
Abstract
Despite effective vision rehabilitation (VR) interventions, no gold standard model of care delivery has been established. The institution of the South East Ontario Vision Rehabilitation Service (SOVRS) introduced a centralized intake, an occupational therapist as a systems navigator, and improved communication pathways between low vision services in order to optimize regional VR care. The aim of this study is to compare the SOVRS model of VR to a traditional, hospital-based pre-SOVRS-implementation model using referral data.
A single-site (Vision Rehabilitation Clinic at Kingston Health Sciences Center), retrospective medical chart review was performed. Data were gathered from the electronic medical records of patients who received a low vision assessment at the pre-SOVRS-implementation clinic (2017) and the SOVRS clinics (2019).
A total of 245 charts were reviewed over the two study periods. There were no significant differences in the age, gender, or diagnoses causing vision loss between 2017 and 2019. One hundred nine incoming referrals were received in 2017, with 136 in 2019, representing a 25% increase in incoming referrals (p < .001). The proportion of incoming referrals from non-ophthalmologists rose from 3.7% in 2017 to 31.9% in 2019 (p < .001). The number of outgoing referrals also increased significantly, from 113 outgoing referrals in 2017 to 259 in 2019 (p < .001), equivalent to a mean of 1.04 ± 0.68 (± standard deviation) outgoing referrals per incoming referral in 2017 and 1.90 ± 0.97 outgoing referrals per incoming referral in 2019. Outgoing service referrals also diversified significantly in 2019 (p < .001), with more referrals to services such as VR health service organizations and community services.
The SOVRS model was able to increase both the quantity and diversity of incoming and outgoing referrals by adopting several key strategies during its development. By expanding referrals, SOVRS increased the services available to patients and enabled a larger population to receive VR care.
Introduction
As the age of the Canadian population doubles over the next 25 years, and the proportion of patients with low vision grows in parallel, so too will the need for vision rehabilitation (VR) (Aljied et al., 2018; Statistics Canada, 2015). Low vision carries significantly elevated risk of falls, fractures, depression, and mortality (Klein et al., 1998; Senra et al., 2015; Zheng et al., 2012). VR offers the mainstay of care for patients with low vision, with interventions such as provision of assistive devices, strategies to enhance safety, environmental modifications, and supportive programs having demonstrated reductions in vision loss associated morbidity (Binns et al., 2012; Jian-Yu et al., 2020; Macnamara et al., 2021; Pijnacker et al., 2011; Stelmack et al., 2008, 2017; van der Aa et al., 2016; Zijlstra et al., 2013). Various health care authorities, including the World Health Organization, have reported on recommended VR interventions and preferred practise guidelines based on their demonstrated efficacy (Fontenot et al., 2018; World Health Organisation, 2015). Despite established interventions, no standard model of care delivery exists. Models of care can vary widely due to differing levels of eyecare provider training, funding, and resources (Ryan, 2014; van Nispen et al., 2020). These include community-based, hospital-based, primary care, and multidisciplinary models (Ryan, 2014; van Nispen et al., 2020).
The heterogeneity of VR models leads to variance in the types and availability of services. A scarcity of rehabilitation providers, inadequate insurance coverage of VR, and poor interdisciplinary communication have led to fragmented and underutilized VR services in Canada (Basilious et al., 2019; Gold et al., 2006; Mwilambwe et al., 2009). These gaps in service delivery have resulted in poor integration and coordination of services, no formal methods to transition patients between services, and poor awareness of VR services (Gold et al., 2006; Lam et al., 2015). This variance in the services offered given the differing models of care illustrates the importance of developing a strong, standard, community integrated model of VR.
Prior to 2018, the Vision Rehabilitation Clinic at Kingston Health Sciences Center (KHSC) utilized a traditional hospital-based model of VR. In this model, an ophthalmologist practicing Low VR independently performed low vision assessments (LVAs), and subsequently referred patients to community services such as Vision Loss Rehabilitation Ontario (VLRO). In an effort to overcome the barriers described above, a new service delivery model was introduced at the Vision Rehabilitation Clinic at KHSC. The South East Ontario Vision Rehabilitation Service (SOVRS) was established in 2018 with the goals of improving access, minimizing wait times, and increasing the speed and quality of service referrals. SOVRS is a partnership between the two primary providers of VR services, VLRO and the Vision Rehabilitation Clinic at KHSC, with support from the South East Local Health Integrated Network (SELHIN). SOVRS offers holistic, integrated, interprofessional care, that is centrally organized but regionally administered, a departure from the previous traditional hospital-based model. SOVRS introduced an occupational therapist as a systems navigator, who could both provide expert advice about locally available VR resources and perform thorough intake interviews for all patients prior to assessment by the ophthalmologist. In addition, a standardized referral form was created and a centralized intake system for all regional referrals was introduced to streamline the referral process. Regional satellite clinics were also established at different sites in the community to improve ease of access to care. Improved communication pathways between providers within SOVRS, such as systems to allow for sharing of patient information, were developed. Finally, SOVRS sought to educate regional referral sources through knowledge translation events.
As both the pre-SOVRS-implementation VR clinic and SOVRS offer care through assessment and subsequent referral to appropriate VR services, referral data can provide insight into the efficacy of the model and the range of services that patients were able to access. This study compares the SOVRS model of VR to the more traditional, hospital-based, pre-SOVRS-implementation model through the examination of incoming and outgoing referral data. The aim of this study was to determine if the change to the SOVRS model of care resulted in more comprehensive VR using referral patterns (quantity and diversity of referrals) as a surrogate marker.
Methods
This retrospective chart review was approved by the Health Sciences Research Ethics Board at Queen’s University (#6022546). All participants provided informed verbal consent to participant in this study. Data were gathered from the electronic medical records of patients who had a LVA at the pre-SOVRS-implementation VR clinic (1 January 2017 through 31 December 2017, immediately prior to the transition to SOVRS model) and at the SOVRS clinics (1 January 2019 through 31 December 2019, one year after the transition to SOVRS model). Referral data from 2018 were excluded as the services transitioned to the new model of care. Included patients met the following inclusion criteria: (1) the patient received a LVA at the KHSC Vision Rehabilitation Clinic during the specified date ranges and (2) the patient did not opt-out of research. One patient opted-out of research in 2019, and two patients opted-out in 2017.
Data from a random sample of 40 patients’ medical records were extracted by two authors to ensure agreement and consistency in data extraction. The complete data set was then extracted by one author. Information included demographics; age at the time of incoming referral, gender, date of the incoming referral and LVA; and diagnose(s) causing vision loss. Incoming referral information was extracted including the location and occupation of the referring clinician. For each incoming referral and subsequent LVA, all outgoing referral information was collected, including the total number of outgoing referrals, the types of services referred to, and the organization and occupation of individuals who would receive the referral. Outgoing referrals were further classified as formal referrals (a formal outgoing referral from the clinic was sent), informal referrals (a patient recommendation for services was provided), interprofessional collaboration (collaborative patient care was discussed between SOVRS and another agency), or knowledge transfer (a communication intended to educate the recipient about the status of the patient).
Statistical analysis
Statistics were performed in SPSS 27.0 (IBM Corp., Armonk, NY). The statistical analysis compared the 2017 (pre-SOVRS-implementation VR clinic) group to the 2019 (SOVRS) group. All categorical data are expressed as frequencies and percentages, while continuous data are described as means ± standard deviation or medians and quartiles. Categorical demographic data such as gender, diagnoses causing vision loss, profession of incoming/outgoing referral, location of incoming/outgoing referral, type of service referral, and classification of outgoing referral were analyzed using Pearson chi-square tests for statistical comparisons between the groups. Scale data including age and total number of outgoing referrals were analyzed using Mann–Whitney U tests. Normality of the scale data were assessed using with the Kolmogorov–Smirnov test. Values of p ⩽ .05 were considered statistically significant, and no adjustments were made for multiple comparisons.
Results
A total of 245 charts were reviewed over the two study periods. During the 2017 period, 109 LVAs were performed and during the 2019 period, 136 LVAs were performed.
Patient demographics
There was no significant difference in age between the two time intervals, with a median age at time of referral of 81.0 (inter-quartile range [IQR] 67.5–87.0) in 2017 and 79.0 (IQR 62.0–86.75) in 2019, p = .315 (Mann–Whitney U). Age of patients had a strong negative skew (Kolmogorov–Smirnov). There were also no significant differences from 2017 to 2019 in gender or diagnoses causing vision loss (Pearson χ2; Table 1). Age-related macular degeneration made up the largest cause of vision loss, present in 59.6% of patients in 2017 and 58.1% in 2019, followed by glaucoma in 17.4% of patients in 2017 and 18.4% in 2019.
Demographic data of patients assessed at the Vision Rehabilitation Clinic at KHSC in 2017 (pre-SOVRS-implementation) and 2019 (SOVRS).
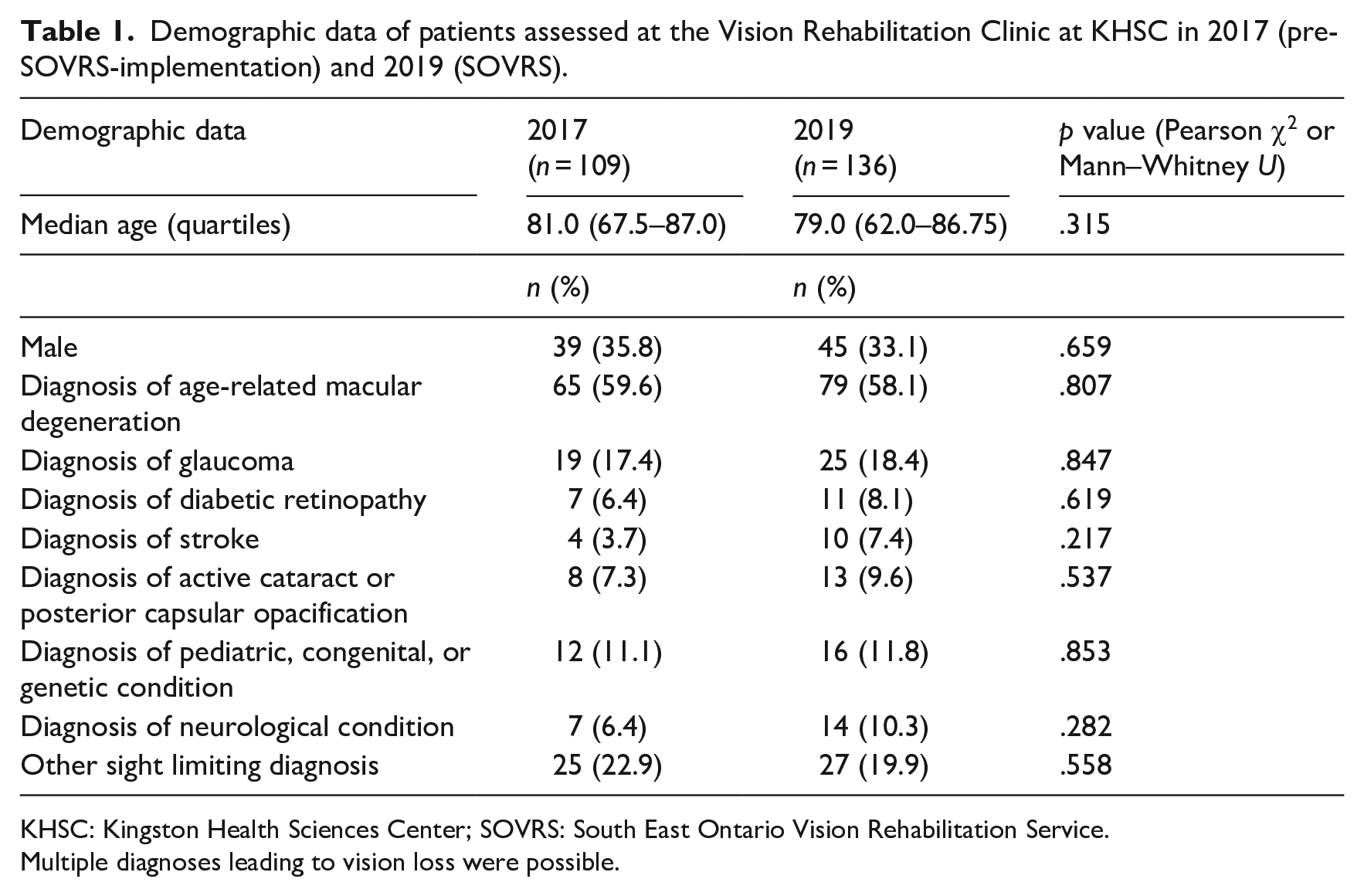
KHSC: Kingston Health Sciences Center; SOVRS: South East Ontario Vision Rehabilitation Service.
Multiple diagnoses leading to vision loss were possible.
Incoming referrals
A total of 245 LVAs were conducted at the VR clinic at KHSC, with 109 in 2017 and 136 in 2019, representing a 25% increase in total LVAs, p < .001 (Mann–Whitney U). Four of the associated referrals were received from outside of Kingston in 2017, growing to 16 in 2019, p = .024 (Pearson χ2). In 2017, the majority of associated referrals were from ophthalmologists within KHSC, with the referral network widening to include community partners, community physicians, and other regional hospitals in 2019. The proportion of incoming referrals from non-ophthalmologists rose from 3.7% (7) in 2017 to 31.9% in 2019 (43), p < .001 (Pearson χ2). This statistically significant increase can largely be attributed to the 6.6 times increase in referrals from optometrists, from 5 to 33, p < .001 (Pearson χ2). Other sources of increasing non-ophthalmologist referrals were family physicians and occupational therapists. Note that the location of incoming/outgoing referrals were not recorded in two 2017 charts, and profession data were not recorded in two 2017 charts and one 2019 chart.
Outgoing referrals
The number of outgoing referrals increased significantly, from 113 outgoing referrals in 2017 to 259 in 2019, p < .001 (Mann–Whitney U). For each incoming referral in 2017, there was a mean of 1.04 ± 0.68 outgoing referrals (median of 1), a value that nearly doubled to 1.90 ± 0.97 outgoing referrals per incoming referral in 2019 (median of 2), p < .001 (Mann–Whitney U). The outgoing referrals were organized according to the type of service referred to, such as VR health service organizations (typically referral to VLRO), community services (peer support programming or volunteer services), mental health care, ophthalmology care, transportation, and more (Table 2). There was a highly significant difference in services referred to between years, p < .001 (Pearson χ2); the diversity of referrals expanded in 2019, with more referrals to non-VR services such as mental health care, financial, workplace, or job support, allied health care, and community services (Figure 1). The relative proportion of referrals to health service organizations decreased due to a much larger increase in all other referrals (Table 2). However, despite making up a smaller proportion of referrals, the number of referrals to VR health service organizations increased from 0.66 per patient in 2017 to 0.95 per patient in 2019.
Classification of services in Vision Rehabilitation Clinic at KHSC outgoing referrals in 2017 (pre-SOVRS-implementation) and 2019 (SOVRS).
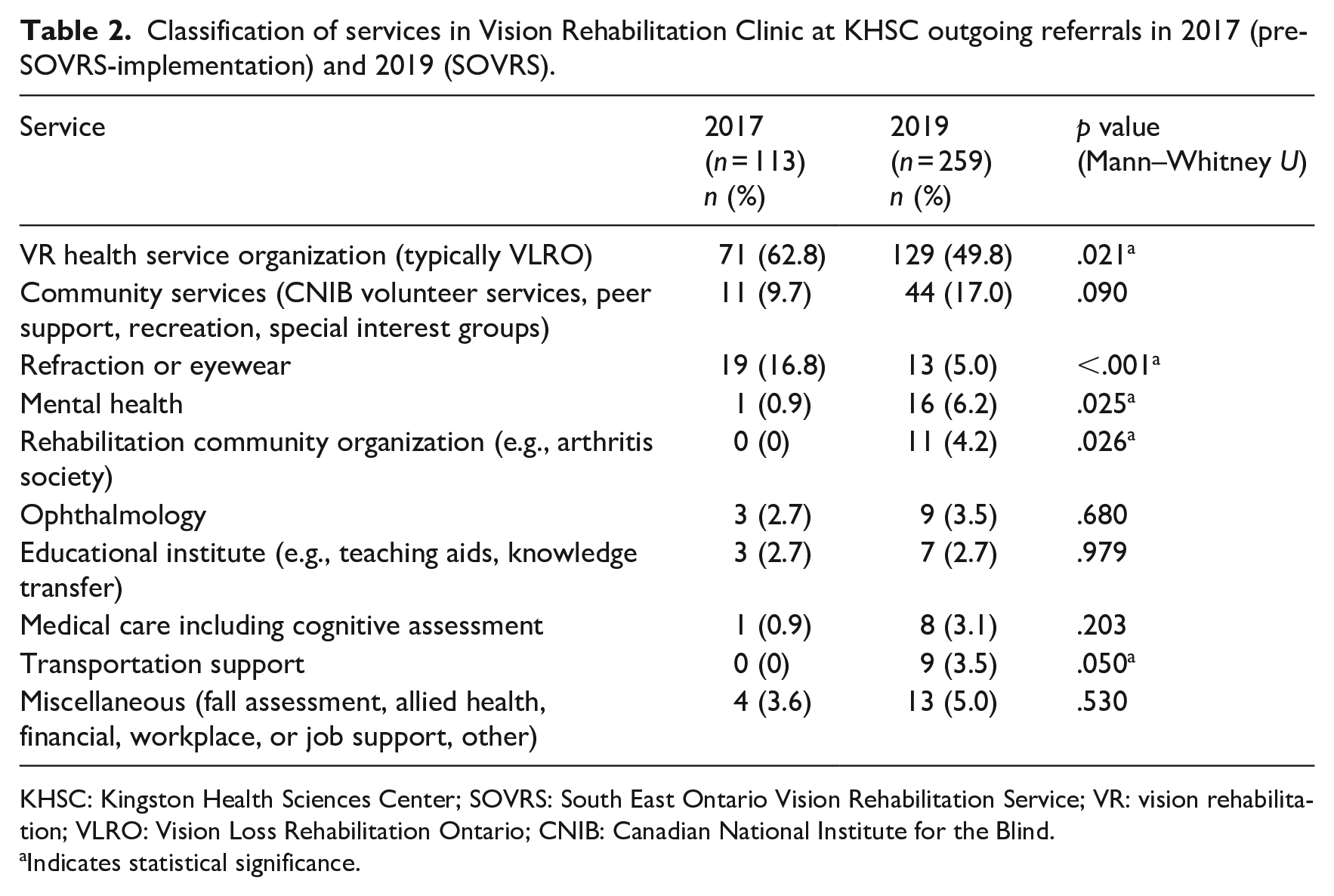
KHSC: Kingston Health Sciences Center; SOVRS: South East Ontario Vision Rehabilitation Service; VR: vision rehabilitation; VLRO: Vision Loss Rehabilitation Ontario; CNIB: Canadian National Institute for the Blind.
Indicates statistical significance.
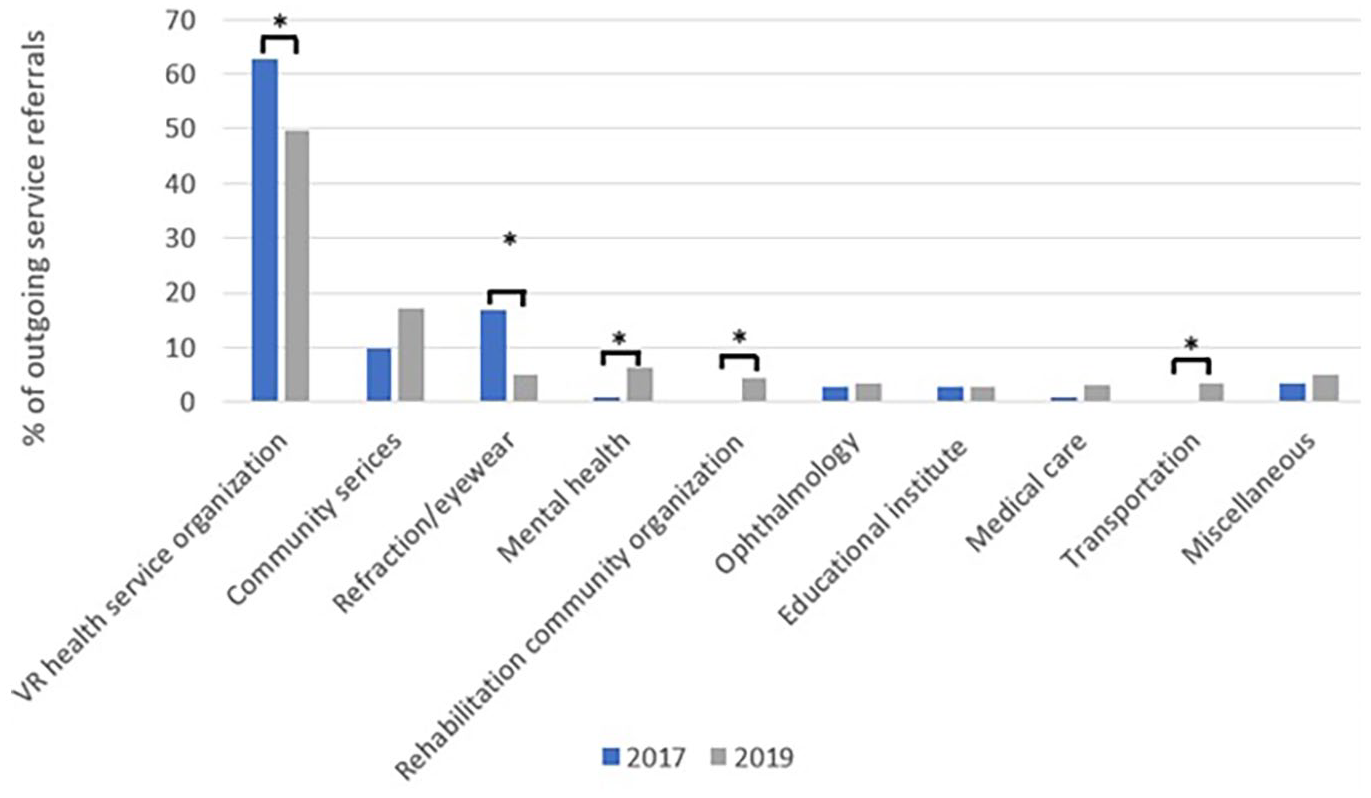
Percentages of outgoing service referrals from the VR clinic at KHSC in 2017 (pre-SOVRS-implementation) and 2019 (SOVRS).
Similar to the increased diversity of services in outgoing referrals, there was a statistically significant increase in the diversity of the professions receiving outgoing referrals between 2017 and 2019, p < .001 (Pearson χ2; Table 3). A higher proportion of 2019 referrals were to VR specialists, family physicians, and community organizations (including local volunteer services; Figure 2). Despite an increase in the quantity of each type of referral, there was no significant difference in the characterization of referrals as formal, informal, interprofessional collaboration, or knowledge transfer referral, p = .726 (Pearson χ2). In both years, 81% of referrals were formal and 16% were informal. Knowledge transfer referrals decreased from 4% of total referrals in 2017 to 2% in 2019, while interprofessional collaboration grew from 0% to 1% of total referrals.
Professions receiving outgoing referrals in 2017 (pre-SOVRS-implementation) and 2019 (SOVRS).
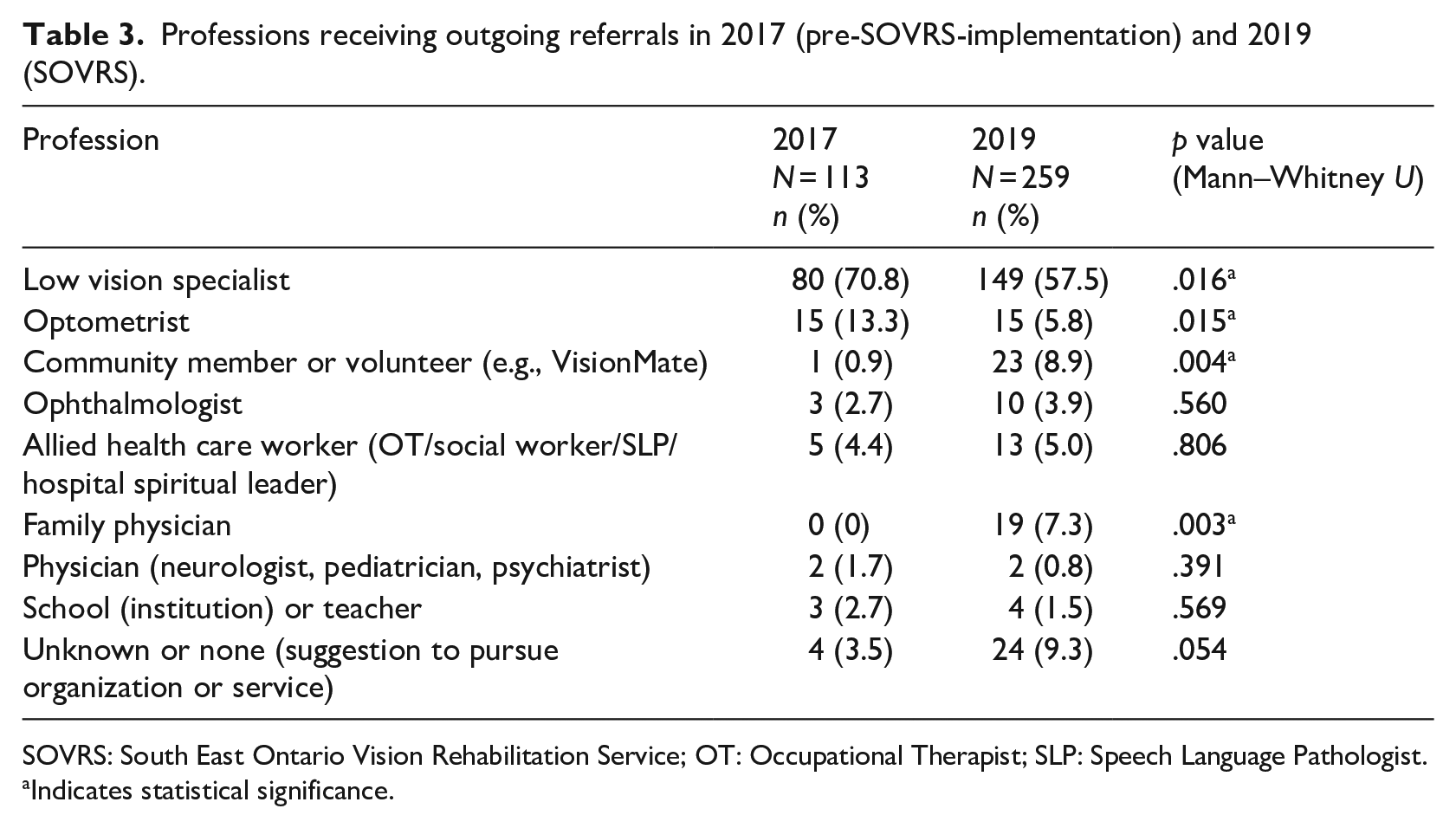
SOVRS: South East Ontario Vision Rehabilitation Service; OT: Occupational Therapist; SLP: Speech Language Pathologist.
Indicates statistical significance.
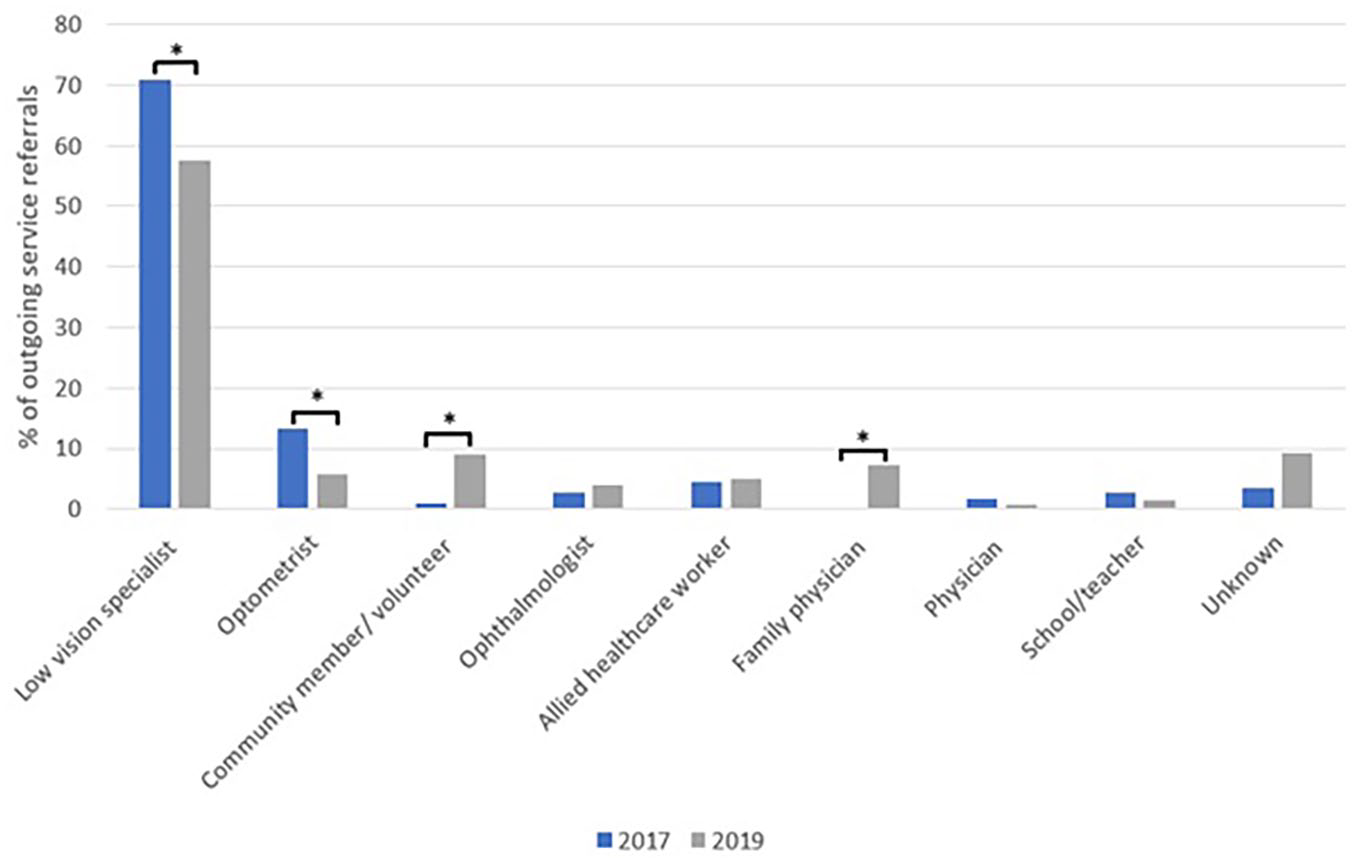
Profession receiving outgoing service referrals from the VR clinic at KHSC in 2017 (pre-SOVRS-implementation) and 2019 (SOVRS).
Discussion
The SOVRS model of VR iterates on hospital-based care delivery, with a focus on developing relationships with community organizations and personalization of care, with promising preliminary results. Once patients access SOVRS, referrals to rehabilitation or external services could be provided at any point during their journey; during triage, the intake interview, the LVA, follow-up appointments, or any subsequent communications between the health care team, the patient, or other care providers. Implementation of the SOVRS model increased the quantity of both incoming and outgoing referrals, and the diversity of outgoing patient service referrals. Despite the demonstrated efficacy of VR, no definitive model of service delivery has emerged (Lim et al., 2014). A 2020 Cochrane Review by van Nispen et al. detailed a large spectrum of effective care delivery models, including hospital-based, outpatient, community-based, and integrated multidisciplinary VR, with some unique models, including one that sought to train family member as caregivers (van Nispen et al., 2020). The SOVRS model has promising preliminary results, and should be further evaluated for consideration as an effective care delivery model.
Patients who access VR often require complex care, with multiple comorbidities, vision loss, hearing loss, and other lifestyle factors affecting their well-being (Aljied et al., 2018). Furthermore, significant barriers in access to care exist such as transportation for patients in rural areas, regionally limited services, and high costs of care (Gold et al., 2006). All of these factors must be considered by a VR team seeking to improve function associated with vision loss, which can be best addressed by holistic patient assessment and a multidisciplinary team (World Health Organisation, 2015). In addition, referral to VR services requires a comprehensive understanding of the services a patient is able to access in their community (World Health Organisation, 2015). With the introduction of an occupational therapist as a systems navigator in the SOVRS model, the clinic was empowered to better understand the complex needs of patients, and subsequently refer to more appropriate community-based services. This leads, in part, to the significant increase in outgoing referrals seen in this study (113 in 2017 to 259 in 2019). Formal partnerships formed with organizations such as VLRO allowed for bidirectional sharing of patient health information resulting in better integrated VR care, while improved communication along the referral pathway facilitated more timely and informed service referrals. The in-depth intake interview with the systems navigator allowed for exploration of a patient’s complex needs and goals, enabling personalized goal setting and services referrals. This was reflected in both the increase in outgoing referrals and the diversity of outgoing referrals, with increased referrals to transportation services, community organizations, and mental health care that addressed the holistic needs of patients and not just needs directly related to vision loss.
Awareness of VR services among eyecare providers and low vision patients is a significant barrier to VR uptake (Lam et al., 2015). The 2011 Montreal Barriers Study identified that 13% of low vision participants were aware of VR services but chose not to access them, while 33% of participants were unaware of their existence (Overbury & Wittich, 2011). Efforts from the SOVRS team to educate regional referral sources through knowledge translation events were intended to ameliorate the lack of understanding and awareness of VR services and increase use. These efforts were effective, as the clinic conducted 109 LVAs after incoming referrals in 2017 which grew to 136 LVAs after incoming referrals in 2019. Referrals were also received from a broader geographical area, allowing more individuals the opportunity to access VR. As optometry maintains the most regular contact with patients, education of this population could be a high yield route to identify patients with significant vision loss and refer for LVA. This is supported by the fact that our study demonstrated an increase of over 25% in incoming referrals from optometrists after the introduction of the SOVRS model. VR clinics should seek to build relationships with local health care and eyecare to support appropriate referral to VR services when required.
Comparison between different models of VR delivery can be challenging, particularly given the lack of a unified marker that can be used for comparison. Most VR services are multidisciplinary, specific to a community, and lack a centralized patient tracking system, making comparison challenging. However, a common feature of most VR models is the referral of patients with limited on-site provision of VR services. Referral data should be considered as a surrogate marker for service provision as it circumvents differences in care delivery and could be considered analogous to the out-of-clinic services a patient receives. Circumventing heterogeneity could allow for comparison between models and support stronger study of care delivery within VR.
This study has two notable limitations. The first is that there is no way to ensure that patients received a service when using referrals as a surrogate marker. This is particularly challenging for informal referrals, where it was assumed that the patient would follow-up independently to receive a service. The second limitation is the assumption that increased number and diversity of referrals will lead to better patient care; no outcomes such as fall reduction, mental health, or reading ability were examined in this study. However, examining outcomes following the change of VR model presents an opportunity for future study. In addition, the SOVRS model could be compared to other models using patient referrals as a surrogate marker for care provision; both the types of services that patients receive and the model’s impact on outcomes are worth considering.
Conclusion
The SOVRS model of VR included the implementation of a centralized intake system for all regional referrals, an occupational therapist as a systems navigator, and knowledge translation events for regional providers within the circle of care. This novel model of VR led to an increased quantity of both incoming and outgoing patient referrals. SOVRS also met a wider spectrum of patients’ complex needs through increased diversity of service referrals. Connecting patients with regional community support services and health service agencies is presumed to improve patient outcomes when compared to the previous hospital-based model of care. With the proportion of patients with low vision expected to grow significantly in the coming years, there is need to identify an effective model of VR, and a model that is feasible for implementation at other centers. Early study of the SOVRS model is promising and warrants further investigation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Presentations
The contents of this manuscript have not been presented at any meetings prior to submission.