
Abstract
The economic, social, and health impacts of the COVID-19 pandemic are expected to increase the occurrence of intimate partner violence (IPV) victimization. IPV victimization may, in turn, contribute to physical and mental health, substance use, and social distancing behaviors during the COVID-19 pandemic. The primary objective of the current study was to understand the extent to which 1) COVID-19 stressors are associated with IPV victimization and 2) IPV victimization is associated with health and health behaviors. Participants (N = 1,813) completed an online survey between May 15 and 28, 2020 that assessed COVID-19 stressors (financial anxiety, social disconnection, health anxiety, COVID-19-specific stress), IPV victimization, physical and mental health, substance use, and movement outside of the home. Structural equation modeling indicated that greater COVID-19-related stressors were associated with greater IPV victimization during the pandemic, even after controlling for enduring vulnerabilities associated with IPV victimization. Additionally, greater IPV victimization during the COVID-19 pandemic was associated with higher levels of substance use and movement outside of the home, but not poorer physical and mental health. COVID-19 stressors may have detrimental relationship effects and health implications, underscoring the need for increased IPV intervention and support services during the pandemic. Findings from the current work provide preliminary correlational evidence for a theoretical model centered on IPV victimization, rather than perpetration.
Introduction
Intimate partner violence (IPV) is defined as physical, sexual, or psychological harm, or the threat of such harm, within a romantic relationship. It is recognized by the Centers for Disease Control and Prevention as a serious public health issue with lifetime prevalence rates of over 35% for women and 28% for men (Black et al., 2011). Although some models of IPV, such as the Duluth Model, propose that IPV stems from perpetrators’ desire for power and control over their partners (Pence et al., 1993), other models of violence and aggression underscore the important role of situational factors (e.g., conflict, life stress) in predicting violent interactions (Finkel & Eckhardt, 2013; Riggs & O’Leary, 1996). For example, the I3 model posits several interrelated processes that can lead to aggressive behavior; namely, that certain situational and dispositional qualities are likely to foster aggression (Finkel & Eckhardt, 2013).
Preliminary evidence documents IPV as a persisting and escalating problem during the COVID-19 pandemic (Jetelina et al., 2020; Matoori et al., 2020) with early police reports of several major U.S. cities revealing increased incidents of IPV relative to 2019 (Boserup et al., 2020). This increase in IPV victimization during the pandemic may be due to the increase of situational stressors related to the COVID-19 pandemic, such as economic stress, social isolation, and pandemic-related stress (Peterman et al., 2020; Van Gelder et al., 2020). In line with theories of aggression, situational stressors associated with the pandemic may explain why perpetrators may be more likely to aggress during the pandemic. Additionally, these stressors are likely shared by both victims and perpetrators and, thus, should also predict greater IPV victimization, not merely perpetration.
Pietromonaco and Overall’s (2020) adapted vulnerability-stress-adaptation model provides a framework to understand how COVID-19 stressors may contribute to IPV victimization. The model illustrates how COVID-19 stressors, along with pre-existing vulnerabilities (e.g., lower socioeconomic status, attachment insecurity), should affect relationship processes, quality, and stability during and after the pandemic. Specifically, Pietromonaco and Overall (2020) note that external stress (e.g., situational stressors resulting from the pandemic) may cause disturbances in the way partners interact, leading to disrupted adaptive relationship processes and resulting in more maladaptive processes, such as greater negativity and hostility.
By integrating models of IPV and relationship functioning during COVID-19, we can better understand how COVID-19 stressors may lead to increased IPV victimization during the pandemic. Stressors such as economic hardship and social isolation have previously been associated with IPV in general (Fox & Benson, 2006; Lanier & Maume, 2009; Miles-Doan, 1998; Smith & Weatherburn, 2013; Van Wyk et al., 2003), and the widespread increase of these stressors during the COVID-19 pandemic in addition to pre-existing vulnerabilities may function to increase IPV victimization. Specifically, stressors such as financial stress and social disconnection may minimize victims’ abilities to seek support and leverage resources that yield positive alternatives to an abusive relationship (Finkel & Hall, 2018). Pandemic-related health anxieties may increase tendencies to stay indoors, increasing proximity to abusive partners and the likelihood of victimization.
Not only are COVID-19-related stressors likely to increase IPV victimization, but IPV victimization may, in turn, contribute to negative health-related outcomes such as poorer physical and mental health and increased substance use behavior. Even when no overt violence is occurring, victims of IPV have described the experience of abuse as a chronic stressor of real or perceived threat (Smith et al., 1995). The chronic stress of IPV victimization has implications for physiological dysregulation (Yim & Kofman, 2019), which can contribute to a multitude of downstream negative mental and physical health outcomes often associated with IPV (Breiding et al., 2008; Campbell, 2002; Coker et al., 2002; McCauley et al., 1995; Wuest et al., 2008). The stress associated with experiencing IPV victimization during COVID-19 may also prompt individuals to turn to substance use as a coping mechanism. Problem alcohol use, for example, is often cited as a consequence of IPV-related stress, used by victims as a means to cope or self-medicate (Øverup et al., 2015). The use of alcohol and other substances by IPV victims is particularly important to consider during the COVID-19 pandemic given that typical intervention and support modalities may operate at reduced capacities, limiting external resources to which victims can turn.
IPV may also be associated with health behaviors related to COVID-19 such as social distancing behaviors that impact the likelihood of infection and the spread of the virus. One component of social distancing that could be particularly relevant to examine in relation to IPV is movement outside of the home, defined here as the frequency with which individuals leave their home to visit others or a public space. To our knowledge, no work has examined how IPV is associated with movement outside of the home. Two potential relationships are possible. IPV victimization could lead to less movement outside of the home (i.e., greater social distancing behaviors), perhaps if victims choose to stay home in order to minimize the risk of perpetrators feeling rejected and aggressing (Finkel & Hall, 2018; Pence et al., 1993). Alternatively, IPV victimization could lead to greater movement outside of the home (i.e., less social distancing behaviors) if victims feel the need to escape the home to increase their personal safety and reduce stress (Riggs & O’Leary, 1996). Determining whether IPV victims are differentially engaging in social distancing behaviors may be particularly important to consider during the COVID-19 pandemic if victimization is related to behaviors that increase victims’ risk for COVID-19 infection if other safety guidelines are not followed.
Current study
The primary objective of the current study was to integrate theories of relationship functioning during COVID-19 with those of intimate partner violence in order to understand the extent to which 1) COVID-19 stressors are associated with IPV victimization during the COVID-19 pandemic and 2) IPV victimization during the pandemic is associated with health and health behaviors. The central hypothesis was that greater COVID-19 stressors (e.g., financial anxiety, social disconnectedness, health anxiety) would be associated with greater IPV victimization during the pandemic, and greater IPV victimization would be associated with worse physical and mental health and greater substance use. We explored the extent to which IPV victimization was related to movement outside of the home. Given that it is plausible for IPV to be associated with either an increase or a decrease in movement outside the home, no directional hypothesis for this relationship was proposed.
Finally, individual factors which have been shown to increase vulnerability for IPV victimization (e.g., Widom et al., 2014) and are theorized to disrupt relationships (Overall et al., in press; Pietromonaco & Overall, 2020) were accounted for to examine the unique associations between COVID-19 stressors, IPV victimization, health, and health behaviors. Specifically, we assessed attachment insecurity, adverse childhood experiences, and (lower) pre-COVID-19 socioeconomic status (SES). Individuals high on attachment anxiety (i.e., preoccupation with relationship partners, excessive need for approval) can find it difficult to leave abusive relationships due to their fears of abandonment and negative views of self (Velotti et al., 2018). Individuals high on attachment avoidance (i.e., discomfort with emotional closeness, chronic self-reliance, distrust of others) are unlikely to seek help when in abusive relationships and may falsely perceive themselves to be immune to the psychological abuse of another (Velotti et al., 2018). Exposure to adverse childhood experiences that involve a history of family abuse and dysfunction is thought to increase the risk of IPV victimization in adulthood as individuals internalize the acceptability of abuse through social learning (Stith et al., 2000; Widom et al., 2014). Finally, we accounted for SES prior to COVID-19, as lower socioeconomic factors including lower levels of education and income are known to increase risk of IPV victimization (Cunradi et al., 2002; Sorenson et al., 1996; Spencer et al., 2019).
Method
Participants and power
Participants were recruited through ResearchMatch, a national health volunteer registry supported by the U.S. National Institutes of Health, to complete an online survey. In order to participate, individuals were required to be in a romantic relationship of at least 4 months and currently cohabitating with their partner. A total of 1,869 participants consented and completed the survey; however, 56 (2.90%) participants failed one or both attention check items (Maniaci & Rogge, 2014), leaving a final sample size of 1,813. Participants were predominately female (79.70%) and white (88.40%) with an average age of 44.60 (SD = 16.04, 19–89). Most participants were married (1,251, 69.00%) and with their partner for an average of 16.13 years (SD = 14.16, 5 months–68 years). Complete descriptive statistics for the sample characteristics are presented in Table 1. Power was estimated at 1.0 for the overall model using MacCallum et al.’s (1996) method for detecting the difference between a good fitting model (Root Mean Square Error of Approximation [RMSEA] ≤ .05) and a poor fitting model (RMSEA ≥ .08).
Descriptive statistics of sample characteristics.
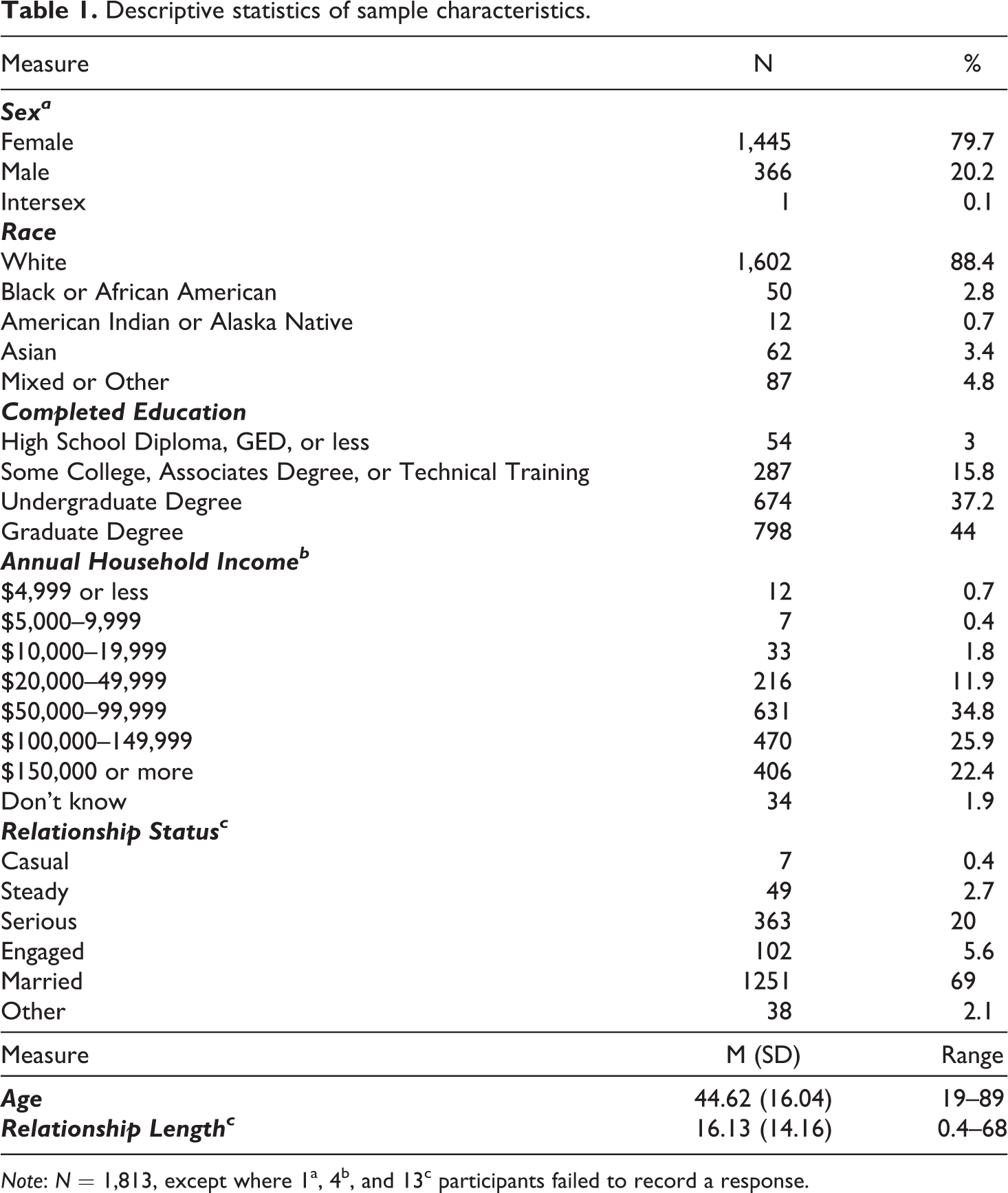
Note: N = 1,813, except where 1a, 4b, and 13c participants failed to record a response.
Procedure
All study procedures were approved by the Ohio University institutional review board and informed consent was obtained from all individuals prior to administering the survey. Data was collected using a secure, online survey platform between May 15 and 28, 2020, a time when shelter-in-place orders were being loosened in nearly all 50 states. This provided an opportune time for individuals to reflect on their shelter-in-place experience during the initial response to the COVID-19 pandemic in the U.S. Due to the sensitive nature of the study questions, safety and ethical guidelines for protecting potential victims of IPV were incorporated (Ellsberg & Heise, 2005). Specifically, participants were continually asked to confirm that they were in a safe, private location, provided a link on each survey screen to immediately exit the survey (if necessary), and given information about national IPV resources before and after the survey.
Measures
Unless otherwise stated, items were averaged to form composites. Full versions of all scales are presented in the electronic supplementary materials (ESM). Descriptive and reliability statistics for the primary study variables (listed below) are presented in Table 2.
Descriptive and reliability statistics for study variables.
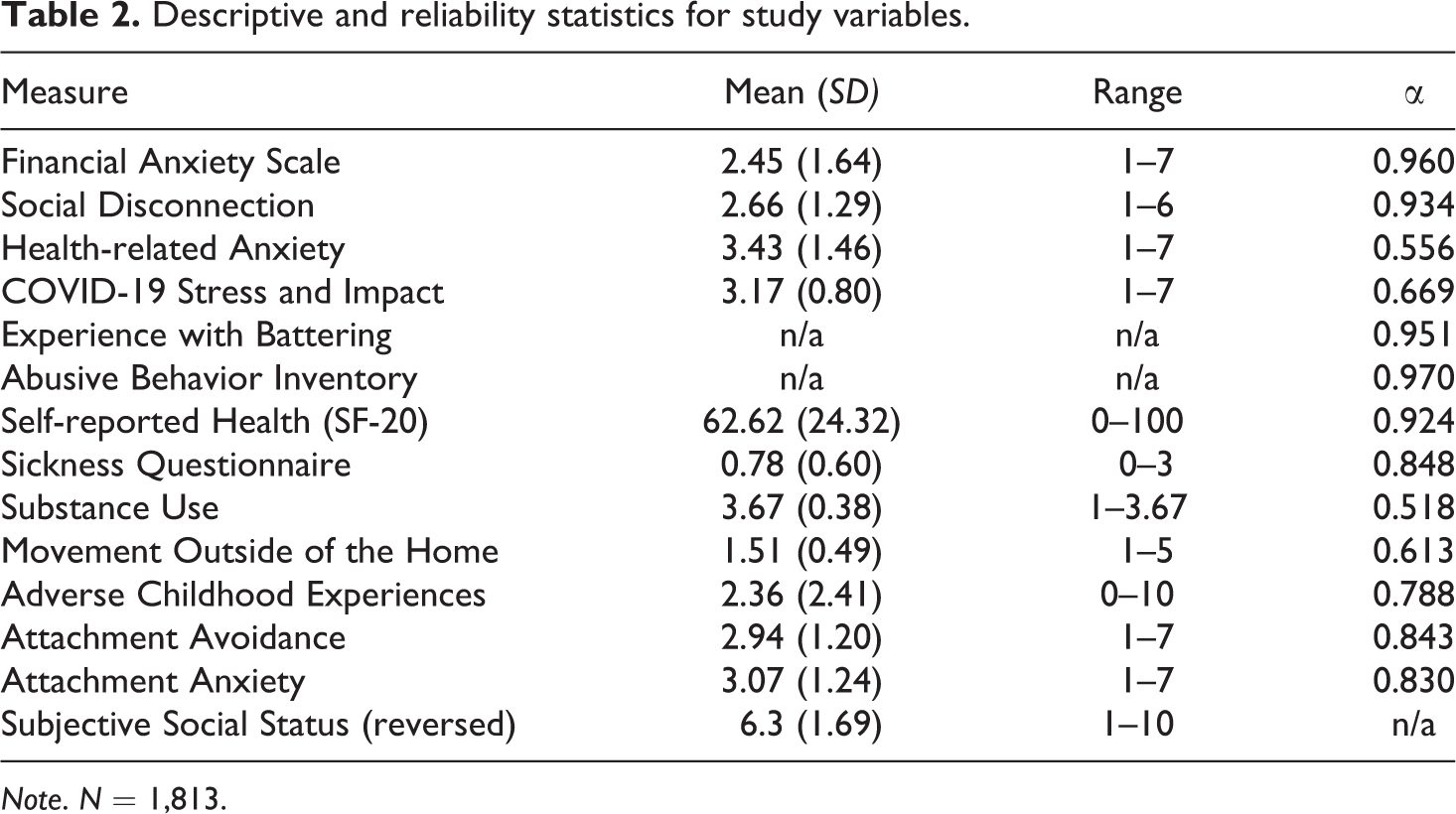
Note. N = 1,813.
COVID-19 stressors
Four scale composites indexed COVID-19-related stressors. Financial anxiety. An adapted version of the 7-item Financial Anxiety Scale (Archuleta et al., 2013) asked participants to report their feelings of anxiety about their financial situation during the COVID-19 pandemic. Higher scores were indicative of greater financial anxiety. Social disconnection. The 8-item Social Connectedness Scale (Lee & Robbins, 1995) assessed participants’ feelings of social disconnection, with higher scores indicating greater disconnection. Health anxiety. Three items adapted from the Health Anxiety Inventory (Salkovskis et al., 2002) assessed feelings of fear, worry, and the tendency to ruminate about COVID-19; higher scores indicated greater health anxiety. Perceived stress and impact. Two face-valid items from the Pandemic Stress Index (Harkness et al., 2020) assessed how much participants felt that COVID-19 impacted their life and how stressed they were about COVID-19; higher scores indicated greater feelings of stress and impact.
Intimate partner violence victimization
Participants completed two measures of IPV victimization during the COVID-19 pandemic, both of which were adapted with language that applied to all genders and sexual orientations. Experience with Battering. The Experience with Battering (Smith et al., 1995) scale includes 10 items measuring experiences as a victim of IPV by asking about the presence of battering without specification of behavioral incidents. These items were summed such that higher scores on this measure indicated more experience with battering. Experience of Abuse. The 29-item Abusive Behavior Inventory (Shepard & Campbell, 1992) assessed behavioral manifestations of IPV that individuals might have experienced as victims. These items were summed such that higher scores on this measure indicated more experience of abuse. Using both measures allowed us to identify IPV victims based on the subjective experience of IPV along with its discrete behavioral components. Standard cutoffs (Smith et al., 1995; Zink et al., 2007) were used to dichotomize each scale, with participants whose summed scores were higher than 19 on the Experience with Battering measure and 39 on the Abusive Behavior Inventory being considered as battered (N = 151, 8.3%) or abused (N = 179, 9.9%), respectively.
Physical and mental health
Two scale composites indexed physical and mental health during the COVID-19 pandemic. General health. The Short-Form 20-item Health Survey (Ware et al., 1992) assessed self-reported general health during the pandemic. For analyses, scores were multiplied by −1, with higher scores indicating worse general health. Sickness behavior. The 10-item Sickness Behavior Questionnaire (Andreasson et al., 2018) assessed individuals’ momentary symptoms of inflammatory activation, with higher scores indicating more sickness behavior.
Substance use
Six face-valid items assessed the degree to which individuals reported using drugs or alcohol during the COVID-19 pandemic. Higher scores indicated greater substance use during the pandemic.
Movement outside of the home
Six face-valid items assessed the degree to which individuals left their home to visit close others or go to public spaces within the past week. Higher scores indicated greater frequency of leaving the home during the past week.
Vulnerabilities
Four scale composites assessed vulnerabilities for IPV victimization. Adverse childhood experiences. Childhood relationship experiences during the first 18 years of life were indexed by the Adverse Childhood Experiences questionnaire (Felitti et al., 1998). Endorsements of these experiences were summed, with higher scores indicating more adverse childhood experiences. Attachment avoidance and anxiety. The Adult Attachment Questionnaire (Simpson et al., 1996) indexed how individuals relate to their romantic partners to assess attachment avoidance and anxiety. Higher scores on each sub-scale indicated greater attachment avoidance or attachment anxiety. Subjective SES. An adapted version of The MacArthur Subjective Social Status Scale (Adler et al., 2000) was used in which individuals mark 1 of 10 rungs on a ladder that best described their perceived standing relative to others in the U.S. prior to the COVID-19 pandemic. Scores were reversed, with higher scores indicating lower perceived SES.
Results
Zero-order correlations between study variables are depicted in Table 3. To test predictions, a Structural Equation Model (SEM, see Figure 1) was developed in which the two independent variables—COVID-19 stressors and vulnerabilities—were modeled as latent variables. COVID-19 stressors included the indicator (i.e., observed) variables: financial anxiety, social disconnection, health anxiety, and perceived stress and impact. Vulnerabilities included the following indicators: adverse childhood experiences, attachment avoidance, attachment anxiety, and subjective SES. IPV victimization was modeled as a latent variable with two indicators: experiences with battering and experience of abuse. Physical and mental health was modeled as a single latent variable consisting of general health and sickness behavior. Substance use and movement outside the home were both modeled as single observed variables.
Zero-order correlations among primary study variables.
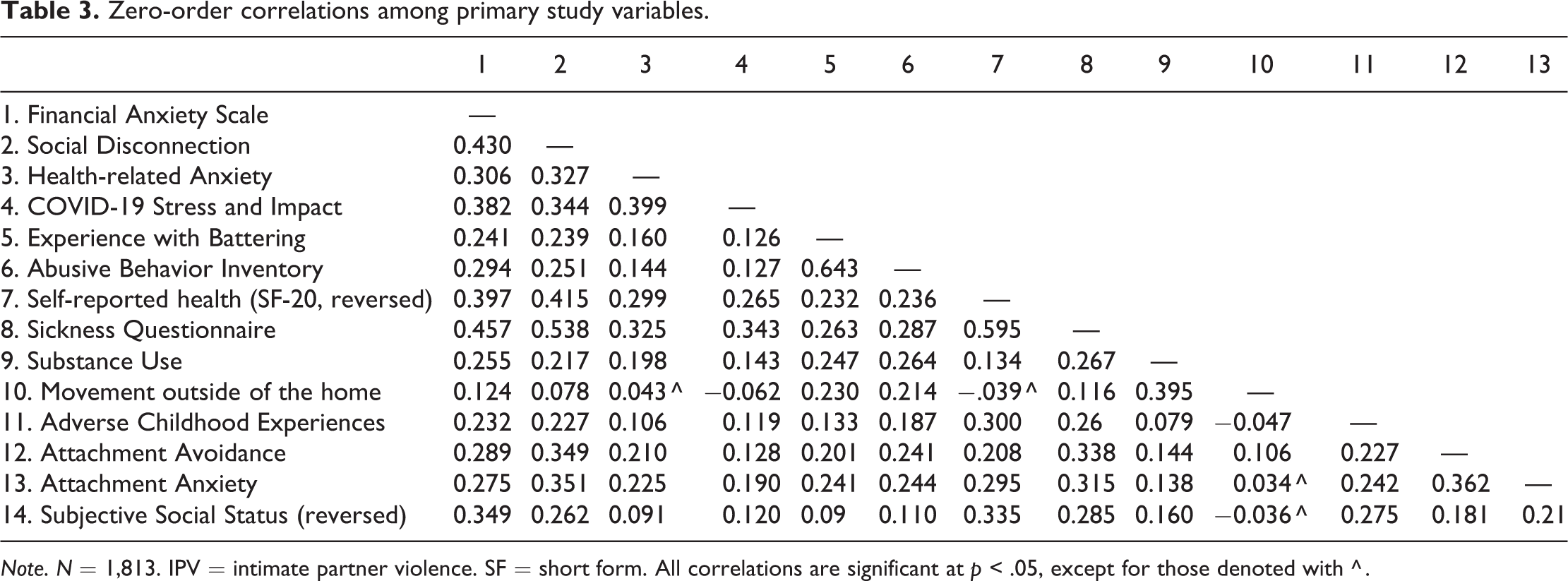
Note. N = 1,813. IPV = intimate partner violence. SF = short form. All correlations are significant at p < .05, except for those denoted with ^ .
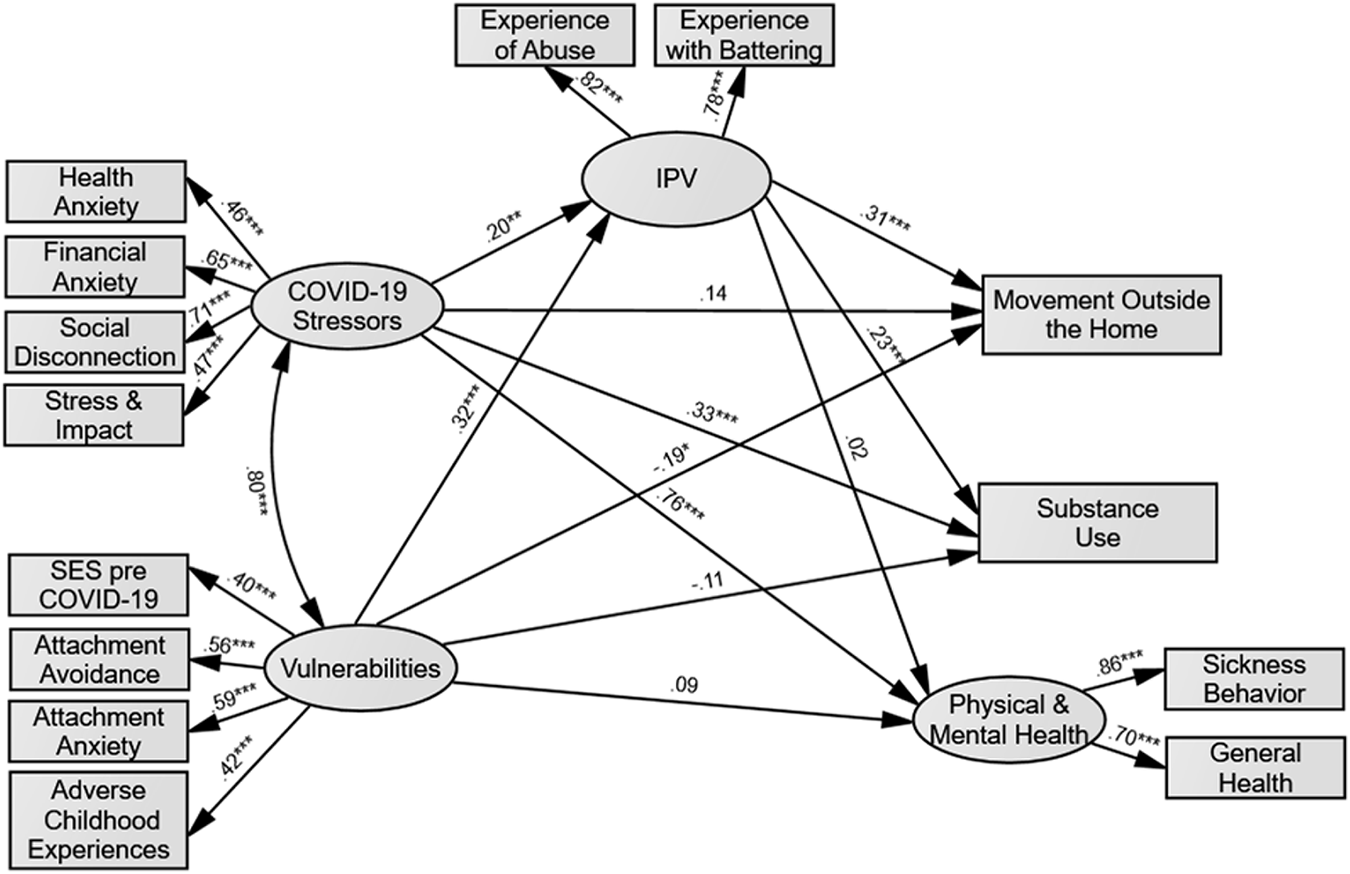
Structural equation model with standardized path coefficients. Note. Error covariances between indicators are not displayed for ease of interpretation. *p < .05; **p < .01; ***p < .001.
As shown in Figure 1, the direct paths were freely estimated connecting COVID-19 stressors and vulnerabilities with IPV as well as the three health-related outcome variables. The direct paths between IPV and the three outcome variables were also freely estimated. Finally, because models of IPV and vulnerability-stress acknowledge that stressors and vulnerabilities are associated, the association between these latent constructs was estimated. Maximum Likelihood Estimation was used to estimate the proposed model, and model evaluation was based on Hu and Bentler’s (1999) combination approach, with the Comparative Fit Index (CFI) and Tucker Lewis Index (TLI) ≥ .95 and the Root Mean Square Error of Approximation (RMSEA) and Standardized Root Mean Residual (SRMR) ≤ .06 judged to indicate a very good fit.
Given that the model consisted of several latent constructs comprised of several indicators, we first estimated a full measurement model (Confirmatory Factor Analysis [CFA]) in order to determine the goodness of fit of the derived latent constructs. This approach is consistent with the two-step approach to model building (Anderson & Gerbing, 1988). The CFA demonstrated very good to excellent fit: χ2(45) = 268.54, p < .05; CFI = .96; TLI = .94; RMSEA = .05; SRMR = .03.
The full SEM demonstrated good fit to the data, χ 2 (62) = 398.04, p < .001; CFI = .95; TLI = .92; RMSEA = .06; SRMR = .04. 1,2 As shown in Figure 1, greater COVID-19 stressors and vulnerabilities were associated with greater IPV victimization during the COVID-19 pandemic. Greater COVID-19 stressors were also associated with greater substance use and poorer physical and mental health but were not significantly associated with movement outside the home. Greater vulnerabilities were associated with less movement outside the home, but no significant associations were found with substance use or physical and mental health. Finally, greater IPV victimization during the pandemic was associated with greater movement outside of the home and substance use, but no significant association was found with physical and mental health.
To test whether IPV victimization mediated the associations between COVID-19 stressors and vulnerabilities and health and health behaviors, specific indirect effects were estimated by bootstrapping the sample to 5,000 replications and estimating the 95% bias-corrected confidence intervals (MacKinnon, 2008). As presented in Table 4, IPV victimization had an indirect effect on the associations between COVID-19 stressors and vulnerabilities and health behavior variables (substance use and movement outside of the home), but not on physical and mental health. Due to the correlational nature of these data, mediational analyses should be interpreted with caution.
Specific indirect effects.
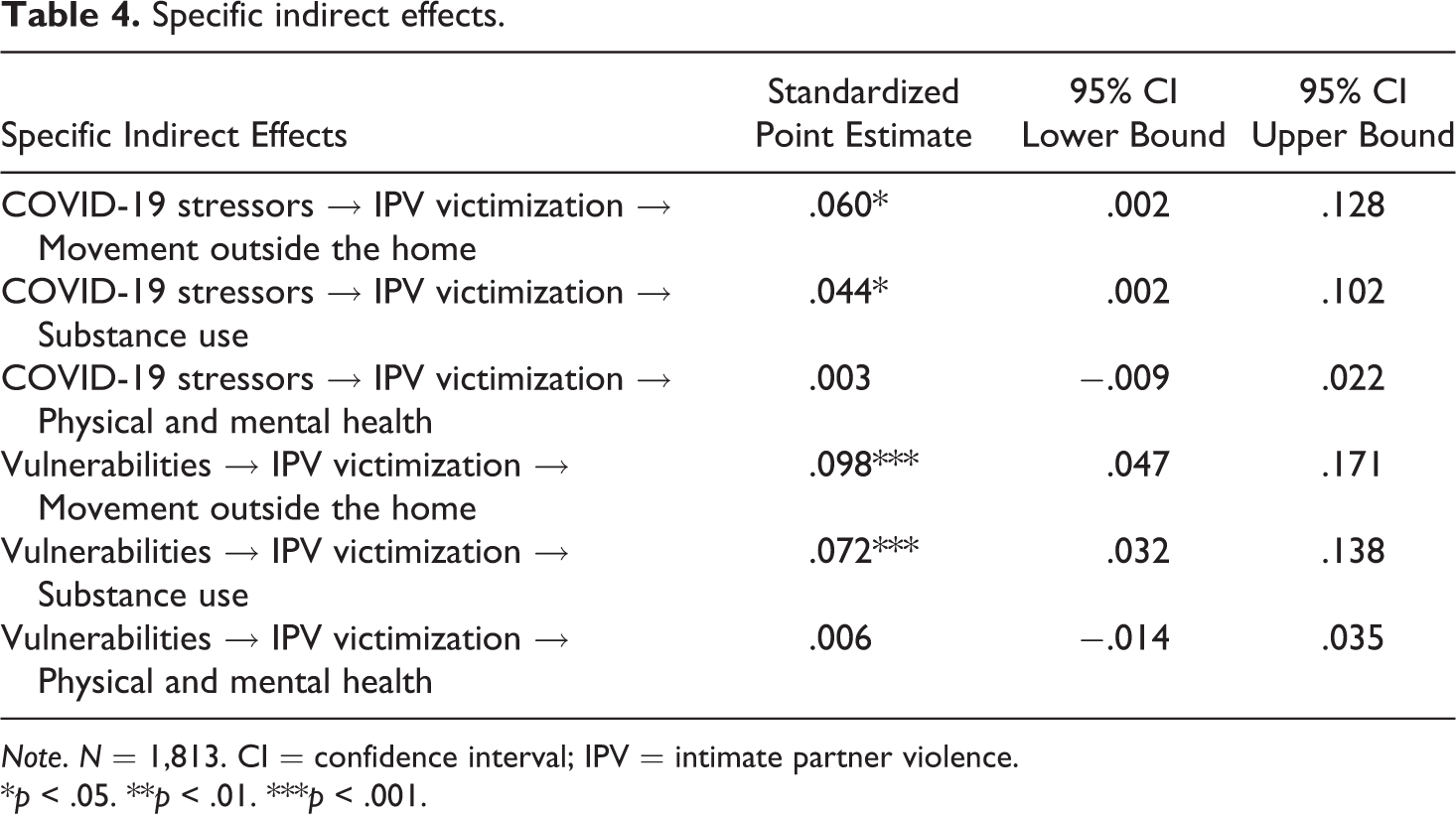
Note. N = 1,813. CI = confidence interval; IPV = intimate partner violence.
*p < .05. **p < .01. ***p < .001.
Discussion
The current research highlights the importance of examining IPV during the COVID-19 pandemic and contributes to existing models of IPV and relationship functioning. First, we found that COVID-19-related stressors were associated with greater IPV victimization during the pandemic, even after controlling for enduring vulnerabilities associated with IPV victimization. This finding is consistent with the adapted vulnerability-stress-adaptation model (Pietromonaco & Overall, 2020) and supports models of aggression and partner violence (e.g., the I3 model), which suggest that situational stressors are risk factors for IPV perpetration (Finkel & Hall, 2018). Further, our findings extend models such as Dutton’s (1995) nested ecological theory of partner violence (see also: Spencer et al., 2019) by demonstrating how situational stressors (i.e., exosystem-level factors) are related to IPV victimization, even after controlling for individual-level (i.e., ontogenetic-level) factors. This finding also reinforces the position that ongoing and future crisis response systems should recognize IPV as a potential consequence of stressful conditions and prioritize prevention and intervention efforts within response plans. Moreover, these findings suggest that addressing the stressful context surrounding victims, such as adopting policies that reduce financial strain or implementing virtual support programs, may help reduce IPV victimization during the pandemic.
Second, the results revealed that greater IPV victimization during the COVID-19 pandemic was associated with higher levels of substance use and movement outside of the home, but not worse physical or mental health. The positive association between IPV victimization and substance use may reflect attempts to reduce the stress of victimization, consistent with self-medication models of IPV and substance use (Øverup et al., 2015). Although the underlying motivation for why individuals were leaving the home was not assessed, greater movement outside the home may act as a way for victims to physically distance themselves from their partners, thereby reducing stress and avoiding further abuse.
While these health behaviors may facilitate stress reduction for victims in the short-term, they may have important longer-term consequences for both individual and community health. Substance use is related to greater risk for negative health outcomes over time (Schulte & Hser, 2014), and thus IPV victims who engage in substance use behavior may eventually experience worse health outcomes. Frequent movement outside the home is particularly relevant during the COVID-19 pandemic, as social distancing behaviors are one key mechanism to reduce the spread of the virus. More movement outside the home could potentially put IPV victims at greater risk of contracting the virus, especially considering some evidence that suggests IPV victims may already be at an increased risk for infection due to the effects of chronic stress on the immune system (Garcia-Linares et al., 2004; Yim & Kofman, 2019). More movement outside of the home may also facilitate greater community spread if other social distancing guidelines, such as keeping 6 feet between oneself and others and wearing a mask, are not followed.
We did not find support for our hypothesis that greater IPV victimization would be associated with worse physical and mental health. We propose two potential explanations for this outcome. First, the association between COVID-19 stressors and physical and mental health was strong, leaving little remaining variance for IPV to predict. Second, given the evidence that has accumulated showing that IPV victimization is linked to worse health outcomes (Breiding et al., 2008; Campbell, 2002; Coker et al., 2002; McCauley et al., 1995; Wuest et al., 2008; Yim & Kofman, 2019), we caution readers from concluding that IPV victimization is unrelated to health. Instead, the lack of association between IPV victimization and health could be attributable to the cross-sectional nature of our data. Although few studies have evaluated the relationship between IPV victimization and health prospectively, it is possible that health effects associated with IPV victimization develop over time by continuing to influence stress-related biological processes (Yim & Kofman, 2019). Gerber and colleagues (2008), for example, found that physical symptoms of people experiencing IPV increased over time. Thus, worse health among IPV victims may not be apparent in our cross-sectional analyses, but could develop over the course of the pandemic and beyond.
Although the large sample size and thorough assessment of constructs are notable strengths, there are inevitable limitations and caveats. The data were cross-sectional, which limits the ability to make causal conclusions. As one example, poorer mental and physical health prior to the COVID-19 pandemic may have contributed to greater COVID-19 stressors. The worsening of COVID-19 in the U.S. may result in increased pandemic-related stress over time and, therefore, even greater IPV victimization and worse health outcomes for victims. The cross-sectional nature of our data limits our ability to understand whether and how these relations may have changed across the course of the pandemic. Despite the limitation of cross-sectional data, these results provide an important snapshot of these associations early in the pandemic. Dyadic data were not obtained (due to privacy and security concerns), which prevented the inclusion of perpetrator and situational features that are known to predict IPV. Even though our hypothesis that IPV victimization should be associated with worse physical and mental health was unsupported, the large association between COVID-19 stressors on mental and physical health underscores the profound association between COVID-19 stressors and the wellbeing of people, even if they do not contract the virus (only 0.4% of participants in this sample reported testing positive for COVID-19).
Despite these limitations, this study has important theoretical and practical implications. By integrating the adapted vulnerability-stress-adaptation model (Pietromonaco & Overall, 2020) with models of aggression and violence (Finkel et al., 2009; Finkel & Eckhardt, 2013; Finkel & Hall, 2018; Riggs & O’Leary, 1996), our findings provide correlational evidence for a new model of IPV victimization rather than perpetration. Although certain stressors have been identified as risk factors for IPV victimization (e.g., financial stress; Smith & Weatherburn, 2013), the models that utilize stressors as predictors of IPV have focused primarily on predicting perpetration. Our findings provide a step toward understanding whether these stressors also contribute to victimization and emphasize the importance of examining external stressors in intimate partner violence research. Our findings also provide evidence that IPV victimization during COVID-19 is linked to potentially harmful substance use behaviors and risky social distancing behaviors. Moreover, our findings linking IPV victimization to greater substance use and more frequent movement outside the home demonstrate ways in which victims of IPV may attempt to buffer stress.
In sum, COVID-19 stressors are likely to have detrimental relationship effects and health implications. Future research should examine these relationships over time and investigate potential factors that moderate the associations between stress, IPV, health, and health behaviors. Our results also underscore the need for increased IPV intervention and support services during the pandemic. These services would not only benefit individual health and wellbeing (e.g., decreasing substance use, the risk of COVID-19 infection, and stress and the potential injury from acts of violence), but may also help curtail the spread of the virus by reducing the need to leave home and come into contact with other people.
Supplemental material
Supplemental Material, sj-pdf-1-spr-10.1177_02654075211012098 - Examining associations between COVID-19 stressors, intimate partner violence, health, and health behaviors
Supplemental Material, sj-pdf-1-spr-10.1177_02654075211012098 for Examining associations between COVID-19 stressors, intimate partner violence, health, and health behaviors by Abriana M. Gresham, Brett J. Peters, Gery Karantzas, Linda D. Cameron and Jeffry A. Simpson in Journal of Social and Personal Relationships
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Open research statement
As part of IARR’s encouragement of open research practices, the author(s) have provided the following information: This research was not pre-registered. The data used in the research are available. The data can be obtained by e-mailing
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.