
Abstract
Background
Although cystic fibrosis (CF) is a progressive, life-limiting, genetic disease, recent advances have extended survival, allowing persons with CF the time and physical and mental health to form romantic relationships. Previous studies have shown the importance of dyadic coping to positive psychosocial functioning and relationship satisfaction for people with serious chronic illness and their romantic partners, but little work has been done with persons with CF and their partners. The present study examines dyadic coping processes in persons with CF and their romantic partners.
Methods
16 adults with moderate to severe CF (Mage = 42.3, 43.8% identified as cisgender male, 56.2% identified as cisgender female) and their romantic partners (Mage = 43.8, 56.3% identified as cisgender male, 43.7% identified as cisgender female) participated in individual semi-structured interviews focused on topics related to quality of life, communication, and palliative care. We conducted a directed content analysis utilizing Berg and Upchurch’s (2007) developmental-contextual theoretical model to examine dyadic coping processes in persons with CF and their romantic partners.
Results
Consistent with the developmental-contextual model of dyadic coping, couples described adapting to health and functional declines that occurred over time. Dyads were aligned in their appraisals of illness representation, illness ownership, and perspectives of illness as a shared stressor; they used shared coping mechanisms that included supportive and collaborative actions rather than uninvolved or controlling strategies.
Conclusions
We recommend family-based approaches to medical decision-making and goals of care conversations with persons with CF and their partners, aligning those approaches with supportive and collaborative coping configurations. This may improve psychosocial outcomes for patients and their partners.
Introduction
Cystic Fibrosis (CF) is a progressive, life-limiting, genetic disease that affects over 90,000 patients and their families worldwide (Bell et al., 2020). It is generally diagnosed in childhood, requiring life-long intensive treatment. Persons with CF (PwCF) experience continuous uncertainty regarding health status and decline, and their families face caregiver burden (Kavalieratos et al., 2021; MacKenzie et al., 2014). However, with recent medical advances over the past decade, median survival has increased from 25 to 53 years of age in 2021 (Foundation, 2021; MacKenzie et al., 2014), and novel therapeutics have the potential to further extend survival for more than 90% of PwCF who are eligible for these therapeutics (Collins, 2019).
With this marked increase in life expectancy due to novel therapeutics, more PwCF have had the opportunity to form romantic relationships with long-term partners. Together with their partners, these PwCF face physical and emotional challenges related to symptom and disease management, complex treatment decisions including cost of medical care, disease progression, and advance care planning (Hobler et al., 2018; Quittner et al., 2016). Although previous studies of couples dealing with serious chronic illness have shown the importance of dyadic processes for individual coping, well-being, and relationship satisfaction, little research has been conducted with coping in PwCF and their romantic partners (Delelis et al., 2008; Werner et al., 2021). A survey-based study of 16 PwCF and their partners found high marital satisfaction, elevated levels of anxiety in a majority of couples, and less frequent use of coping strategies than chronic disease population norms (Delelis et al., 2008). A qualitative study of dyadic coping in 17 PwCF and their partners found two main patterns of dyadic coping: cooperation (similarities in perception of CF and of their roles in the relationship) and tension (difficulty accepting the disease, negative emotions, sense of burden, and loneliness) (Werner et al., 2021).
Dyadic coping in romantic partners is an interactional pattern in which positive and negative responses to stressors influence coping at the individual- and dyad-level (Bodenmann, 1995). Successful dyadic coping with romantic partners has been associated with positive psychosocial adjustment, better disease management, and survival from serious illnesses. In addition, marital satisfaction attributed to dyadic coping has been found to buffer the effects of the patient’s disease limitations on romantic partner distress and caregiver burden (Berg & Upchurch, 2007). Various theoretical models have been developed and tested (e.g., developmental-contextual model, cognitive transactional model) for dyadic coping (Badr & Acitelli, 2017; Bodenmann et al., 2019; Werner et al., 2021).
Berg and Upchurch (2007) have defined a developmental-contextual model for couples coping with chronic illness which may be particularly relevant for PwCF. In Berg and Upchurch’s (2007) model, coping is described as a transactional and relational process over time, with actions by each member of the dyad mutually influencing the other; coping is also seen as influenced by the kind of chronic illness the couple faces. Major components of the model include: dyadic appraisal, dyadic coping, and dyadic psychosocial adjustment. Dyadic appraisal consists of alignment by the dyad in illness representation (controllability, consequences), illness ownership, and shared stressors. Dyadic coping configurations are represented by coping strategy categories that include supportive, collaborative, controlling, and uninvolved. Dyadic coping is enhanced when each member of the dyad perceives the other to be involved via supportive coping (social, emotional, and/or instrumental support) and collaboration (active engagement, joint problem solving), as opposed to being involved through control (taking charge or taking over, overprotection, protective buffering) or being uninvolved (e.g., patient perceives that they are coping individually). Successful dyadic psychosocial adjustment (e.g., higher sense of self-efficacy, positive coping behaviors) is associated with relationship patterns that are aligned in dyadic appraisal and dyadic coping.
In the current study, we examined the following research questions: (1) What does dyadic coping look like for PwCF and their romantic partners? (2) Is Berg & Upchurch’s (2007) conceptual model a good fit for this disease population? This study is a secondary analysis of a mixed-methods study of unmet palliative care needs for patients with moderate to severe CF (Hobler et al., 2018). Using qualitative content analysis, we applied Berg and Upchurch’s (2007) conceptual model to examine dyadic appraisal and coping in PwCF and their romantic partners.
Methods
Procedure
In the original study from which this sample was selected, PwCF included adults (≥18 years) receiving care at the University of Washington Adult Cystic Fibrosis Program, with moderate to severe CF lung disease (FEV1% predicted <65%) (Hobler et al., 2018). Recruited PwCF were asked to refer a family member or friend closely involved with their care; this analysis utilized data from romantic partners only. Data collection occurred from June 2015–February 2016 in Seattle, WA.
Sample
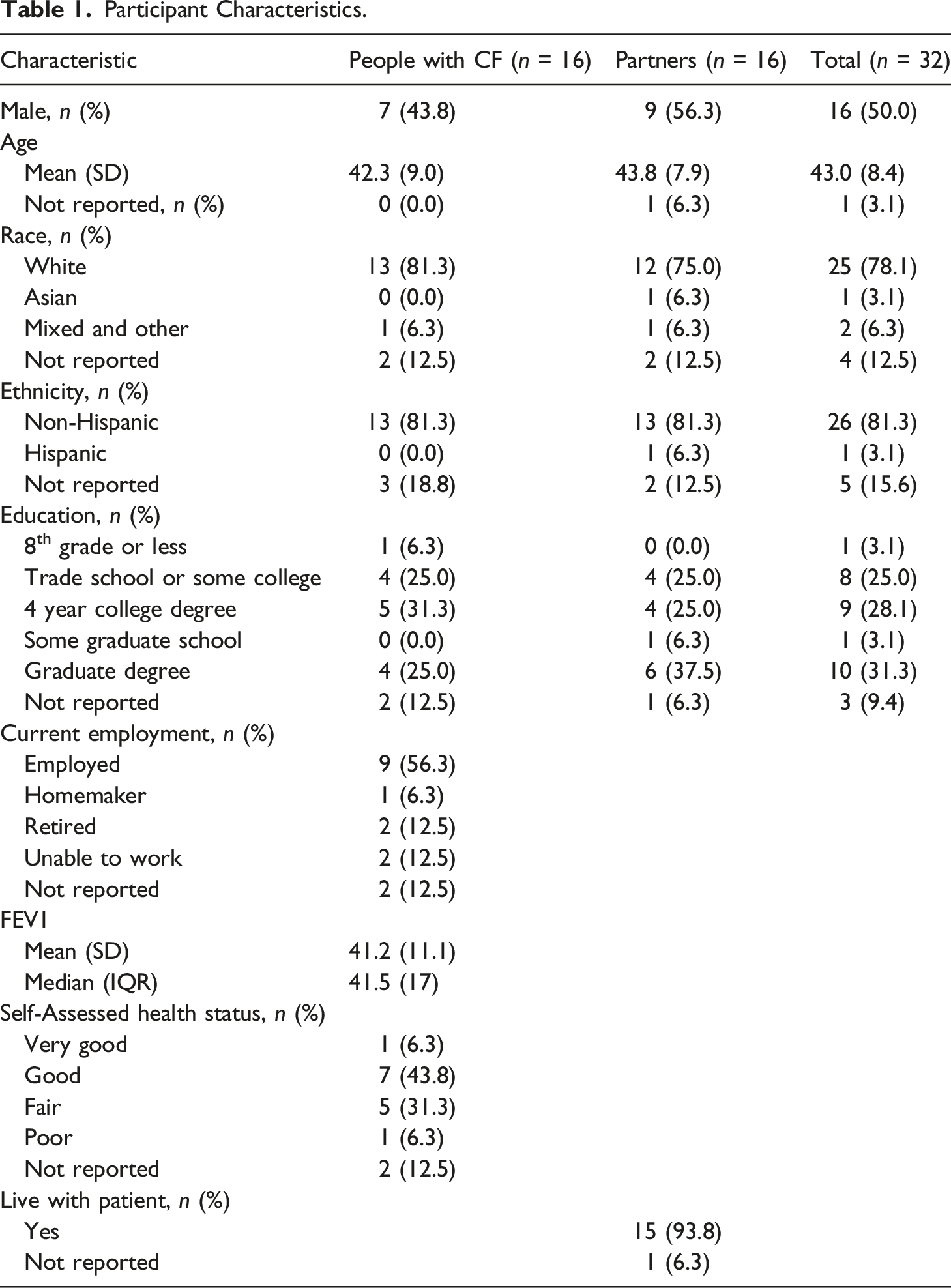
Participant Characteristics.
Measures
Participant Characteristics
Demographic data for PwCF were obtained from questionnaires (race, ethnicity, education, employment, health status) and from the Electronic Health Record (age, gender, FEV1). Demographic information for partners were obtained from questionnaires (age, gender, race, ethnicity, relationship and living status) (Table 1).
Interviews
Semi-structured, one-on-one, 30–60 minute interviews were conducted with patients and partners separately and addressed quality of life and symptoms; communication with clinicians and family; and palliative care services (Appendix A). Interview prompts included communication around treatment choices, goals of care, palliative care, difficult conversations, and challenging issues. Dyadic coping was not queried specifically but rather emerged as a key theme in patient and family member interviews.
Data collection
A researcher trained in qualitative research conducted the interviews and administered questionnaires (MH). Interviews were audio-recorded, transcribed verbatim, and deidentified. The study was approved by the University of Washington Human Subjects Division and participants provided consent.
Analyses
We conducted a directed content analysis (Hsieh & Shannon, 2005), utilizing Berg and Upchurch’s (2007) model to examine dyadic coping processes in PwCF and their romantic partners. This model’s emphasis on developmental and temporal processes that couples encounter as they face challenges of a disease that spans across the adult lifespan from young-to late-adulthood, and who have had to readjust to illness changes over time, is particularly appropriate for this population (Berg & Upchurch, 2007). Codes and coding definitions were based on components of Berg and Upchurch’s (2007) model with dyadic appraisal as a parent code (with subcodes: illness representation, illness ownership, shared stressor) and dyadic coping as a parent code with subcodes (uninvolved, supportive, collaborative, controlling). For the dyadic coping parent code, we created an additional inductive subcode (normalcy). Striving for “normalcy” was a coping configuration that showed up repeatedly in couples and was added to Berg & Upchurch’s (2007) model. Interview data from the couples as a dyad was utilized as the unit of analysis. All 32 PwCF and partner transcripts were coded by a primary coder (NL) and secondary coder (RAE), and consensus meetings were held to reach agreement. Synthesis of analyses were discussed with the full research team to finalize results of this study. We utilized Dedoose software (www.dedoose.com) for coding and analysis.
The multi-disciplinary analysis team included a clinical psychologist with expertise in mental health research (NL), physician-researchers with training in cardiovascular and pulmonary disease and palliative care (KJR, MLA, CHG, EKK), and health services investigators with expertise in palliative care and qualitative research (KSB, RAE). In the spirit of self-reflexivity, we acknowledge our standpoint as healthy and educated individuals in Seattle, Washington. Additionally, as the first and senior authors are psychologists (NL, RAE), we are interested in psychological constructs such as coping and this lens influences all aspects of the research process, from research questions of interest to study design, data collection, analysis, and interpretation of interview transcripts. Research team members have relevant clinical and personal experiences with PwCF, but are neither PwCF or romantic partners of PwCF. Thus, we do not personally identify with or relate to the lived experiences of participants in our study. However, our research and clinical backgrounds provide important training for us to synthesize relevant findings.
Results
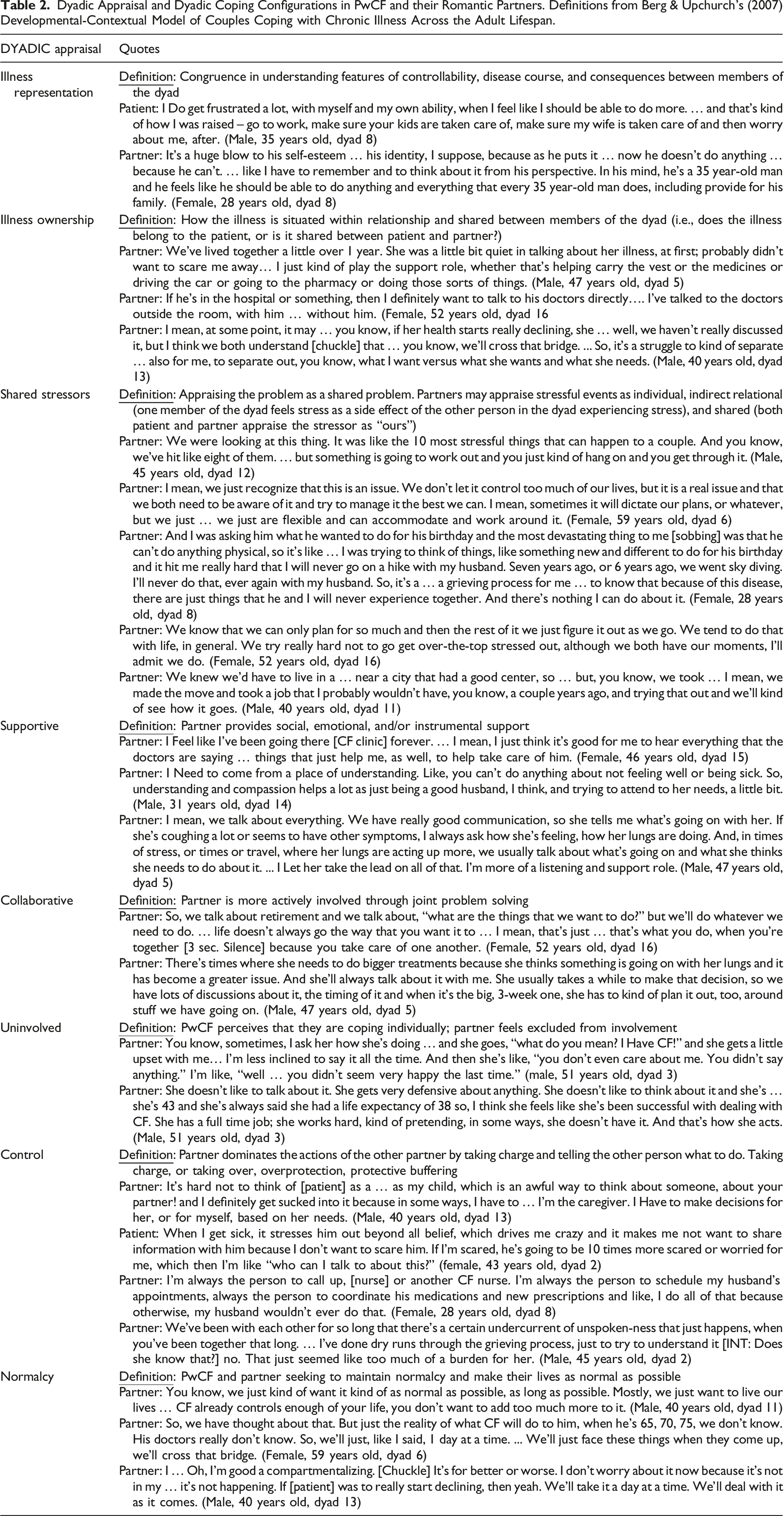
Dyadic Appraisal and Dyadic Coping Configurations in PwCF and their Romantic Partners. Definitions from Berg & Upchurch’s (2007) Developmental-Contextual Model of Couples Coping with Chronic Illness Across the Adult Lifespan.
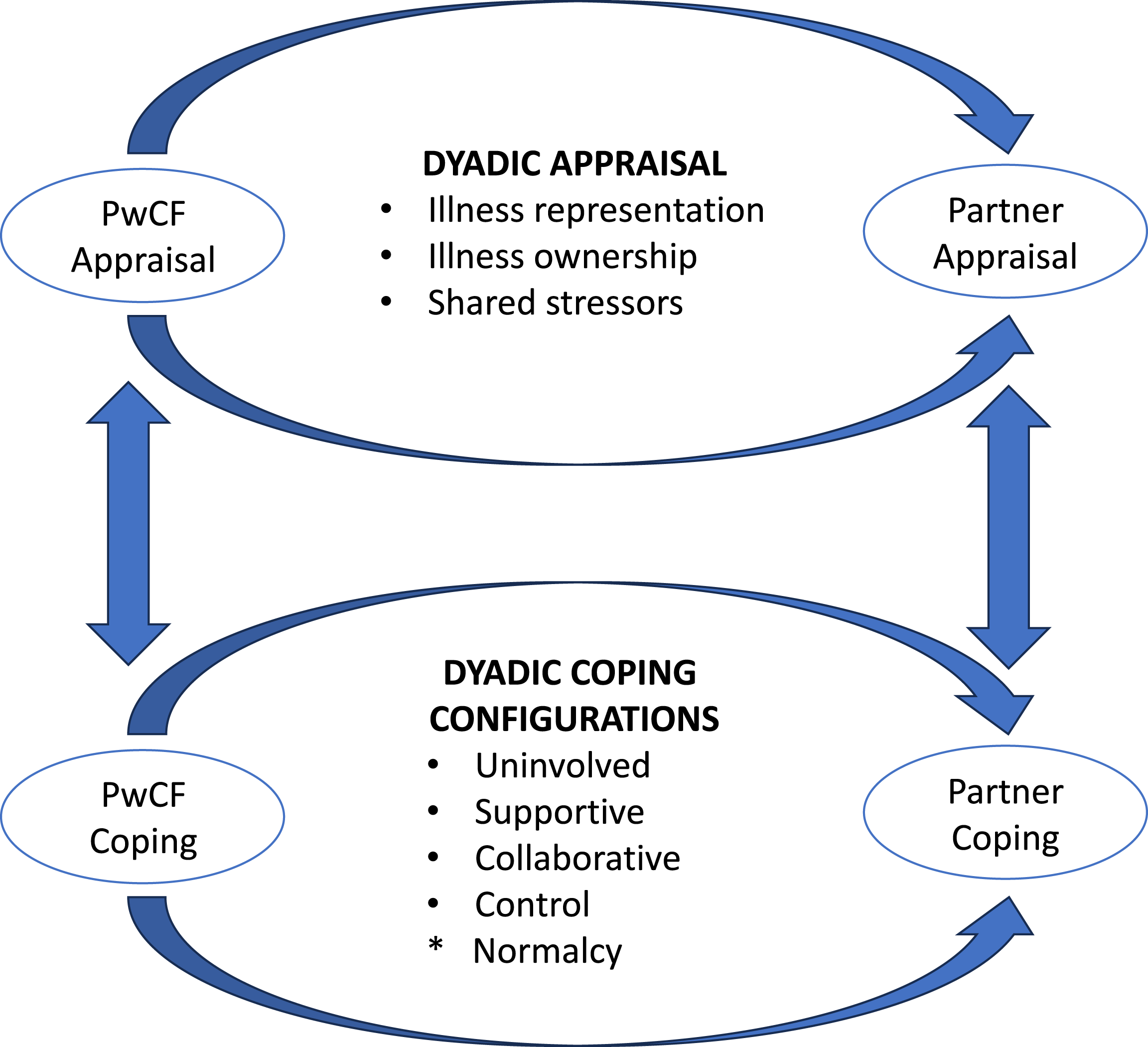
Dyadic appraisal and coping configurations demonstrated by PwCF and their romantic partners. Model adapted and annotated from “A developmental-contextual model of couples coping with chronic illness across the adult life span” by Berg & Upchurch 2007, Psychological Bulletin, 133, p. 933. *Normalcy is a new coping configuration added to the model.
Dyadic Appraisal
The dyadic appraisal component of Berg & Upchurch’s (2007) model consists of alignment by the dyad in illness representation, illness ownership, and shared stressors. Couples were generally aligned in their appraisal of illness representation, illness ownership, and shared stressors (Table 2). With regard to “illness representation” (i.e., congruence in understanding features of controllability, disease course, and consequences), couples described changes in functioning and hospitalizations for exacerbations as unpredictable with periods of relative stability followed by sudden decline. In terms of disease course and consequences of the illness, PwCF and their romantic partners engaged in a shared cycle of continually readjusting and relearning life with CF, based on stage of illness. In terms of features of controllability or lack of controllability, we heard from PwCF and their partners that PwCF had the tendency to push themselves to do too much (e.g., working full-time, exercising too hard), or that PwCF and/or partners were frustrated or saddened that the PwCF couldn’t do more of the things they wanted or needed to do. In terms of “illness ownership” (i.e., does the illness belong to the patient, or is it shared between patient and partner?), all of the partners we interviewed followed the PwCF’s lead on preferences for illness ownership. However, we found that the illness was described as “owned by the patient” by younger couples, and as “belonging to the couple” by older couples. All couples approached CF as a “shared stressor” (i.e., appraising stressors surrounding illness as a shared problem and “ours”). They described how characteristics of the PwCF’s illness (e.g., unpredictability, functional declines) as well as the need to ensure access to care determined both professional (e.g., work, education, retirement) and personal life decisions (e.g., having biological children, where to live, travel, finances). Couples acknowledged the impact of CF on quality and quantity of life, joint decision-making, and the balance between living in the moment and being prepared for CF complications.
Dyadic Coping
The dyadic coping component of Berg & Upchurch’s (2007) model consists of supportive, collaborative, controlling, and uninvolved coping configurations. The majority of dyadic coping configurations that we identified utilized positive and adaptive strategies, including “supportive” (i.e., partner provides social, emotional, and/or instrumental support) and “collaborative” (i.e., partner is more actively involved through joint problem solving) approaches (Table 2). “Supportive” coping processes included emotional support such as shared optimism, hope, functional denial, and avoidance of end-of-life conversations. Partners and patients reported that they couldn’t go on living their lives if they were focused on the “what if’s”. Both patients and partners described “collaborative” coping that included joint problem-solving that allowed them to continually adapt to CF over time. Regardless of how the PwCF was doing in terms of illness progression or CF management, PwCF and their partners discussed not wanting to be defined by their illness, and the family made accommodations to maintain quality of life and relationship satisfaction.
Not captured in Berg & Upchurch’s (2007) model, PwCF and their romantic partners commonly expressed the sentiment of striving for “normalcy” despite functional declines, “taking it 1 day at a time”, and “we’ll deal with it as it comes”. As CF is typically diagnosed in childhood, PwCF have lived with CF most of their lives and couples have lived with CF for the duration of their relationship. As a progressive life-limiting illness, PwCF and their romantic partners are continually adapting to the PwCF’s declining health status. Thus, striving for normalcy and continually adjusting to the new normal is commonly utilized as an adaptive and shared coping strategy. Our adapted version of Berg & Upchurch’s (2007) model incorporates “normalcy” (a new inductive code) as an additional coping configuration in Table 2 and Figure 1.
In contrast to these supportive and collaborative strategies, a few participants identified experiences of feeling “uninvolved” (i.e., PwCF perceived as coping individually, partner feels excluded from involvement) or “controlling” (i.e., partner dominated the actions of the other partner by taking charge and telling the other person what to do) approaches. We found that younger couples, more likely than older ones, endorsed being “uninvolved”, describing it as a way to respect and align with what appeared to be a patient’s preference. This finding was comparable to “illness ownership” in which younger couples, as compared with older ones, were more likely to defer ownership to the PwCF. In a few instances, partners discussed taking “control”. They talked about the need to take over, take charge, or provide excessive amounts of help. Within “controlling” coping configurations, some partners and PwCF also talked about an approach that has been called “protective buffering” (Berg & Upchurch, 2007), a kind of “control” and overprotection that occurs when one partner takes on behaviors that allow them to intentionally hide their concerns, worries, fears, and negative emotions in order to avoid conflict or protect the emotional well-being of their partner. As one example of “protective buffering”, CF dyads often reported that they have not had goals of care and advance care planning conversations with providers (i.e., conversations about death, dying, and end-of-life goals of care), or at least do not remember them, and did not believe their partner was ready to have such difficult conversations.
Discussion
We applied Berg and Upchurch’s (2007) developmental-contextual model of coping with chronic illness across the adult lifespan to PwCF-partner dyads. This conceptual model was an excellent fit for our study population. Persons with moderate to severe CF and their partners described aligned appraisals of illness representation, illness ownership, and perspectives of illness as a shared stressor. The majority of dyads described adaptive dyadic coping configurations over the course of illness. Our couples demonstrated “supportive” dyadic coping that included mutually cultivated optimism and hope in spite of limitations in quantity and quality of life in PwCF; this finding was consistent with the only other study to examine dyadic coping in CF couples (Werner et al., 2021). Another prominent feature of “supportive” coping in CF couples showed that partners deferred to the PwCF to determine their level of involvement and type of support. Consistent with Berg and Upchurch’s (2007) model, couples described “collaborative” coping processes that allowed them to adapt to health and functional declines in a PwCF and to make adjustments in expectations, daily routines, and future plans.
Berg & Upchurch’s (2007) model was based on a comprehensive literature review of couples coping with chronic illness. They identified 51 coping studies involving dyadic coping including illness populations such as cancer, lupus, chronic pain, diabetes, osteoarthritis, and heart disease. Consistent with previous findings on a dyadic approach to coping with chronic illness, we found that romantic partners commonly shared stressors and actively engaged in shared coping strategies (Berg & Upchurch, 2007). According to the dyadic perspective, when couples face a stressor, such as chronic illness, the stress management resources of both partners may be activated to maintain or restore a state of homeostasis in the individual, within the romantic relationship, and in relation to other social partners. Similar to previous studies of dyadic coping in chronic illness populations, we found reciprocity of support given and received among partners (Manne & Zautra, 1989; Schulz & Schwarzer, 2004; Wright & Aquilino, 1998).
Dyadic appraisal and coping processes may differ based on the type of chronic illness as they vary in their timeline (onset and course), consequences (daily management, cognitive and functional impairments), and controllability (how controllable the disease is) (Berg & Upchurch, 2007). CF is typically diagnosed in early childhood, characterized by a progressive decline in lung function, and is a frequently fatal genetic disease. Although PwCF described high levels of self-efficacy in disease management due to dealing with CF their entire lives, our sample of PwCF and their romantic partners largely described shared illness ownership and collaborative coping configurations. Older couples who were together longer and had dealt with multiple changes in health status over the years described less stress and emotional upheaval during such transition points. This is similar to past findings that suggest that long-term relationships are characterized by increased relationship satisfaction, shared goals and decision-making, less negative behaviors, and lower levels of conflict (Carstensen et al., 1995; Levenson et al., 1993). In our sample of PwCF and their romantic partners, we observed minimal use of maladaptive coping strategies. Even “uninvolved” and “controlling” coping configurations that are categorized as negative/maladaptive in the background literature were described as necessary and beneficial (e.g, use of protective buffering by PwCF and their romantic partners, “that there’s a certain undercurrent of unspoken-ness that just happens when you’ve been together that long”). Not captured in Berg & Upchurch’s (2007) model, all couples were striving for “normalcy”, to make their lives as normal as possible as a family unit despite health declines. The theme of striving towards normalcy in the context of coping with health conditions (e.g., cancer, Parkinson’s) has previously been explored (Haahr et al., 2021; Sjövall et al., 2011).
Our findings have implications for health providers and their approach to communication and support. All dyads described their romantic relationships as critically important to illness appraisal and coping. Thus, we recommend that clinicians invite partners to be involved in medical decision-making and goals of care conversations; in so doing, clinicians may facilitate a greater level of involvement and support individual and dyadic coping. Additionally, when navigating difficult conversations, clinicians may be able to capitalize on positive coping skills, such as shared optimism and normalization, while also addressing resistance in the form of “protective buffering” and overprotection. By including romantic partners in these discussions, clinicians may be able to address resistance, foster hope, and set realistic expectations in communications with PwCF and their families.
Our study has several limitations. First, the data only provide a snapshot of dyadic relationships from interviews and filtered through characteristics and biases inherent to this methodology. Second, we did not collect relationship satisfaction, dyadic coping, or psychosocial outcome measures; thus, our deductive inferences on the psychosocial adjustment component of Berg & Upchurch’s model are limited. We cannot draw conclusions on the impact of specific dyadic appraisal and coping configurations on positive or negative psychosocial outcomes in PwCF and their partners. Third, we examined data cross-sectionally which allowed us to compare younger and older dyads but were unable to evaluate developmental or historical changes in dyadic appraisal and coping over time. Fourth, we did not include those who may have been in a long-term relationship that ended. We also included only PwCF with moderate to severe lung disease; differences in disease severity could impact these key relationships. Additionally, there was overrepresentation of White and non-Hispanic PwCF and of those with college and graduate school degrees. We did not collect information on sexual orientation or disability. These limitations may decrease generalizability to the broader population of PwCF. Finally, interviews were conducted prior to the widespread availability of highly effective modulator treatments for a majority of adults with CF (Heijerman et al., 2019; Middleton et al., 2019). Although these new therapies may change the lived experience of CF for PwCF and their partners, with reduced frequency of exacerbations and slowed disease progression, our findings remain relevant in the setting of this chronic, progressive illness – particularly for those with more advanced disease.
In summary, our interviews with PwCF and their romantic partners suggest that these dyads are often aligned in their understanding and appraisal of illness and in their approach to coping with CF as a shared stressor over time. Despite the supportive and collaborative coping configurations of the PwCF-partner dyads, striving for normalcy frequently resulted in avoidance of goals of care and advance care planning conversations. Family-based approaches to medical decision-making and goals of care discussions may be particularly useful to these PwCF and their partners.
Supplemental Material
Supplemental Material - “We’ll Deal With It as It Comes”: A Qualitative Analysis of Romantic Partners’ Dyadic Coping in Cystic Fibrosis
Supplemental Material for “We’ll Deal With It as It Comes”: A Qualitative Analysis of Romantic Partners’ Dyadic Coping in Cystic Fibrosis by Nancy Lau, Kathleen J Ramos, Moira L Aitken, Christopher H Goss, Krysta S Barton, Erin K Kross, and Ruth A Engelberg in Journal of Social and Personal Relationships
Footnotes
Acknowledgements
In memory of Mara Hobler, PhD, who conducted and coded the interviews for this study. This work would not have been possible without her contributions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Food and Drug Administration (R01 FD006848), Cystic Fibrosis Foundation (AITKEN14Q10; RAMOS17A0), National Heart, Lung, and Blood Institute (5K12 HL137940-03; K23HL138154), National Center for Advancing Translational Sciences (UL1 TR000423), National Institute of Diabetes and Digestive and Kidney Diseases (P30 DK089507).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.