
Abstract
To support vision rehabilitation workers, an intervention guideline for the rehabilitation of children with cerebral visual impairment (CVI) was developed. It combines currently available theoretical and practice-based knowledge in the domains of academic performance and mobility. The aim of this study was to evaluate the perceived value of the guideline by professionals. Two studies were performed. First, a process analysis of the guideline was performed to evaluate its strengths and weaknesses. Eleven therapists used a concept of the guideline for 3 months and were interviewed about their expectations (before) and experiences (afterwards). In a second study, the guideline was introduced to 24 professionals working with school-aged children with CVI. The participants filled in a short survey with five questions about their perceived knowledge of and skills in dealing with CVI. The guideline complied with the expectations of the professionals, and the professionals improved in knowledge of CVI and the ability to explain what CVI is. The survey results indicated improvement in self-confidence to perform CVI-specific interventions, and the interviews also showed professionals had expected to learn more options for intervention. After training, the professionals felt more secure about their interventions while using the guideline. This was probably caused by an improvement in their knowledge about CVI and about available interventions. However, the improvement was small and still not perfect and could be enlarged by adding more concrete intervention suggestions to the guideline. The intervention guideline for CVI offers an overview of available theoretical and practice-based knowledge. Improvement in knowledge on CVI can be used directly in rehabilitation practices. A great advantage of the guideline is that therapists are now better prepared to explain the nature and consequences of CVI to a client.
Keywords
Cerebral visual impairment (CVI) has become the leading cause of significant vision loss in children in developed countries (Bennett et al., 2020; Fazzi et al., 2007; Kran et al., 2019). Despite the prevalence of CVI, interventions for CVI are still in their infancy, regarding both the availability of suitable intervention methods and the quality of these interventions (Delay et al., 2022). To help service providers, an intervention guideline for the habilitation and rehabilitation of children with CVI (developmental age 4–18) was developed (Fonteyn-Vinke et al., 2020). Vision habilitation and rehabilitation workers are trained professionals with various backgrounds like occupational therapy or pedagogy/special needs who have specialized in vision (often called early interventionists); they will be referred to as vision therapists. Rehabilitation, habilitation, (early) intervention, therapy, and treatment will be used interchangeably as they all mean working methodically with a person to reach a higher level of development/independence. The lack of a generally accepted definition for CVI, and subsequently how to diagnose CVI, and the lack of clear advices how to deal with CVI are barriers to the effective habilitation and rehabilitation of CVI (Boonstra et al., 2022; Pilling et al., 2023; Sakki et al., 2018). Goal of the guideline was therefore to bring together the best available knowledge about CVI in an accessible way.
The guideline uses the definition of CVI suggested by Sakki et al. (2018), also used by Boonstra et al. (2022) and mentioned by Pilling et al. (2023). ‘CVI is a verifiable visual dysfunction, which cannot be attributed to disorders of the anterior visual pathways or any potentially co-occurring ocular impairment’. A key aspect of CVI is that it refers to vision dysfunctions that originate from brain injury and disorders of the cerebral visual pathways. The visual dysfunction can be not only in basic visual functions, such as reduced visual acuity, impaired contrast sensitivity, and visual field deficits, but also in visual processing functions, such as visual selective attention (i.e., a mostly subconscious decision where to focus visual attention on within a visual scene, either on details or more globally on the environment), motion perception, visuospatial processing, or object recognition (Bennett et al., 2020; Boonstra et al., 2022; Dale et al., 2022; Dutton & Bauer, 2019; Ortibus et al., 2011; Zuidhoek, 2020).
Symptoms of CVI can be present in varying combinations, resulting in a population of children with CVI that is highly heterogeneous and making one uniform method of intervention impossible (Zuidhoek, 2020). As a result of a range of visual processing problems (Ben Itzhak et al., 2020; Zihl et al., 2023), children with CVI experience difficulties in various life circumstances, developmental domains, and quality of life (Sakki et al., 2021). The two most notable domains where school-aged children with CVI experience problems are learning and academic performance (Dale et al., 2022) and mobility (Chokron & Dutton, 2016; Dutton & Bauer, 2019). In learning and academic performance, it is not only reading that is affected by CVI, as a result of for instance visual crowding effects, but also all learning that includes dealing with charts, figures, drawings, photos, maps, and tables, for which visual analysis, synthesis, and interpretation are necessary. All subjects and tasks for which these visual perceptual skills are necessary are grouped under the term academic performance. Because of their relevance to children’s lives, the two domains, learning and academic performance and mobility, were chosen in the guideline and this study.
To help overcome these problems, interventions are listed in the guideline. These interventions overlap partly with interventions designed to treat children with ocular impairments. For instance, for both groups, perceptual learning can be used to improve acuity. Supportive aids, such as magnification or extra light, as well as compensatory strategies, such as using hearing or touch to compensate for loss of certain visual functions or spatial cues to find objects more easily, can be used. Finally, environmental adaptations can be made, such as using large font sizes or extra spacing between letters in case crowding hinders reading. To date, the use of interventions originally designed for children with ocular impairment but applied to children with CVI lacks empirical evidence that they are effective (Delay et al., 2022). It is even questionable whether they are the treatments of first choice, since Martín et al. (2016) observed that education and (re)habilitation strategies developed for people with ocular vision loss are not always effective for people with CVI. Martín et al. (2016) explained this failure originates from neglecting the different conditions responsible for brain plasticity in ocular and cortical/CVI.
The impact of CVI on children’s daily lives is not always obvious and sometimes hard to understand. In response, enhancing awareness of what it is to live with CVI has been successfully applied in recent years. Simulation programmes, such as ‘CVI Experience’ (Pilon-Kamsteeg et al., 2019) and the ‘CVI in the Picture Experience Kit’ (in Dutch), which were compiled to be used alongside the book ‘ CVI in the Picture’ (Zuidhoek, 2020), were developed to teach professionals and parents what it means to live with higher-order visual dysfunctions. In the authors’ clinical experience, by raising awareness about the daily consequences of CVI, vision therapists become inspired and motivated to create tailor-made interventions. Yet, there is still a great deal of uncertainty as to which techniques should be applied in (re)habilitation, as few evidence-based interventions are available. At best, vision therapists must rely on their own experiences, creativity, and flexibility.
To guide these professionals, the best available evidence for interventions were collected by ophthalmologists, orthoptists, psychologists, vision therapists, and teachers in an intervention guideline (Fonteyn-Vinke et al., 2020).
An intervention guideline is a document with systematically developed recommendations, aimed at improving the quality of care, based on systematic summaries of scientific research and considerations of the advantages and disadvantages of various treatments, supplemented with expertise and experiences of healthcare professionals and healthcare users (Brouwers et al., 2010a, 2010b; Regieraad kwaliteit van zorg, 2012). A treatment guideline offers guidance and practical instructions on how to act as a professional. The aim of the CVI guideline is to support therapists in making clinical decisions (American Psychological Association, 2002; Brouwers et al., 2010a, 2010b). Therapists receive information about the most effective treatments through the treatment guideline, so that the most recent knowledge can be implemented in clinical practice (American Psychological Association, 2002; Brouwers et al., 2010a).
An intervention guideline gives general recommendations on treatment options, whereas a protocol describes exactly how many sessions a treatment consists of, which methodologies must be applied, and what the therapist must do step by step (Hansen, 2002). This makes the prescriptions of a protocol not only clearer, but also more binding than a treatment guideline (Hansen, 2002; Swinkels et al., 2004).
The intervention guideline CVI focuses on two key areas of development, academic performance and mobility, and includes three main components: (1) a theoretical framework describing the functional hierarchical structure of vision and visual perception in CVI. The guideline follows Zuidhoek’s (2020) theoretical framework consisting of a hierarchy of visual functions. He distinguishes lower-order functions, such as visual acuity, eye movements, and visual field, and higher-order functions, such as global and local visual selective attention, perception of place, orientation, movement, speed, direction, and identification of objects. (2) A literature search using PubMed to look for available treatment methods (training or intervention) for children with CVI specifically, and the group of children with perceptual problems in general. (3) An inventory of practice-based clinical treatment components within Royal Dutch Visio (see Fonteyn-Vinke et al., 2020).
In an internal quality control according to the AGREE-II tool (Brouwers et al., 2010a, 2010b), the guideline scored positive on 83% of the items in the domain Subject and goal. On the domain Involvement and Stakeholders, the quality score was 74%, and for Clarity and Presentation, 96.3%. The scores for Methodology (44%), Application (36%), and Independency of authors (28%) indicated room for improvement.
The aim of this study was to evaluate the perceived value of the use of the intervention guideline by professionals involved in the habilitation and rehabilitation of school-aged children with CVI. To do so, two consecutive field studies were conducted. The first study was qualitative and the second study quantitative. Study 1 consisted of a process analysis of the preliminary guideline to come to the final guideline. It was the final step in the development of the guideline. Study 2 determined service providers’ satisfaction and practical use of this final guideline after they were trained in the use of the guideline. An overview of the study is depicted in Figure 1.
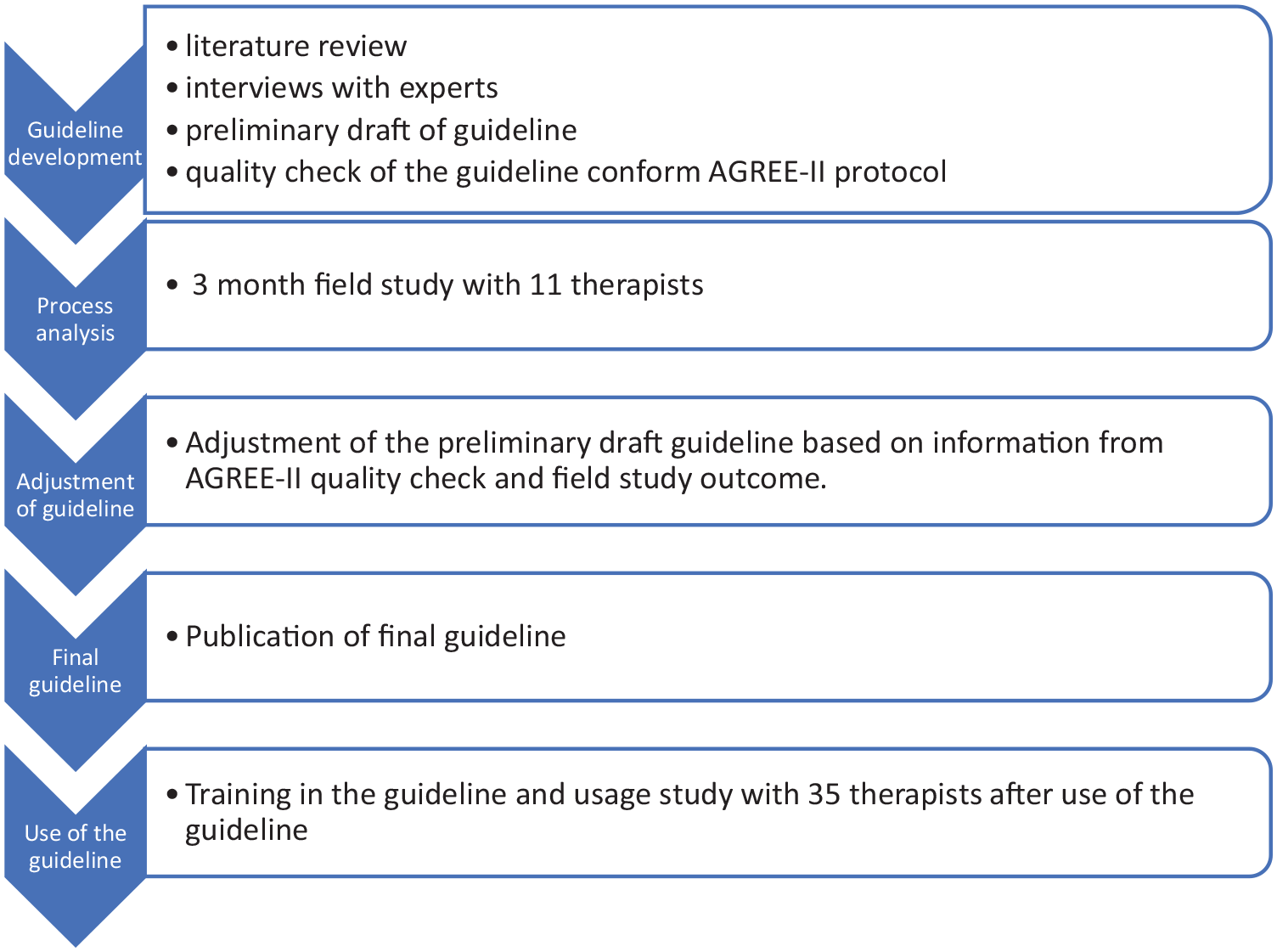
Overview of the development of the guideline interventions for CVI.
Field study 1: process analysis
Methods: study 1
Participants
In this pilot study, 11 vision therapists participated. Almost all vision therapists working with children with CVI at Royal Dutch Visio were invited to participate. From the 13 therapists who showed interest to volunteer, 11 signed up for the study. Drop-out consisted of two therapists who were unable to use the intervention guideline in the demanded period, due to health-related problems in one therapist and no available client with CVI at that moment for the second therapist. Eight participants were occupational therapists and three early interventionists. The age of the participants ranged from 27 to 59 years (M = 43.91, SD = 13.25). Experience with the treatment of children with CVI varied widely, from only 3 months to over 20 years.
Study design
A process analysis of the guideline was conducted as a pilot study with 11 therapists of Royal Dutch Visio. They used the concept of the intervention guideline in their treatment of children with CVI between 4 and 12 years of age in a fixed period of 3 months. Semi-structured interviews were held by the second author (H.F.) before and after the use of the guideline. In the first round of interviews, the therapists were given the opportunity to formulate their expectations about the guideline. In the second round of interviews, after using the guideline for 3 months, the questions concentrated on the usability of the guideline, strength and weaknesses of the guideline, and recommendations for adjustments (see supplemental material: Survey and questions for semi-structured interview). All interviews were transcribed before analysis with the help of the ATLAS.ti 8 software (Friese, 2019). The thematic analysis of the interviews was performed according to the method described in the work by Braun and Clark (2006). Themes, divided into before and after the study of the guidelines, were gathered inductively, that is, in a bottom-up way, and were not wedded to any pre-existing theoretical framework. Although the authors tried not to code the data to fit their pre-existing conceptions or theories about CVI, it is acknowledged that as Braun and Clark (2006) wrote, ‘. . . researchers cannot free themselves of their theoretical and epistemological commitments, and data are not coded in an epistemological vacuum’ (pp. 83–84). The sensitizing concepts that guided the authors’ analyses can be found in the introduction of this article. Fragments of the interviews were coded by the second author (H.F.) and discussed with the first and fourth authors (A.F-V. and M.P.J.V.). Afterwards, these open codes were grouped in content-based themes. Given the limited character of this first study, reaching data saturation was not feasible, and therefore not achieved. The fragments described in this article are all translations from the original Dutch citations. An overview of all answers to qualitative reporting issues according to the COREQ guidelines (Tong et al., 2007) is added as supplemental material.
Instruments
The intervention guideline for the treatment of school-aged children with CVI (Fonteyn-Vinke et al., 2020) consists of six chapters describing the theoretical framework, the basic elements of a intervention programme, how to perform an assessment, what the treatment principles are, interventions aimed at academic skills, and interventions aimed at mobility. The guideline is accompanied by appendixes describing the literature search, therapeutic materials, and ‘work sheets’ with a summary of strategies to treat higher-order visual dysfunctions (see Table 1). The intervention guideline (in concept) was available for all vision therapists during the treatment period.
Content of the intervention guideline for CVI.
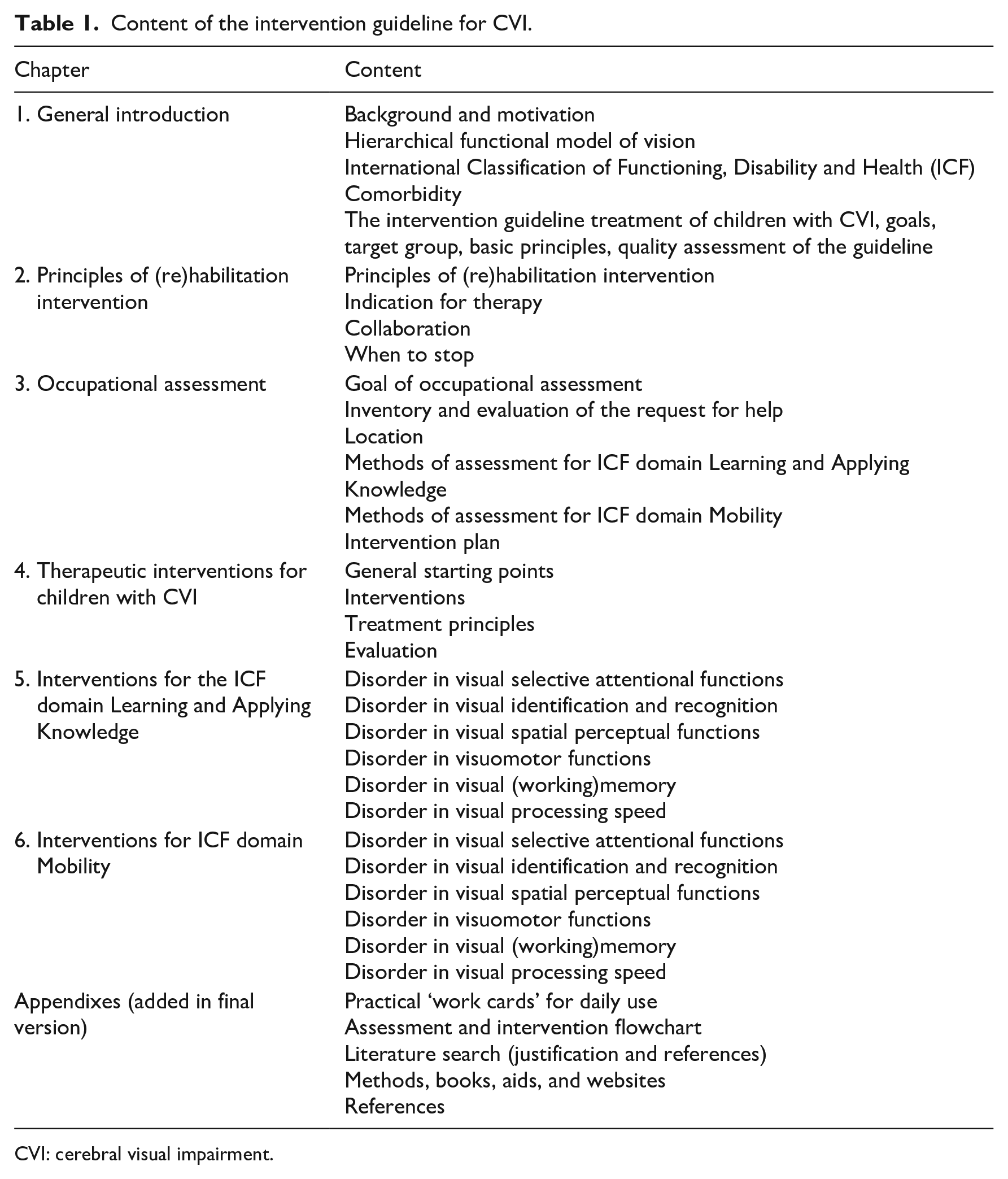
CVI: cerebral visual impairment.
Results study 1: process analysis of the guideline
The interview transcripts were analysed and quotes were coded in an open way. In a second round of axial coding, open codes were categorized in themes. The main themes are presented.
Sources for intervention
Before the use of the guideline, therapists formulated sources of information they used to create the most appropriate treatment plan, for example, their own experience and consultation with colleagues and/or literature, such as the books ‘Cerebral Visual Impairment in Children’ (Zihl & Dutton, 2015); ‘Cortical Visual Impairment: An Approach to Assessment and Intervention’ (Roman-Lantzy, 2018), and ‘CVI in the picture’ (Zuidhoek, 2020). One therapist said, ‘Sometimes it’s also a hunch, “maybe it’s good to do this now”, or from your intuition and from your experience of course. Intuition comes from your experience, I think. So, I trust my experience’.
Expectations and experiences about the guideline
Figure 2 shows the expectations formulated in the first round of interviews compared to the experience after 3 months of use. Expectations regarding a practice-oriented description with concrete recommendations which leads to a roadmap for treatment were fulfilled. As a participant said, ‘Where it felt before to me, much more like, oh I’ll try this, try that, and now you can focus a bit more’; ‘I found it useful that everything is in one place’. Also, the overview of current knowledge on CVI was appreciated, especially regarding the more practice-based information assembled. A participant formulated this in the following way, ‘There you have a bit more luggage. Then you observe the children a bit differently and sometimes you understand things they do better’. According to the participants, the intervention guideline fell short in the amount of evidence-based treatments that were presented. However, all therapists also realized there still is little evidence-based knowledge to present, see the quote, ‘I had hoped for a little more detail and evidence’. Participants also missed a checklist or other assessment instruments to guide the intervention, as well as a digital version of the intervention guideline.
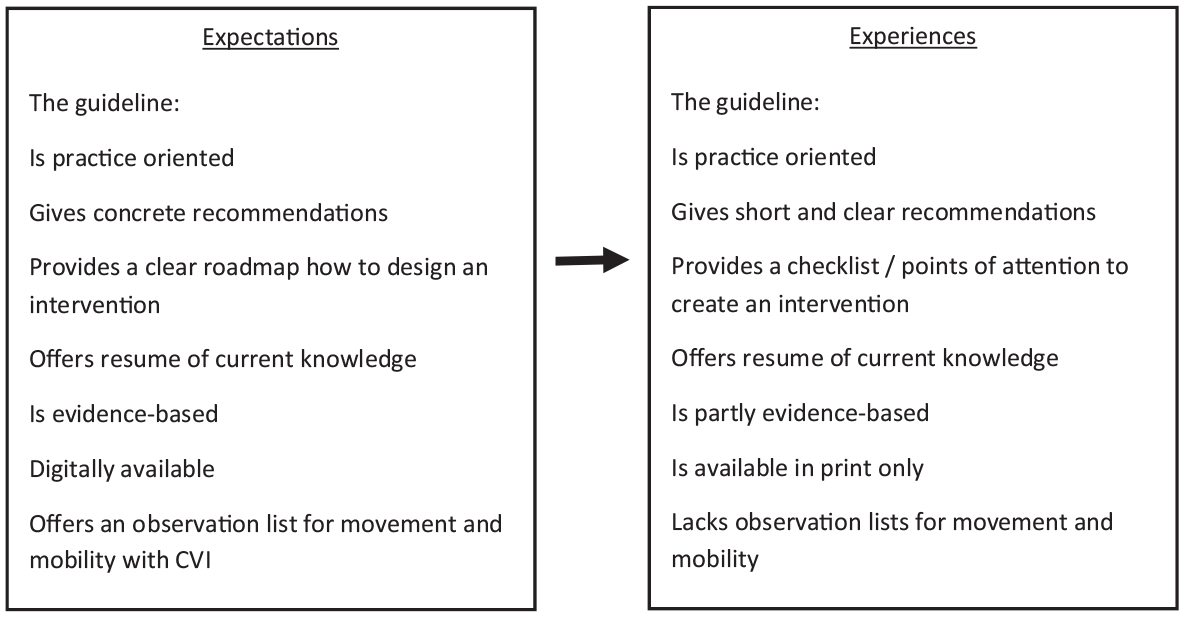
Expectations before the use of the guideline compared to the experiences of the vision therapists after 3 months of use.
Strength and weaknesses
Participants described what they found were the strengths and weaknesses of the guideline intervention for CVI. The strongest elements were analysing adequately the request for help from the client, the interdisciplinary approach and cooperation within the intervention team, training the child with CVI in their natural surroundings (home, school), and the possibility to customize the training to the specific problems the child encounters. Exemplary quotes from one of the therapists was, ‘So that you ask well, where are the problems? I think that’s really necessary it’s in multiple areas, not just scholastic areas. But also at home, shopping, maybe getting dressed’; ‘And also that as a supervisor you can get along very well with parents. There is room for that. You can do a lot to provide guidance. Fully attuning your input to what is desired and what is needed’; ‘I also think it’s very strong that you are involved with a team around a child. That you work very multidisciplinary’. Weaknesses experienced by the different therapists included questions about how to adjust the (re)habilitation programme to the specific individual needs and skills of the client (caused by the large variety in performance level); how to translate theoretical knowledge to daily practice; and how to deal with comorbidities. Participants phrased it this way, ‘I think I also miss things; I also forget things. I don’t have a checklist like ‘this, this and this I must observe’’; ‘That it is just very complex. That it is not standard like with hemianopia. But that the problems can be so diverse, that makes it difficult for me’; ‘Well, yes . . . because it really depends on the person. Because my colleague might do it very differently. I don’t even know’. Note that the practice at that time was that professionals relied on their own experience, expertise, and current level of knowledge about CVI to create the most optimal treatment plan.
The weaknesses of the intervention guideline were connected to these omissions. For example, therapists complained that the knowledge was still global and not specific and did not offer a solution to the difficulties they experienced. Therapists said, ‘Only the tips are . . . I don’t know how it could be otherwise, but the tips are partial parts. And what I find exceedingly difficult is to make it a whole’; ‘Each time those words, those terms that remain difficult. So, this is about visual selective attention. And then, oh, you have global and local visual selective attention of course, these are for both. Yes. Okay. Sometimes I need a little more explanation’.
In addition, some therapists did not feel that the assembled knowledge was ‘new’ but was better organized. Other therapists responded that a strength of the guideline was the new insight they gained after reading the intervention guideline. Other assets were the clear organization of knowledge and the link between theoretical knowledge and actual daily clinical practice. The participants made two recommendations: (1) to add clinical value they suggested to arrange the recommendations formulated in the intervention guideline on level of evidence and (2) to add more practical information, such as lists of Information and Communication Technology aids and observation items.
Conclusion: study 1
After the first study, the intervention guideline was adjusted to incorporate the suggestions made by the participants. In short, the main changes consisted of adding an extra appendix listing specific materials, methods, books, and websites, describing the selected interventions in more detail, and providing a digital version of the intervention guideline. Arranging the recommendations according to level of evidence was not possible, as most of the recommendations were practice-based, and too little evidence-based research on this topic was available.
Field study 2: use of the guideline
Methods: study 2
The second study was conducted after introduction of the revised intervention guideline for all professionals working with school-aged children with CVI at Royal Dutch Visio.
Study design, variables, and statistical analyses
In a pre–post-test design, all vision therapists included in a course about the intervention guideline for CVI were asked to fill in a brief survey (see Table 2 for the variables) the week before the training course and 3 months after the training. Answers were scored on a visual analogue scale ranging from 0 to 10. No psychometric information is available on the self-developed questionnaire; questions were analysed separate from each other. Within-group effects on the scores for each question were tested in SPSS-24 with the non-parametric Wilcoxon matched pairs signed-rank test with 95% significance levels.
Statements in the survey.
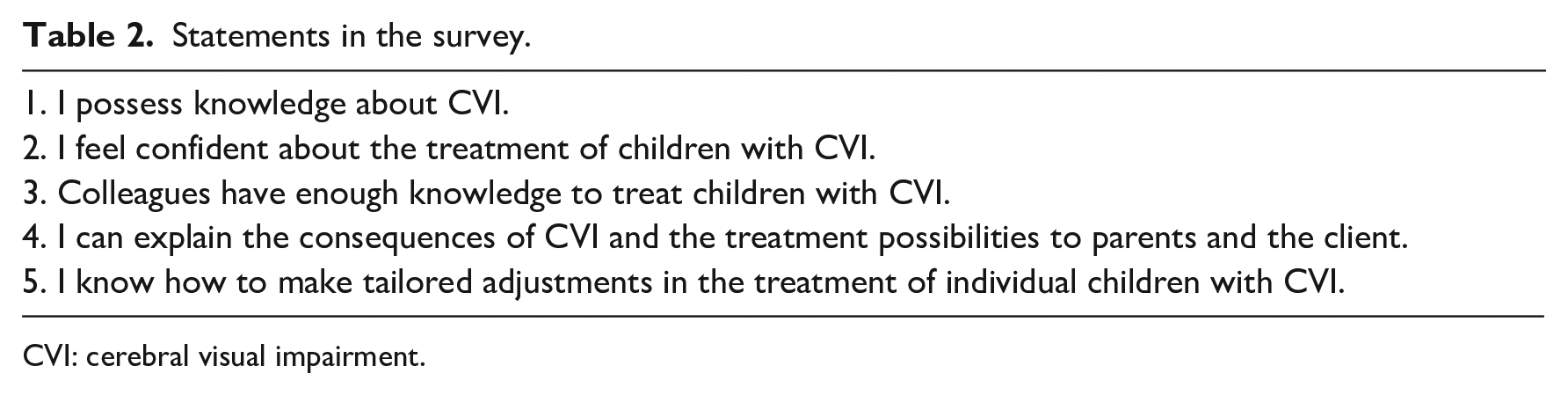
CVI: cerebral visual impairment.
Participants
All professionals who enrolled voluntarily in a course on the intervention guideline CVI were invited to fill in the questionnaire. Of these 68 professionals, 52 filled in the first questionnaire 1 week before the course started in May and formed the participants in study 2. Lack of time was the main reason therapists did not answer the survey before the course. The participants were asked to fill in the questionnaire a second time in September and were asked to use the intervention guideline in the meantime. The second survey was filled in by 24 (46%) of the original 52 participants. Reasons for nonresponse were checked by personal contact between the authors and the professionals participating in the training course. Drop-out after filling in the first questionnaire was due to non-use of the guideline within the 3 months after the training (no clients available during the summer holidays) and lack of time. Participants were between 23 and 61 years of age (M = 43.67, SD = 11.53). Among those who filled in the questionnaire twice, five were employed as occupational therapists, seven as early interventionists for children with visual impairments, three as early interventionist for children with multiple impairments, eight as itinerant teachers, and one as psychologist. Their experience with the habilitation and rehabilitation of children with CVI varied, from 6 months to 35 years. The average number of children supported by the itinerant teachers was 8.5 (range 0–22); the vision (re)habilitation workers (occupational therapists and early interventionists) saw, on average, 4.3 children (range 0–20) and the psychologist saw all children but only for assessments, not for interventions. Frequency of visiting a child with CVI ranged from weekly (n = 6), bi-weekly (n = 4), monthly (n = 4), and less than once per month (n = 8). No information on visit frequency was available for two respondents.
Training course
All professionals of Royal Dutch Visio working with primary and secondary school-aged children were invited to participate in a course on the CVI guideline. To allow all interested professionals to participate, the course was given four times in a short period of time. Participation was voluntary. Set-up of the training consisted of individual preparation by each participant by reading the Intervention guideline (online available) and to prepare a case study, to be used during the training. The participants were allowed 4 hr study time for this. The actual training session was conducted online and lasted 3 hr with a group of 12–15 participants and with two teachers present.
The training consisted of a short lecture on the development and the use of the guideline, and practicums with case studies. The first case study was prepared by the teachers and discussed with the whole group. In the latter part of the training, the participants were divided into four small groups to discuss the use of the intervention guideline for their own case studies. Teachers were present in each break-out room half the time. A plenary discussion of important topics and remaining questions finalized the training. The background of the teachers in this course were neuropsychology and occupational therapy; all were co-authors of the Intervention guideline. Teaching material consisted of the guideline itself, the book CVI in the picture (Zuidhoek, 2020), and a PowerPoint presentation, including a case study with assessment and intervention information as well as video footage.
Results: study 2 – survey on the use of the guideline
Study 2 focused on the effects after the course and post-use of the intervention guideline for the 24 therapists who filled in the questionnaire twice. The themes were perceived knowledge, self-confidence in treatment, explanation of CVI consequences, CVI-specific treatment, and perceived knowledge of colleagues. The pre- and post-use scores are shown in Figure 3.
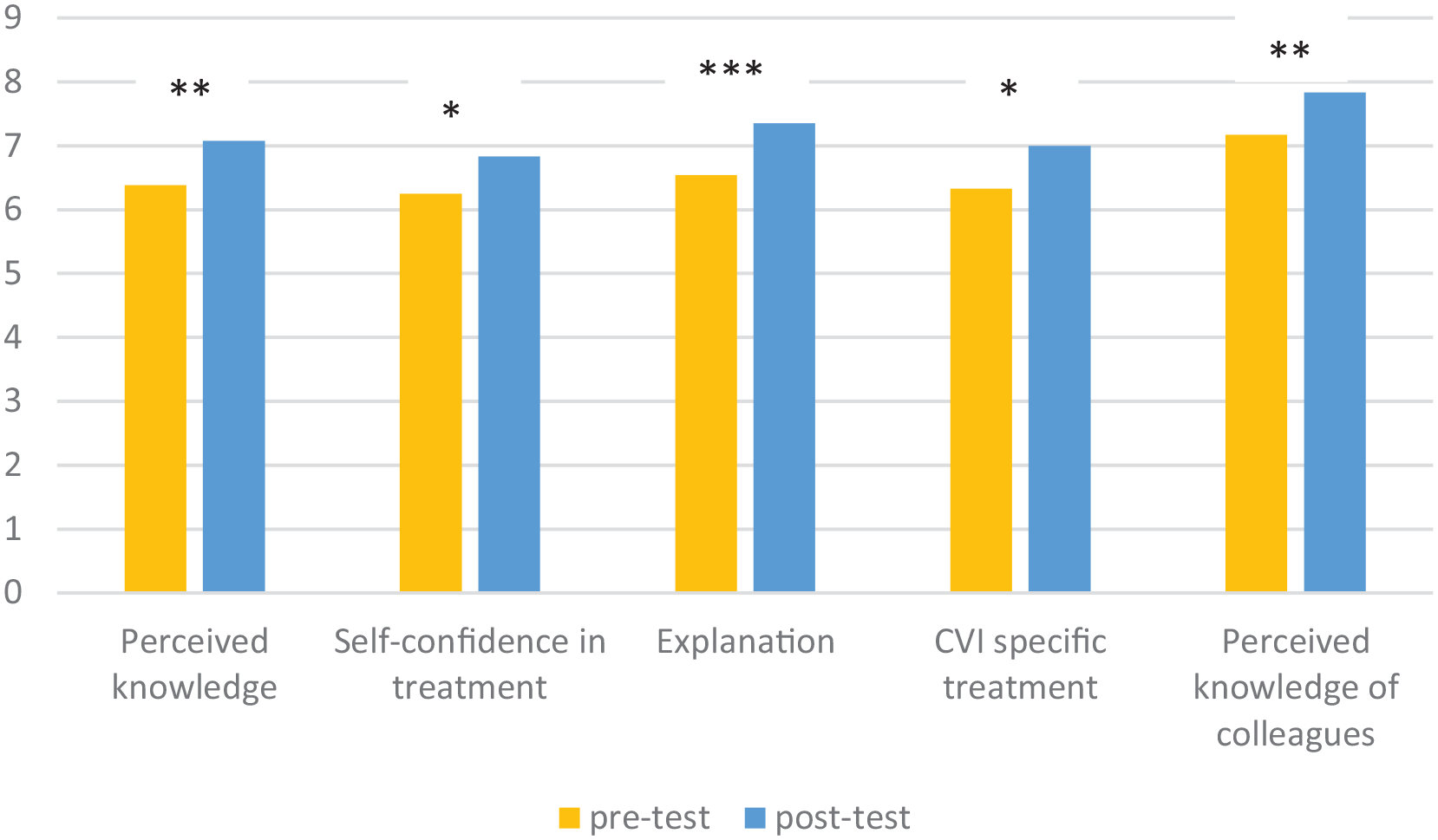
Mean scores on visual analogue scales (range: 0–10) on the survey before and after training in the intervention guideline.
Given that improvement was expected all T tests were done with half-sided exceedance probabilities. The perceived knowledge on CVI improved significantly after the training and use of the intervention guideline (mean: 6.38 before vs 7.080 afterwards), T = −2.90, p = .004, d = 0.60. The participants’ level of self-confidence during the treatment of clients with CVI improved significantly (mean before 6.25 vs 6.83 afterwards), T = −1.98, p = .030, d = 0.40. Also, they felt their explanation of CVI and the visual behaviour of the clients to the client system improved significantly (6.54 vs 7.38), T = −3.62, p < .001, d = 0.73. With the use of the guideline, the professionals felt that the interventions offered to clients with CVI were more specific and tailored to individual clients (6.37 vs 7.00), T = −2.23, p = .018, r = 0.31. Finally, the perceived knowledge of colleagues improved significantly (mean 7.17 before vs 7.83 afterwards), T = −2.71, p = .006, d = 0.55. Correlation analyses between years of experience and improvement after training showed moderate negative correlations for Perceived knowledge, Self-confidence in treatment, Explanation, and CVI-specific treatment adaptations (Rho’s, respectively, −.57, −.44, −.59, and −.46). Perceived knowledge of colleagues did not correlate significantly. So professionals with the lesser amount of years of experience profited more from the training than the ones with more years of experience.
Discussion: study 2
The purpose of this study was to evaluate the clinical relevance of the use of an intervention guideline for the visual habilitation and rehabilitation of school-aged children with CVI. Professionals in vision (re)habilitation followed a training course and used the intervention guideline for 3 months. In general, the participants felt more confident in their interventions for children with CVI after the course and the use of the guideline. They experienced more knowledge on CVI in themselves and in colleagues. In addition, they showed more skills in explaining CVI-related problems to the children and their parents and felt they could create more specific intervention plans.
The therapists did not find enough concrete and specific adjustments for the visual (re)habilitation interventions they already gave. This might be related to the lack of evidence-based interventions for children with CVI. Although the intervention guideline collected and organized available knowledge and interventions, no advice on which specific evidence-based treatment option should be used in a certain situation could be prescribed. The answers given by therapists were analysed anonymously. This prevented an analysis of knowledge, satisfaction, and need for more information based on the participants’ expertise and experience. The theoretical framework based on Zuidhoek (2020) seemed to have provided the participants with enough information to interpret the visual behaviour of children with CVI and created ample awareness on visual functioning of the children diagnosed with CVI. The intervention options mentioned in the guideline were specific for the different higher-order visual functions originating from the theoretical framework. However, the theoretically present division in these functions is hard to find in the daily practices of the participants, which made it challenging for them to adjust their intervention plans. Moreover, the guideline assembled mostly practice-based intervention options, since hardly any evidence-based treatments are available for children with CVI. More research on CVI-specific treatment options is therefore still necessary.
This study was limited in time and number of participants. Almost one-third of the therapists were not able to fill out the second survey. Although children with CVI form about half the population of children with vision impairment, not all children with CVI are diagnosed as such, so that per professional the number of clients in whom CVI is established with certainty is low. The vision therapists who did fill out the survey twice varied in occupational years and preliminary education. This heterogeneity makes it hard to draw solid conclusions about for whom the guideline is especially useful.
In conclusion, the intervention guideline for school-aged children with CVI seems to partially fulfil a need for information regarding the visual (re)habilitation for children with CVI. The intervention guideline helps in formulating goals and in evaluating the (re)habilitation process of children with CVI regarding academic performance and mobility issues. In their daily practice, the therapists felt more confident about their interventions while using the guideline. This was probably caused by an improvement in their general knowledge about CVI and about available treatment options. However, the improvement was small and still not perfect and could be enlarged by adding more concrete intervention suggestions to the guideline.
General discussion and conclusion
The report describes the development of and first experiences with a guideline on CVI interventions for teachers and early interventionists. The guideline made available the best available knowledge on how to help children with CVI in the International Classification of Functioning, Disability and Health (ICF) domains of motor development and mobility, and of learning and applying knowledge. As described, children with CVI experience a range of visual processing problems (Ben Itzhak et al., 2020; Zihl et al., 2023). As a result, interventions for learning and academic performance and mobility will differ for each child. As Dutton and Bauer (2019) remarked, ‘CVI has many possible variables, giving every affected child their own unique pattern of visual experience, limitations and resulting behaviours’ (p. 53). Unfortunately, the number of empirically proven interventions for children with CVI is rather limited. A fact recently confirmed by Delay et al. (2022) concluded that intervention research for children with CVI is still in its infancy. Although interventions for children with CVI may be beneficial, comparing results is difficult due to inconsistency in outcome measures (Delay et al., 2022). Taken together, this means that the guideline does not consist of fully worked-out interventions or cookbook instructions on ‘how to do a CVI intervention’. Instead, the guideline provides an extensive list of intervention strategies tailored to the higher-order visual function problems children with CVI encounter. It is supplemented with work cards, summarizing recommendations for each visual function, a resource appendix with materials and methods useful to apply to children with CVI, and a list of references (Fonteyn-Vinke et al., 2020). Of the categories of interventions that might be effective according to Delay et al. (2022), visual stimulation, task/environmental adaptations, vision training, acupuncture, stem cell transplantation, and transcranial electric stimulation, the guideline uses only task/environmental adaptations and vision training. As there is insufficient evidence that isolated training of visual functions actually work, they were not included in the intervention guideline.
Since CVI can co-exist with several ocular conditions, such as retinopathy of prematurity, the distinction between ocular and CVI is not distinct (Dutton & Bauer, 2019). This means that interventions for CVI should also take into account interventions designed for ocular disorders. We agree with the call made by Dutton and Bauer (2019) that we need to ‘know each child’s set of perceptual limits and how and why these constrain learning, to work out how each child can be parented and taught using perceptible and meaningful approaches’(p. 54). The guideline developed by Fonteyn-Vinke et al. (2020) helps the vision therapist with listing the abovementioned aspects of vision. The guideline also fits the three-step intervention approach described by Dutton and Bauer: (1) compensate for the lack of function, for example, enlargement of print for low visual acuity, or increased spacing of print in case or crowding problems; (2) introduce alternative approaches for vision, for example, listening to the spoken word instead of reading; and (3) train the child in all salient strategies within the child’s capabilities to bypass vision or compensate for visual function that does not work.
Are substantial improvements to be expected once children are trained with the help of the guideline? We tend to be modest in answering this question. First of all, because effect studies with the help of the guideline have not been pursued yet. Second, because, as Delay et al. (2022) showed in a recent scoping review, the majority of interventions for CVI show low to medium effect sizes, which minimizes the reliability, validity, and generalization of results. Moreover, these authors also concluded that the intervention results were ambiguous. For now, we see the guideline as a starting tool that helps professionals improve their interventions for children with CVI.
Supplemental Material
sj-docx-1-jvi-10.1177_02646196241230268 – Supplemental material for Effects of a guideline for children with cerebral visual impairment on the daily practices of vision habilitation and rehabilitation workers
Supplemental material, sj-docx-1-jvi-10.1177_02646196241230268 for Effects of a guideline for children with cerebral visual impairment on the daily practices of vision habilitation and rehabilitation workers by Anke Fonteyn-Vinke, Hajar Fakir, Marieke Steendam and Mathijs P J Vervloed in British Journal of Visual Impairment
Supplemental Material
sj-docx-2-jvi-10.1177_02646196241230268 – Supplemental material for Effects of a guideline for children with cerebral visual impairment on the daily practices of vision habilitation and rehabilitation workers
Supplemental material, sj-docx-2-jvi-10.1177_02646196241230268 for Effects of a guideline for children with cerebral visual impairment on the daily practices of vision habilitation and rehabilitation workers by Anke Fonteyn-Vinke, Hajar Fakir, Marieke Steendam and Mathijs P J Vervloed in British Journal of Visual Impairment
Footnotes
Authors’ Note
The first draft of this manuscript was written by Anke Fonteyn-Vinke in 2022. Due to illness, Anke passed away later that year. To honour Anke, we kept her as the first author of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.