teaching to care, and within this process, they focus more on pragmatic aspects of care. The various elements theorized in the Psychological Processes for Care Framework used, including identifying and anticipating others’ needs and deciding on the responsibility of addressing needs, were neglected in caregivers’ reports of teaching care. Implications argue in favor of psycho-educational programs for caregivers that can systematically address two pressing issues in learning-teaching care - the complexity involved in care processes and understanding the intersubjective nature of the construction of caring relationships.
Care within the family is a foundational pillar of a caring and humanitarian society (Noddings, 2002). It is a relational practice that creates an environment for children and parents to feel safe (Tronto, 2015), and it is deeply connected to most of the United Nations’ goals for worldwide sustainable development (e.g., Ki-moon, 2015). As a practice, care entails “the relationships and activities involved in maintaining people daily and intergenerationally” (Glenn, 2010, p. 5), and it is essential for the maintenance of any society as it fosters human development and the creation of all social relationships. Understanding how care comes to be practiced has significant and widespread implications for various societal spheres, such as determining public health services (Eriksson, 2002), social foster and elderly care services (Keating et al., 2021), family care policies (Tronto, 2013), and educational practices (Bozalek et al., 2020). Therefore, across the lifespan in various societal institutions, there is a question of and need for care.
Much of the scholarship on unpaid family care has focused on the outcomes of how care is practiced by adult caregivers, including how it is often gendered (Glenn, 2010; Perry-Jenkins & Gerstel, 2020), how caregivers feel about their experiences of caregiving, including concerns with burn out (Mikolajczak & Roskam, 2020) or feeling unprepared (e.g., Raudasoja et al., 2022), and the effectiveness of interventions in improving how care is practiced (e.g., Wyatt Kaminski et al., 2008). However, the focus on how care is practiced has resulted in most research on the phenomenon of care assuming the caregiver is already in the social role of caregiving (e.g., mothers (Raudasoja et al., 2022), fathers (Kopystynska et al., 2023), and grandparents (McLaughlin et al., 2017). For instance, many educational interventions often focus on supporting parents in their caregiver roles (e.g., Myntti et al., 2018; Sone et al., 2023; Wrede et al., 2008; Wyatt Kaminski et al., 2008). Consequently, less is known empirically about how individuals become practicing family caregivers (e.g., before one-time external researcher parental interventions), particularly how learning and teaching about and to care happens throughout their life (Noddings, 2002). Given that caregivers have previously reported feeling underprepared for their role (e.g., Raudasoja et al., 2022) and that care plays a central role in supporting the well-being of children and families (Scherer et al., 2019; Zimmer-Gembeck et al., 2022), there is a need to investigate how care is learned and taught, not only formally (e.g., through interventions) but also informally (e.g., by family members). Thus, in the present study, we investigate how care within the family functions as an educational outcome (i.e., something to be taught and learned).
The present study investigated caregivers’ experiences in learning and teaching care, aiming at understanding the core elements circumscribing such experiences and whether and how those elements become content to be learned and skills to be practiced. Furthermore, this study undertook a cross-cultural approach, juxtaposing experiences of two significantly different societies regarding care systems and practices, the USA and Finland. The study provides the first steps to elaborating on an approach for systematically analyzing teaching and learning care across different social contexts.
A care framework: From a form of labor and emotional engagement to a psychological and educational effort
Feminist theorists have widely described care as a form of labor that requires physical actions and emotional engagement (Tronto, 2013). Care involves three types of activities: direct caring (physical care, emotional care, and services to meet needs), maintaining the physical space in which individuals live, and fostering relationships and social connections (Glenn, 2010). Theorists have also noted that engaging in the act of practicing care requires several steps, including (1) caring about (noticing need); (2) caring for (responsibility for and determining how to respond to their need); (3) caregiving (competently acting out the caring behavior); and (4) care-receiving (responsiveness to and assessing the effectiveness of the caregiving) (Tronto, 2013). Scholars highlighted a distinction between caring about and caring for something or someone. Caring about entails being aware of and demonstrating concern toward something or someone; it does not involve effective physical activity attending to specific needs. In contrast, caring for someone requires engaging in certain actions, including physical and psychological processes (Noddings, 2003).
Employing a new theoretical framework that builds on this literature, the Psychological Processes for Care Framework (Midgette & Ferreira, In press), we define care as “sustained and committed attention to, responsiveness, and engagement in addressing the needs of another (within the family)” (Midgette & Ferreira, In press). This framework incorporates the pillar idea from Tronto’s (2013) theorization, entailing any physical and psychological actions necessary to nurture our bodies and caring relationships with others in the world, and notes both the cognitive, behavioral and even motivational prerequisites to engaging in the practice of care. However, unlike prior frameworks, this definition broadens the phenomenon’s scope to include all care receivers’ needs (whether ill or dependent, e.g., (Hermanns & Mastel-Smith, 2012) within the family. The focus is on identifying family members’ needs across different social situations and ages and describing the psychological process employed in practicing care, which fundamentally depends on the relationship between family members. Consequently, our definition incorporates the idea that care depends on individuals’ developing psychological capacities, such as those involved in social cognition, grounded in action, and guided toward maintaining human life.
This framework allows us to consider care as having distinct learning outcomes by breaking down psychological processes involved in enacting care (e.g., “need conceptualization; skills of enacting care step; See Figure 1). Considering the need to test this framework empirically and to investigate how caring can be enacted, taught, and learned, and thus can direct educational initiatives supporting care practices within the family, in the present study, we test out this framework to investigate caregivers’ actual experiences of learning and teaching care within the family. Psychological Processes for Care Framework (Midgette & Ferreira, In press). Note: The figure is extracted from authors, under review.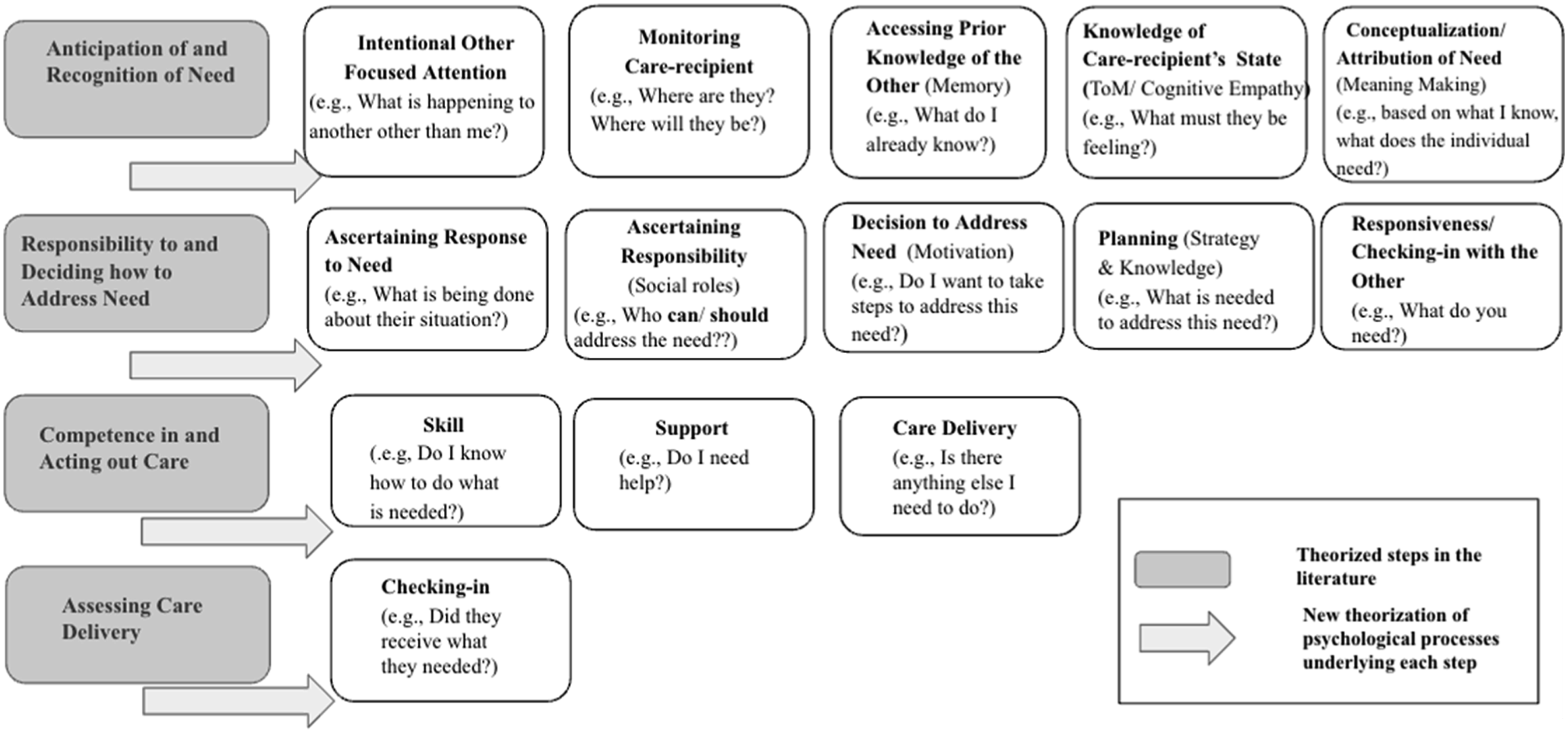
Teaching and learning to care within and for the family
Theories on teaching care have primarily targeted adults out of the family context, including those focused on formal educational contexts such as higher education (Hamington, 2020) and vocational or professional development of caregiver professionals (MecKelvey, 2018; Swanson, 1991). In both cases, scholars incorporate care ethics principles and different care steps into their teaching practices. Hamington (2020) emphasizes the world’s relational and agential character, proposing that care is entangled with the environment and bodies. Thus, teachers should consider that “how we teach is what we teach and how we learn is what we learn” (p. 45). Focusing on the education and training of professional nurses, Swanson (1991) proposed a middle-range theory of care to guide nursing professionals in their work with patients and families. Along the road, this theory has been re-purposed for educational contexts targeting nursing professional training, and the steps initially described by Swanson (1991) are used to guide teachers’ practices (MecKelvey, 2018).
Within the context of the family, although many external formal interventions have been developed to support parents in their function as caregivers as adults (e.g., Myntti et al., 2018; Sone et al., 2023; Wrede et al., 2008; Wyatt Kaminski et al., 2008), less is known about how parents learned to care before such interventions. Prior research suggests that caregivers may not have been taught how to care within the family effectively. In fact, the research suggests that caregiving within the family is often difficult and that many caregivers report feeling unprepared. For example, research has shown that when adults come to officially perform the role of caregivers within the family, such as in parenting situations, they often feel unprepared for the task. Raudasoja et al. (2022) found that Finnish mothers reported challenges with being prepared for parenthood, an issue that participants justified as being connected to not having “role models for being with children” (p. 760). The lack of knowledge and experience in caring for an infant was also true among teenage mothers across different cultures (Erfina et al., 2019) and negatively influenced Hong mothers’ sense of competency (Ngai et al., 2011). Thus, how people become caregivers, focusing on the developing process of this social role, is understudied. Consequently, there is a pressing need for empirical work addressing care as something that must be taught and learned.
Learning to practice care
Theoretically, the family can be one of the first contexts where individuals learn to provide care (Noddings, 2002). From a perspective of skill sets involved in enacting care, Rogoff et al. (1993; 2001; see also Correa-Chavéz et al., 2015) have found that children learn through collaborative engagement in daily tasks. This learning process occurs mainly through observing caregivers and contributing to socially based tasks in a household; an explanation synthesized in the idea of learning by observing and pitching in (LOPI). However, besides LOPI, which focuses on collaborative learning practices within the family, the field of care studies lacks a systematic framework for how care, involving the skill sets needed to complete care labor tasks within the family and other psychological prerequisites, is learned. Two main theories could potentially explain how children learn care behaviors and orientations: social learning theory (Bandura, 1973) and the moral development of a caring orientation (Gilligan, 1982; Skoe, 1993). The first proposes that behavioral tendencies are learned by imitation, repetition, and practice under naturally occurring conditions. Thus, children could incorporate caring behaviors by being directly exposed to them, especially by family members, as they are theorized to be significant role models. The latter theoretical framework proposes that a caring orientation occurs gradually through a sequence of specific behaviors that support reflective processes, starting with self-concern and moving from exclusive other-oriented concern to a balanced concern for both self and others. Pivotal for developing care is a growing understanding of responsibilities in the context of more differentiated dynamics between self and others. However, these approaches have less consideration for which experiences are fundamental to the learner in guiding their learning and when they occur, particularly in the care context.
These theories may be in part helpful in understanding how care is learned, as according to our definition, care involves contributing to the household as a task and a skillset to be learned (Rogoff et al., 1993; 2001; 2015), engaging in behaviors one has seen others engage in (Bandura, 1973), and other-oriented concern (Gilligan, 1982; Skoe, 1993). However, more than these frameworks are needed to explain how we learn that completing a household task is also an act of care. For example, care also involves understanding that the task aims to meet another’s needs. Thus, there is a need to investigate the process of learning to care holistically across the caring steps (Figure 1), from caring about (an orientation to the other) to caring for (skill sets with specific caring goals). Only through such an approach can we investigate whether a behavior is imitative or done with caring intentions. Thus, when considering care as a learning process, it is important to investigate how learners understand and interpret which situations helped them to learn to care.
Present study
The present study is a descriptive-interpretative qualitative research study with an exploratory design based on focus group interviews. In taking such an approach, the exploratory research questions guide the study to define domains of investigation and carefully understand and represent the experiences or observations under investigation (Elliott & Timulak, 2021). In this case, the study investigates care within the family as an educational endeavor. We aimed to test the Psychological Processes for Care Framework (Midgette & Ferreia, under review) empirically in two cultural contexts: Finland and USA. In the U.S., there is no systematic or universally applied formal educational or counseling program to support individuals in learning how to be parents and/or to provide care within the family. In contrast, in Finland, parents count on universal family health and social support services, including Neuvola (Ministery of Social Affairs and Health, 2010). Neuvola offers services through an educational health approach focusing on parenting guidance and developmental follow-ups during pregnancy and across the child’s first five years. Additionally, in Finland, all children starting at upper secondary education are required to attend home economic classes, with course content including issues of “housing and living together,” which aims to “allow the pupils to get acquainted with good manners, equal use of resources, and taking responsibility in the family.” (Finnish National Board of Education [EDUFI], 2014, p. 472). Thus, these family caregivers living in these two different countries may have very different experiences of learning and teaching care. However, research on the impacts of informal learning in the US and formal learning opportunities in Finland is scarce. Investigating how parental caregivers in both cultures learn and practice teaching their children how to provide care within the family can give additional insight into what formal and informal educational processes contributed and contribute to individuals learning how to be caregivers within the family. Therefore, the present study aims to provide the first steps to elaborating on an approach for a systematic analysis of teaching and learning about care, unraveling the core elements circumscribing such teaching and learning experiences, and understanding how they become content to be learned and skills to be practiced. To following questions guided this investigation: 1. How do caregivers learn about and care? 2. How do caregivers teach care?
Methods
Participants
Participants were 25 caregivers from the US (seven focus groups, Mage = 38.48, SD = 8.62, range 29–66, Median = 36) recruited primarily in College Station - Texas, and 20 from Finland (five focus groups, Mage = 40.61, SD = 5.66, range 28–45, Median = 33.5) recruited in Pirkanmaa region (Tampere, Nokia, Pirkala and Kangasala). The only inclusion criteria were that caregivers had children or cared for children who belonged to their family between the ages of 0–18. Caregivers noted caring for biological children, as well as taking in and caring for foster children, grandchildren, and great-nieces. Given our research goal to investigate caregivers’ experiences and practices, we recruited participants with the goal of homogeneous sampling. Thus, participant homogeneity was based on the shared status of unpaid family caregivers with a child within the household. Furthermore, to assess cultural differences, shared cultural context was an additional recruitment goal so that the number of focus groups for each country was sufficient for within-country homogeneity to also compare across countries. Most participants from the US were women (84%), married and Christian (88%), and identified as Non-Hispanic White (64%), while the remainder identified as Latinx (24%), Black or African American (8%), and Asian American (4%). US participants reported having an average of 2.28 children (range 1–5), with ages ranging from 4 months to above 18 years (as a second, third, or fourth child). Participants had a range of educational backgrounds, with 32% having a master’s degree, 28% having a bachelor’s degree, 24% having a doctorate, 4% having a vocational degree, 4% having some college education, and 8% having a high school diploma. Yearly income ranged from less than $10,000 to more than $150,000. In Finland, 95.8% of participants were women; 50% were Christians. While all participants had lived in Finland for at least 10 years and were Finnish citizens, 41% identified as Finnish, 33.3% as European, and 25.6% as non-European. Finnish participants reported having, on average, 2.1 children (range 1–3), with ages ranging from 7 months to 16 years. Most participants had master’s degrees (61%), 9% had doctoral degrees, 9% had high-school degrees, 10% had bachelor’s, and 10% had vocational degrees. Three of the participants in Finland were on maternal leave, while the remaining 17 were working full-time, with working hours varying between 37.5 to 40 hours a week. Most respondents (60%) reported a monthly income between €2000 and €4000, 20% earned less than €2000 and 20% above €4000.
Procedures
Data was collected through focus groups. Compared to interviews, focus groups allow for the researcher to take on a peripheral role, as a moderator, rather than leading every element of the conversation (Nyumba et al., 2018). Thus, caregivers could take a more active and engaged role in what and how they shared experiences, not only based on the researcher’s probing but in response to each other’s interests. One of the strengths of this method is that it allows participants to build on and draw on other’s experiences and thus generate responses that can be richer than those obtained from researcher-led one-on-one interviews (Thomas et al., 1995). Thus, in the present study, we employed the use of focus groups to meet our goal of exploring in-depth the collective experiences of caregivers, particularly with a focus on teaching and learning care. The data used in this study belongs to a larger project developed in collaboration between the authors and was collected from October 2021 to February 2022. The study received IRB approval from each author’s university for data collection in each country (U.S. protocol # IRB2021-0900 M, “Thinking about Care Within the Family”; Finnish protocol # Statement 59/2022, “From care receiving to caregiving: a developmental and cross-cultural investigation into the conceptualization of care within the family”). Given our goal to investigate caregivers’ experiences, participants were recruited through purposeful sampling. US participants were recruited through listservs and social media (e.g., Facebook) and received $30 for participation. Finnish participants were recruited via email listing accessible via daycare centers belonging to the first author’s network and received a movie ticket as compensation for their participation.
Given the cross-cultural goal of the study, the focus group protocol was designed by a team that included a member living in each country and familiar with the culture of each cultural context studied (as recommended by Cuoco et al., 2022). The protocol was translated from English to Finnish by a native Finnish speaker with a background in cross-cultural qualitative research and then back-translated. The protocol was also piloted to ensure the operationality of the interview script, respecting the semi-structured nature of the focus groups. Focus groups were conducted virtually through Zoom in the US and in person in Finland, with a minimum of 3 participants per group (M = 3.5), and lasted an average of 1.5 hours. Our number of focus groups per country (5 in Finland and 7 in the US) met the criteria for focus group data saturation found in the literature (e.g., Hennink & Kaiser, 2022). We also recruited with the goal that each group met at least the minimum number of participants recommended by the literature (e.g., Krueger, 1994), with the goal of more as scheduling between participants allowed, ultimately having group sizes that were not so unwieldy so that participants all had the opportunity to share their experiences and ideas in more depth (Mosadeh, 2012). U.S. focus groups were led by the first author, a Brazilian-American faculty member, ciswoman, married, heterosexual, and without children. Finnish focus groups were led by a research assistant, Turkish-Finnish, ciswoman, married, heterosexual, and with two children, who were trained to conduct focus group interviews by the second author. Participants were asked to discuss a series of questions (see Appendix A), which explored how caregivers conceptualized, practiced, and reflected upon learning and teaching care. Focus group questions included questions aimed at understanding their experiences of learning (e.g., How do you think you learned to provide care for others? Who taught you? In which ways? Why?) and teaching (e.g., In what ways do you think your child (and or other family members) are encouraged to take care of others?). This study focused on analyzing the experiences of learning and teaching care. The focus group interviews in the USA were conducted in English. In Finland, participants could choose to use Finnish or English according to their comfort levels; language was negotiated within all groups before the beginning of the interviews. All groups chose English. To ensure that the protocol was followed as planned, the focus group moderators in both countries were instructed to be attentive to any signs of participants’ distress, confusion, or doubt about the questions being asked and, if necessary, stop, clarify, or re-ask the question in another manner.
Analysis
Focus groups were recorded and transcribed verbatim. The material in Finnish was translated into English by a native speaker with professional proficiency in English and then back-translated, ensuring that semantic meanings were preserved. Transcripts were analyzed thematically (Boytazis, 1998; Braun & Clarke, 2006, 2021), supported by Dedoose (Version 9.0.62), a qualitative coding software. Due to the exploratory nature of our study, our approach was inductive. The initial step was to employ a codebook thematic approach (Boyatzis, 1998), where initial codes were created for each data set (Finnish and US separately) through familiarization with the text, inductively developed by each culturally informed respective coder (the second author as the US-based researcher coded US data, and the first author as the Finnish based researcher coded Finnish data) based on semiotic meanings (Braun & Clarke, 2006, 2021). Our choice of semiotic meanings as our level of analysis was due to our focus on participants’ explicit interpretations of teaching and learning. In developing our codebook, each code was given a name, definition, and example(s) of an excerpt that contained the code from the text. This approach served as an important foundation for comparing across codebooks in a culturally informed way, as definitions, rather than code names, allowed for discussion of nuances in how ideas were discussed within each data set (as well as whether ideas were present in both datasets). Considering that we were aiming to compare culturally shared and distinct experiences of teaching and learning care, the codebook approach, which included making the definitions of ideas we identified in the data explicit, allowing for a strong and clear basis for cross-cultural understanding across the two researchers drawing from data sets from distinct cultures.
The following step consisted of code developers reviewing codebook decisions to achieve the first finalized codebook (for the final codebook, please contact the first author). Following code application, themes were developed by each coder for each country as they had in-depth familiarity with the data. Rigor was ensured through peer debriefings, where the researchers met frequently and engaged in discussion throughout data familiarization, code development (including a 2-week intensive with daily sessions), code application, theme development, and narrative writing (Janesick, 2015). The authors, who were also the main coders, continuously checked each other’s code definitions and discussed the application, interpretation, and coherence of themes. Themes were created based on code prevalence (across focus groups and overall frequency of application), code co-occurrence, and shared underlying meanings and assumptions. These were reviewed through re-reading excerpts associated with the code(s) concerning our research question. As a final step, reflexivity was ensured through multiple sessions of thematic discussion where the researchers from both countries would explore different aspects of specific topics in the material from micro (local) to macro (cross-cultural) perspectives. In such sessions, socio-cultural particularities were also considered, contextualizing the narratives under analysis. This process ensured a coherent theme development process.
Results
The examination of experiences of learning and teaching care within the family across Finland and the US is explained through three main themes. One theme common to both countries addresses participants’ experiences in learning care: “Imperfect mirroring of past parenting and present parenting practices.” The other two themes, “Actions tell more than words” and “Teaching them for the world,” illustrate experiences of teaching care in the US and Finland, respectively. This study explored cultural similarities and differences to understand how specificities of the learning context can influence learning. In the following lines, results are presented in detail according to all three themes. The similarities and distinctions are described within each theme, followed by a theme-centered discussion.
Learning: Imperfect mirroring of past parenting with present parenting practice
This theme brings out the shared patterns of meanings explaining how childhood experiences are noted as the foundation of learning for present caregivers caring behaviors and, in many situations, guide decision-making processes in parenting. However, although the theme is shared between the countries, what is incorporated from the past and how it affects current care practices differs significantly (see supplementary files).
Observing what (not) to do
For all participants across cultures, learning about care involved reflecting on their experiences while growing up. Thus, learning about care for caregivers started by observing how care was provided to them in childhood. Most of the participants’ learning was through observation processes, rather than direct instruction (although some did have parents, particularly mothers, who taught them practical skills, such as how to cook). Family figures such as mothers, grandparents, and extended family were noted as role models for what to do and not to do once they became caregivers themselves. For example, “I see a lot of my mom and how my mom took care of me, in me; in how I’m taking care of my family (…) she did everything for me and my brother and now I feel like I have to do everything, plus taking care of her. It is very interesting!” (Finland, mother, 38 years old) “I think for most of us, the starting point is what our parents did or didn’t do and, we make a choice to do the things that we thought they were good at and to do something different on the things they didn’t.” (USA, grand-aunt and mother, 66 years old)
However, the evaluation of their experiences differed across cultures. While participants in Finland stressed finding the positive aspect of the experiences as the focal point of the learning process, those in the US primarily noted their behavior as being guided by what not to do. Thus, for US participants, although a few did report observing positive parental models and thus aiming to emulate positive experiences growing up, as shown below, the majority focused on avoiding negative examples. “Yeah, you model, you model those that you know that have treated you nicely. You know, kind of- you know even as a teacher, you know, I model my teaching style after the teachers that I had that were great. You know, and then the family members that I had that were really loving and caring, my grandmother and my aunt. You know like I said my mother ehh, you know she was pill, so I kinda know okay let me not do that.” (USA, mother, 36 years old)
As evidenced also by those who had positive role models, a central guiding element for US caregivers was Avoiding parental mistakes. Most participants’ learning came from experiencing and observing negative, inadequate, or problematic caregiving that they received from their caregivers. Thus, participants noted that they learned what not to do through examples of caregiving mistakes they wanted to avoid. Often, their experiences growing up served as a negative learning experience, where caregivers wanted to do the opposite of what their caregivers did with them: “You know my parents weren’t very patient, my dad wasn’t, my mom wasn’t patient at all. …So I’ve tried to be come from that level of concern and you know just try to be more positive about it. Instead of kind of come- bring, do things the way I was accustomed to growing up. I wanted to flip the script so that’s how I- what I’m proud of with my kids.” (USA, mother, 36 years old) “And that’s, that’s my approach also, it’s that I guess since we didn’t get it growing up, now we’re giving it and these kids are like “wait, what’s this?” But they, they’ve been accustomed, and I want, like I said I want, I want to be there for my kids and my grandkids. Because I didn’t get that.” (USA, mother and caregiver to spouse with cancer, 59 years old)
Parental figure mistakes, as understood by the participant, did not only serve as a signal of what to avoid it also provided guidance and motivation for how they could become better caregivers: “...obviously my husband and I are very aware of things that we feel that we were not fully met as kids… Just to- we obviously want a better environment for him than what either of us grew up in.” (USA, mother, 33 years old) “… I think I also learned how to be protective from the lack of getting that as a child for my mother, like there are times and ways I wish she would’ve protected me and my siblings better, um but she was just stretched way too thin and so wasn’t able to do that, and so through that lack of example I think I learned the need for a parent to be a protector.” (USA, foster and biological mother, 45 years old)
In addition, US caregivers stressed the need for Unlearning Lessons. Participants noted that the impact of negative caregiving examples and experiences not only served as motivations for doing better and guiding their behavior in ways not to be, but they also had a negative impact, in that participants found themselves having to “unlearn” problematic behaviors that they had observed and/or been a recipient of while growing up. In other words, participants noted that they ended up learning ways of caregiving that they disagreed with and needed to unlearn: “But there are definitely bad things from both that I have to unlearn, and I am still realizing things even now, why do I have to compulsively clean when my husband comes home, oh it’s because my dad said, whenever he gets home “go clean the house, go clean the house. So yeah, it comes from a lot of different ways, a lot of different people.” (USA, mother, 33 years old) “I know that’s what I learned what not to do and ummm and unfortunate, maybe I learned certain behaviors that probably that just don’t benefit me or benefit my own children that I’m still unlearning.” (USA, mother, 37 years old)
For participants in Finland, focusing on the positive was the central idea. Although they reported experiencing bad and unpleasant situations in their childhood, including traumatic upbringing circumstances, e.g., alcoholism and neglect, learning care was associated with using the positive aspects of these experiences in their favor, thus focusing on what should be done or how parenting can be improved. For example, participants noted: “I think my dad’s second wife wanted to erase me from their lives, (…) She was really not treating me well when I was little, and I think that she made a massive difference between kids. I think that got me more sensitive. I use that in my adulthood now, also at work. I know who is feeling bad, I know somehow it is really weird! I think I got some emotional intelligence from that! It is really hard to explain.” (Finland, father, 38 years old) “I was 5, dad was an alcoholic, so mum got full custody. She has been taking care of me and my sister with the help of her own parents who are still alive and very close to me. She had problems, but she made sure that I have a scarf on or gloves you know… she was caring, and I focus on that.” (Finland, mother, 34 years old)
Participants conveyed being aware of lacking certain elements in care practices and reported understanding that their parents did what they could, e.g., “it was a loving home, but love was not shown. There weren’t many hugs and kisses, but they did love us” (Finland, mother 42 years old). These memories also included observations of other parents than their own. Some participants reported being influenced by friends’ families and observing uncles and aunts as parents. Thus, the role models from childhood experiences were built by focusing on positive experiences and memories.
Self-comparison with other parents
Finnish participants also noted that observing other parents was part of their learning process and that with it came self-judgment. Although they recognized that every family is different and requires a distinct set of care behaviors, e.g., “most of the people who love their kids and their families, do the best they can, and it is different things and different times and different families.” (Finland, mother 45 years old), the comparison impacted how they saw themselves. This comparative lens increased their self-awareness, e.g., “he is a little bit more authoritarian type of educator than I am. I am more ‘let us talk it out, let them make their mistakes and learn from them’ type of parent” (Finland, mother 34 years old), but also boosted critical self-judgment, e.g., “I feel I am providing a little bad care myself at home when I am not able to do that!” (Finland, mother 34 years old).
I am learning on the job versus parenting in the best teacher
Participants in Finland and the US often reported learning care while currently parenting (“on the job”). In the case of US parents, learning while parenting often resulted from having limited knowledge of how to care when they first became parents. For all focus groups, this process of learning included self-teaching. It often occurred through seeking knowledge from “knowledgeable” others, including learning from one’s spouse, parenting support groups, general oral tradition, and doing one’s own research, e.g., reading books, social media, or listening to podcasts. Many participants agreed that they had not directly been taught before they became caregivers: “Yes, it is a necessity. No one might have ever taught you and you are suddenly doing it. I am also in this Facebook group for moms who work in higher education, and I learn a lot of stuff on there, from these other moms in the Facebook group who put out tips and things. I have also, through that been connected to big little feelings, it’s like Instagram/Facebook page, and recently doctors Becky good on the inside.” (USA, mother, 36 years old) “… The first time I changed a diaper, was the nurse showing me how to change a diaper in the hospital with my first son, I had never changed one before, so watching how others did it and picking up their way of how to swaddle, and these basic skills to keep a child alive is where I learned from others, mostly my wife, and watching her do it, and picking things up.” (USA, father, 42 years old)
Self-teaching versus finding my way with guidance
However, while participants in the US mainly relied solely on themselves to look for information, Finnish caregivers leaned on the support of health services and professional counseling offered in public care, e.g., Neuvola. For example, participants in Finland noted: “I think we learn mostly by example, but then we see that from Neuvola you get information from many places and you read books, sign up on a course. I feel I was lucky!” (Finland, mother 34 years old). “I am currently in a parenting course to learn more skills, I am doing an online course! I think one of the abilities you need is the ability to listen, and you need emotional intelligence and the ability to analyze and to act without judging, but you need to have fairness and the skill to run a family; like to be the main person behind it, to carry all the main needs to organize and to coordinate and to think about timing and planning.” (Finland, mother 34 years old)
Unprepared for caring
While Finnish participants had initial social support for preparing for practicing caregiving, participants in the US noted not feeling prepared for caring for the family. There was general agreement across US focus groups that parents, in general, didn’t have all the knowledge required to be caregivers before they became parents. In fact, a participant noted that “not everybody knows how to raise a child” and suggested the need for parenting classes: “You know I do- this is probably not part of this answer or question but, I do feel like every parent if you’re pregnant, at least, for the first time, the parent should go through a parenting class. Like a child development class just to teach the basic needs and processes and whatever for a child and how to be with a child for the first time ever in their lives. I don’t feel like that happens enough and it’s just a choice it’s not required, and I really do think that should be a requirement because not everybody knows how to raise a child or they weren’t raised in the best household to be able to have had that example of raising children.” (USA, mother, 32 years old)
Surprising parenting lessons
Differently, for participants in Finland, parents reported being surprised by what parenting taught them. Participants noted learning to trust their partners more, and to be patient and tolerant to themselves and others. For example, one participant noted herself having tantrums and reflected on the experience: “Sometimes I catch myself having tantrums over somebody not making their bed or something, and then I tell myself that I should remember what is most important! but it is not always that easy” (Finland, mother, 45 years old). Another caregiver noted how having the second child made her more patient, affecting her parenting: “An important skill is definitely patience, at any age. Patience! So, with the first one, I noticed I have been very impatient in a way that he starts mastering his ability and he grows up or he needs to learn how to do something with perfection by a certain age, and so on... I notice that with the second one, I am much more patient and I just let her do things when she is ready to do them. And I think they learn better with patience”. (Finland, mother 33 years old)
In summary, learning care for both groups was informal and fundamentally grounded in caregivers’ experiences. However, groups differed on their sources of information about how to caregive. While role models for US participants were predominantly close family members and experiences served as examples of what to avoid or improve, Finnish groups also incorporated other parents in ways of learning about care and emphasized how their experiences impacted who they are, often focusing on the positive. In addition, while US participants noted being underprepared and having to teach themselves, Finnish participants reported being surprised by what parenting can teach them.
Teaching: Actions tell more than words versus teaching them to be independent & caring citizens
This study also investigated ideas of how participants taught care. Teaching experiences included two distinct main themes: For participants in the US, the theme “Action tells more than words” reveals the general idea that teaching care happens when parents provide examples of care, primarily through how they care for their own family members. When children see parents acting they learn what to do. Concomitantly, care is learned when parents provide the opportunity for children to practice acts of care, particularly those relating to care labor e.g., house chores. Practicing via play, helping with household chores, or taking care of pets are the most common explanations for the process. For the Finnish participants, teaching care is best captured through the theme “Teaching them to be independent & caring citizens”, which asserts participants’ complex reasoning regarding teaching care as preparing children to care for themselves and others, living in society as an autonomous and caring person. Similarly to the US, Finnish participants informed their varied teaching methods, e.g., by example, play, and negotiating with children. However, this theme also brings together patterns of meanings related to participants reflecting on the objectives of teaching care, bridging the teaching process and the content being taught, which was also prevalent in the Finnish data (see supplementary files).
Teaching through examples
Although caregivers in Finland and the US reported fewer similarities in teaching care, one exception was regarding the methods used to facilitate children’s learning. Participants in both countries noted that examples are the main method through which children learn. They learn by observing and reflecting on the situations. For example, when caregivers are caring for someone that is sick, e.g., “they witness that we are providing care for our parents as in the case of Tina, and they naturally understand care too” (Finland, mother 42 years old), or when engaging in different contexts in society, e.g., “I think, it is important for kids to see how we react and how we socialize also with all different kinds of people, from different backgrounds, and different ages, and different cultures, and different whatever!” (Finland, mother 33 years old). Participants often noted that children liked to imitate others, particularly when engaging in chores and childcare: “I think that the child, the children, they learn how to take care of others given their situations and whatever they are exposed to… my daughter that is now, 5 but when she was in daycare, she was in the baby room, I remember and she would come home, and she still has babies, till this day, little toy baby dolls that she plays with, she lays them all on the ground, she picks them up, she talks to them she is so sweet and kind, and she is like this, and she is just so gentle, and I’m like, where, how, what…]” (USA, mother, 33 years old) “ So I think in a lot of ways he just copies a lot of what we do, he sees us cook, he wants to cook, he sees us clean, he wants to clean, he sees us take out the trash, he wants to take out the trash, that kind of thing. I don’t know if that will last, but we’ll take it while we can.” (USA, mother, 36 years old)
Teaching through play versus toys as instruments of practice
Another common ground between Finnish and US focus groups was the use of play. The use of play was mentioned in the discussion of most focus groups in both countries to teach children about care. However, participants in Finland noted using play activities to teach children to take care of their toys, e.g., “I’ve been teaching them that they need to take care of their dolls as well because they play with dolls that they can’t just throw them around and be violent to them” (Finland, father, 37 years old) and for teaching specific behaviors parents identified children had difficulties with. For example: “We also teach her how to share or how to be fair. We were playing picnic with toys and her father came, then we tried to teach her that she could give one of the cups to her dad because when she plays she wanted all the cups for herself” (Finland, mother, 35 years old).
While for participants in the US, the play was reported to be used to provide children with the opportunity to practice household chores, facilitating the exercise of engaging in household activities that will be involved in care labor in the future. Several participants noted how toys, such as dolls and toy versions of tools family members can use to complete chores (e.g., toy stove), assisted children in practicing care: “I am thinking about our older son, you know, he has a little baby doll that comes with a little diaper and especially since seeing his brother, he likes changing the baby’s poopy diapers all the time. He takes it off and puts it back on. But he’ll say oh we have to change my baby’s diaper, mommy, and then we have a little baby doll that he keeps in the bathtub that we call the bath baby, which he is recently baby henry.” (USA, mother, 36 years old) “... she still has babies, till this day, little toy baby dolls that she plays with, she lays them all on the ground, she picks them up, she talks to them she is so sweet and kind, and she is like this, and she is just so gentle.” (USA, mother, 33 years old)
Pet care
The same idea is reported by US American caregivers as being applied to taking care of pets. A few participants noted using pets to encourage children to practice care, including need recognition and practice noticing needs by communicating with them and asking them questions. For instance: “So, for us, we have two dogs, and that’s been something that I’ve really used to teach her how to care for others, and I know it’s a dog instead of a person, but, um, and so, as we talk about, first we talk about other people’s needs, like oh the dogs are hungry… and then when she got big enough, she carried the smaller dog bowl, which is as big as she is though, and so getting her to actively do that, giving her an active role in something that she can do.” (USA, mother, 30 years old) “And like with our cat, she used to pull the cat’s tail, and the cat would be really nice about it but would just obviously meow and get all upset, and I would say, “See how the cat is upset now? We don’t want to pull her tail cause it hurts” and just trying to explain to her.” (USA, mother, 29 years old)
However, while the discussion of teaching care in US American focus groups provided many details on how care is taught, participants in Finland reported the overall aim of teaching children to care. It is possible to notice in the Finnish focus groups an emphasis on what they taught parallel to how they did it.
Teaching them to be independent & caring citizens
It was common for participants in Finland to report teaching care with the goal that their children Be as independent as they can be and that they would be Considerate toward others. Being independent meant, on the one hand, teaching care as encouraging children to do things by themselves, e.g., clothing, bathing, preparing food, and clearing after themselves; actions that can be related to the labor of care within a household. On the other hand, it also meant teaching children to face challenges in life, including dealing with disappointments and thinking about money and how to invest it for the future. For example, participants described children being excited to learn to deal with their money: “What we have started to also play with the oldest is weekly money. (…) We promise him ten euros per week if he always does his homework, he goes to his in-time hobbies, and he helps a little bit with the housework and so on… so he is very excited about that! We try to teach him investing, by the way, which is also something, in a way, would qualify as a need, not as a basic need but maybe an educational need, I would call it.” (Finland, mother, 33 years old)
Parallel to teaching children to be independent, caregivers reported supporting children’s learning to notice and care for others outside the family. Caregivers across all focus groups in Finland reported teaching children how to socialize with others respectfully, e.g., “to socialize with others, give examples and also encourages them to verbalize their feelings” (Finland, mother, 28 years old), or “we encouraged both kids to think about how their actions make other people feel. Whenever one of them is crying, as a result of the conflict, as part of resolving, you look at the other person and think how they feel about the action” (Finland, mother, 34 years old). These two complementary dimensions (independence and consideration for others) composing the objectives of care for participants in Finland suggest a direct relationship between caring within the family and living in society. Thus, suggests that teaching care will support children to become autonomous and supporting adults.
Overall, two aspects of teaching care are particularly relevant. First, it is still being determined whether there is a direct relationship between what a caregiver learns about care from books and guidance and how they teach care. Teaching by example, i.e., by doing, is how participants reported learning care themselves, which indicates a repetition of learning-teaching strategies. Second, although in both groups teaching care addresses only one step of the psycho-educational process of care framework, Finnish caregivers seem to approach care more globally than US groups.
Discussion
Leveraging in-depth focus group interviews with 45 caregivers, this study examined how parents approached learning and teaching care within the family in the USA and Finland. Testing out the Psychological Processes for Care Framework (Midgette & Ferreira, In press), we found that learning care was often informal, grounded on participants’ perceptions of childhood experiences of being (or not) cared for, and contingent on their present experiences of being a caregiver - “learning on the job,” which suggests the need for an educational and psychological theory of learning care and a more systematized intervention to support parents in teaching care within the family cross-culturally. When it comes to teaching, although Finnish and US caregivers approached teaching differently, they both primarily focused on only one or two steps of the caring process. Thus, our study indicates the need for a closer exploration of how learning to engage various steps of the caring process occurs, such as learning how to conceptualize needs and ascertain responsibility in addition to the skills needed to carry out the action of caring, learning how to live interdependently in social relationships (Tronto, 1995, 2013).
Challenges in relying on informal sources of knowledge
Our study finds that shared processes of learning to care for Finnish and US caregivers: all caregivers reported learning by observing and also by doing while caregivers as adults. Thus, overall, learning was informal and based on experiences. This is in keeping with previous studies on how children come to collaborate and learn to engage in social activities, such as doing chores, by observing adults and participating in joint activities (Correa-Chávez et al., 2015; Rogoff et al., 2001; Silva-Oliveira et al., 2022) and with a series of studies indicating that parenting skills are built gradually during the process of parenting as adults (Hodkinson & Brooks, 2022; Raudasoja et al., 2022). However, there are several challenges, discussed in detail below, in caregivers’ reports of their learning experiences for thinking about the education of caregivers.
First, caregivers relied primarily on experiential, self-teaching, and informal processes of learning, which may hinder their ability to develop a comprehensive understanding of care. In both countries, groups reported self-teaching through books, research, and other professional-produced materials to guide their parenting practices. This is in keeping with prior research finding that caregivers often spend time gathering information and continuously learning about how to provide care, although with this came the challenge of potentially not receiving accurate information (Cuoco et al., 2023). Indeed, in our study it was unclear how the content in such materials was transformed into practice or how the scientific/professional guidance was taken as a reference for care practices. For example, caregivers in Finland did not elaborate on the opportunities for formal teaching during their schooling and through Neuvola services, nor did participants in the US groups about what they learned through private counseling and research. This suggests that, on the surface, caregivers are more likely to rely on their own experiential learning (i.e., through past and present experience; Kolb, 1984) than on the systematic and formal teaching they receive, regardless of the new trends and knowledge (Miller, 2017). Alternatively, what is learned and then operationalized may be a matter of a hierarchical knowledge domain, where experiential learning operates at a deeper level than learning through systematized knowledge. Finally, we find that observation of what happened in the past was something that US adults had to often teach themselves to unlearn, given the power of observation and experiential learning during childhood. However, in both cases, reliance on experiential learning alone in an informal context may make it challenging for learners to identify the elements of their experience that make the situation one of care– i.e., learners may not focus on or be aware of all the elements involved in the process that they experience as care.
Secondly, the informality of the learning process resulted in scattered and multiple sources of learning care. Our results indicate cultural differences in the sources that served as caregivers’ references to learning care. While US groups reported learning by observing their parent’s behaviors primarily, building the nuclear family as the main reference for learning care, Finnish participants included observations of other parents, both in their past experiences (e.g., parents of their friends) and in present time (e.g., other parents within their social network, Raudasoja et al., 2023). In both cases, there are consequences of primarily relying on observations and personal perception to create references of care. On the one hand, the ample source of models reported in the Finnish groups, i.e., family, friend’s parents, and other parents, provides a wider scope of caring examples, which could explain why Finnish groups reported noticing the experience of parenting as a rich learning process, while US participants depicted a sense of unpreparedness and struggle. Likewise, a broader reference frame could be implicated in the more global approach to care adopted by Finnish caregivers, which included independence and a sense of citizenship in their teaching lessons. Nevertheless, informally incorporating a variety of references of care can also be detrimental for parents, particularly young ones. For example, in investigating the causes of parenting burnout among Finnish parents, Sorkkila and Aunola (2020) have called attention to the behavior of comparing parental skills and dangerously undertaking a socially prescribed idea of a perfect parent. Perfectionism related to parenting is one of the main variables correlated to Finnish parent burnout (Raudasoja et al., 2022; Sorkkila & Aunola, 2020). On the other hand, the narrower reports the U.S. shortcoming of primarily relying on their parents as a model for parenting is that they can limit one’s perspectives on how situations can develop (Holden, 2019). It impoverishes learning processes and, in this case, traps parents in either copying a pre-experienced model, often reproducing a behavior without reflection, or creating a caring relationship based predominantly on specific behaviors to be avoided.
Disconnections between learning and teaching care
Whereas caregivers in both countries also report relying on informal processes (e.g., serving as a role model) to teach care, results indicate that what they learned about care (content) is not precisely what they aim to teach care to be to their children. While caregivers in both groups described their learning experiences as connected to how they felt cared for, they don’t explicitly mention the construction of good memories– of making their child feel well cared for–, as a guiding principle in their own teaching care practices. Teaching is primarily pragmatic, involving household chores (US) or actions relevant to independent adult life in society (Finland). In both cases, there is a lack of coherence and systematization between learning and teaching care. While previous studies have consistently shown the relevance of observations and participation in learning care processes (Correa-Chávez et al., 2015; Rogoff et al., 2001), our results open the debate on the need for other approaches, one that supports the integration of experience and systematized knowledge and that is more capable of enlightening the socio-material affordances for caring in relations within the family.
Particularly, we call attention to how care starts before caring acts are in place (Midgette & Ferreira, In press). It entails many psychological processes involving anticipating needs and understanding the context and the role of people in responding to others’ needs, all of which are fundamentally related to how one learns to know the other in a caring relationship. The feelings experienced growing up were central in our participants’ reports, evidencing the fundamental relational component in learning care (Noddings, 2003). Aligned, previous work suggests that care within the family depends highly on intimacy, affection, and bonds of trust within social interaction (Glenn, 2010; Noddings, 2003). However, there is no empirical indication of how we learn to establish these elements and ensure that care happens in a well-functioning relational environment. Our study suggests, from the absence of reference to many of the “higher” cognitive requirements involving the process of care (Midgette & Ferreira, In press), that teaching practices of care, despite the formal educational processes available in Finland, are yet far from including intersubjective skills that can support one to identify possibilities for care actions (affordances for care), which are an essential part of the care process.
In addition, besides the lack of elements related to identifying affordances for care, teaching care, even from a more global perspective as portrayed in the Finnish caregivers’ description, was still mainly guided by attributes caregivers find to be important for a future independent adult (e.g., dealing with their own frustrations, using money - to invest, and take care of themselves) instead of building the bases for interdependence. It shows the immense gap yet to be bridged in educational endeavors aimed at supporting a caring orientation. We call attention to the need for enlarging theoretical perspectives in approaches to learning and teaching care and argue the way to focus on understanding and creating systems to promote skilled human actions, including those dependent on social interactions and engagement (Rietveld et al., 2018).
Implications and final considerations
The need for more intentional and comprehensive approaches to care education
Investigating how parents educate their children and aim to teach them how to practice care has implications for considering how health and psycho-educational programs can support parents in this aim. Based on our results, we argue in favor of psycho-educational programs and health intervention processes that can systematically address two pressing issues in learning-teaching care - the complexity involved in care processes and understanding the intersubjective nature of the construction of caring relationships. Using (Midgette & Ferreira, In press)’s framework to guide the psychological processes in care associated with experiential (phenomenological) perspectives to support the analysis of the interpersonal mechanisms involved in learning could bring a comprehensive psycho-educational approach to care.
On the one hand, (Midgette & Ferreira, In press)’s framework facilitates breaking down the complex steps and psychological processes involved in care, affording more tangible planning for learning-teaching experiences. For example, our results from US participants indicated that many caregivers have concentrated mainly on teaching how to perform specific care-related acts. However, teaching children to undertake household chores (i.e., competence in care as a skill), although important, will not ensure that caring will happen in the future (Fairchild, 2021). Teaching care must include noticing the needs and reflecting on how and whose responsibility is to address them, competencies that are not developed spontaneously through observing caregivers perform acts of care. Thus, teaching to care requires intentionality and an explicit mediation of sense-making of what, how, and why things happen.
To conclude, the current study suggests a lack of educational engagement in teaching all the elements involved in care, particularly those involving establishing and sustaining a caring relationship. We suggest considering employing the (Midgette & Ferreira, In press)’s framework in dialogue with enactive cognition theory and particularly the work around the concept of participatory sense-making (De Jaegher et al., 2017; Di Paolo et al., 2018) and the framework for developing skilled intentionality (Rietveld et al., 2018), since these could provide a comprehensive understanding of the intersubjective processes embedded in caring relationships relevant to learning-teaching care. When both are applied in learning-teaching care, this perspective focuses on how the caring relationship is established, developed, and maintained between caregivers and care receivers. An enactive perspective calls for a process that seeks to understand what is relevant to both individuals within interactions so that all their actions confluence and learning happens. Ultimately, it would mean clarifying the reflective and analytical processes connected to how the interactions between caregivers and care receivers are established, allowing for changes in the “bad parenting behaviors” from one generation to the other. Such a psycho-educational program would contribute immensely to enhancing parents’ repertoire in care, decreasing stress created by uncertainties revolving around care, and preventing generational trauma. Ultimately resulting in better parenting.
Limitations
Although the current study made an important contribution to the field by lending empirical support to the call for making care an educational objective, it had several limitations. First, our study was limited to caregivers who were taking care of children up to the age of 18. Caregivers may teach their children to care by accompanying them through their caregiving process. Thus, future research should investigate the role of those who teach care within their family of older children across, ideally, the lifespan. Moreover, we did not investigate the caregiver’s sexual orientation or disability status. Future research is needed to investigate how various positionalities within a society influence caregivers' experiences of learning and teaching others how to practice care. In addition, the study was limited to caregivers’ recollections and self-report of their experiences teaching and learning. Future research is needed to observe how caregivers engage in teaching care (e.g., similar to Rogoff et al.’s (2001) methodology) with the intent to teach care (thus paired with field interviews), as well as developmental interviews to ask children and caregivers across the lifespan how they are learning to care. It may be possible that memories of how caregivers learned in their childhood may not match what children themselves feel and believe that they are learning. Finally, the current study was limited to two cultures within the West.
Supplemental Material
Supplemental Material - Learning and teaching care within the family: Experiential learning reflecting informal teaching
Supplemental Material for Learning and teaching care within the family: Experiential learning reflecting informal teaching by Juliene Madureira Ferreira, and Allegra J. Midgette in Journal of Social and Personal Relationships.
Footnotes
Acknowledgements
We would like to thank Aynur Koyuncu for helping with data collection for the Finnish focus groups and Marla Sarmiento for helping with data collection for the US focus groups.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Open research statement
As part of IARR’s encouragement of open research practices, the author(s) have provided the following information: This research was not pre-registered. The data used in the research are not available until the completion of the project. The data can be partially obtained by emailing:
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.