
Abstract
Several studies of paternal postpartum depression (PPD) typically use homogenous samples. As a growing population and susceptibility to experiencing postpartum depression, little is known about the risk factors associated with paternal postpartum depression among Latino fathers. The nonrandomized convenience sampling strategy yielded a heterogeneous sample of 101 Latino fathers. Predictors of paternal PPD were coping skills, age, having a partner in PPD treatment, and egalitarian gender attitudes were estimated using a single logistic regression model. A second logistic regression model was performed using STATA’s stepwise estimation to obtain a final model with only significant predictors for paternal PPD symptoms. Results from the logistic regression models indicate that Latino fathers who reported higher maladaptive coping skills had increased odds of being above the clinical cutoff for paternal PPD (OR: 1.99, 95%CI: 1.02–3.90, p < .05). The results of the stepwise logistic regression indicated that increased maladaptive coping skills (OR: 2.14, 95%CI: .11–4.13) as well as having a partner in PPD treatment (OR: 2.66, 95%CI: .84–8.44) increased the odds of scoring above the clinical cutoff for paternal PPD. In addition, being older decreased the odds of scoring above the clinical cutoff for paternal PPD (OR: .87, 95%CI: .77–.99). Findings indicate that when a Latino father is younger, endorses maladaptive coping skills and has a partner in PPD treatment, it is associated with increased odds of paternal PPD. In addition, culturally responsive treatment implications for Latino men are discussed.
Keywords
The Latine 1 community comprises diverse individuals across races, ethnicities, countries of origin, and ancestry. The Latine population reached 62.1 million in 2020 and is one of the fastest-growing ethnoracial groups in the United States (U.S. Census, 2021). It has been documented that Latino fathers (Mexican and Dominican) are actively involved with their partners and babies during the prenatal and postnatal periods (Cabrera et al., 2009; Tamis-LeMonda et al., 2009). Extant research documented that Latino men are susceptible to developing paternal postpartum depression (paternal PPD), comparable to Latina women (Ceballos et al., 2017; Paredes & Parchment, 2021; Roubinov et al., 2014). Worldwide, one out of every ten fathers experience paternal PPD (Scarff, 2019). A meta-analysis conducted over 29 years involving over 28,004 participants found prenatal depression and paternal PPD were relatively higher between the first 3–6 months postpartum period but might progress over a year (Paulson & Bazemore, 2010; Rao et al., 2020). Moreover, a review article found that hormonal changes (i.e., decreased testosterone levels) during pregnancy and for several months following the birth of the child might predispose fathers to experience paternal PPD (Kim & Swain, 2007). These changes can also exacerbate existing symptoms associated with PPD (Kim & Swain, 2007). While research has established PPD as a mental health problem among fathers, our knowledge regarding risk factors associated with paternal PPD among Latino fathers is limited.
Coping skills and paternal PPD
Coping skills are the conscious strategies, cognitions, and behaviors that one employs to regulate responses to adversity and distress (Carver & Connor-Smith, 2010). Coping strategies can be emotion-focused, problem-focused, support-seeking, and meaning-making (Folkman & Moskowitz, 2004). They are not necessarily adapted independently, and individuals can engage in multiple coping strategies occurring simultaneously. Incorporating these strategies is necessary for managing stress that can aid overall health. Pregnancy and the birth of a child can be stressful times for families. Research notes that fathers with paternal PPD engage in maladaptive coping skills, such as lower levels of interaction with their partner and child (Bronte-Tinkew et al., 2007). The increased economic demands of caring for the family may result in him spending more time at work while becoming avoidant towards their own feelings (Bronte-Tinkew et al., 2007; Roubinov et al., 2014).
If fathers experience PPD symptoms and are unable to incorporate adaptive coping skills (e.g., seeking support, engaging in enrichment activities, and malleable masculinity identity; Davis et al., 2011; Paulson et al., 2006; Spendelow, 2015), it can have severe consequences for their family. The consequences are their interactions with their children, their partners’ interactions with them, and their children’s behavior (Bradley & Slade, 2011). Specifically, paternal PPD is associated with adverse emotional and behavioral outcomes in children aged 3 to 5, with an increased risk of conduct problems in boys (Ramchandani et al., 2005). Without mechanisms to assist fathers in coping with challenges associated with the birth of a child, they tend to be more prone to participate in child abuse and neglect (Takehara et al., 2017). However, more studies are needed to investigate coping strategies and paternal PPD among Latino men.
Age and paternal PPD
Extant research notes that there is an association between age and postpartum depression. A recent study sampled over one million women from 138 countries found that the percentage of women self-reporting PPD symptoms was highest among 18- to 24-year-olds, at 10%. The rate of PPD then steadily declined with increasing age, dropping to 6.5% for 35- to 39-year-olds before rising slightly to 6.9% among women 40 and older (Bradshaw et al., 2022). Similar findings were further corroborated by a sample of Swedish women aged 15 to 24 who had more than two times the risk of PPD than older women (Silverman et al., 2017). For fathers in their twenties and first-time fathers, there seems to be an increased risk of depressive symptoms in the postnatal period (Bergström, 2013; Kumar et al., 2018). Specifically, low levels of educational attainment, income, partner relationship quality, and financial concerns among Swedish fathers increased the risk of depressive symptoms in the postnatal period. Still, these factors could not explain the increased risk among young fathers in their 20s (Bergström, 2013). Given that age appears to be associated with depressive symptoms in the postnatal period, there is limited evidence of this relationship among Latino fathers.
Partner PPD treatment and paternal PPD
Fathers can be important in supporting their partner in receiving PPD treatment. Fathers’ support of their partner receiving PPD treatment is associated with the mother’s decrease in PPD symptoms and other psychiatric conditions (Misri et al., 2000). Conversely, low paternal partner involvement was associated with mothers 2.34 times more likely to experience PPD compared with those whose partners were actively involved in maternal and child health services (Kebede et al., 2022). There has also been evidence of a significant association between maternal depression and paternal PPD (Epifanio et al., 2015; Paulson & Bazemore, 2010). Lastly, having a partner with PPD considerably influences a man’s risk of developing PPD by a ratio of 2.5, with an incidence of 24%–50% (Thomas, 2019; Wee et al., 2011). Given the evidence of the connection between partner PPD treatment and paternal PPD, there is limited understanding of this relationship with Latino men.
Latino gender norms and roles
Gender is discursively constructed and socially and culturally grounded. The organizing principle of acceptable masculine and feminine behaviors is essential in how an individual respond to physical problems and understands psychosocial problems (Eisler & Blalock, 1991). Gender norms restrict or influence men’s behavior, limit the expression of their gender identity to what is socially acceptable, and impact the individual and their social systems. Men who adhere to traditional male gender norms (i.e., assertive, aggressive, and hypermasculine) reported lower levels of happiness and well-being yet viewed other men as content with their lives (Kim et al., 2020). Although the majority of the participants in the study were American and White, the findings were significant in their use of a person-centered approach in evaluating men’s well-being in the context of masculinity. However, it is critical to consider masculinity and its influences in Latino culture because gender norms are neither universal nor unchanging and vary over time. Further, understanding the relative importance of ‘masculinity’ to an individual’s identity may significantly assist in successfully supporting men to self-manage their PPD symptoms.
Latino gender roles have evolved to view Latino masculinity as multifaceted. Machismo is a multidimensional construct consisting of more emotionally responsive, collaborative, and flexible masculinity styles (Torres et al., 2002). Machismo also encompasses caballerismo, suggesting an egalitarian view of machismo, including “family centeredness, social responsibility, and emotional connectedness” (Estrada & Arciniega, 2015, p. 192). Egalitarian values play a crucial role in men’s mental health. Latino men who embraced the egalitarian view of caballerismo were more likely to be content with the type of connection they have with their social support system and have an overall better quality of life (Estrada & Arciniega, 2015; Ojeda & Piña-Watson, 2014). In addition, familismo (collective commitment to family), respeto (respect), personalismo (importance of warm personal interaction), and simpatía (sympathy) are Latino cultural values tied to egalitarian masculine identity and parenting (Cabeza De Baca et al., 2014; Calzada et al., 2010; Mogro-Wilson & Cifuentes, 2021; Sotomayor-Peterson et al., 2012). As a result, egalitarian gender roles among Latino fathers should be viewed in the Latino cultural context.
Masculine gender role stress theory
Masculinity is conceptualized as an achieved status or an identity regulated by one’s beliefs, societal and cultural expectations, and enculturation. Stress is regarded as a relational concept and not defined as a specific kind of external stimulation nor a specific pattern of psychological, behavioral, or subjective reactions (Lazarus, 1991). Instead, stress is viewed as a relationship between individuals and their environment. Masculine gender role stress theory (MGRS), which has its roots in Bem’s Gender Schema Theory (1981), asserts that men who engage in a rigid commitment to maladaptive masculine identity and socialization may produce stress and result in dysfunctional coping behaviors (Eisler & Blalock, 1991). This adherence to rigid gender norms, also seen in younger men, can create unhealthy and dysfunctional behavior patterns and the lack of the ability to recognize and cope (Ojeda & Liang, 2014). Additionally, for a father whose partner is in PPD treatment, supporting them with their treatment and taking care of a newborn can further increase their stress. In the PPD period, an adjustment for all family members, the picture of understanding fathers’ PPD symptoms through this lens becomes more apparent in the postnatal period.
Current study
Several studies examining paternal PPD largely used homogenous samples (Da Costa et al., 2019; Lin et al., 2021; Massoudi et al., 2013; Psouni et al., 2017; Roubinov et al., 2014). To address the vastness of the Latine experience, it is important to have samples that attend to the representativeness of subjects (Lewis, 2021). Examining Latino fathers’ experiences with PPD can bring insights for clinical interventions and thus improve the delivery of social services for this at-risk population. The purpose of highlighting these specific themes is to continue emphasizing the importance of examining prevention and intervention efforts to reduce the negative impacts of paternal PPD on Latino fathers’ mental health.
Although there is a large body of literature on Latino gender roles and parenting, research on the intricate relationship between coping skills, age, a partner in treatment for PPD, egalitarian gender roles, and Latino father paternal PPD is limited. If a father has an egalitarian view of machismo (caballerismo), it is related to engagement in adaptive coping strategies (Eisler & Blalock, 1991; Ojeda & Liang, 2014). Younger and first-time fathers have been noted to have increased odds of paternal PPD (Bergström, 2013; Kumar et al., 2018). Lastly, having a partner receiving PPD treatment also interconnects with paternal PPD (Misri et al., 2000).
Method
Data source and study sample
The present study obtained ethical approval from a private university’s Human Subjects Institutional Review Board (Protocol # 170514). A simple nonrandomized convenience sampling strategy was employed to recruit participants from local mental health and counseling offices in a vast metropolitan southeastern region in Florida, United States. The advantage of convenience sampling is that it will yield a sufficiently large pool of relatively diverse participants (Jager et al., 2017). Recruitment occurred over 7 months with father-targeted materials (Spanish and English) given to local mental health and health facilities explaining the study. The second author of this paper used this sampling technique due to their clinical experience of seeing many men accompany their partners for their medical and mental health appointments. It has been noted that the best way to reach, engage, and recruit fathers is to meet them where they are (National Responsible Fatherhood Clearinghouse, n.d). It involves visiting locations fathers frequent, such as medical and mental health facilities, community centers, and employment programs (National Responsible Fatherhood Clearinghouse, n.d).
When a participant expressed interest in the study, they were contacted by phone, and a meeting was scheduled within two weeks of the initial phone call at the participant’s convenience. Upon meeting potential participants, they were screened to determine if they met the inclusion criteria. Inclusion criteria included: (1) identify as a cis-gender Latino man having been born in Central or South America, Cuba, Puerto Rico, or the Dominican Republic, or born in the United States with Latino heritage, (2) have at least one infant under the age of 12 months for whom they are financially responsible for, (3) participated in the prenatal maternal care, and (4) have a relationship with the mother of the infant. If participants met the criteria, they were given a consent form.
Once consents were signed, participants received a questionnaire and measurement battery that took approximately 20 minutes to complete. The questionnaire asked the following: (1) the age of the father, (2) if they are a father (parent) of a child less than one year of age, (3) the birth order of the child, (4) the number of children they have, (5) the gender of the most recent child born, (6) the country they were born in, (7) country of origin of their parents, (8) the number of years living in the United States, (9) highest education level attained, (10) if their wife or partner is currently or has been in treatment for postpartum depression, (11) income, and (12) to what degree they identify with the Latino culture. Questionnaires and measurement batteries were available in both Spanish and English. The interview took around 40 minutes and was conducted in Spanish or English. The sampling strategy yielded 101 Latino fathers.
Dependent variable
The primary outcome of interest was paternal PPD, assessed using the Edinburgh Postnatal Depression Scale (EPDS), which is a valid and reliable measure for paternal depression (Matthey et al., 2001). A recent systematic review and meta-analysis of studies validating the EPDS found that the accuracy of cut-off scores was unaffected by the prevalence of depression, the father’s age, or the language the scale was translated (Shafian et al., 2022). The ten-item EPDS has been validated among Latino fathers in previous studies and is used to measure the risk for major depression (Paredes & Parchment, 2021; Roubinov et al., 2014). Sample items include: (1) I have been able to laugh and see the funny side of things, (2) I have looked forward with enjoyment to things, (3) I have blamed myself unnecessarily when things went wrong, (4) I have been anxious or worried for no good reason, (5) I have felt scared and panicky for no good reason, (6) Things have been getting on top of me, (7) I have been so unhappy I have difficulty sleeping, and (8) I have felt sad or miserable. A higher sum score on the EPDS indicates a higher risk for postnatal depression. This analysis used the clinical cutoff score of 10 or above to identify fathers at risk for developing postnatal depression (Edmondson et al., 2010). The EPDS has a Cronbach’s α of .72.
Independent variables
Predictors of paternal postnatal depression were egalitarian gender attitudes, coping skills, and having a partner in PPD treatment. Egalitarian gender attitudes were assessed using the Gender Role Attitudes Scale (GRAS), consisting of 20 items (García-Cueto et al., 2015). The GRAS measure examined respondents’ views on gender roles, assessing egalitarian and traditional gender views. Sample items for the GRAS measure include People can be aggressive and understanding, regardless of their sex; and people should be treated regardless of their sex. Each item was scored from (1) totally disagree to (5) totally agree. The GRAS measure demonstrated good internal reliability (α = .84). A higher score on the GRAS scale indicated more egalitarian attitudes toward gender roles, while lower scores indicated more traditional gender attitudes.
A previous paper discussed the development of the Coping scale (Paredes & Parchment, 2021), consisting of seven items informed by extensive mental health experience in a hospital setting working with Latino fathers and the COPE Inventory (Carver et al., 1989). The seven items are: (1) I have used substances like alcohol or drugs, (2) I have avoided my wife, (3) I have avoided my child, (4) I have spent more time at work, (5) I have done nothing and ignored it, (6) I have turned to faith, and (7) I spoke to a mental health professional. Three items were identified as retracting from the scale reliability and were removed for the purposes of this analysis (e.g., I have used substances like alcohol or drugs, I have turned to faith, and I spoke to a mental health professional). The final scale contained four items (I have avoided my wife, I have avoided my child, I have spent more time at work, and I have done nothing and ignored it) focused on maladaptive coping techniques and demonstrated adequate reliability (α = .74). Items was scored (4) every time to (0) never. The total possible scale score was 28. Higher scores on the maladaptive coping scale indicate higher maladaptive coping techniques. Lower scores on the maladaptive coping scale represent fewer maladaptive coping techniques. To assess if fathers had a partner in PPD treatment, respondents were asked, Is your partner in PPD treatment? Respondents answered yes or no to the question.
Statistical analysis
Descriptive statistics were used to describe the sample of Latino fathers using STATA 17. The relationship between the outcome of interest, PPD symptoms, and the selected predictors, GRAS, maladaptive coping techniques, and partner in PPD treatment, were estimated using a single logistic regression model. To aid in the interpretation of models, the predictors were standardized using z-score conversion. This conversion will allow for a comparison of predictors in relative impact. The models included the number of children the fathers reported having, if their youngest child was planned, and age as control variables. The controls selected were proposed to conceptually have a relationship with PPD symptoms. A second logistic regression model was performed using STATA’s stepwise estimation to obtain a final model with only significant predictors for PPD symptoms. The probability to remove option was set to a .1 significance level.
Results
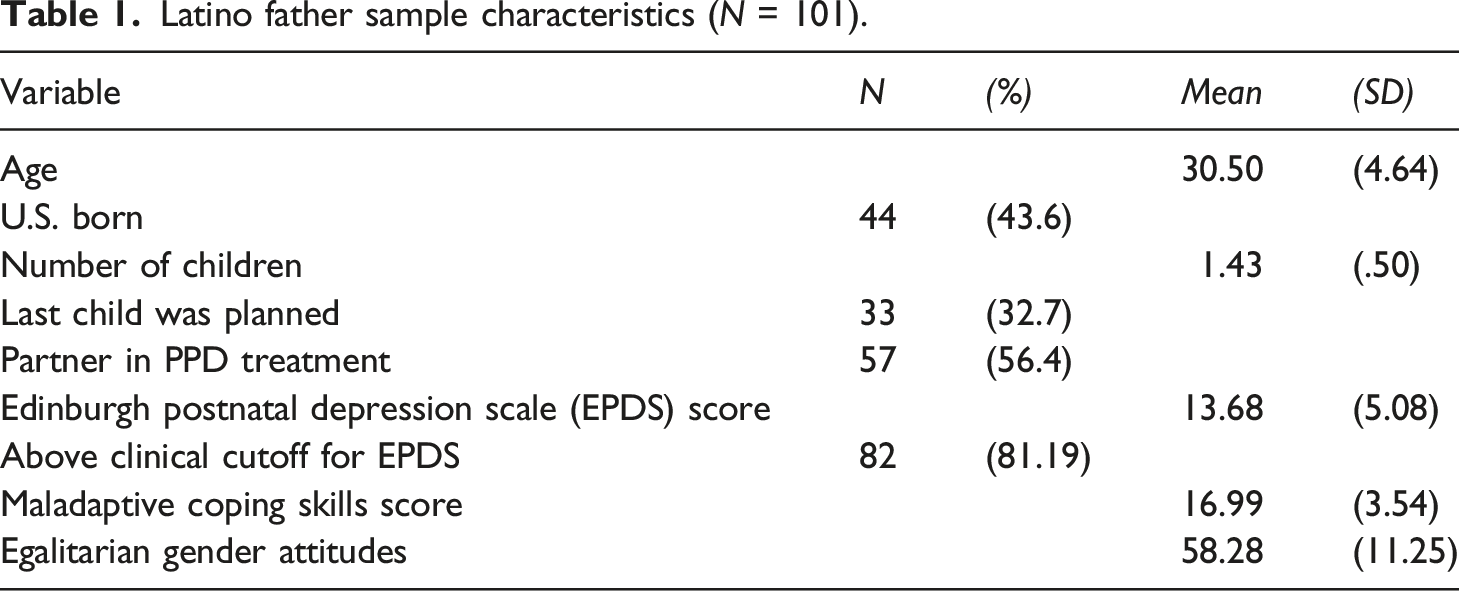
Latino father sample characteristics (N = 101).
Intercorrelations between outcome, predictor, and control variables.
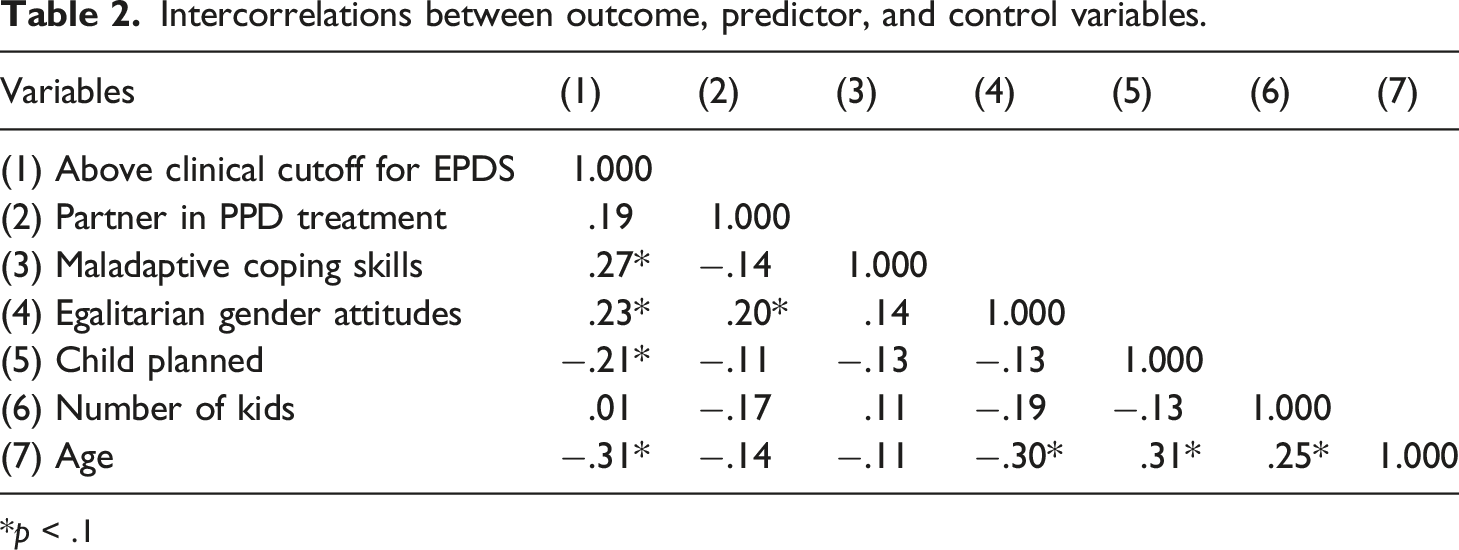
*p < .1
Logistic regression analyses of unweight results for Latino paternal PPD (N = 101).
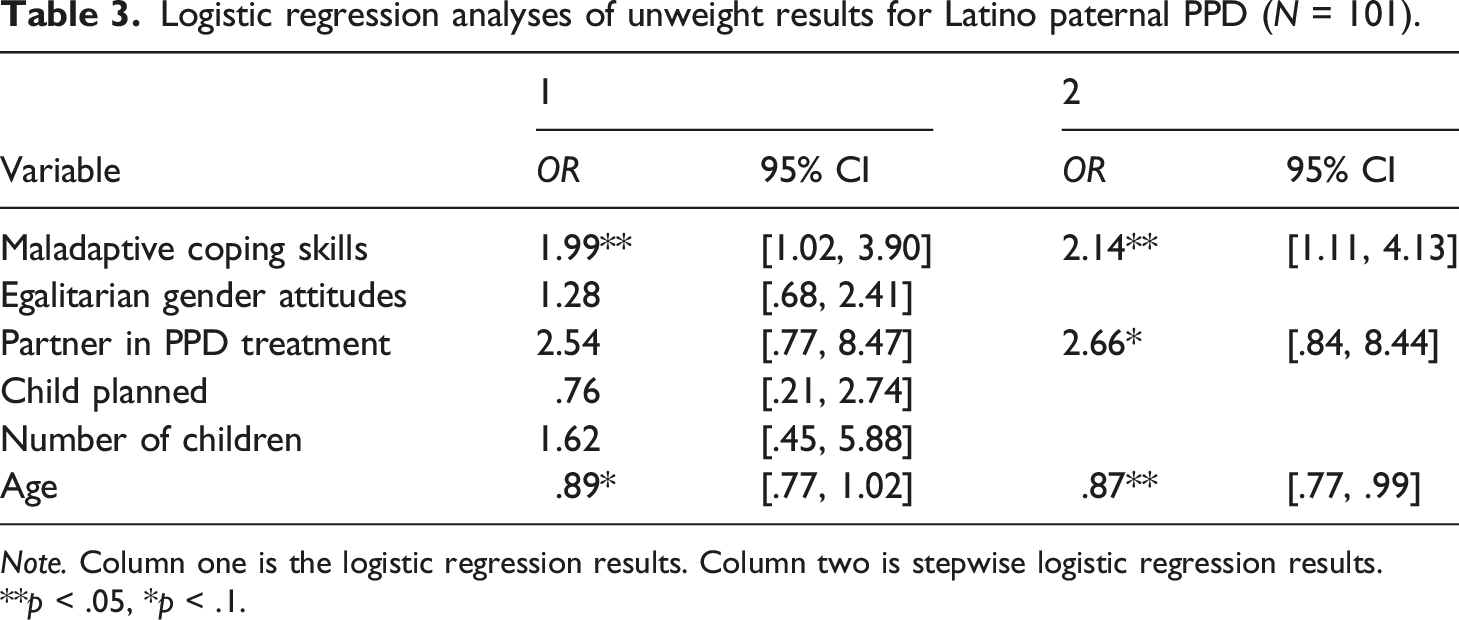
Note. Column one is the logistic regression results. Column two is stepwise logistic regression results.
**p < .05, *p < .1.
Discussion
Maladaptive coping skills and paternal PPD
Our findings demonstrated in both the logistic and stepwise logistic regressions that when a Latino father reports higher maladaptive coping, it increases the odds of being above the cutoff of PPD. Specifically, when a Latino father avoids his wife and child, spends more time at work, and ignores his feelings, these maladaptive coping techniques increase the odds of paternal PPD. MGRS theory underscores that these activities result in dysfunctional coping behaviors (Eisler & Blalock, 1991). Other studies corroborate this finding. In particular, one study found that when a Mexican-American father was seeking treatment for paternal PPD, that individual had difficulty knowing how to help his wife, who was experiencing maternal PPD (Hernandez et al., 2022). He would spend more time at work, finding it difficult to articulate his feelings with his therapist and wife (Hernandez et al., 2022). Another study found that fathers had difficulty understanding postpartum mental health conditions while experiencing a wide range of difficult emotions for them to articulate (Battle et al., 2021). Experiences of paternal PPD are characterized by the inability to cope, emotional lability, and dysphoria, making it increasingly challenging for these fathers to enable adaptive coping techniques (Letourneau et al., 2011). These findings highlight fathers’ complex feelings and experiences during the postpartum period and the need to assist them in modulating these adverse effects.
Partner in PPD treatment and paternal PPD
More than 50% of Latino fathers in our study reported that their partner is in PPD treatment, a similar result found in other studies (Madsen, 2009; Ramchandani et al., 2005). In addition, Latino fathers were more than two times more likely to meet the criteria of paternal PPD when their partner is in PPD treatment than fathers whose partners were not in PPD treatment. MGRS theory postulates that stress is a relationship between individuals and their environment (Eisler & Blalock, 1991). When mothers experience PPD, 24%–50% of partners also experience depression (Goodman, 2004). Approximately 10% of fathers will experience paternal PPD in the first year postpartum, indicating a possible indirect effect (Paulson & Bazemore, 2010). Furthermore, men with PPD partners experience more complex psychological distress than men without PPD partners (Roberts et al., 2006). experiencing PPD. A possible explanation for this is that both caregivers experience depression in the postnatal period.
Age and paternal PPD
Study findings indicated that age negatively correlated with meeting the clinical cutoff of paternal PPD. In addition, in our stepwise logistic regression, Latino fathers who are younger had increased odds of paternal PPD compared to older fathers. To our knowledge, this is the first study to demonstrate this finding among Latino fathers. Another study found similar findings among Mexican-American fathers (Roubinov et al., 2014). Our sample consists of relatively young fathers (ages 22–43), suggesting that younger Latino fathers are at increased odds of experiencing paternal PPD than older fathers. A possible explanation is that young fatherhood is associated with limited educational attainment, restricted economic opportunities (Lemay et al., 2010), and hindered psychological development that can result in poorer psychological functioning (Pears et al., 2005). MGRS theory suggests that unhealthy and dysfunctional behavior patterns may produce stress and increase the risk of depressive symptoms (Bergström, 2013; Eisler & Blalock, 1991; Kumar et al., 2018). Becoming a father is a major life transition, especially for young men, because they are expected to negotiate the transition to parenthood and early adult developmental tasks. These stressors may be further exacerbated by the hormonal changes that occur in men following the birth of a child (Kim & Swain, 2007).
Egalitarian gender roles and paternal PPD
For Latino fathers, cultural markers, such as caballersimo, a component of machismo, familismo, respto, and personalismo, inform not only their gender expectations but also how they see themselves as fathers (Henry, 2017; Owen, 2010). The odds of meeting the clinical cutoff for paternal PPD did not significantly differ between traditional and egalitarian gender attitudes. Similar results were found in exploring the correlation between egalitarian gender attitudes and paternal PPD (Paredes & Parchment, 2021). According to the MGRS theory, gender plays an important role in how one responds to stressors, whether it be psychosocial or environmental (Eisler & Skidmore, 1987). What is surprising about this finding is that it has been noted that endorsement of traditional gender role beliefs has been associated with detrimental emotional health outcomes among Latinos (Nuñez et al., 2016). Findings from this study suggest that coping skills appear to be a stronger predictor of paternal PPD than gender role attitudes. Gender role socialization affects how one feels and behaves, subsequently affecting depressive symptom presentation (Genuchi & Mitsunaga, 2015). This association appears to indicate that gender role socialization is more distal to the relationship with paternal PPD.
Treatment implications
This study aims to explore risk factors associated with paternal PPD among a sample of heterogenous Latino fathers. It does not seek to generalize research findings but provides insights into factors that appear to be associated with paternal PPD. It demonstrated the process underlying paternal PPD, which allows for more robust inferences (Smith & Little, 2018). However, it is important to contextualize these findings to enhance PPT treatment that engages with fathers. Therefore, treatment implications should be viewed as a way to further contribute to addressing Latino fathers' paternal mental health needs.
Age
Fatherhood further contextualizes how men view themselves and their roles in their families. Young fatherhood should not be viewed within a deficit perspective characterized by the extent to which they do not meet societal ideal conditions for pregnancy and parenthood (Paschal et al., 2011). It should be viewed as an opportunity and intervention to assist these men in enabling nurturing and provider roles for their families and partners. Young fathers may not have the maturity or knowledge of their emotional process to seek this type of guidance and support. Additionally, young fathers may lack extended support systems and role models and deal with complex identity changes. To support the needs of younger fathers, it is essential to bolster their support system, which can provide guidance and mentorship in developing parenting skills while navigating the transition to adulthood (Reeves, 2006). A potential support system could be a father’s support group where older Latino fathers can support younger Latino fathers, and vice-versa, in adjusting to parenthood in the postnatal period. This level of support can potentially strengthen these fathers’ cultural values of caballerismo and familismo. Given the strong role of the father within the Latino family context, understanding and supporting men’s adjustment to parenthood may offer an important insight into promoting healthy fathering and strengthening the overall family system (Pinto & Coltrane, 2009).
Adaptive coping
Implementing culturally relevant coping strategies in treating Latino fathers with PPD is essential. For Latino men, coping skills must be culturally grounded in their experiences. Cultural-specific aspects of caballerismo, familismo, respeto, and personalismo should be incorporated into the treatment sequelae of Latino men to assist them in developing adaptive coping techniques. More than 60% of Latino fathers in the sample identify with the Latino culture. Social cohesion and cultural connection to Latino heritage may prompt health benefits (Ruiz et al., 2013). Helping Latino fathers become more emotionally engaged, caballerismo may, in turn, help influence help-seeking behaviors and improve coping skills (Davis & Liang, 2012; Gonzalez et al., 2013). Increasing fathers’ identification with familismo and respeto may also enhance their ability to seek help and respond to their own needs and the needs of their family. It can also aid in establishing more harmonious interpersonal relationships with themselves and their loved ones (Glass, 2010) while reframing their thoughts (Terrazas & McCormick, 2018). In addition, anticipatory guidance that addresses the significant physical, emotional, psychological, and developmental changes may be one of the most critical aspects of helping to incorporate adaptive coping skills in working with expectant and new fathers (Torres, 2010). Lastly, helping Latino fathers embrace more personalismo can improve interactions with their family, particularly their partner and child. Bringing these culturally congruent values in working with Latino fathers in developing more adaptive coping skills can potentially aid in reducing the risk of paternal PPD (Ayón & Aisenberg, 2010; Davis & Liang, 2012; González, 2013; Smith et al., 2012).
PPD treatment
Researchers have suggested that providers give psychoeducation to the father’s partner and disseminate information to these fathers simultaneously in the clinic (Fletcher et al., 2006; Walsh et al., 2020). It is not enough for the therapeutic alliance to be strong between the clinician and clients. It is also necessary for the clinician to emphasize and be sensitive to the Latino cultural factor of familismo (Gerena, 2021). In addition, father-specific meetings, according to Fletcher et al. (2006), can prepare fathers for the mother’s birthing process while also providing peer support. Men can be engaged in PPD treatment when their female partner is also seeking treatment by increasing their engagement in pre-and-postnatal care (Bradley & Slade, 2011; Goodman, 2004). Behavioral change in families is unlikely to be sustained when only one parent is the sole target of a parenting intervention.
There should be multiple modes of access to care for the treatment of paternal PPD for fathers. Seeking help from family, peers, elders, or traditional healers is not necessarily harmful and can be viewed as ancillary support reflecting the Latino cultural values of personalismo (Ayón & Aisenberg, 2010). Structural barriers to accessing treatment, such as having multiple jobs or working long hours, may conflict with their ability to receive treatment. Therefore, incorporating accessible times and appointments for treatment would be beneficial. A same-gendered therapist who can be emotionally available, model that behavior, and create space for Latino fathers would aid in their involvement and reduce treatment attrition (Caperton et al., 2020; Eddy et al., 2019). Parent education and prevention should increase awareness of PPD and decrease the potential stigma associated with paternal depression in the postnatal period. Identifying problems from an individualistic perspective without considering systems of oppression, effects of colonialism, and generational trauma tends to blame the individual. All these factors impact Latino men and must be used as a lens in treating this population. Lastly, to provide culturally congruent treatment, especially for Latinx families, it is necessary to bolster their access to bicultural and bilingual mental and behavioral health providers in couples and individual PPD treatment for mothers and fathers (Furman et al., 2009).
Strengths and limitations
Latino paternal postnatal depression is an under-researched and underdiagnosed entity. This study identified two mechanisms that should be included in treatment for Latino men who meet the cutoff of PPD. Previous studies regarding PPD among men focus on predominately culturally homogenous samples (Gross & Marcussen, 2017; Howarth & Swain, 2020; Roubinov et al., 2014). The current study sought to include heterogeneity within the Latinx community to explore variables associated with the odds of PPD in fathers. This is essential in providing a culturally relevant and responsive approach to potentially treating these men. There is limited information regarding the treatment needs of Latino men who experience PPD. This study sought to address this and add to the literature.
Limitations of this study should be considered, mainly as a guide for future research. The cross-sectional design limits generalizability and inference on the temporality of the acquisition of PPD. Convenience sampling from mental health and counseling offices yielded a diverse but relatively small sample (Jager et al., 2017). The current study cannot ascertain whether the findings would be similar if participants were not recruited from these settings. However, exploring the individual mechanism of paternal PPD among Latino fathers offers increased power and precision of inference (Smith & Little, 2018). With moderate reliability, the Coping scale designed for this study has not undergone rigorous quantitative examination to be validated.
The omission of behavioral health risk factors such as prenatal depression symptoms, history of depressive symptoms, family history of mental health, and detailed pregnancy and birth history of their partners were outside the scope of the current study, but future research should examine it. Lastly, over a third of Latino fathers did not report their income level, making it challenging to have it as a covariate in our model. Future studies should have several indicators to assess income to capture multiple components of socioeconomic status. These limitations appear not to prove fatal to the study’s design or results.
Conclusion
As a growing population, it is essential to meet the mental and behavioral health needs of Latino fathers, especially when there are documented barriers to low utilization of mental health services among Latinx communities (Kouyoumdjian et al., 2003; Piñeros-Leaño et al., 2022). Supporting the mother and the developing infant through the postnatal period is stressed when discussing a positive outcome for the family, often leaving out the father’s pivotal role. A paradigm shift in viewing depression in the postnatal period as an issue affecting mothers and fathers would serve as a solid basis for conducting a thorough family assessment. This study proposes that Latino paternal PPD and culturally congruent treatments can be a catalyst in researchers evaluating or creating services specifically for Latino fathers with a solid evidence-based framework that centers on the values of the Latino culture. More work is needed that focuses explicitly on preventing paternal PPD, with close attention to representative samples sensitive to the considerable cultural variability in paternal involvement prenatally and postnatally. Implications from this study present a unique opportunity to develop prevention interventions that can be presented to fathers in the prenatal period to address possible postnatal symptoms.
Footnotes
Acknowledgements
The authors want to thank and acknowledge all the Latino fathers participating in this study. We appreciate your time and hope these findings increase culturally responsive treatment for men experiencing PPD.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.