
Abstract
Marital satisfaction is a multidimensional construct that encompasses the satisfaction with marital interactions and with the emotional and the practical aspects of marriage. Marital satisfaction has a great impact on personal well-being and affects the family as a whole; low marital satisfaction has been associated with unhappiness and with higher divorce rates. Furthermore, marital satisfaction is related with family functioning and is an indicator of the quality of the parenting relationship. The Enrich Marital Satisfaction (EMS) scale is a two-factor and 15-items self-report measure that assesses satisfaction with the marital relationship. This study analysed the psychometric properties of the EMS among two samples: at-risk (N = 273, M = 37.05 years, 82.05% women) and community (N = 205, M = 38.38 years, 52.2% women) Portuguese parents. Participants completed the EMS and measures of parenting sense of competence, parenting stress, and parenting alliance. Confirmatory factor analyses showed that the revised two-factor model obtained the best fit, after removing a few items. Measurement invariance across the two samples was demonstrated. The EMS showed good psychometric properties, namely internal consistency, convergent and discriminant validity. The EMS is a time-efficient tool for both researchers and practitioners who need to assess marital satisfaction, a relevant dimension for family functioning and parenting.
Romantic interactions are the most significant interpersonal relationships in contemporary cultures. They involve emotional and physical intimacy and lead couples to jointly organize their familial, work, and personal responsibilities. Marriage is perceived as a step towards the initiation of adult life and the achievement of stability (Marques, 2001). Within this domain, marital satisfaction is a crucial subjective construct related to the relationship quality, encompassing intimacy, commitment, affection, agreement, and support (Delatorre & Wagner, 2020; Kwan et al., 2015). It consists of the evaluation that a person makes about the relationship, considering individual expectations (Feijão & Morais, 2018). Marital satisfaction is a key factor in individual and family wellbeing, because the degree of satisfaction in the marital domain has effects in the relationships with significant others and in the functioning of the whole family (Al-Darmaki et al., 2019; Kanter & Proulx, 2021; Kincaid, 2021; Oosterhouse et al., 2020; Yoo, 2020).
A satisfactory marital relationship brings several benefits to the individual, such as a high quality of life and emotional health (Ferrão et al., 2019). Men tend to report higher levels of marital satisfaction than women (Jackson et al., 2014), although this difference is not consistent in all studies (Belsky et al., 1991; deMontigny et al., 2013; Kim, 2010; Liu & Wang, 2015). In addition, sociodemographic factors such as good health and a high income are protective factors to the maintenance of a high marital satisfaction (Mosmann et al., 2006). The individuals who are satisfied with their marriage tend to have higher levels of happiness and greater ability to deal with adverse situations (Bradbury et al., 2000), a greater sense of perceived parental competence and fewer depressive symptoms (e.g., Choi & Jung, 2021). In addition, marital satisfaction is the strongest predictor for coparenting quality (Fan et al., 2020) and influences the self-efficacy and perceived competence to perform the parental role (Eskandari et al., 2019).
In contrast, conflicts in the relationship and, consequently, low marital satisfaction can impair the individual’s psychophysiological and social functioning and are strongly related to high divorce rates (Bradbury et al., 2000; Ferrão et al., 2019). The literature in this area has consistently shown that marital dissatisfaction is mainly reported by women (Jackson et al., 2014; Shen, 2001), unemployed and lower income individuals (Capistrant et al., 2020; Mosmann et al., 2006).
Specifically, low-income couples tend to exhibit more hostility and less warmth than their higher income counterparts (Conger et al., 1990; Masarik et al., 2016). This phenomenon is partly explained by the Family Stress Model (e.g., Conger et al., 1999), which suggests that the economic pressures that couples face increase each spouses’ emotional distress, and this in turn can lead to or heighten interpersonal conflict. Financial hardship seems to have a more important role in the couple’s communication quality than other variables such as past life events or depression (Williamson et al., 2013).
The number of children also seems to impact the marital relationship, as couples with more children tend to report lower marital quality than couples with fewer children (Belsky & Pensky, 1988; Twenge et al., 2003). Having a child can significantly destabilize a romantic relationship, because it takes the couple to a new stage in their life cycle, representing a crisis that implies rearrangements (deMontigny et al., 2013). It means that the exercise of parenting may be a potential risk factor for marital dissatisfaction, as it takes time away from the couple’s intimacy (Twenge et al., 2003) and increases stress (Kwan et al., 2015). In this line, marital satisfaction changes throughout the different developmental stages of the couple; some authors argue that these variations can be represented in a U-shaped model, where marital satisfaction is high during the first years of the relationship, followed by a decline in subsequent years - which corresponds to the challenge of parenthood - and rising again years later, when the children are older and the couple regains time to focus on their romantic relationship (Pérez & Estrada, 2006; Stephen & Raj, 2014).
Regarding the influence of marital satisfaction in family functioning, research shows that low levels of marital satisfaction are associated with more distant parental-child relationships (Christopher et al., 2015), harsher discipline (Liu & Wang, 2015), and lower paternal responsiveness and sensitivity to children (Knopp et al., 2017), which is detrimental to the children’s development (Ferrão et al., 2019). Existing research emphasizes that the marital relationship between parents may have important repercussions in children’s’ socioemotional development and behavioural problems (Konishi et al., 2018). In addition, marital dissatisfaction has adverse effects for the members of the couple, such as cardiovascular problems (Liu & Waite, 2014), alcoholism (Cranford et al., 2011) and a decrease in self-esteem (Voss et al., 1999). Low marital satisfaction has also shown strong associations with increased levels of anxiety (Delatorre & Wagner, 2020), depression (Goldfarb & Trudel, 2019) and burnout (Mikolajczak et al., 2018).
The relevance of marital satisfaction for individual well-being and its centrality to the entire family system functioning has justified the elaboration of several measures to assess this construct. Measuring this construct becomes even more pressing in at-risk families, where the children’s well-being may be compromised and where the marital satisfaction may act as a protective factor (Abidin, 1992; Belsky & Jafee, 2015). The continuity between the affective tone of the marital dyad and the parents-child triad – a “spill-over effect” – has been observed in numerous studies, where frequent marital conflict is associated with inadequate parenting because these conflicts diminish the availability of parental support (Wilson & Gottman, 2002). Unsatisfactory marital relationships have also been associated to inadequate maternal behaviour, lower maternal sensitivity and to an insecure and disorganized mother-child attachment (Finger et al., 2009).
Some of the instruments that assess marital satisfaction conceptualize it as a multidimensional construct and focus on different aspects, such as communication (Schumm et al., 1979), intimate relationship (Braiker & Kelley, 1979) or adjustment (Spanier, 1976), whereas others consider that satisfaction is unidimensional (Goldfarb & Trudel, 2019). The most used measures in the literature are the Dyadic Adjustment Scale (DAS; Spanier, 1976), the Relationship Assessment Scale (RAS; Hendrick, 1988), the Marital Adjustment Test (MAT; Locke & Wallace, 1959) and the ENRICH Marital Satisfaction Scale (EMS; Fowers & Olson, 1989, 1993).
The Marital Satisfaction Scale was developed based on the Evaluating & Nurturing Relationship Issues, Communication, Happiness inventory (ENRICH Inventory; Fowers & Olson, 1989) comprising 125 items for the evaluation of the marital relationship. This complete version consists of 14 scales - Idealistic Distortion, Marital Satisfaction, Personality Issues, Communication, Conflict Resolution, Financial Management, Leisure Activities, Sexual Relationship, Children and Parents, Family and Friends, Equal Roles, Religious Orientation, Marital Cohesion and Marital Change. The original study of ENRICH Inventory was conducted with 672 couples (mostly White), showing adequate consistency values for all scales, except for the Sexual Relationship subscale (α = .48). However, due to the length of this measure, Fowers and Olson (1993) created the EMS, a shorter version of ENRICH Inventory, aiming to assess satisfaction with the marital relationship, using 15 items which are grouped into two subscales: Marital Satisfaction (MS) with 10 items and the Idealized Distortion (DI) with five items. These two scales allow to compare the scores of each spouse and to analyse the degree of distortion implicit in this subjective evaluation, revealing two components of satisfaction - the perceived and the real one felt by each spouse (Fowers & Olson, 1993). Items in this measure cover dimensions such as communication, conflict resolution, partner’s personality characteristics and habits, financial management, leisure activities, sexual relationship, the exercise of parental responsibility, religious orientation and other values, and the relationship with the families of origin (parents and in-laws) and friends. The resulting score classifies marital satisfaction on a scale of five points, ranging from “very low” to “very high”. Using a national sample of 7261 American couples (mostly White, with a mean age of 32.5 years), the authors reported good psychometric properties with a Cronbach’s alpha of .86, a test re-test reliability coefficient of .86 and strong total-item correlations, with values ranging between .52 to .82 (Fowers & Olson, 1993). Concurrent validity was measured by the Locke-Wallace Marital adjustment test (Locke & Wallace, 1959) and the single item Family satisfaction, showing high positive correlations with both (.73 and .81, respectively).
Since then, this scale has been used in several investigations exploring the associations of marital satisfaction with individual health (Roberson et al., 2018), depressive symptoms (Goldfarb & Trudel, 2019) and stress (Najmi et al., 2018). This concept has also been assessed in relation to other relevant variables of family functioning, such as co-parenting alliance (Camisasca et al., 2019), parenting self-efficacy (Hajihashemi & Amidi-Mazaheri, 2018; Kwan et al., 2015), and parenting stress and practices (Liu & Wang, 2015; Twenge et al., 2003).
Furthermore, although some studies chose not to use the idealized distortion subscale (e.g., Arab et al., 2015; Escribà-Agüir & Artazcoz, 2011), the EMS has been adapted and validated in other countries, such as Brazil (10 items; Ferrão et al., 2019), China (10 items; Li, 1999), Spain (10 items; Escribà-Agüir & Artazcoz, 2011), India (15 items, Pandya, 2019), Iran (10 items, Arab et al., 2015) and Japan (10 items; Suzuki, 2010). Most of these validation studies reported psychometric similar results to the original validation, with satisfactory validity and internal consistency. Additionally, in the Brazilian version of the instrument, structural invariance between men and women was also verified (Ferrão et al., 2019). In Portugal, Marques (2001) adapted the longer version of this instrument, the ENRICH inventory, with a sample of 174 married individuals living in Coimbra (75.9% women, ages ranging 22–57 years). The results revealed high levels of internal consistency, with a Cronbach’s alpha of .93, supporting the reliability of this measure. However, this version contains 80 items, which precludes its inclusion in an assessment battery of family functioning, thus limiting its clinical utility. It is paramount to validate time-efficient instruments that do not overburden participants and that allow professionals and academics to gather information about family relationships.
In the European Portuguese context, the brief ENRICH Marital Satisfaction Scale has not yet been used and there are no published validation studies, neither with normative adults nor with at-psychosocial risk couples. In Portugal there is a need for short, valid and reliable scales that measure marital satisfaction. The number of divorces in Portugal has increased in the last decades, converging with the number of marriages. The divorce rate for every 100 marriages in 2019 was 61.4. Regarding blended families, the available data are less recent but show that they constituted 8.12% of the family units (PORTDATA, 2021). Since marital satisfaction seems to be determinant for individuals’ well-being, for the stability of the marriage (Bradbury et al., 2000), and, consequently, of the entire family system (Fan et al., 2020; Kwan et al., 2015), it is important to evaluate this domain.
The present study analyses the psychometric properties of the EMS among a Portuguese sample of community and at-risk parents, using confirmatory factor analysis to examine its internal structure. At-risk parents refer to those who face serious problems and accumulate multiple stressful life events (e.g., marital conflict, abuse, economic problems, violent neighbourhood, or inadequate social networks). These personal and relational circumstances in which they live hinder or limit their parenting skills, however, the situation is not severe enough to require child out-of-home placement (Byrne et al., 2012). In our study, the at-risk sample was defined as parents whose children had an active case in Child Protection services, whereas the community sample parents’ children had never been had an active case in those services.
We expect that: (1) the two-factor structure of the EMS would be replicated among the two samples; (2) the EMS would show cross-sample measurement invariance; (3) the EMS would show good internal consistency; (4) the EMS would show convergent and discriminant validity, with significant positive correlations with parenting alliance, parenting efficacy and satisfaction measures, and significant negative correlations with parenting stress; and (5) differences would be found among community and at-risk parents regarding marital satisfaction, with at-risk parents reporting lower levels of marital satisfaction than their community counterparts.
Method
Study design
This was a quantitative, cross-sectional descriptive study, with a simple retrospective investigation plan. Is also an instrumental study, because it aims to assess the psychometric characteristics of a measure (Montero & León, 2005).
Participants
Two samples from Algarve (South of Portugal) were included in this study: a community sample of 205 parents (M = 38.39 years; SD = 5.84 years; age range = 23–53 years) who voluntarily agreed to participate and an at-risk sample, including 273 parents whose children had an active case in Child Protection Services (CPS) (M = 37.05 years; SD = 8.07 years; age range = 19–58 years).
The community sample was composed of 52.2% of mothers and 47.8% fathers, with a medium-high education level: 42% had completed secondary education and 28.3% had completed higher education. Regarding work qualification, 33.2% had low qualification jobs, 41% medium qualification jobs and 25.9% high qualification jobs. On average they had 1.69 children (SD = 0.79, Range = 1–7) and 47.3% were girls, with an average of 6.90 years (SD = 3.19).
The at-risk sample was composed mainly of mothers (80.1%) and had a lower educational level: 52% had not completed compulsory education and 30.6% had completed only primary education. Regarding work qualification, 71.2% had jobs with low qualification, 24.8% had jobs with medium qualification and 4% with high qualification. On average they had 2.63 children (SD = 1.53, Range = 1–10) and 41.2% of their children were girls, with an average of 10.83 years (SD = 4.68).
No significant differences were found between the community and the at-risk samples regarding participants’ age (t = 0.94, df = 462.03, p = n. s., d = 0.08), but differences were found on participants’ education level (χ 2 = 152.11, df = 3, p ≤ .001, Cramer V = 0.57), work qualification level (χ 2 = 50.54, df = 2, p ≤ .001, Cramer V = 0.39) and sex distribution (χ 2 = 49.01, df = 1, p ≤ .001, Cramer V = 0.32).
Instruments
The Enrich Marital Satisfaction scale (EMS, Fowers & Olson, 1993). As described before, EMS evaluates the global satisfaction with the marital relationship. It is a self-report measure comprising 15 items, rated on a 5-point scale ranging from 1 (“No, totally disagree”) to 5 (“Yes, totally agree”), that includes two subscales: Marital Satisfaction (MS, 10 items, e.g., “I am very satisfied with our way of making decisions and solving problems”) and Idealized Distortion (ID, five items, e.g., “Our relationship is perfect”). The Idealized distortion scale is used to correct the Marital Satisfaction scale score when the participants describe the marriage in an implausibly positive way. Global EMS score is calculated with the following formula: marital satisfaction - [(marital satisfaction) * (correlation between marital satisfaction and marital distortion)2 * (marital distortion * 0.01)]. Higher scores indicate higher marital satisfaction. The Portuguese version was developed by a process of forward-backward translation with the collaboration of two translators who had a background in psychology research. The cultural adaptation was particularly considered, considering clarity, common language use, and conceptual equivalence of the scale.
Parenting Alliance Inventory (PAI), (Abidin & Brunner, 1995, Portuguese version: Nunes et al., 2021a). The PAI assesses the degree of commitment and cooperation between parents in childrearing. It is a self-report measure, comprised by 20 items (e.g., “When there is a problem with our child, we work out a good solution together”), answered through a 5-point scale ranging from 1 (“Strongly Disagree”) to 5 (“Strongly agree”). The total PAI score is obtained by adding the 20 items; higher scores indicate stronger support between partners as parents. The psychometric data of the present study demonstrate adequate internal consistency (α = .96 to at-risk sample, and α = .95 to community sample).
Parenting Sense of Competence (PSOC). The PSOC (Johnston & Mash, 1989, Portuguese version: Nunes et al., 2016) is a 16-item self-report measure, measuring two dimensions of parenting: efficacy (7 items, e.g., “I honestly belief I have all the skills necessary to be a good mother to my child”) and satisfaction (9 items, e.g., “My talents and interests are in other areas, not in being a parent”). For both subscales, items are presented on a 6-point scale ranging from 1 (“Strongly disagree”) to 6 (“Strongly agree”). Higher scores indicate greater parental sense of competence. In this research, the PSOC showed satisfactory levels of internal consistency, with α = .74 on efficacy and α = .84 on satisfaction for community sample; α = .74 on efficacy and α = .70 on satisfaction for risk sample.
Parenting Stress Index - Short Form (PSI), (Abidin, 1995, Portuguese version: Santos, 2008). This is a self-report instrument that measures three dimensions of stress associated with the parenting role: Parental Distress (PD), Parent-Child Dysfunctional Interaction (PCDI) and perception of the child as a Difficult Child (DC). The subscale Parental Distress quantifies the individual’s feelings of discomfort with the parenting role (e.g., “I feel that I cannot handle things”). The Parent-Child Dysfunctional Interaction subscale evaluates the extent to which the parent feels that the child meets the parent’s expectations and the way their interaction makes the parent feel (e.g., “My child doesn’t giggle or laugh much when playing”). The Difficult Child subscale focuses on the child’s characteristics and behaviours that facilitate or restrain the parent (e.g., “My child cries or fusses more often than other children”). The PSI is composed by 36 items answered on a 5-point range where 1 (“Strongly Disagree”) to 5 (“Strongly Agree”). The minimum and maximum possible scores for PSI are 12–60 for each subscale and 36–180 for the PSI-SF total score, where higher scores correspond to greater distress associated with the exercise of parenthood. Internal consistency for the present study, estimated by Cronbach’s alpha, was adequate for all subscales in both samples (α = .89 to PD, α = .80 to PCDI, α = 75 to DC, and α = .91 to total PSI for community sample; and α = .82 to PD, α = .80 to PCDI, α = 84 to DC, and α = .90 to total PSI for the at-risk sample).
A sociodemographic questionnaire was also applied to gather information about participants’ sex, age, education level and work status.
Procedures
This study was approved by the Scientific Council of the Faculty of Human and Social Sciences of University of Algarve (Ref. CC_55_20/12/2017). At the recruitment stage, all participants were informed about the study aims, the anonymous and confidential nature of their responses as well as the possibility of withdrawing from the study at any point without consequence. Participants did not receive any compensation. Written informed consent was obtained from all participants. The questionnaires were applied individually, with paper-pencil and face-to-face. The procedures differed for the two sub-samples. For the at-risk sample, mothers and fathers with an active case in the CPS of Algarve (South of Portugal) were asked to participate in the study by their caseworker. Parents’ inclusion criteria were: (1) Having been enrolled in CPS for family preservation reasons for at least 3 months and (2) Not facing a family crisis during the recruitment and data collection periods. For the community sample, 14 master students from the Psychology Department of the University of Algarve using a snowball sampling technique, were asked to collaborate in this study by recruiting five parents each who never had an active case in CPS, and to have them complete the questionnaires.
Statistical analysis
Data were processed with IBM SPSS 24.0 (IBM Corp., Chicago, IL.) and EQS 6.3 (Bentler & Wu, 2015). Missing data on the item level were extrapolated using the missing value analysis of SPSS (EM algorithm) after checking that data were missing completely at random using Little’s MCAR test (p = .08). If more than 10% of the items of a questionnaire were missing, the case was excluded from the corresponding analyses. Therefore, 2 cases were deleted from subsequent analysis. Statistical assumptions for parametric analyses were checked following (Tabachnick & Fidell, 2019) recommendations, namely normality, univariate and multivariate outliers, linearity, and multicollinearity, with satisfactory results.
To assess the factorial structure of the Portuguese version of the EMS, a Confirmatory Factor Analysis (CFA) performed with ML robust estimation methods was applied (Byrne, 2014). Goodness of fit indices were calculated, including Satorra-Bentler chi-square/degrees of freedom, Comparative Fit Index (CFI), Incremental Fit Index (IFI), Root Mean Square Error of Approximation (RMSEA) and Akaike Information Criterion (AIC). Values higher than .90 were considered as acceptable for the Incremental Fit Index, also known as Bollen’s IFI (West et al., 2014). Regarding the AIC, that aims to measure the discrepancy between the true model and the hypothesized model, the model with the smallest AIC should be selected (DiStefano, 2016). The CFA was completed on the original scale items using a correlation matrix. Modification indices were considered to check if any suggestion of model modification would significantly improve the measurement model. Items with standardized loading above .30 were retained because factorial loads should be considered significant when they are higher than this value (DiStefano, 2016).
Measurement invariance was also evaluated. The S-Bχ 2 difference test, the ΔCFI, and the ΔRMSEA was used to determine if the constraints significantly deteriorated the fit of the model (Cheung & Rensvold, 2002). Cronbach’s alpha was used to analyse reliability. Pearson correlations were used to analyse associations between scale variables and to analyse convergent and discriminant validity. Univariate analysis of variance tests was used to compare groups. To clarify the degree of accuracy of the statistical judgments and the strength of the relationship between the variables effect size calculations (η2 and r) were performed.
Results
Confirmatory factor analysis
Goodness of fit indices for different ML models of EMS (community and at-risk sample).
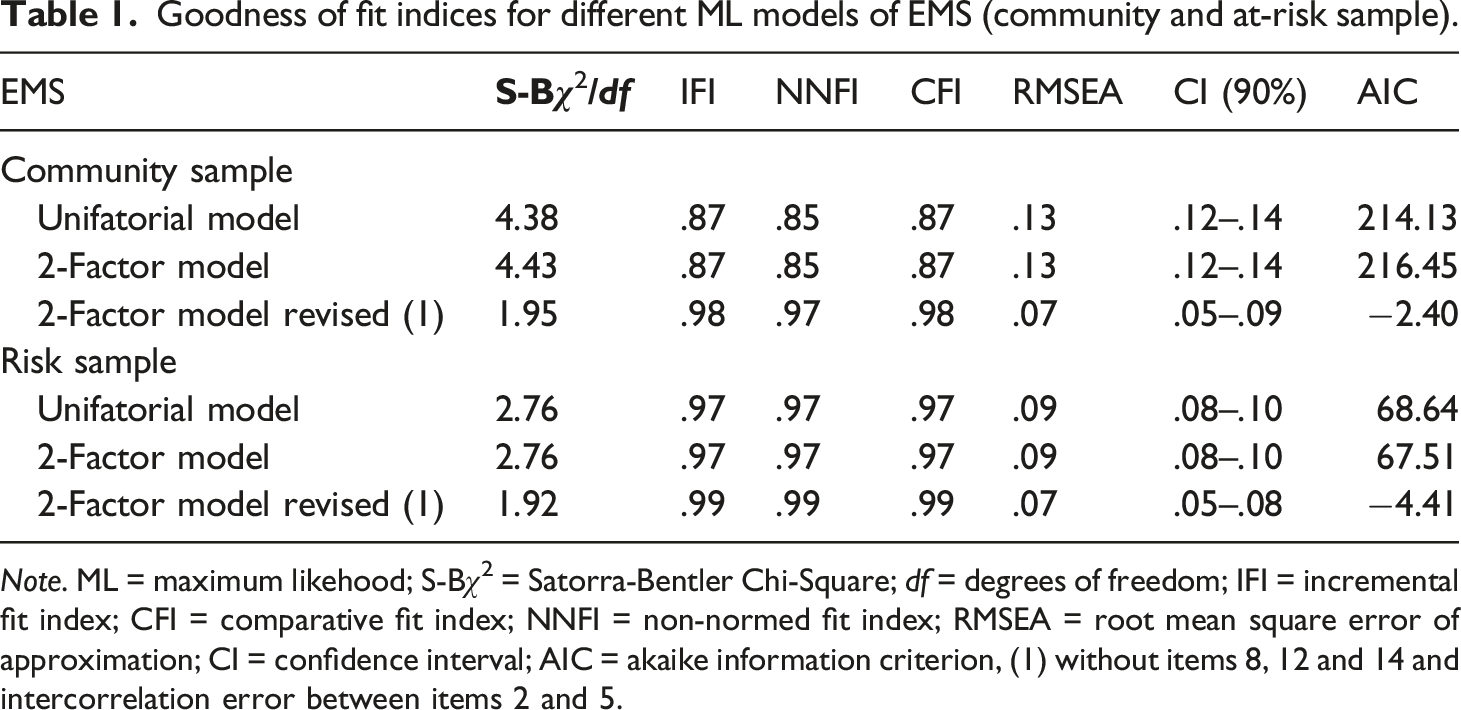
Note. ML = maximum likehood; S-Bχ2 = Satorra-Bentler Chi-Square; df = degrees of freedom; IFI = incremental fit index; CFI = comparative fit index; NNFI = non-normed fit index; RMSEA = root mean square error of approximation; CI = confidence interval; AIC = akaike information criterion, (1) without items 8, 12 and 14 and intercorrelation error between items 2 and 5.
In this model, the problematic items that presented low loadings and low corrected item-total correlations were removed (items 8 “I am unhappy about financial position and the way we make financial decisions”, 12 “I am not satisfied with the way we each handle our responsibilities as parents” and 14 “I am dissatisfied about relationship with my parents, in-laws, and/or friends” from factor marital satisfaction).
Items loadings for EMS (community sample/risk sample).
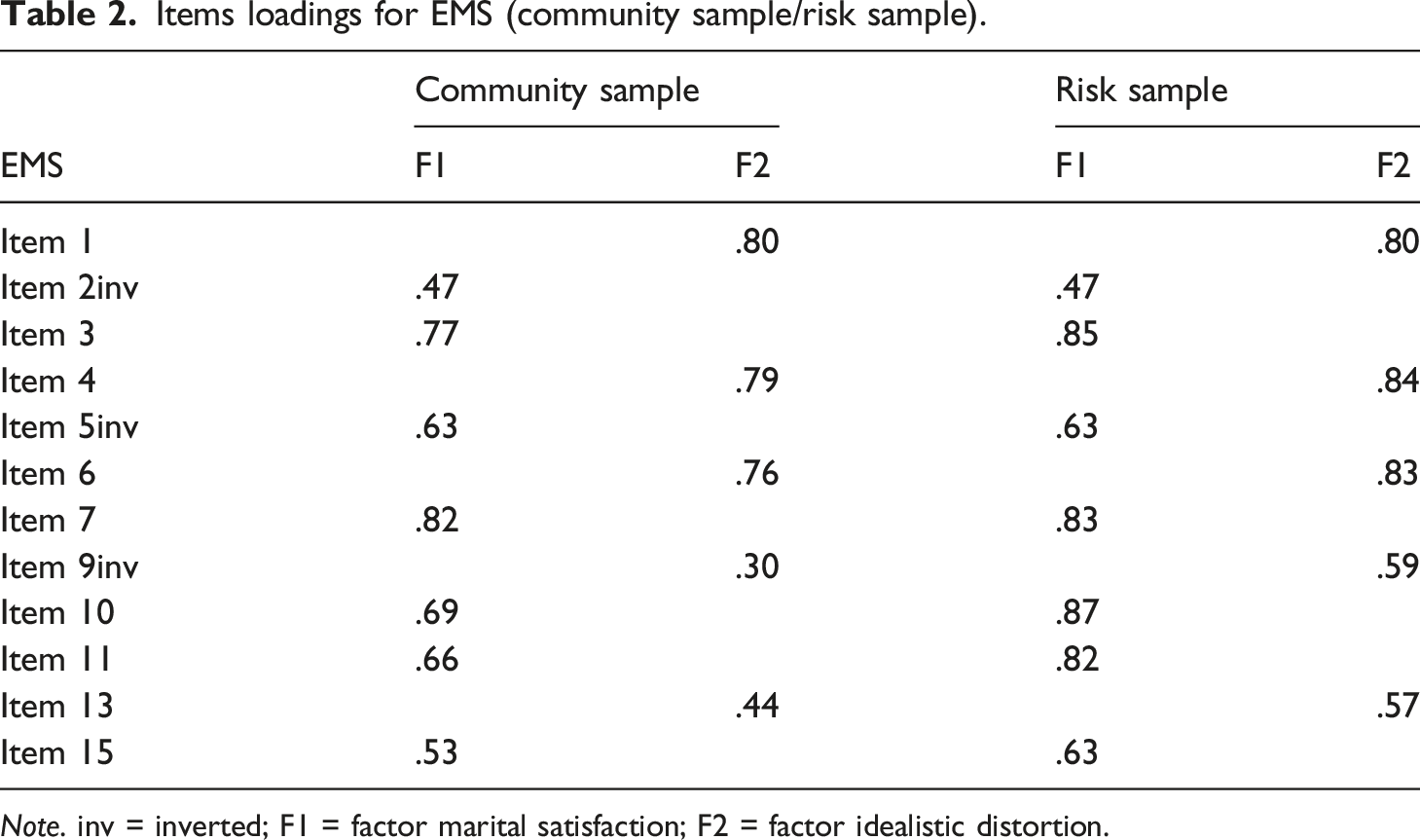
Note. inv = inverted; F1 = factor marital satisfaction; F2 = factor idealistic distortion.
Cross-samples invariance
Tests for invariance of the EMS goodness of fit statistics.
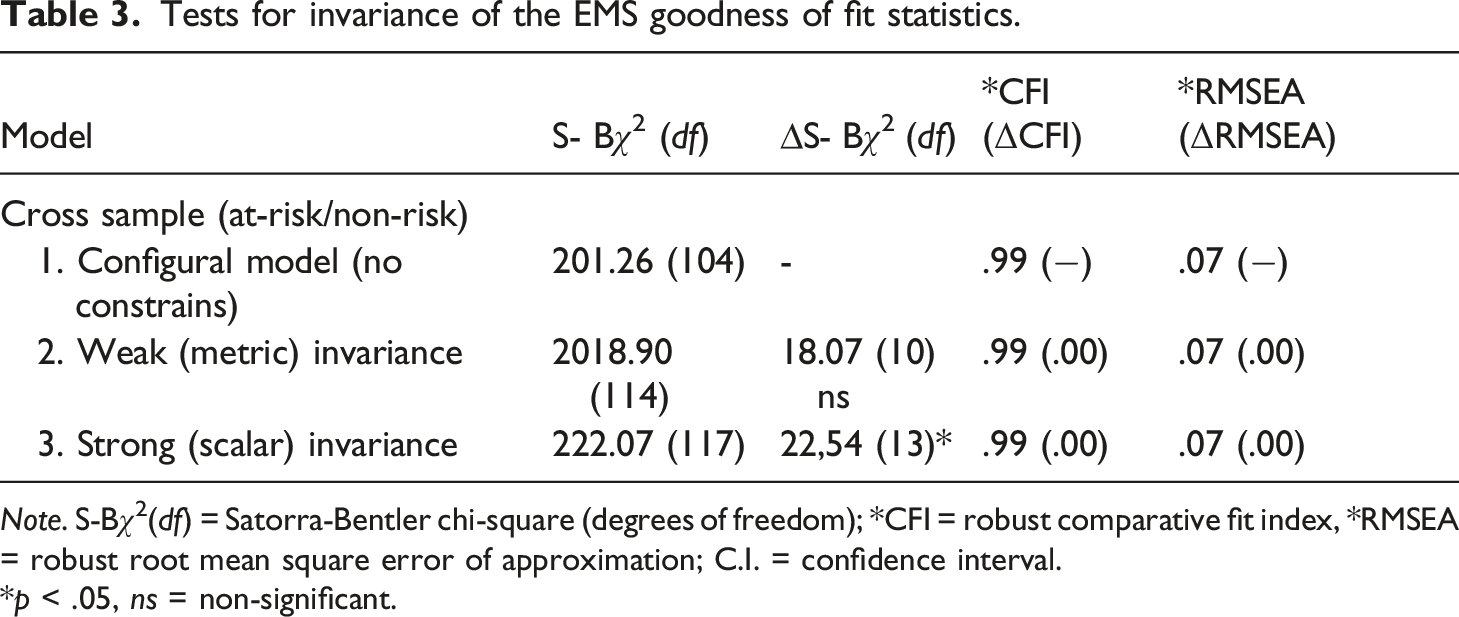
Note. S-Bχ2(df) = Satorra-Bentler chi-square (degrees of freedom); *CFI = robust comparative fit index, *RMSEA = robust root mean square error of approximation; C.I. = confidence interval.
*p < .05, ns = non-significant.
Reliability analysis
Cronbach’s alphas, mean inter-item correlations, and corrected item-total correlation ranges.
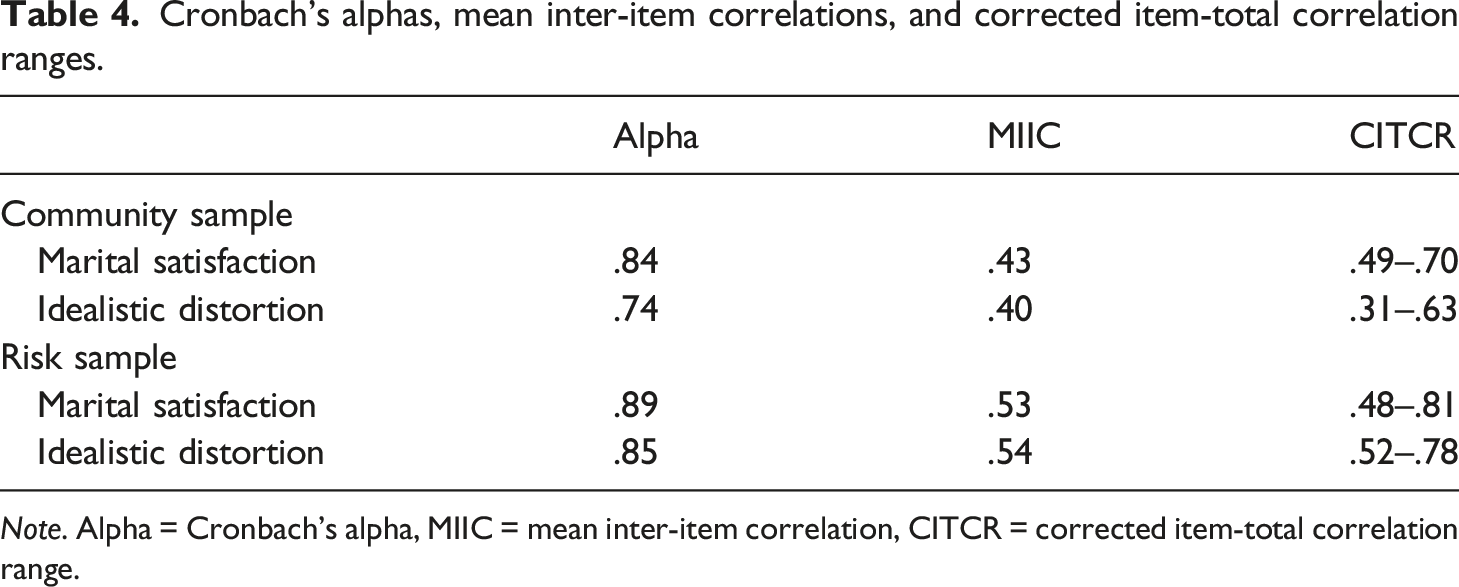
Note. Alpha = Cronbach’s alpha, MIIC = mean inter-item correlation, CITCR = corrected item-total correlation range.
Convergent and discriminant validity
EMS convergent and discriminant validity.
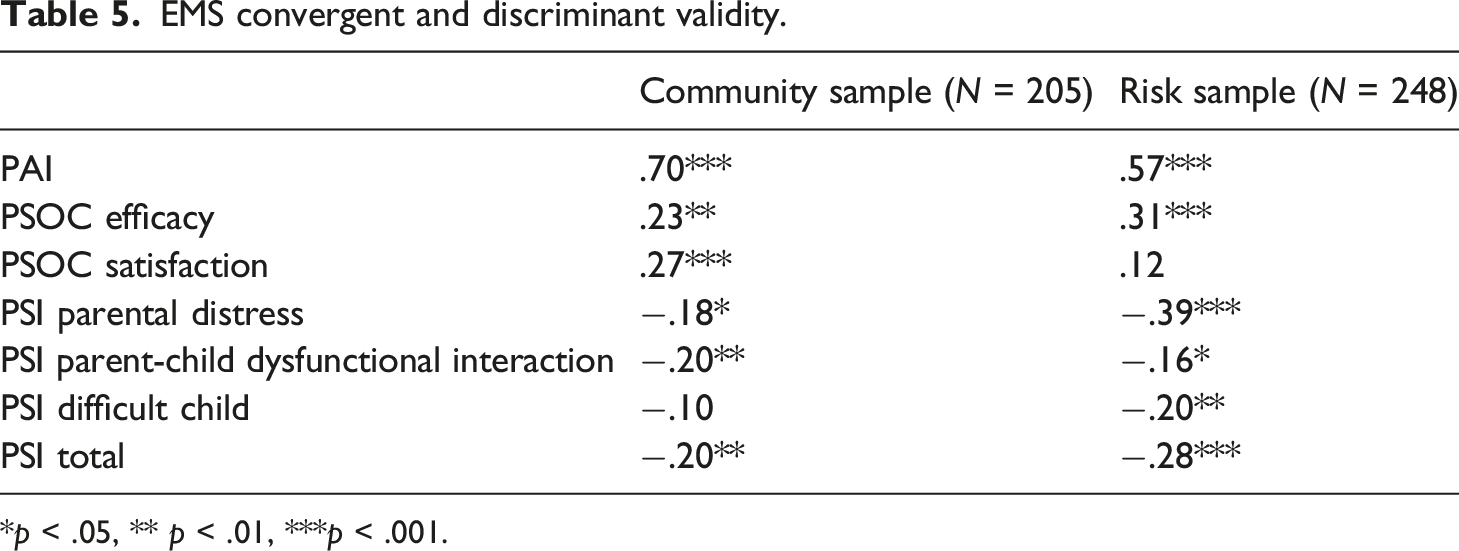
*p < .05, ** p < .01, ***p < .001.
Known groups validity
Comparisons of mothers (n = 309) and fathers (n = 144) in PAI.

Discussion
Marital satisfaction is an important subjective aspect of individual and family well-being, with relevant effects on their functioning (Oosterhouse et al., 2020; Ünal & Akgün, 2020). Therefore, it is important for researchers and professionals to assess this construct with adequate and valid instruments. One of the most used scales for measuring marital satisfaction is the Enrich Marital Satisfaction scale (EMS; Fowers & Olson, 1989, 1993), and its authors developed a 15-items brief version to fill in the extent of some measures developed to assess this construct. Although in the Portuguese setting Marques (2001) had adapted a version of the EMS, it was the longer version, which could limit its usability. Also, in this setting, there is a scarcity of validated instruments assessing marital satisfaction. The present study intended to assess the psychometric properties, particularly the internal factor structure, internal consistency, convergent and discriminant validity of the Portuguese Enrich Marital Scale short form (Fowers & Olson, 1993). In addition, it also aimed to analyse its potential adequacy for couples from the community population and from at-risk one.
Considering the extant literature (e.g., Escrib-Agüir & Artazcoz, 2011; Ferrão et al., 2019; Pandya, 2019), as well as a previous analysis of loading scores and item-total correlations, three different models were tested, namely unifactorial, bifactorial and bifactorial revised. This third model was a result of the bifactorial model previously tested and depended on the goodness of fit indices scores. The model that showed the best fit was the bifactorial revised, composed by 12 items, after a thinning process which led to the elimination of three items. Since we aim to achieve a relevant measurement to marital adjustment and satisfaction assessment, which provides good and valid information regarding these issues, but with the least and best fit items, to answer to practical concerns by researchers and practitioners that intend to develop multivariate studies or evaluations (Fowers & Olson, 1993), the third tested model responded adequately to these needs. The three items eliminated had contents related to dissatisfaction in respect to financial aspects, parent responsibilities and family relations, which can be interpreted as misrepresentations of the construct evaluated or a cultural difference, that is, Portuguese couples may expect and demand more intimacy, commitment and affection from their relationships, than agreement and support, to feel satisfied with their marriage (Feijão & Morais, 2018).
Moreover, all items’ loadings in both samples were above .30, as recommended and the instrument revealed good internal consistency in the two subscales and in both samples. These results showed that the 12-items solution satisfied the basic psychometric requirements, and that the measurement of the marital Idealized Distortion is adequate for this Portuguese short-form version. According to the authors, there are some questions raised about the Idealized Distortion scale (e.g., as the fact of there is no empirical evidence that confirm the relation between these items and the assessment of distortion on marital satisfaction), but the correction provided can play an important role in marital satisfaction adjustment and this feature is one of a kind in this type of instrument (Fowers & Olson, 1993).
The measurement of cross-samples invariance supports the assumption that the same underlying construct is being measured across groups. Also, the corrected item-total correlation range showed satisfactory values in both samples (i.e., at-risk and community samples), and the mean inter-item correlations were slightly above the recommended .50 in the at-risk sample, but above .40 in the community sample. These results show the discriminant power and internal consistency reliability of this measure, revealing that EMS can constitute an important instrument for marital satisfaction assessment, in at-risk and community couples. This is an important achievement, since marital satisfaction can constitute a relevant variable for understanding family functioning, as, for example, marriage can affect and be affected by the exercise of the parenting role, in regard to intimacy (e.g., Twenge et al., 2003) or potential stressful situations (e.g., Kwan et al., 2015). Furthermore, some factors like unemployment, low income or illness situations can affect marital satisfaction (Mosmann et al., 2006), making it relevant to assess it in at-risk communities.
Aligned with our expectations, positive correlations were found between the EMS, the Parental Alliance Inventory (PAI) and the Parenting Sense of Competence (PSOC), namely with the efficacy and satisfaction dimensions; and negative relations were observed between EMS and Parenting Stress Index (PSI) total score and subscales (i.e., Parental distress, Parent-Child Dysfunctional Interaction and Difficult Child). When couples are satisfied with their marriage, they tend to have higher levels of parental alliance (i.e., how parents appreciate, respect and value their co-parents’parenting and opinions; Abidin & Brunner, 1995), characterized by good communication, cooperation and conflict management, which are key ingredients for good parenting (Ayala-Nunes et al., 2014). Therefore, couples with higher marital satisfaction tend to present more parental sensibility (Cummings & Davies, 2010), more satisfaction with the parenting role and evaluate themselves as more competent parents (Hou et al., 2019) and report higher levels of closeness in parent-child relationships (Christopher et al., 2015). Conversely, couples’ dissatisfaction can lead to less stress when performing their parent role (Robinson & Neece, 2015).
Regarding samples specificities, the community sample had higher scores in PAI, PSOC satisfaction and in the PSI Parent-child dysfunctional interaction, whereas the PSOC efficacy, PSI total, Parental distress and Difficult child had a higher magnitude in the at-risk sample. The group validity analysis revealed significant differences between the samples, with higher means in the at-risk sample, but a small effect size. Studies have pointed out that, compared to parents from community population, in at psychosocial risk contexts, parental sense of competence can be different (Nunes & Ayala-Nunes, 2017), and at-risk parents can perceive more stress and be more dissatisfied in performing their role, but cumulatively have a distorted self-evaluation and assess themselves as more competent. These can be due to the fact that when in very stressful environments, parents tend to consider daily situations in an automatic and plain way, have fewer self-correction systems (Nunes et al., 2021b) and minimize the barriers and constrains faced. Although they activate these strategies, the stress experienced can cause strong effects on socioemotional and behaviour features in the children (Konishi et al., 2018), and therefore the child can be perceived as difficult.
Another aspect we explored were the differences between mothers and fathers of both samples. Results showed only significant differences in the at-risk sample, with fathers reporting higher marital satisfaction, although of low magnitude. These findings are congruent with other studies that also reported that women tend to have lower levels of marital satisfaction than men (Jackson et al., 2014; Shen, 2001). However, this is not a solid finding, since several researchers have found the opposite (Belsky et al., 1991; deMontigny et al., 2013; Kim, 2010; Liu & Wang, 2015), and in this work the differences found did not show a high effect size. Research has shown that couples who are not satisfied with their relation can see their family roles affected, because there can be a bidirectional relationship between family components and individual features (e.g., Christopher et al., 2015; Knopp et al., 2017). Kim (2010) showed in Korean couples that the type of family (e.g., remarried), boundary ambiguities and role conflict can show significant impact on married couples’ marital satisfaction. Another explanation for men reporting higher marital satisfaction than women can be that women are more family’ focused and have higher expectations, which can be reflected in lower evaluations, although, in the case of at-risk sample, these evaluations can be unrealistic. Thus, it is important for instruments to be sensitive for these sex differences, and EMS can constitute a relevant tool for parents’ assessment, namely in the Portuguese context.
Although our aim was achieved, some limitations must be pointed out: we did not develop a very exhaustive study in respect to validation aspects, such as temporal stability. Also, the samples were split depending on their origin (community sample vs. at-risk sample) and no other assessment was made to identify specificities (e.g., years of marriage, type of marriage, existence of previous breaks, household, specific problems with children), that may have impact on marital satisfaction and can allow for a more comprehensive view of this complex phenomenon. So, we suggest that future research take these considerations into account, make an extent diagnosis of potential risks in both samples, and develops more comprehensive psychometric and validity studies, allowing researchers and professionals in their interventions with families.
Implications for practice
As mentioned, the EMS can be a useful, reliable and valid tool for Child Welfare Services and for practitioners working with families and/or parents. When designing and implementing their evaluation and/or intervention plans, practitioners engage in a complex process that involves decisions in respect to instruments and their length. This EMS version can allow researchers to reduce the length of their evaluation’s protocols. More extended instruments can yield more information, but brief versions can bring relevant inputs with less effort for participants. Another added value of this EMS refers to this construct itself: frequently, couples assess themselves in a very positive and exacerbated way, so not only it is important to assess marital satisfaction, but also to count on a correction subscale, which can help practitioners to understand couples functioning in a more adjusted light. Thus, incorporating marital satisfaction a when developing a child-centred intervention, can support decision-making process, because families must be viewed as a unit, with vulnerabilities, strengths, and specificities. Another practical implication is its usefulness to integrate indicators for diagnosis, monitoring and impact assessment of community-intervention programs, that can constitute a truly challenge for professionals and researchers.
Marital satisfaction is a central construct for individual well-being and for the entire family system functioning, thus requiring adapted and valid measures to assess it. The EMS brief-form can be presented as so: an accessible, rapid, and effective tool for the evaluation of marital satisfaction, useful for researchers and professionals alike.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by national funds through FCT - Fundação para a Ciência e a Tecnologia - as part the project CIP - Refa UID/PSI/04345/2020
Ethics
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or ethical standards. This project was approved by the Scientific Council of the Psychology and Educational Sciences Department of University of Algarve, Reference No.55/20/12/2017.
Informed consent statement
Written informed consent was obtained from all subjects involved in the study.
Data availability
Data can be available to consultation when request to the corresponding author.
Open research statement
As part of IARR’s encouragement of open research practices, the authors have provided the following information: This research was not pre-registered. The data used in the research are available. The data can be obtained by emailing: