
Abstract
Cerebral visual impairment (CVI) is the most common cause of visual impairment in children in the United Kingdom. The mainstay of management is providing strategies and environment adaptations to allow the child to use their vision for learning and independence. It is therefore important to understand educational access policies to facilitate timely and appropriate referral to qualified teachers for learners with visual impairment (QTVI) by ophthalmologists. QTVIs were recruited from VIEW (Visual Impairment England and Wales) and the Scottish Sensory Centre (QTVI organisations) via email, newsletter and social media. Respondents were directed to an online electronic questionnaire. 116 responses were received; this represents around 18% response rate. All services accepted referrals for children with cerebral visual impairment (CVI). The majority of services (97%) did not have a strict visual acuity threshold for children with CVI. There is an inconsistent approach in the diagnosis of CVI across the United Kingdom, with some QTVI expressing concern that this had prevented children with visual dysfunction from accessing help. QTVI indicated they would welcome more referrals for Cerebral VI, at an earlier age, and that a formalised referral pathway would be beneficial. Children with CVI are accepted for support by QTVI/sensory services regardless of visual acuity. Some services welcomed referrals for children undergoing assessment where CVI had yet to be confirmed. However, the formal diagnosis of CVI by an ophthalmologist as a pre-requisite to access services in other areas emphasises the need to improve clinicians’ confidence in the diagnosis of CVI. Ophthalmologists are encouraged to engage with local QTVI/sensory teams to facilitate exchange of information and appropriate and timely referral of children in need.
What was known before
Cerebral visual impairment (CVI) is the most common cause of visual impairment in children in the United Kingdom.
The management of CVI is dependent on strategies to support the child to access learning and education.
What this study adds
Education services no longer apply strict visual acuity thresholds, instead considering the child’s visual broader visual function.
Many services do not require formal diagnosis with CVI prior to referral and welcome early engagement as soon as visual difficulties are recognised.
For children with normal acuity, it is important for clinicians to state in the referral the specific nature of the visual impairment which presents a barrier for the child to access learning.
Cerebral visual impairment (CVI) is the most common cause of visual impairment in children in the United Kingdom (Teoh, Solebo, Rahi, & British Childhood Visual Impairment and Blindness Study Interest Group, 2021). Recent studies have shown that around one in five children in special school (Donaldson et al., 2019) and one in 30 children in mainstream school have brain-related visual problems (Williams et al., 2021).
The mainstay of management of cerebral visual impairment is in developing strategies to enable children to use their vision more effectively, through adaptations to their environment and visual tasks they are required to perform in daily life. For children, this encompasses adjustments to enable them to access education and maximise their academic potential. A UK study identified that parental and teacher understanding of the child’s CVI and individual information on strategies to support the child were important to promote successful intervention (Goodenough et al., 2021).
The recent publication of a Future Commission Report (Guide Dogs UK, 2021) by the charity Guide Dogs highlighted how accessing services and support at the right time can be a gateway to increasing confidence, happiness and independence in children and young people with a vision impairment and can have a positive impact for parents, carers and families (Robertson et al., 2021).
The newly updated Royal College of Ophthalmologists Ophthalmic Services for Children Guidance (Royal College of Ophthalmologists, 2021) states that ‘children with a confirmed visual disability should have access to local QTVIs . . . Signposting families to these supportive services is important’. (p. 3) and ‘Active regular communication to outside agencies such as visual impairment teachers is important’ (p. 8). All children with visual dysfunction require referral to sensory support services and qualified teachers of learners with visual impairment (QTVI) by ophthalmologists. While some children with CVI will have coexisting ocular visual impairment (OVI), others will have normal visual acuity and a normal ocular examination.
It is therefore important for ophthalmologists to understand non-acuity based referral criteria for children with CVI. This understanding is also reinforced by The National Sensory Impairment Partnership (NatSIP) which defines vision impairment not through acuity but through visual function: From a functional standpoint, a child or young person can be considered to have a vision impairment if this interferes with optimal development, learning and achievements unless adaptations are made in the methods of presenting learning experiences, the nature of the materials used and/or the learning environment. (National Sensory Impairment Partnership, 2021)
The aim of this study was to describe the current requirements and criteria used by individual services for referral to QTVI/sensory services in the United Kingdom for children with a diagnosis of cerebral visual impairment.
Methods
Participants were recruited via email, newsletter and social media posts to members of VIEW (Visual Impairment England and Wales) and through the Scottish Sensory Centre, Scotland, organisations for Qualified Teachers of the Visually Impaired (QTVI). Respondents were directed to an online electronic questionnaire. Responses were anonymous, and the study was approved by the Biomedical, Natural, Physical and Health Sciences Research Ethics Panel, University of Bradford. All responses received by the close date were included.
A copy of the questionnaire is shown in Figure 1 encompassing the following areas:
Visual acuity thresholds for referral (near and distance).
Requirement for sight impairment registration prior to referral.
Requirement for formal diagnosis/consultant ophthalmologist involvement.
Referral processes for cerebral visual impairment.
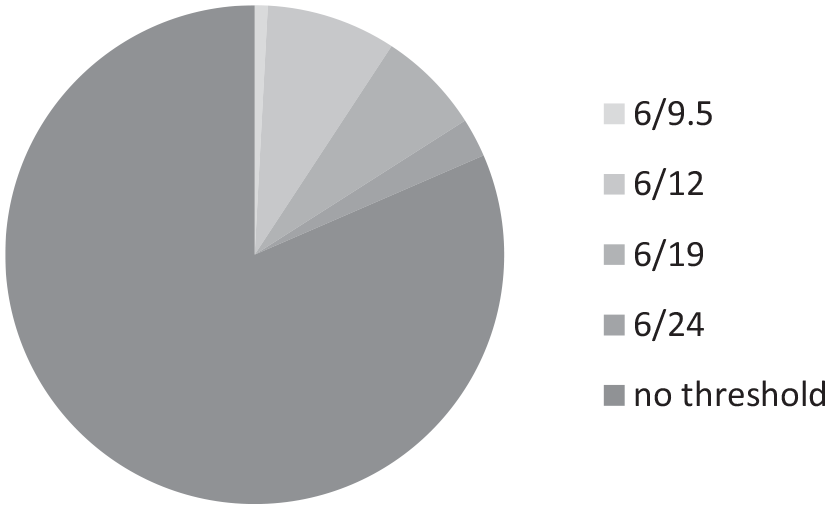
Reported distance acuity threshold below which a referral to QTVI would be accepted for ocular visual impairment.
Results
116 responses were received; 87 from England, 23 from Scotland, 4 from Wales and 1 from Northern Ireland. There are approximately 650 QTVI in the United Kingdom: this represents around 18% response rate.
Visual acuity threshold for referrals for ocular or cerebral visual impairment
22 (19%) respondents indicated their service adopted a distance visual acuity threshold for referral into services, as shown in Figure 1. Near acuity thresholds were described by 13 (11%) respondents, shown in Figure 2.
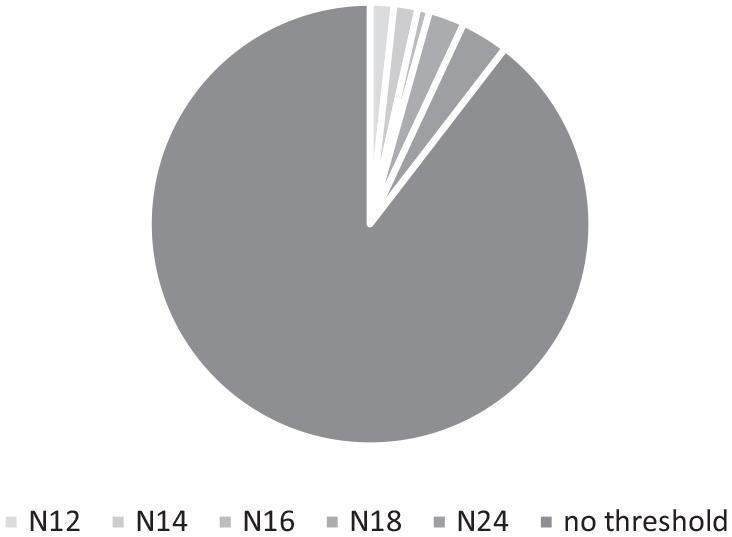
Reported near acuity threshold below which a referral to QTVI would be accepted for ocular visual impairment.
However, all but four participants commented that in effect there were no acuity thresholds to be met for a referral to QTVI to be made. Rather, a more holistic needs-based approach was taken, in relation to visual field, nystagmus, cerebral visual impairment, and night blindness/photophobia.
Referrals for cerebral visual impairment
All services accepted referrals for children with cerebral visual impairment from ophthalmology teams. 74/96 (77%) respondents offering additional information indicated there were no specific criteria or thresholds to be met. 24 respondents (21%) commented on the importance of a diagnosis of ‘cerebral visual impairment’ being specifically mentioned in the referral for them to begin the assessment process. Six services were able to accept a child with suspected CVI and one respondent stated their team were involved in the diagnosis and assessment process in conjunction with the hospital eye team.
Two respondents required combined ocular and cerebral visual impairment with acuity of 6/12 and 6/19 being set by their local schools as a threshold for funding. One practitioner explained how, for children with normal acuity, it was important for clinicians to specify in the referral that visual impairment was a barrier for the child to access learning.
Free text comments revealed two main themes:
Variation in approach from ophthalmologists around diagnosis and referral to refer to QTVI – either A. Cerebral Visual Impairment was underdiagnosed and/or under-referred by hospital specialists (16 respondents) or B. There had been a recent increase in workload due to Cerebral Visual Impairment referrals (14 respondents)
Referrals often lacked detail regarding the areas of the child’s visual dysfunction (13 respondents)
Underdiagnosis of CVI was perceived by one respondent to be more often seen in children with complex needs. An equal number of respondents commented positively and negatively about local attitudes to CVI diagnosis. Some reported that their local eye services were closely involved with QTVI and made a lot of CVI referrals, whereas others lamented a lack of interest from local ophthalmologists who are more reluctant to make the diagnosis, and symptomatic children are sent away being told there is nothing wrong with their vision.
On a more positive note, three respondents reported recent training they had received in CVI and that a structured approach to referrals, assessments and provision of support had been developed.
Sight impairment registration (England, Wales, and Northern Ireland only)
Only two respondents indicated that sight impairment registration was a pre-requisite of being able to accept a referral. One respondent stated this was a result of funding being delegated to schools and that each set their own threshold for ‘buying in’ services. One service indicated that funding for habilitation services may be affected by sight impairment registration.
This study has certain limitations: we cannot be certain that the respondents represent the whole of the United Kingdom, nor that reporting bias may be present for those participants who have an interest in CVI. To preserve anonymity, we were unable to collect data on the participants’ education authority. We cannot be certain that multiple responses were not received for the same education authority; however, it could be supposed that QTVI may have decided among the team which member would respond to the study recruitment email. The strength of the study is in the diversity of views expressed, representing the spectrum of experiences which parents and children may encounter and making a case for reducing inequalities in access.
Conclusion
The James Lind Alliance Sight Loss and Vision Priority list (James Lind Alliance, 2013) rated cerebral visual impairment identification, prevention and treatment as its top research priority in childhood onset disorders. Studies into the temporal trends in visual impairment in children in the United Kingdom state that ‘tackling cerebral visual impairment is now the biggest challenge and biggest opportunity for reducing the burden of childhood blindness’ (Teoh, Solebo, & Rahi, 2021).
The results of our study show wide ranging variation in practice with regard to QTVI referrals and support for children diagnosed with Cerebral Visual Impairment. It is clear that no national visual acuity threshold criteria exist for referral into sensory services/QTVI and that local areas develop their own policies. Future studies would benefit from a targeted approach to individual education authorities to maximise response rate and coverage across all regions of the United Kingdom. This would also provide a more reliable denominator from which to draw conclusions. Developing standardised criteria for services is complicated; however, the call for a universal process by the study participants is echoed in a recent Creating The Future Commission from a national sight loss charity (Guide Dogs UK, 2021).
It is noteworthy how important it is for the referring ophthalmologist to state explicitly that the child has a diagnosis of cerebral visual impairment on a letter to QTVI services. Ophthalmologists may be unaware than nearly a quarter of services were unable to offer support in the absence of a formal diagnosis by an ophthalmologist. It is also evident that providing adequate information regarding the nature of the child’s visual impairment, beyond a simple acuity measurement, is valued by QTVI for them to begin the assessment process. A Core Outcome Set for children with CVI was recently published to establish baseline function and demonstrate progress, and this may be a useful starting point (Pease et al., 2021).
Even though the responsibility for Education has been devolved to the four nations of the United Kingdom, it is clear that across the United Kingdom QTVI consider any child in whom vision may be a barrier to learning warrants referral into education sensory services. Communicating this message clearly to ophthalmologists is important to have a lasting impact on the learning outcomes of the growing population of children with CVI.
The study has revealed barriers which children with CVI may experience in fulfilling their potential, and the role that eye health professionals play in improving this. Ophthalmologists are unlikely to have an in-depth knowledge of local resources and requirements within education and habilitation; it is therefore vital that they understand how and when to refer a child into sensory services to enable them to access support.
Supplemental Material
sj-pdf-1-jvi-10.1177_02646196221143315 – Supplemental material for Cerebral visual impairment and educational support in the United Kingdom: Understanding thresholds for providing support
Supplemental material, sj-pdf-1-jvi-10.1177_02646196221143315 for Cerebral visual impairment and educational support in the United Kingdom: Understanding thresholds for providing support by Rachel F Pilling and John Ravenscroft in The British Journal of Visual Impairment
Footnotes
Acknowledgements
The authors thank VIEW, the Scottish Sensory Centre and the participants for their contributions.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Prof. J.R. is editor of this journal.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.