
Abstract
Age-related macular degeneration (AMD) is a prevalent eye disease, which can lead to vision loss, impacting daily functioning. This study aimed to evaluate the effect of low-vision rehabilitation techniques such as magnifiers, telescopes, and microperimeter feedback, on improving reading speed and reducing depression in AMD patients. This study is a systematic review and meta-analysis. A systematic search of databases MEDLINE (OVID), EMBASE (OVID), and CINHAL (EBSCO), gray literature including ClinicalTrials.gov and ProQuest Dissertations and Theses Global (ProQuest), Conferences of The Association for Research in Vision and Ophthalmology, American Academy of Ophthalmology, and Canadian Ophthalmological Society were done from inception to 27 July 2022. Fixed-effect and random-effect models were applied to account for heterogeneity between studies. Publication bias was checked through funnel plots. A total of 33 studies (2611 subjects) were included;14 studies were included in the meta-analysis (1123 subjects) and 19 were included in the qualitative analysis. We found a non-significant increase in reading speed (effect size [ES] = 0.02, 95% confidence interval [CI] = [−0.18, 0.23]) for studies comparing patients who received no low-vision rehabilitation, versus the intervention group of AMD patients who received low-vision rehabilitation. We also found a significant decrease in reading speed (ES = −0.92, 95% CI = [−1.46, −0.39]) between studies evaluating the difference in reading speed at baseline visits compared to the follow-up visits in AMD patients who received low-vision rehabilitation. Low-vision rehabilitation was also found to result in a decrease in depression severity when compared to control groups, as well as from initial assessment to subsequent follow-up visits. Individuals with AMD who engaged in low-vision rehabilitation demonstrated improved reading speeds compared to their own baseline and to those who did not receive any interventions. Furthermore, these interventions also contributed to a reduction in symptoms of depression.
Keywords
Introduction
Age-related macular degeneration (AMD) is a major cause of visual impairment. In 2020, around 6.22 million cases of moderate and severe visual impairment (MSVI), in adults aged 50 and older, were attributed to AMD (GBD 2019 Blindness and Vision Impairment Collaborators, & Vision Loss Expert Group of the Global Burden of Disease Study, 2021). Visual impairment poses significant challenges in performing activities of daily living (ADLs), including tasks such as cleaning, eating, and dressing, as well as instrumental ADLs (iADLs) such as shopping, driving, and managing finances (J. C. Brown et al., 2014; Whitson et al., 2014).
The impact of AMD on work productivity is substantial. Individuals with AMD face annual income losses of approximately US$55,180 (M. M. Brown et al., 2016) and an unemployment rate of around 77% (Honda et al., 2021). The global economic burden of MSVI and blindness is alarming, with the associated annual productivity loss estimated to be US$410.7 billion (Marques et al., 2021). Implementation of strategies to assist individuals with visual impairment in obtaining and retaining employment could yield substantial productivity benefits and enhance the global economy Marques et al., 2019]. With an aging population and the growing participation of older adults in the workforce (Dixon, 2003), low-vision rehabilitation for people with MSVI have become increasingly necessary.
AMD affects macula, an area of the retina that contains the highest concentration of photoreceptors responsible for sharp central vision (Deng et al., 2021). While central vision is compromised, peripheral vision usually remains intact and is often the focus of low-vision aids (Elliott et al.,1991). Unfortunately, AMD is an incurable disease, making low-vision rehabilitation critical in maintaining independence for those affected (Bressler et al., 1988).
Reading abilities tend to deteriorate as vision worsens (Horowitz et al., 2006). Several low-vision rehabilitation strategies have shown to improve reading speed (Cheong et al., 2009; Nilsson et al., 2003; Scanlan & Cuddeford, 2004; Seiple et al., 2011; Smith et al., 2005; Vingolo et al., 2007) and depression scores (Brody et al., 2006; Girdler et al., 2010). Reading speed serves as a reliable indicator of functional reading capacity, which is why it was selected as the primary outcome for this meta-analysis. AMD can cause severe depression and diminished quality of life (Casten et al., 2004). Low-vision rehabilitation not only improves visual function but also boosts psychological well-being in AMD patients (Cimarolli et al., 2012). Hamade et al. (2016) carried out a meta-analysis examining the influence of low-vision rehabilitation on reading speed and depression in AMD patients. Our objective is to integrate the latest advancements in the field to deliver an updated and precise comprehension of low-vision ’rehabilitation’s effect on individuals with AMD, ultimately contributing valuable knowledge for the creation of future interventions and support networks. All in all, we performed a meta-analysis to assess novel low-vision rehabilitation techniques in people with AMD, specifically focusing on improvements in reading speed and depression scores.
Methods
Studies and participants
This meta-analysis included studies that investigated 20 or more eyes of patients with AMD, irrespective of the AMD subtype, and incorporated the use of low-vision aids, devices, and rehabilitation training. Review articles, case reports, systematic reviews, meta-analyses, letters to editors, and commentaries were excluded. Conference articles were included if they provided adequate study details and data. Non-English studies were excluded to avoid potential translation inconsistencies. There were no restrictions based on publication year or geographical settings. The meta-analysis specifically examined outcomes related to reading speed and depression scores.
Search strategy
We followed the PRISMA guidelines for conducting systematic reviews and meta-analysis, which are outlined in Supplementary Appendix A. Our search encompassed the databases MEDLINE(OVID), EMBASE (OVID), and CINHAL (EBSCO) from their inception until 7 July 2022. Gray literature searches included ClinicalTrials.gov and ProQuest Dissertations and Theses Global (ProQuest). In addition, we manually examined relevant poster presentations and abstracts from conferences such as The Association for Research in Vision and Ophthalmology, American Academy of Ophthalmology, and Canadian Ophthalmological Society. The search strategy is provided in Supplementary Appendix B. As our study solely relied on online data and did not involve human subjects, ethics approval was not necessary (see Figure 1).
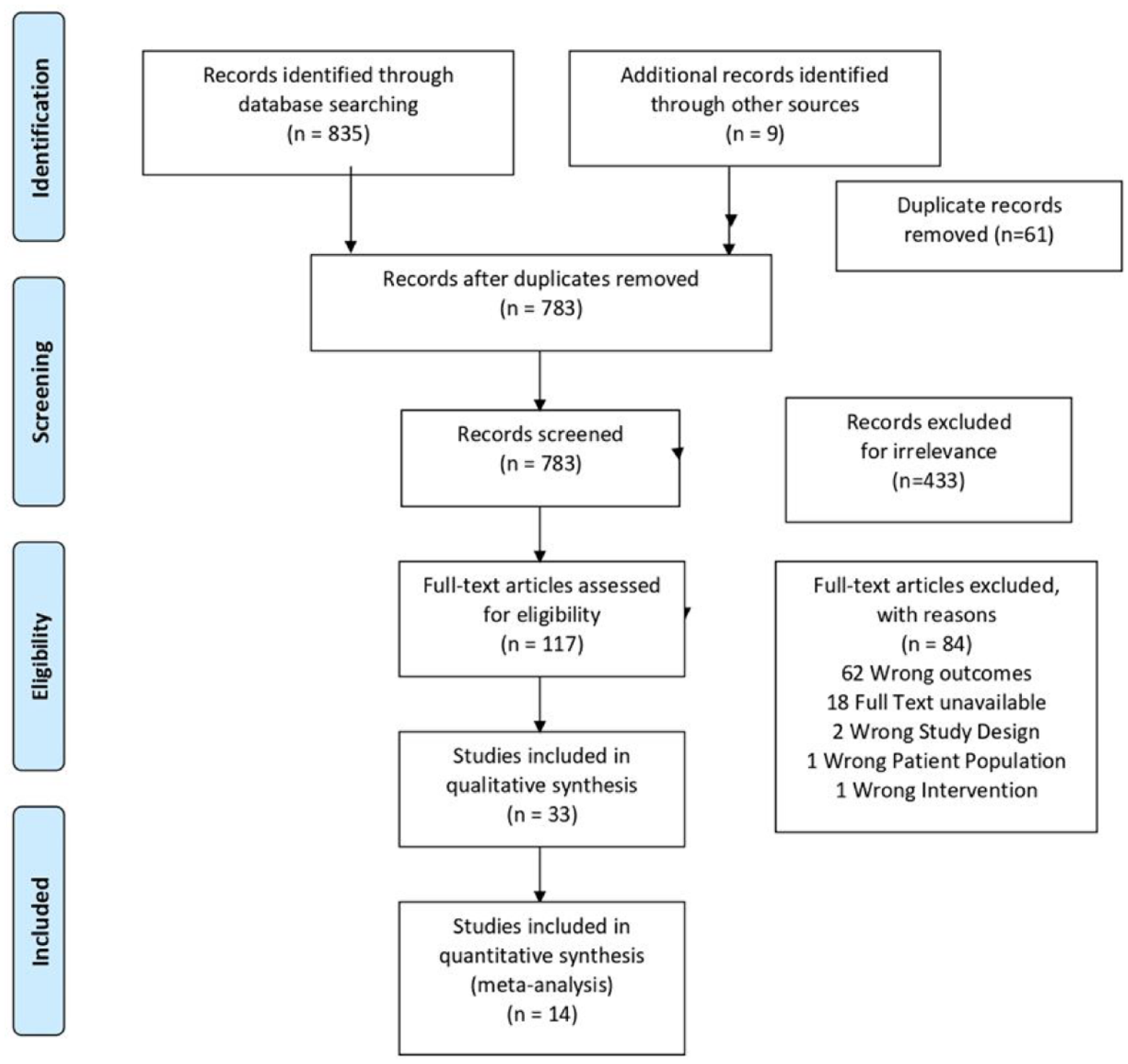
PRISMA flowchart summarizing the results of the literature search.
Study selection
The literature compiled from the databases was imported into Covidence for automatic duplication checks. A manual duplicate check was performed by a reviewer (E.T.). Two reviewers (E.T. and N.S.) independently conducted three levels of screening. The first and second levels involved screening titles and abstracts for literature related to AMD and low-vision rehabilitation strategies. The third level comprised full-text screening of studies that investigated a minimum of 20 adult eyes with AMD and reported outcomes related to reading speed or depression. Conflicts were resolved through consensus, with intervention from a third reviewer, if needed.
Risk of bias assessment
The risk of bias assessment was carried out using the modified Downs and Black checklist (Downs & Black, 1998). Studies with a score exceeding 20 were categorized as high quality, those scoring between 16 and 19 were deemed medium quality, while studies scoring below 15 were regarded as poor quality. A thorough quality check was conducted to ensure the comprehensiveness of our methodology. Given the limited evidence available, no articles of lower quality were excluded from the analysis. Further details on the risk of bias assessment can be found in Supplementary Appendix C.
Data collection process
After conducting the quality-check process, data on study characteristics were extracted from 33 articles (see Table 1), including author, year of publication, study design, study location, and sample size. A total of 14 articles were selected for quantitative synthesis, focusing on the effects of various low-vision rehabilitation strategies on reading speed in AMD patients.
Study characteristics of articles involving AMD patients who underwent low-vision rehabilitation.
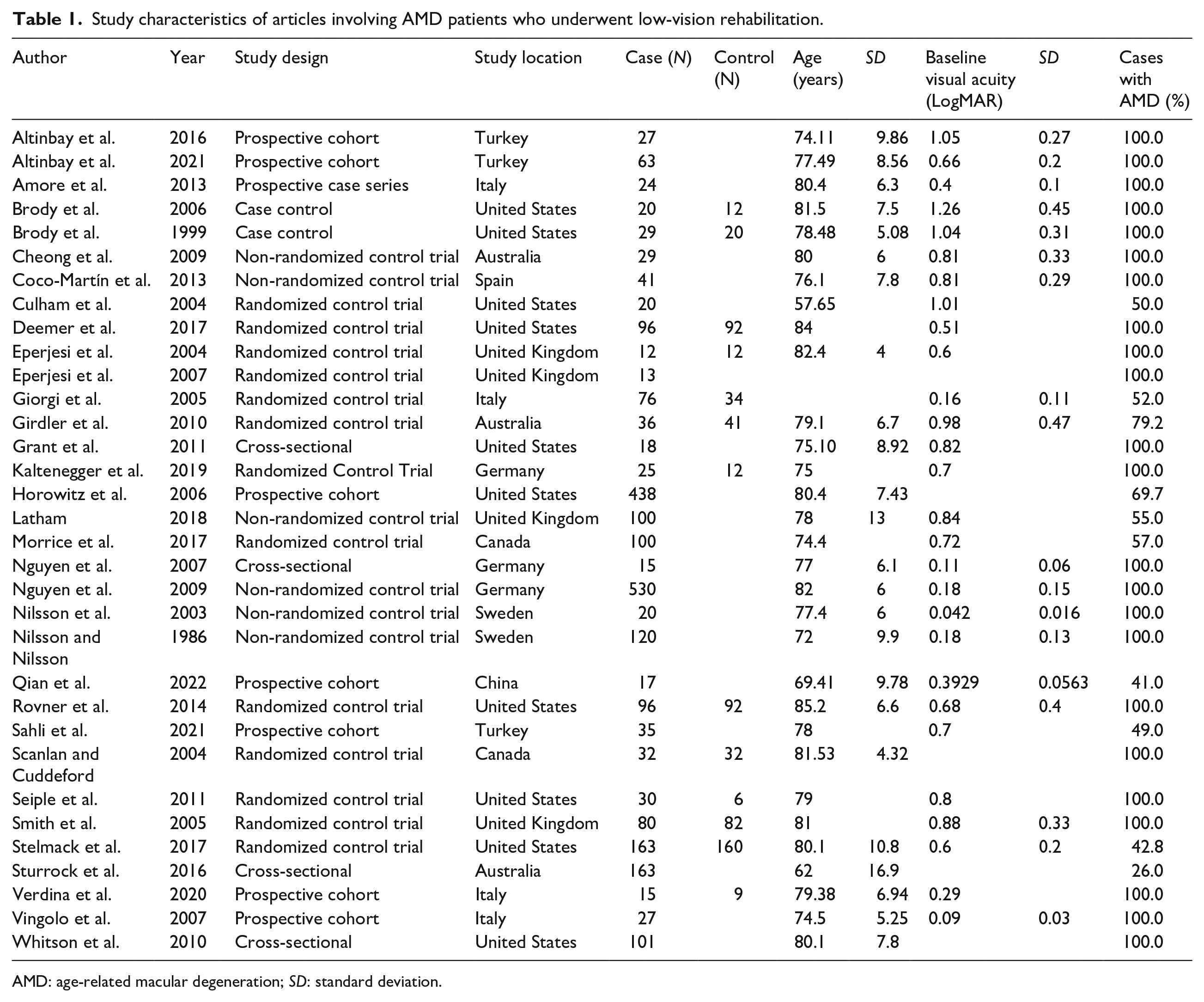
AMD: age-related macular degeneration; SD: standard deviation.
Statistical analysis
The meta-analysis employed STATA 14.0 software (STATA Corporation, College Station, TX) to calculate the effect size or treatment effect as proportions. Heterogeneity among studies was assessed using the I2 value, indicating the proportion of variation across studies attributed to heterogeneity rather than chance. The chi-square test determined if observed differences between studies were due to chance alone. Heterogeneity presence was indicated by a low p-value and a large chi-square statistic relative to its degree of freedom. Fixed-effect or random-effect models were selected based on the level of heterogeneity. Forest plots and funnel plots were utilized for visualizing results and identifying potential publication bias.
Results
Search results
After removing duplicates, searches of online databases and gray literature yielded 783 results. Following title and abstract screening, 666 articles were considered irrelevant, leaving 117 articles for full-text screening. From this, 33 articles were selected for data extraction. A total of 14 studies were included in the meta-analysis, while 20 studies underwent qualitative analysis, with no overlapping data between them. Excluded studies were either deemed irrelevant or did not meet the screening criteria. The Cohen’s kappa (κ) coefficient for abstract and title screening was 0.58, and for full-text screening, it was 0.59.
Study characteristics
Table 1 presents the demographic characteristics of 33 eligible articles (2611 subjects) investigating the impact of low-vision rehabilitation strategies on reading speed in words per minute (WPM) or depression. Of these studies, 14 (1123 subjects) were included in the quantitative analysis of low-vision rehabilitation effects on reading speed. The studies were conducted in various locations, including the United States, United Kingdom, Italy, Turkey, Germany, and Sweden. The sample size ranged from 12 (Eperjesi et al., 2004) to 530 (Nguyen et al., 2009). The mean ages reported in the studies varied from 57.65 (Culham et al., 2004) to 85 (Rovner et al., 2014), representing the targeted age group affected by AMD in this meta-analysis.
Effects of low-vision rehabilitation on reading speed
After low-vision rehabilitation, individuals with AMD demonstrated higher follow-up reading speeds compared to their baseline reading speed. The mean follow-up reading speed was 74 WPM, while the mean baseline reading speed was 58 WPM, resulting in a mean improvement of 15.5 WPM. Microperimeter biofeedback training was the most used low-vision rehabilitation technique, resulting in a mean improvement in reading speed of 15.2 WPM (Altinbay et al., 2021; Qian et al., 2022; Sahli et al., 2021; Vingolo et al., 2007). The largest improvement in reading speed was observed after eccentric viewing training, resulting in an increase of 59.3 WPM (Nilsson et al., 2003). However, not all interventions led to improvements in reading speeds (Culham et al., 2004; Seiple et al., 2011; Smith et al., 2005). The Flipperport (Electronic Head-Mounted, Low-Vision Device) performed the least favorable, leading to a decrease in reading speed of 15.2 WPM (Culham et al., 2004).
Effects of low-vision rehabilitation on depression scores
Table 2 presents studies examining depression in AMD patients undergoing low-vision rehabilitation and the employed depression assessment scales. Findings indicate that low-vision rehabilitation resulted in reduced depression symptoms and severity in AMD patients compared to control groups (Brody et al., 1999, 2006; Girdler et al., 2010). Moreover, follow-up assessments revealed decreased depression symptoms and severity in AMD patients following low-vision rehabilitation (Brody et al., 1999, 2006; Girdler et al., 2010; Horowitz et al., 2006; Kaltenegger et al., 2019).
Studies that investigate the effects of low-vision rehabilitation on depression at baseline compared to follow-up visits in AMD patients.
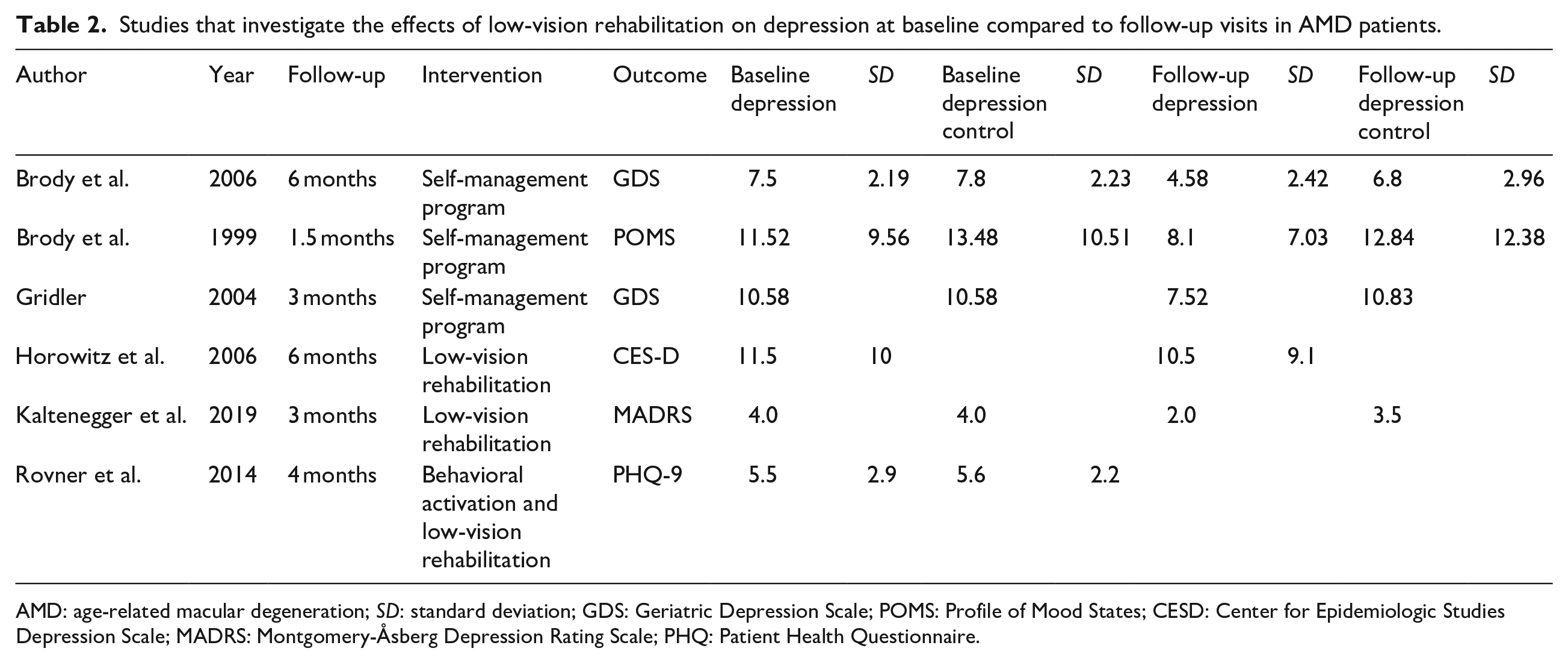
AMD: age-related macular degeneration; SD: standard deviation; GDS: Geriatric Depression Scale; POMS: Profile of Mood States; CESD: Center for Epidemiologic Studies Depression Scale; MADRS: Montgomery-Åsberg Depression Rating Scale; PHQ: Patient Health Questionnaire.
Assessment of study quality and publication bias
Using the Modified Downs and Black Checklist (Downs & Black, 1998), we evaluated the 33 studies included for this systematic review. Among these, 15 were high-quality, 17 were medium-quality, and only 1 was low-quality. Due to the limited availability of evidence, the lesser-quality articles were not excluded from the analysis. Appendix C provides details on the risk of bias assessment and publication bias.
Reading speed in AMD patients who received low-vision rehabilitation versus control group
Figure 2(a) indicates there was no significant heterogeneity (I2 = 33.2 p = .187) between studies comparing the control group, consisting of AMD patients who received no low-vision rehabilitation, versus the intervention group of AMD patients, who did receive low-vision rehabilitation. Studies reported a non-significant increase in reading speed (effect size [ES] = 0.02, 95% confidence interval [CI] = [−0.18, 0.23]) in AMD patients who received low-vision rehabilitation versus those who received no intervention.
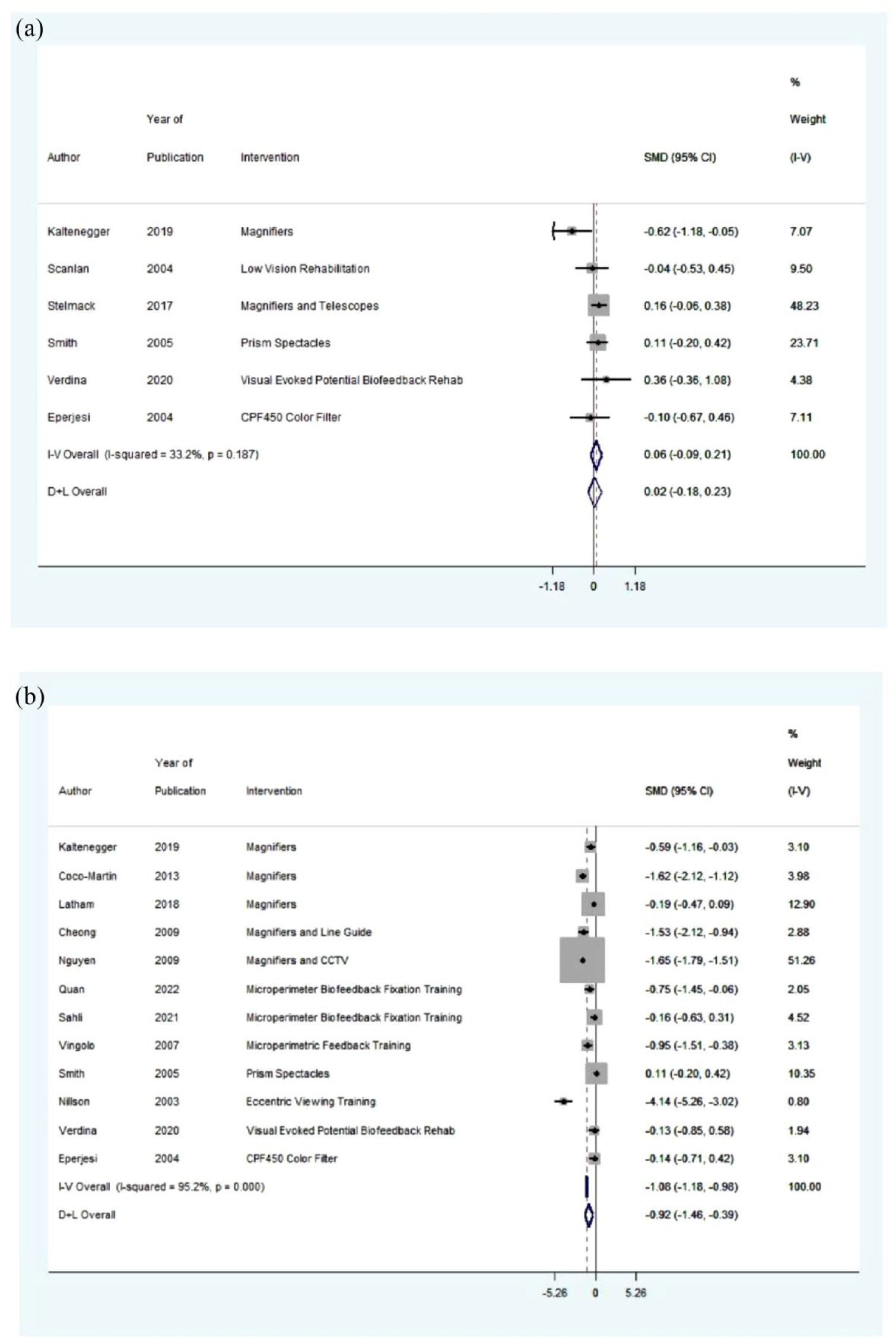
Forest plot for the included studies evaluating (a) reading speed in AMD patients who received low-vision rehabilitation versus those who did not and (b) reading speed in AMD patients from baseline versus follow-up.
Reading speed in AMD patients who received low-vision rehabilitation at baseline versus follow-up
Table 3 shows a variety of different low-vision rehabilitation strategies and the different reading tasks to measure reading speed. Figure 2(b) indicates there was significant heterogeneity (I2 = 95.2 p = .00) between the studies evaluating the difference in reading speed at baseline visits compared to follow-up visits in AMD patients who received low-vision rehabilitation. Studies reported lower reading speeds in baseline compared to follow-up (ES = −0.92, 95% CI = [−1.46, −0.39]) in AMD patients among the control groups. This result suggests that low-vision rehabilitation leads to improvements in reading speed in people with AMD.
Studies that investigate the effects of low-vision rehabilitation on reading speed in WPM at baseline compared to follow-up visits in AMD patients.
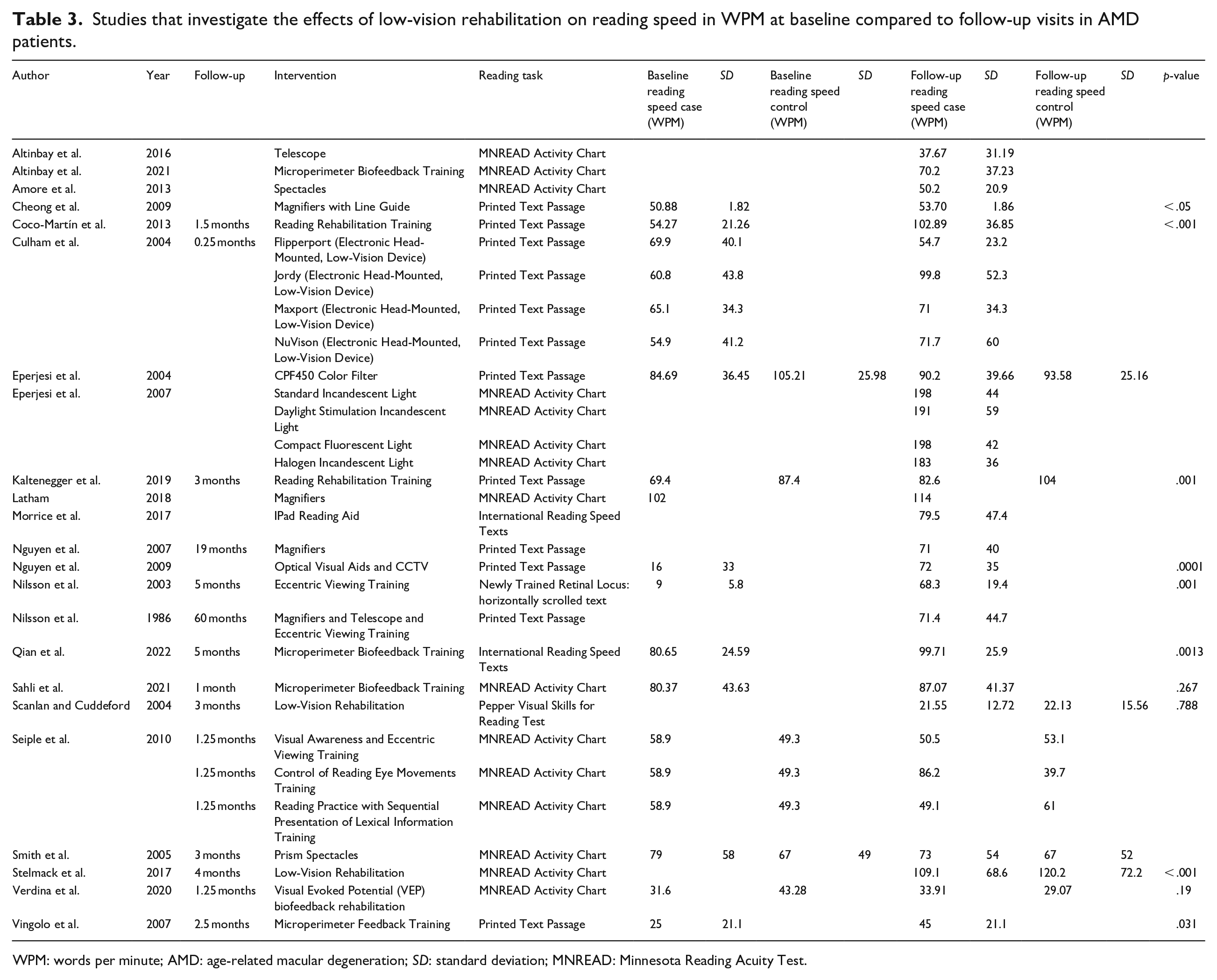
WPM: words per minute; AMD: age-related macular degeneration; SD: standard deviation; MNREAD: Minnesota Reading Acuity Test.
Publication bias
Figure 3 represents funnel plots for studies evaluating reading speed in AMD patients who received low-vision rehabilitation versus those who did not (see Figure 3(a)) and reading speed in AMD patients from baseline compared to follow-up, after receiving low-vision rehabilitation.
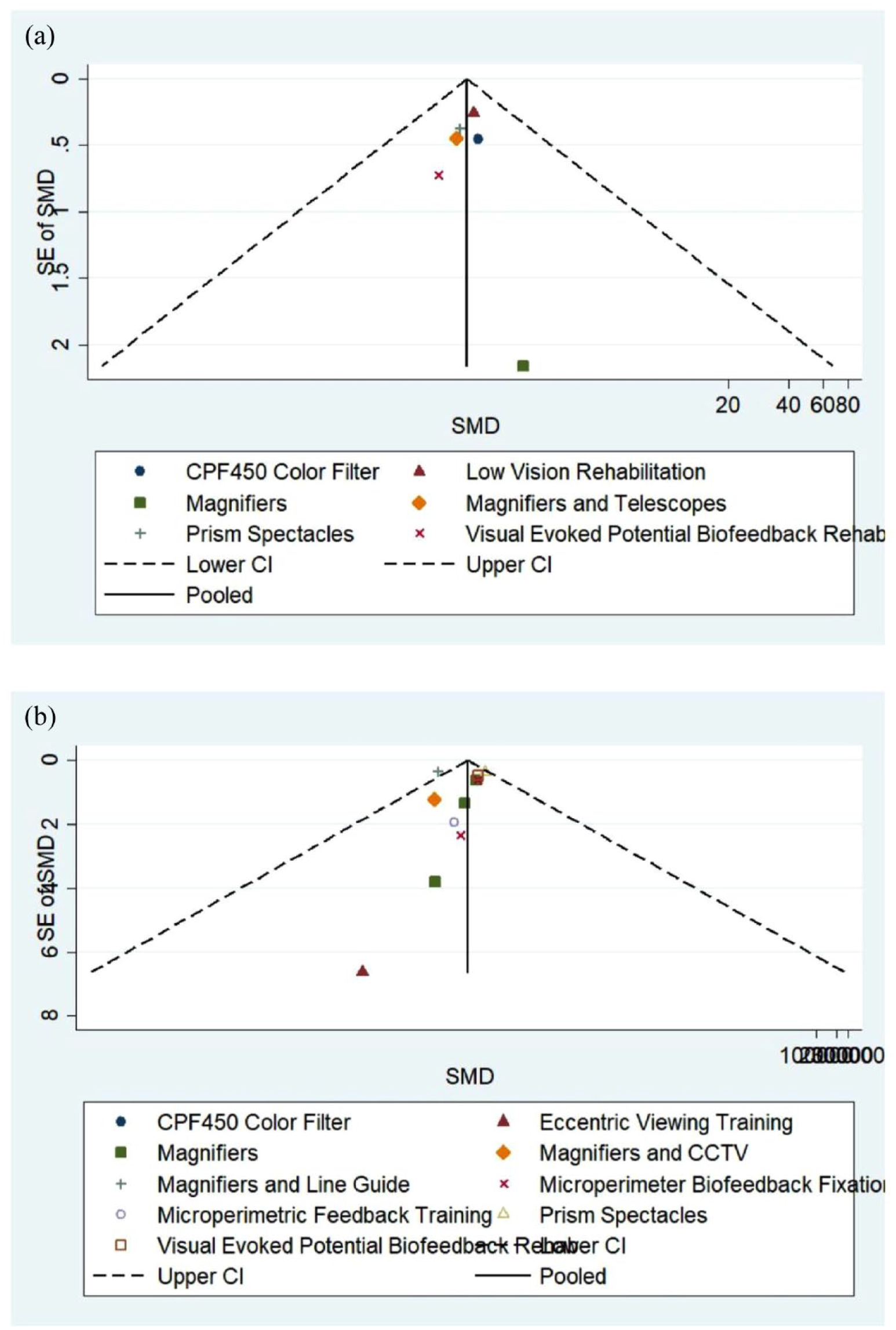
Funnel plot for the included studies evaluating (a) reading speed in AMD patients who received low-vision rehabilitation versus those who did not and (b) reading speed in AMD patients from baseline versus follow-up.
Both funnel plots have few studies at the bottom of the plot which implies that small studies with non-significant results may not be published. Visual inspection of the funnel plot did not reveal any asymmetry.
Discussion
This systematic review and meta-analysis examined the impact of low-vision rehabilitation on reading speed and depression in patients with AMD. A total of 33 articles involving 2611 subjects were included. On average, our findings revealed that low-vision rehabilitation led to an improvement in reading speed, with a mean increase of 15.5 WPM (see Table 3).
Our meta-analysis reported a non-significant increase in reading speed for AMD patients who received low-vision rehabilitation compared to those who did not (see Figure 2). We also found a significantly lower reading speed for AMD patients who received low-vision rehabilitation at baseline compared to follow-up visits (see Figure 2), indicating significant improvements in reading speed from baseline to follow-up.
Low-vision rehabilitation programs focus on training and employing adaptive strategies to optimize the remaining visual function in individuals with visual impairments (Stelmack et al., 2017). By employing personalized interventions, such as magnification devices, large print materials, and high-contrast lighting, AMD patients can significantly improve their reading speed and accuracy (Legge et al., 1992; Virgili et al., 2018). These interventions address the challenges that AMD patients face while reading, such as reduced visual acuity and contrast sensitivity. By enlarging the text and enhancing the contrast between the text and background, we can improve legibility and visibility for faster and more accurate reading (Crossland et al., 2014; Wolffsohn & Cochrane, 1999). The non-significant improvement is due to the heterogeneity among the studies. Factors contributing to this heterogeneity include variations in low-vision rehabilitation approaches, differing management strategies, variations in study populations, inconsistencies in program implementation facilities, differences in program management, varying follow-up durations, adherence rates, and program years. Further research is warranted to provide conclusive insights into identifying the optimal low-vision rehabilitation strategy.
Our results showed that low-vision rehabilitation improves depression in AMD patients (see Table 2). Interventions aimed at improving reading speed and functional vision in AMD patients can alleviate the psychological impact caused by vision loss and enhance their overall functionality (Stelmack et al., 2017). By restoring their ability to efficiently access and process written information, patients can perform work-related tasks more effectively, potentially boosting work productivity and enhancing their quality of life (Wolffsohn & Cochrane, 1999).
While our findings indicate that low-vision rehabilitation can increase reading speed for AMD patients, it does not delay the inevitable vision loss caused by AMD and its subsequent effects on reading speed (Bouwens et al., 2007; Owsley et al., 2009; Sunness et al., 2008).
Nonetheless, these results have important implications for ophthalmologists, as they highlight the value of integrating low-vision rehabilitation services into their practice. Low-vision rehabilitation equips patients with the necessary skills and strategies to make the most of their remaining vision, allowing them to be independent for their daily activities, including reading. By offering such services, ophthalmologists can provide comprehensive care for AMD patients and contribute to better long-term outcomes for this growing patient population.
This study presents several limitations. First, as all titles were accessed online, there may be a selection bias in the inclusion of specific studies. Second, the review only included studies published in English due to the authors’ language limitations. Despite this, the studies originated from various global locations, which should help reduce any potential bias arising from this language constraint. Third, the eligibility criteria restricted the number of studies included. The analysis only considered studies that provided data on reading speed and depression before and after low-vision rehabilitation. Furthermore, a meta-analysis of observational studies is prone to inherent biases present in individual articles. Factors such as income level, socioeconomic status, prior ocular and non-ocular surgeries, family history, other ocular and non-ocular conditions, pre-operative and post-operative medications, medication count, comorbidities, and so on may have affected the original studies’ estimates. Finally, the limited number of studies included and the high risk of bias in each study makes it challenging to reach definitive conclusions. Most included studies had a high risk of bias, primarily due to inadequate blinding and allocation concealment. Therefore, further studies with improved methodological quality examining the impact of low-vision rehabilitation strategies on reading speed and depression scores among AMD patients would offer better insight into the outcomes.
In summary, low-vision rehabilitation may enhance reading speed for individuals with AMD. However, it may not significantly impact depression scores in older adults with AMD. High-quality research is needed to study the effect of low-vision rehabilitation strategies on reading speed and depression scores in adults with AMD.
Supplemental Material
sj-docx-1-jvi-10.1177_02646196231217414 – Supplemental material for Effects of low-vision rehabilitation on reading speed and depression in age-related macular degeneration: A systematic review and meta-analysis
Supplemental material, sj-docx-1-jvi-10.1177_02646196231217414 for Effects of low-vision rehabilitation on reading speed and depression in age-related macular degeneration: A systematic review and meta-analysis by Edward Tran, Nirmit Shah, Riley Xu, Mohamed Aly and Monali S Malvankar-Mehta in British Journal of Visual Impairment
Supplemental Material
sj-docx-2-jvi-10.1177_02646196231217414 – Supplemental material for Effects of low-vision rehabilitation on reading speed and depression in age-related macular degeneration: A systematic review and meta-analysis
Supplemental material, sj-docx-2-jvi-10.1177_02646196231217414 for Effects of low-vision rehabilitation on reading speed and depression in age-related macular degeneration: A systematic review and meta-analysis by Edward Tran, Nirmit Shah, Riley Xu, Mohamed Aly and Monali S Malvankar-Mehta in British Journal of Visual Impairment
Supplemental Material
sj-xlsx-3-jvi-10.1177_02646196231217414 – Supplemental material for Effects of low-vision rehabilitation on reading speed and depression in age-related macular degeneration: A systematic review and meta-analysis
Supplemental material, sj-xlsx-3-jvi-10.1177_02646196231217414 for Effects of low-vision rehabilitation on reading speed and depression in age-related macular degeneration: A systematic review and meta-analysis by Edward Tran, Nirmit Shah, Riley Xu, Mohamed Aly and Monali S Malvankar-Mehta in British Journal of Visual Impairment
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funded by the Academic Medical Organization of Southwestern Ontario (AMOSO) Innovation Fund – 2019, Ref number: #INN20-020.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.