
Abstract
Around 1.5 million Canadians live with some form of vision impairment. The demand for vision rehabilitation (VR) services is projected to increase as the number of older adults with age-related vision loss rises. To inform programmes and policies for VR, we aimed to answer two research questions: (1) How are VR services delivered in Canada? and (2) If gaps exist in current delivery of VR services, how can they be characterized? We used Arksey and O’Malley scoping review framework. A comprehensive search of five databases (PubMed, CINAHL/EBSCO, EMBASE, ProQuest, and Global Health) was performed during January 2019 and then updated in March 2021. Index terms and keywords relating to vision loss or impairment and rehabilitation were used. Non-peer-reviewed (grey) literature, in the form of reports and policies on VR in Canada, was sourced via Google/Google Scholar. To be included, sources had to (1) focus on VR services in Canada, (2) be available in English or French, and (3) be published after 2003. Data were extracted and analysed thematically to describe VR services across provinces and to identify gaps in service delivery in Canada. Out of 1311 studies identified, 62 were included. Findings indicate that the structure of VR services as well as provincial funding for assistive devices varies across provinces. The reported gaps at the level of service providers, users, and delivery systems were lack of awareness about the benefits of VR, limited collaboration and coordinated services between eye care and VR services, delayed referral to VR, shortage of specialists, and insufficient funding and training for vision devices. This article describes VR services in Canada and documents important gaps in VR services and research evidence across provincial jurisdictions. Future work to address gaps, and develop and evaluate interventions to facilitate optimal VR services is imperative.
Vision loss, defined as uncorrectable, partial, or complete impairment of vision, is an important public health concern (World Health Organization [WHO], 2019), with the demand for vision care and rehabilitation projected to rise alongside an increasingly older population with associated age-related eye conditions (Gresset, 2005; National Coalition for Vision Health, 2010). Vision loss now affects over 1.5 million Canadians (Morris et al., 2018), and almost 3.43 million more are at high risk of vision loss due to age-related eye conditions – age-related macular degeneration, cataract, diabetic retinopathy, and glaucoma (Access Economics Pty Limited, 2009). Two recent studies using the data from the 2016 Canadian Longitudinal Study on Aging reported that the prevalence of vision loss was 5.7% in Canadians aged 45–85 years (Aljied et al., 2018), and that 4 million Canadians had at least mild vision loss (logMAR ⩾0.2) (Mick et al., 2021).
Vision loss has profound effects on individuals’ daily functioning and community participation and poses serious implications for health and social care systems (Pérès et al., 2017; WHO, 2019). At an individual level, vision loss is associated with increased risk of depression, social isolation, unemployment, restricted mobility, falls, injuries, medication errors, early placement in long-term care homes, and even mortality (Meyniel et al., 2017; National Coalition for Vision Health, 2010). These are associated with a projected annual cost of $30.3 billion in health and social care by 2032 (Access Economics Pty Limited, 2009; Cruess et al., 2011). However, evidence also suggests that vision rehabilitation (VR) interventions are cost effective, reducing both the impact of vision loss and the costs of care (Taylor et al., 2006). Given the potential cost savings and demographics of low vision and blindness in Canada, there is a need for adequate planning for VR resources (Gresset, 2005). Despite this evidence, VR is often overlooked in health care policies, and vision research is critically underfunded in Canada (Maberley et al., 2006; National Coalition for Vision Health, 2010).
Comprehensive VR refers to ‘a multidisciplinary endeavour that encompasses the full spectrum of a patient’s rehabilitation journey after vision loss, from initial assessment through intensive rehabilitation therapy, laying the foundation for a healthy and independent life in the community’ (Gordon et al., 2015, p. 85). The WHO’s (2013) Global Eye Health Action Plan 2014–2019 explicitly refers to VR as an essential component of eye care and emphasizes its importance in mitigating the negative consequences of vision loss. The Government of Canada, as a signatory to WHO’s VISION 2020 and Global Eye Health Action Plan 2014–2019, has committed to the goal of ensuring universal access to comprehensive eye care and VR for all Canadians (Vision 2020 Canada, 2011; WHO, 2013).
While steps have been taken to improve VR services in Canada (Vision 2020 Canada, 2011), a comprehensive understanding of how services are structured and delivered across Canada is lacking. Hence, this study aimed to describe provincial and territorial VR services (the type of services and their funding arrangements) and uncover gaps in service delivery in Canada to inform future research and service development.
Methods
We conducted a scoping review using the methodological framework published by Arksey and O’Malley (2005) and subsequent recommendations by Tricco and colleagues (2018). The framework includes the following stages: identifying the research question; identifying relevant studies; selecting studies; charting the data; collating, summarizing, and reporting the results; and confirming results with stakeholders (optional). The final, optional step was not considered necessary, given that the research team included both VR providers and stakeholders. In addition, this team composition (providers and stakeholders) promoted an integrated knowledge translation approach to this study (Bowen & Graham, 2013). We used the PRISMA Extension for Scoping Reviews (PRISMA-ScR) to report results (Tricco et al., 2018).
Stage 1: identifying the research question
The questions guiding this review were developed in collaboration with staff of Vision Loss Rehabilitation Canada (VLRC). The research questions were as follows: (1) How are VR services delivered in Canada? and (2) If gaps exist in current VR services, how can they be characterized? While terms such as vision loss and low vision are often used to refer to uncorrectable impairment of the eye(s) or visual system, the authors chose to use the term vision loss because it includes both low vision and blindness. VR – rather than low-vision rehabilitation – is therefore used throughout the manuscript.
Stage 2: identifying relevant studies
A comprehensive search was performed in January 2019 and updated in March 2021. The search strategy was developed by the research team in consultation with a health science librarian. Five scientific databases were searched using index terms and keywords (Table 1) tailored to each database. We included peer-reviewed journal articles, editorials, and letters to the editor. We did not apply a language limit in our search strategy. Non-peer-reviewed (grey) literature was retrieved from Google and Google Scholar using the terms ‘low vision’, ‘vision loss rehabilitation’, and ‘readaptation en deficience visuelle’ in combination with ‘Canada’. The first 100 hits were screened to identify relevant reports and policies using a priori inclusion criteria.
Sources and search terms.
In addition, we searched through the online databases of the Canadian Journal of Ophthalmology and the Canadian Journal of Optometry published after 2003 to increase the likelihood of finding relevant articles in the Canadian context. These two journals were chosen because of their relevance to the field and the fact that not all of their content is indexed in scientific databases.
Finally, reference lists of the most relevant articles were reviewed to identify additional studies/documents. Sources were imported into the bibliographic manager Mendeley Desktop (2019) and duplicates removed.
Stage 3: study selection
The research team screened all titles/abstracts and then completed the full-text review of included sources. Two team members (S.S. and S.W.), who are proficient in French and in English, completed the screening and data extraction of articles/reports in French. To be included, the source had to: (1) focus on vision loss or low-vision rehabilitation services in Canada, (2) be available in English or French, and (3) be published after 2003, when Canada signed the WHO VISION 2020 declaration. Any doubts in selection were resolved in consultation with senior research team members (M.A.S. and D.K.). These team members monitored the overall screening process and provided input to ensure the search was thorough. The final list of identified sources was compiled in a Microsoft Excel (2017) spreadsheet for data charting.
Stage 4: data charting
Study details, including publication details, study location, design, population, focus, and key findings, pertinent to the research questions were extracted from included studies and entered into the spreadsheet. Data extracted from the grey literature included type of report, focus, and key recommendations.
Stage 5: data synthesis and reporting
Following data charting, the research team synthesized the findings, describing VR services across provincial jurisdictions in the form of tables and figures. Thematic analysis was used to identify and describe gaps in service delivery at the level of service providers, service users, and the service delivery system (Braun & Clarke, 2006).
Results
A total of 1311 sources were retrieved from the two searches, of which 62 met the inclusion criteria (Figure 1) (Moher et al., 2009). Findings are presented in three parts. First, characteristics of the included studies are described. Second, findings on VR services at national and provincial levels are presented. Finally, gaps in VR services in Canada are described.
PRISMA flowchart.
Characteristics of included sources
Of 62 sources, the majority (n = 51) were peer-reviewed, while the remainder were non-peer-reviewed reports and policy papers (n = 11). The source type and methodology of peer-reviewed papers are displayed in Figure 2, while Tables 2 and 3 summarize the included sources.
Types of sources.
Summary of peer-reviewed sources on vision rehabilitation in Canada (n = 51).
LVR: low-vision rehabilitation; VL: vision loss; VR: vision rehabilitation; AMD: age-related macular degeneration; RVF: Residual visual functions; LV: low vision; CNIB: Canadian National Institute for the Blind; SD: standard deviation; ADL: Activities of Daily Living; INLB: Institut Nazareth et Louis-Braille du CISSS de la Montérégie-Centre.
Summary of grey literature (policy reports) on vision rehabilitation in Canada (n = 11).
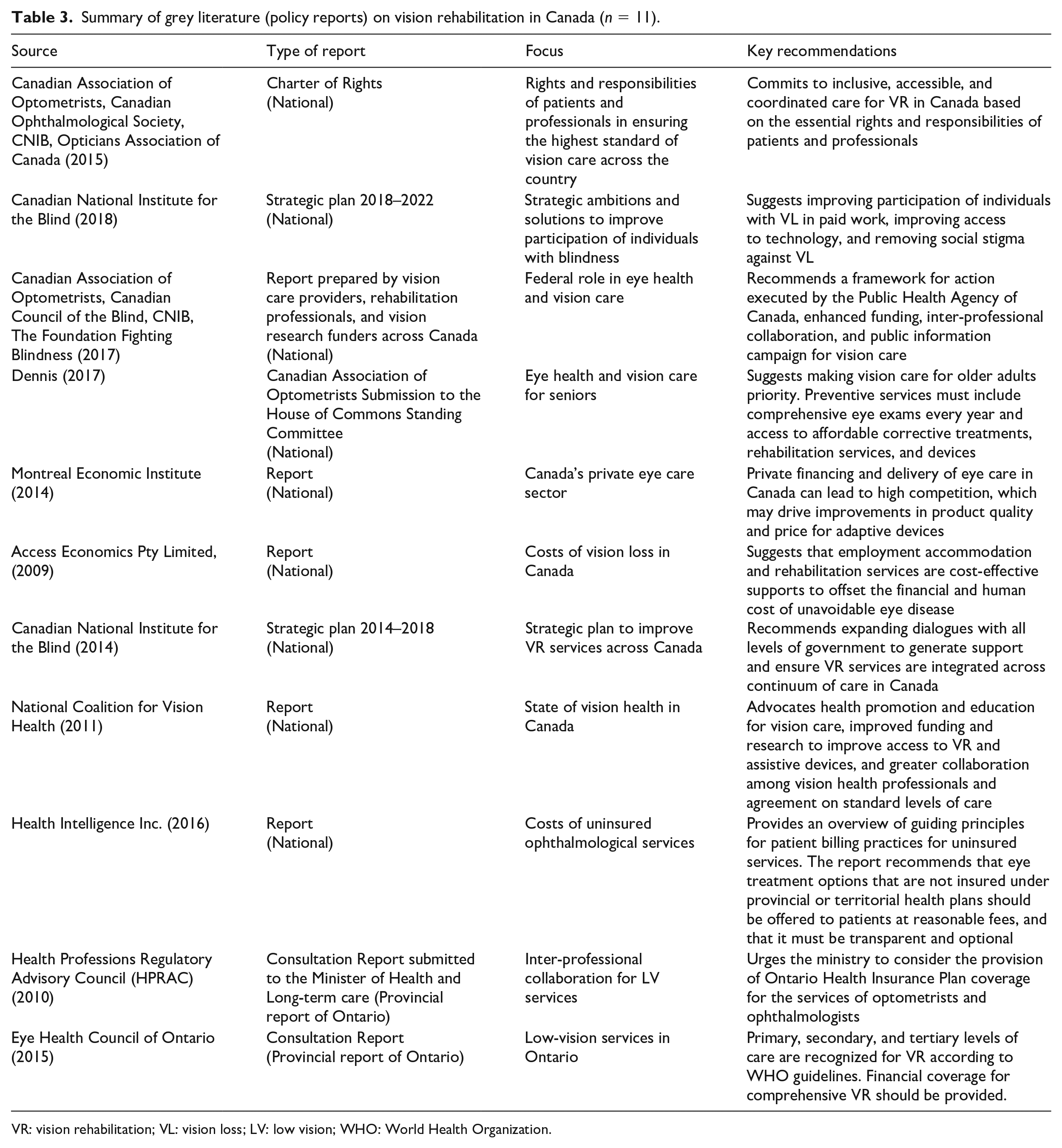
VR: vision rehabilitation; VL: vision loss; LV: low vision; WHO: World Health Organization.
Almost half of the sources were national in scope (n = 30), of which 21 were scientific publications while the other 9 were reports. The other 32 sources included were provincial studies and reports from Ontario (n = 9), Quebec (n = 19), Alberta (n = 2), and one each from Manitoba and Saskatchewan. Of the 62 sources, 18 were published in the last 5 years (2016–2021). Twenty of the 51 peer-reviewed sources involved patients with low vision or VR service users and focused primarily on the utilization, awareness, experiences, and barriers and enablers to VR service use. Eight sources examined the perspective of service providers and focused on the extent of or barriers to VR services. Nine sources discussed or proposed a model of VR services in Canada or discussed operational costs. Other sources (n = 18) focused on topics such as assistive technology, assessment tools, reading skills, service classification system, employment programmes, research in VR, and the role of occupational therapy in VR.
VR service delivery in Canada
The review shows that, in Canada, VR services are delivered in four settings. Each is described below.
VLRC
A number of studies identified the Canadian National Institute for the Blind (CNIB), a nation-wide, registered charity-based organization, as the largest vision loss rehabilitation service provider in the country for people of all ages with vision loss (Canadian National Institute for the Blind [CNIB], 2014; Eye Health Council of Ontario, 2015; Lapointe, 2006; Leat, 2016; M. Markowitz, 2006). VLRC is a health service organization spun out of the CNIB. Today, VLRC is primarily funded by provincial governments, though at the time of publication of most included sources, VLRC was a component of CNIB charitable services. Vision loss rehabilitation involves training in the use of sight enhancement and/or sight substitution skills, strategies, and assistive devices (Gordon et al., 2015, p. 85). This organization provides multidisciplinary vision loss rehabilitation services including functional vision assessments, eye disease education, counselling, essential skills for daily living, travel and mobility instruction, assistive technology services, and, in some provinces, early intervention for children and their families (VLRC, n.d.). Services provided by VLRC are nationwide (with limited service in Quebec) and vary from province to province depending on provincial funding.
University-based/affiliated VR centres
Some studies described VR services provided through university-based VR centres or low-vision clinics, typically located in either Ophthalmology or Optometry departments of University-affiliated teaching hospitals (see Table 4 for example). These VR services include some or all of the following services: vision loss assessment, prescribing of devices and training, fitting and dispensing of low-vision devices, orientation, mobility, and other functional training, and psychosocial support (Harper et al., 2006; Lapointe, 2006; Leat, 2016; Robillard & Overbury, 2006; Swift et al., 2021; Wittich et al., 2013). Services are provided through varying multidisciplinary teams that may include optometrists, ophthalmologists, opticians, low-vision specialists, orientation and mobility instructors, independent living skills instructors, counsellors, assistive technology support, psychologists, occupational therapists, and social workers, depending on the provincial regulations and funding arrangements (M. Markowitz, Daibert-Nido & Markowitz, 2018; Moore et al., 2015).
Province-specific vision rehabilitation services.
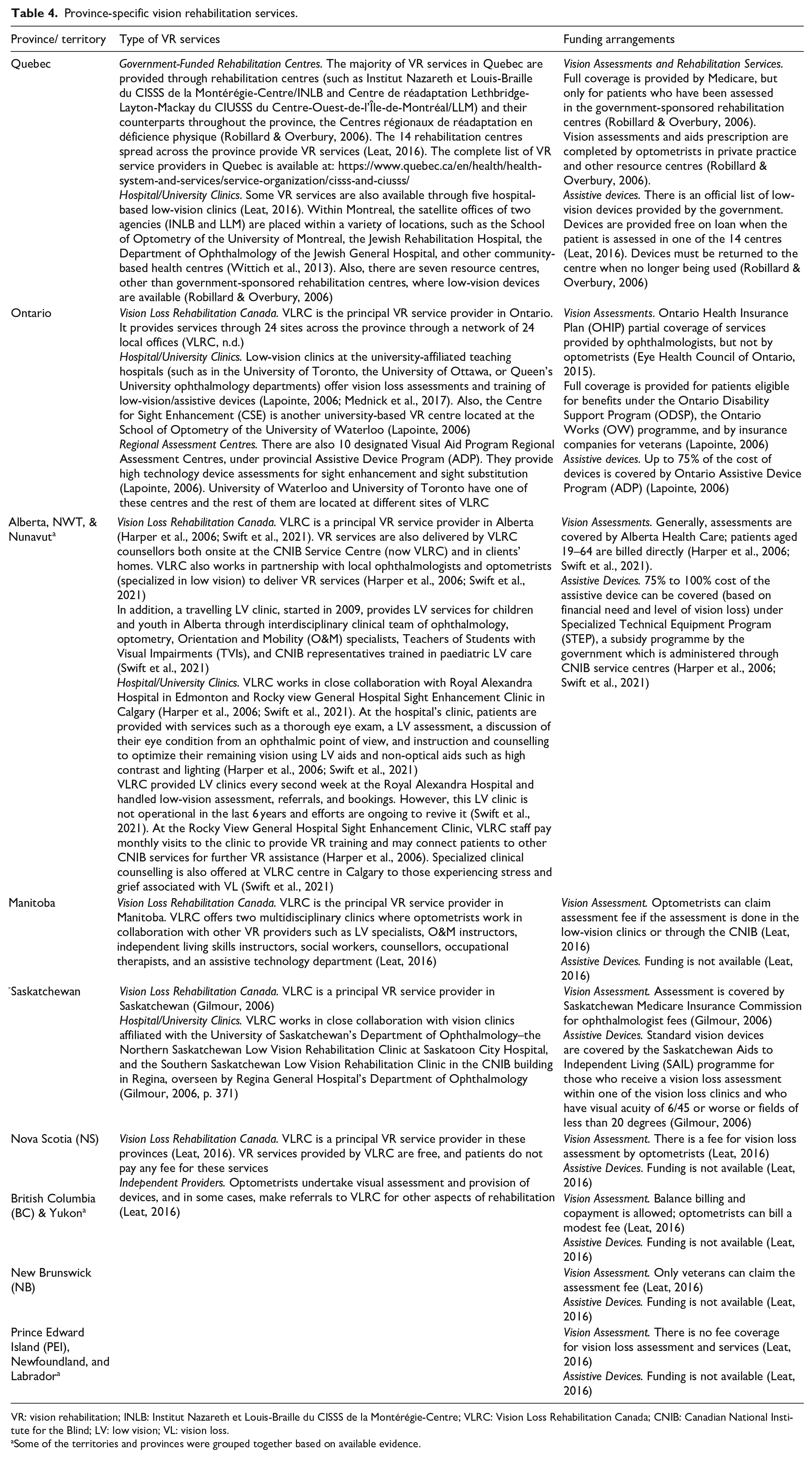
VR: vision rehabilitation; INLB: Institut Nazareth et Louis-Braille du CISSS de la Montérégie-Centre; VLRC: Vision Loss Rehabilitation Canada; CNIB: Canadian National Institute for the Blind; LV: low vision; VL: vision loss.
Some of the territories and provinces were grouped together based on available evidence.
Independent low-vision service providers
Reports from two professional organizations, one national (Dennis, 2017) and one provincial (Eye Health Council of Ontario, 2015), noted that optometrists and ophthalmologists, in conjunction with other rehabilitation professionals (often low-vision therapists or occupational therapists), provide VR services in their offices. These services mostly include assessment for and prescription of low-vision devices (Eye Health Council of Ontario, 2015).
Multidisciplinary rehabilitation centres
Specific to Quebec, VR services are provided through government-sponsored, multidisciplinary rehabilitation centres. There are 14 rehabilitation centres spread across the province to provide VR services (Leat, 2016). Services include multidisciplinary assessments and interventions, psychosocial support, computer and other technical aid assessment, procurement, and training, reading skills training (Duquette et al., 2014), braille and pre-braille lessons, prescriptions for optical aids (Moore et al., 2015), training with the use of implants (Moore & Wanet-Defalque, 2016), home adaptation assessments and interventions (for aids to daily living), and home care support services (Centre intégré de santé et de services sociaux de l’Outaouais, 2019).
Information on province-specific VR services (Table 4) suggests that VR services vary across Canada. Funding also varies from public funding, private funding, or a mix of public and private funding. Two studies (Leat, 2016; Swift et al., 2021) reported that VR services seem most comprehensive in Quebec, followed by Ontario, Alberta, Saskatchewan, and Manitoba (Table 4). Data for Table 4 were compiled from the 62 included studies and is not a comprehensive list of available public or private VR services.
Gaps in VR services in Canada
Gaps in VR provision highlighted in the literature have been grouped by service provider, service user, and system levels.
Gaps at the level of service providers
These included poor knowledge of VR services among eye care and other health professionals, lack of collaboration and coordinated services between eye care professionals and VR service providers, and delayed or no referral to VR. Of 51 peer-reviewed sources, 20 studies focused on the utilization, extent of, and barriers to VR service provision. Eight studies were from the perspective of eye care professionals and underscored a lack of awareness of or misconceptions about VR among eye care professionals and poor care coordination (Adam & Pickering, 2007; Basilious et al., 2019; Gold et al., 2006; Lam et al., 2015; Lam & Leat, 2013; Renaud et al., 2005). For example, a nationwide survey of 459 optometrists in Canada found that many who do not undertake low-vision assessment lacked education, experience, equipment, and devices specific to VR (Lam et al., 2015). These professionals stated that they found low-vision assessments time consuming and cost prohibitive. This is supported by findings of an earlier survey which concluded that only a modest proportion of optometrists perform comprehensive low-vision exams in Quebec (Renaud et al., 2005). Fraser et al. (2019) discussed the notion of stereotyping individuals with VL in a clinical setting that may lead to assumptions about the challenges and needs of the patient. These may differ significantly from the patient’s intended goals. A study of patients in Montreal also revealed that limited time of ophthalmic consultations and lack of effective communication with service providers were barriers to VLR (Southall & Wittich, 2012).
Timely referral to VR was also a common theme identified by service providers and patients. The Montreal Barriers study found that lack of or late referral by the eyecare professionals impeded older adults from obtaining VR services (Overbury & Wittich, 2011). A second study, investigating barriers to ideal referral practices in the Greater Toronto Area, characterized barriers as misconceptions regarding referral criteria and lack of knowledge of VR services among ophthalmologists (Adam & Pickering, 2007). Patients with vision loss have also expressed dissatisfaction with services and the lack of timely referral to appropriate VR services (Gresset et al., 2005; Lam & Leat, 2013; Nia & Markowitz, 2007; Robillard & Overbury, 2006). However, patient attitudes themselves also influence access to services. Using regression analysis (n = 749 patients with vision loss), Fraser et al. (2015) found that motivation to seek VR services decreased when duration of symptoms exceeded 9 years. After this time, individuals may have found compensatory strategies or habituated to impairment. Therefore, early referral to VR services may be important (Fraser et al., 2015).
Some studies recommended education of eyecare providers to overcome identified gaps. Education for optometrists and ophthalmologists emphasizing identification of clients in need and ideal time for referral to appropriate VR services was proposed in several studies (Adam & Pickering, 2007; Lam & Leat, 2013; Lam et al., 2015; Swift et al., 2021). Adam and Pickering (2007) argued that timely referral could be improved by assisting eye care professionals to focus on overall functional capacity rather than limiting decisions to poor visual acuity or decreased visual fields (Adam & Pickering, 2007). Another author emphasized that rehabilitation, focused on restoration of lost vision-related skills, should occur after optimal residual visual functions are achieved with optical devices (M. Markowitz, 2006). Increasing the number of ophthalmologists specialized in VR (Lapointe, 2006), incorporating aspects of VR into ophthalmology residency training, and providing refresher courses to practicing professionals (S. N. Markowitz, 2008) were also proposed. Fraser et al. (2019) suggested that clinicians be educated on the pitfalls of stereotyping patients with VL in clinical practice, including increasing self-awareness of attitudes and beliefs that can influence care provision.
Four studies emphasized the need for occupational therapy in VR (Gilmour, 2006; S. N. Markowitz, 2008; Simpson-Jones & Hunt, 2019; Yoo et al., 2020) as it improves participation in activities of daily living.
M. Markowitz, Daibert-Nido, and Markowitz (2018) suggested that guidelines for reading skills improvement be updated as several tools have been created in recent years that have not yet been incorporated into the recommendations for VR services. A meta-analysis suggested using VR strategies such as micro-perimetric biofeedback, eccentric viewing training, and microscopes teaching programmes to improve reading skills (Hamade et al., 2016). French-language adaptations of assessment tools have been created for standardized assessment between Anglophone and Francophone populations. Examples include the ECLec-DV tool for reading skills assessment (Duquette et al., 2012) and the MIDVAQ tool to measure the impact of VL and VR interventions on ability to carry out activities of daily living (Duquette et al., 2014).
Gaps at the level of service users
Twenty peer-reviewed studies focused on gaps in VR service at the level of service users or patients with vision loss. Lack of awareness, misconceptions, stigma, difficulty with diagnosis acceptance, and poor or delayed service use were key themes that emerged strongly from these studies. For example, a study in Quebec (n = 411 patients with vision loss) found that lack of perceived need for rehabilitation by patients, combined with stigma associated with seeking services for ‘the blind’, was a barrier to service use for older adults (Overbury & Wittich, 2011). Similarly, a survey with 29 ophthalmologists in Ontario indicated a belief that patients may be in denial or confused at the time of diagnosis and may fear being labelled as ‘blind’ because of associated stigma (Adam & Pickering, 2007). However, lack of perceived need is not always associated with stigma. Témisjian et al. (2013) found that general information on low-vision services was not readily available specifically for the Francophone population. Mwilambwe et al. (2009) revealed that patients (n = 448) with less severe visual acuity, but who qualified to receive low-vision services, were less likely to know about and have participated in VR services. Often, individuals with a VL diagnosis find it difficult to accept the diagnosis and must do their own research on available services or get help from a family member to obtain this information (Gresset et al., 2005). A review study on barriers to access VR from the patient’s perspective reported factors such as lack of awareness and misconceptions about VR services among patients, presence of comorbidities, level of education and income, and negative societal views and influence of family and friends play a critical role in access to VR (Lam & Leat, 2013).
To address these gaps, an Ontario study (Adam & Pickering, 2007) suggested that education of the general public could diminish stereotypes and stigma and motivate patients to educate their physicians, request referral, or refer themselves to a VR service. Other suggested solutions to improve utilization of VR services were to improve communication among caregivers about the consequences of vision loss and patient education about the benefits of VR services (Fraser et al., 2014; Jackson, 2006). Finally, counselling and peer support were proposed as ways to overcome the stigma related to vision loss and enhance the quality of life for those with vision loss (Harper et al., 2006).
Once VL services are sought, service providers are encouraged to promote device use and reduce barriers to participation for individuals with VL (Fraser et al., 2019). Given that the task of learning how to use new devices can be daunting, especially in the context of a new diagnosis, use of familiar tools is suggested. For example, Wittich and colleagues (2018) discussed adaptation of a tablet for use by person with low vision. Tablets and smart phones incorporated into mainstream use help to address client fears of being stigmatized.
Gaps at the system level
Gaps that were identified in both the peer-reviewed literature and institutional reports and policy papers included disparities in VR funding and services between provinces; shortage of specialists; inadequacy of insurance coverage; mounting costs of low-vision care; insufficient funding for and training with low-vision devices; outdated training programmes (M. Markowitz, Daibert-Nido, & Markowitz, 2018); the presence of a visual acuity threshold required to provide services (Témisjian et al., 2013); and the need for policies and guidelines on eye health or VR in Canada.
Institutional reports and policy papers specifically reported an insufficient number of VL service providers, inadequate financial coverage for VR assessment and training, outdated provincial assistive devices programme, deficiencies in current models of delivery, and a lack of established educational programmes on VR for occupational therapists (Canadian Association of Optometrists [CAO], Canadian Council of the Blind [CCB], CNIB, The Foundation Fighting Blindness [TFFB], 2017; Dennis, 2017; Eye Health Council of Ontario, 2015; Health Professions Regulatory Advisory Council, 2010; Montreal Economic Institute, 2014; National Coalition for Vision Health, 2010; Swift et al., 2021). A federal report published by the CNIB and other vision care associations highlighted the service gaps for certain populations in Canada, including the young, older adults, and Indigenous populations (National Coalition for Vision Health, 2010). It was found that technology, though having a promising role to benefit patients with VL, is often not available or used, for instance, Argus II retinal prosthesis in VR or use of technology for braille instruction to older clients (Markowitz et al., 2018; Martiniello et al., 2018).
Of particular note, peer-reviewed studies indicated that access to VR services is difficult for those living in rural and remote areas due to limited transportation, local availability, and distance from the VR care centres (Gilmour, 2006; Gold et al., 2006; Témisjian et al., 2013). For example, one study found that, in Ontario, the geographic distribution of ophthalmological services coincided with the largest patient populations, leaving many other regions of Ontario lacking services (Basilious et al., 2019). A national survey of service users and service providers in Canada underscored the disparities in VR care between rural and urban areas and among provinces, identifying disparities in the availability of, and funding for, services and aids (Gold et al., 2006). Lack of a comprehensive listing of VR services in Canada, particularly for rural communities, was also seen as a barrier to access (Jackson, 2006).
Suggestions to overcome system gaps were made across the included studies and reports. Comprehensive planning, adequate funding, proper classification system for operating costs for VR services, and involvement of all stakeholders are required to ensure province-specific service models meet the needs of those with vision loss (Coulmont et al., 2011; Harper et al., 2006; Roy et al., 2009; Swift et al., 2021). A recent review study from Alberta underscored the need for increased funding for the sustainability of VR programmes and better remuneration for community-based VR services considering the wide geographical distribution of patients across the province (Swift et al., 2021). This review, though limited to the province of Alberta, emphasized simplifying access to provincially subsidized vision devices and increasing multidisciplinary efforts to deliver VR (Swift et al., 2021).
A multidisciplinary team including eye care professionals and VR care providers with specialized counsellors, psychologists, occupational therapists, and social workers can help to address the specific needs of clients with vision loss (Gilmour, 2006; Simpson-Jones & Hunt, 2019). Gordon and colleagues (2015) suggested that ophthalmologists and optometrists should be involved in the assessment and initial VR, while specialized rehabilitation professionals should provide post-VR to restore patients’ independence. Similarly, provincial health coverage of optometric services and better communication with other eye care and VR service providers are suggested to provide better VR services (Lam et al., 2015). A study in Quebec evaluated an alternate referral pathway to VR services by placing an optometrist on a part-time basis within an ophthalmology department to provide VR care to clients (Wittich et al., 2013). Findings suggested that the addition of the optometrist may help triage patients with vision loss and facilitate the continuum of care (Wittich et al., 2013).
With respect to operating costs, several classification systems have been suggested to estimate operating costs for VR services in Quebec. These include a base cost for a given impairment, with additional costs based on functional status (Roy et al., 2009). Alternative systems primarily focus on the social or functional profile of the patient (Coulmont et al., 2011).
Two different models for comprehensive VR, both based on the WHO integrated model of VR care, were proposed for Canada: the SmartSight model, also referred to as the Canadian ophthalmology model of low vision (Jackson, 2006), and the three-tiered model for optometry (Leat, 2016, 2020). The ophthalmology-driven model involves four levels, with ophthalmologists identifying and responding to patients early in their eye disease trajectory (level 1 and 2). At level 3, in this model, ophthalmologists also provide basic and comprehensive low-vision evaluation, followed by rehabilitation with the involvement of other professionals at level 4. The second model, advocated by optometry, includes three levels: level 1 involves screening and triage, level 2 involves management of VI patients at a local optometry office, and level 3 involves comprehensive VR for patients with greater disabilities. Interestingly, we could not find studies where these models have been tested for their suitability, acceptance, and effectiveness within the Canadian context.
Discussion
The review shows that VR services in Canada are delivered via a combination of four service settings: VLRC sites, university-based centres, independent low-vision service providers, and, in Quebec, government-sponsored multidisciplinary rehabilitation centres. Overall, vision care in Canada is provided in a hybrid manner where assessments and prescription of vision aids are undertaken in the hospitals and rehabilitation is predominantly provided by community-based organizations (M. Markowitz, 2006; S. N. Markowitz 2016). Quebec is the exception, where rehabilitation is provided via government-funded rehabilitation centres.
Within the hybrid manner of service delivery, disparities exist across jurisdictions and urban and rural geographies. Variability in VR services exists in the type and volume of patients seen, practice patterns, and renumeration policies (M. Markowitz, Daibert-Nido, & Markowitz, 2018). This appears to be related to the availability of dedicated funding by provincial governments, type of assistive device programme available in the province, and proximity to academic centres of ophthalmology or optometry (M. Markowitz, Daibert-Nido, & Markowitz, 2018). It is also important to note that only a modest number of eye care professionals practice in the VR field due to the limited funding and resources necessary to provide VR services (Basilious et al., 2019; Gold et al., 2006; Lam et al., 2015; Renaud et al., 2005; Swift et al., 2021). Quebec-based studies in this review have underscored that VR resources, such as standardized tests in French language, were often not readily available for the Francophone population. In particular, the need for bilingual screening and assessment tools has been identified. Adaptations to widely used tools have been made; however, the available tools remain fewer than those available in English. In addition, more research is warranted for validation of these tools.
The present review highlighted the existing gaps in VR care at the level of service user, service providers, and the system including lack of collaboration and coordinated services between eye care and VR services, delayed referral to VR, shortage of specialists, and insufficient funding and training for low-vision devices. These gaps are consistent with findings from a previous study on VR elsewhere that also reported lack of awareness of available services, referral pathways and what they offer, misunderstandings by both practitioners and patients on the criteria to qualify for or benefit from VR services, miscommunication between practitioner and patients, and patients not identifying as someone experiencing need of VR (Luu et al., 2020). A review of barriers to accessing VR services from patient’s perspectives also presented similar findings and underscored the need for increased funding and education of patients, their families, and eyecare providers regarding effectiveness of VR services to overcome the service gaps (Lam & Leat, 2013).
Lack of a common definition and conceptual understanding of VR across Canada appears to contribute to gaps in VR service delivery. Although there was a joint effort in 2015 to put together a Canadian Charter of Vision Care that outlines the rights and responsibilities of patients and professionals in ensuring the highest standard of vision care in Canada, there is a lack of gold standard definition for VR that has been validated through research in the Canadian context (Gordon et al., 2015; S. N. Markowitz, 2016). The Eye Health Council of Ontario (2011) described VR from the perspectives of major stakeholders (ophthalmology, optometry, opticians, and CNIB). Later, the definition of ‘comprehensive vision rehabilitation’ as provided by a multidisciplinary panel was intended to foster a common understanding of VR care (Gordon et al., 2015). However, there remains a need to delineate the interface between VR and (medical) eye care professionals and services, and who should be the main point of contact to facilitate continuation with the rehabilitation care. This is not unique to Canada. At the international level, the lack of consensus about the standards and delivery models for VR services remains a challenge to standardization of services (S. N. Markowitz, 2016) and contributes to lack of proper referral patterns for VR across the globe (Luu et al., 2020; National Academies of Sciences, Engineering, and Medicine, 2016; Ryan, 2014).
Findings from this review support the idea for multidisciplinary teams to provide comprehensive rehabilitation care to those with vision loss in Canada. A multidisciplinary team may include opthalmologists, optometrists, opticians, low-vision specialists, orientation and mobility instructors, independent living skills instructors, counsellors, assistive technology support, psychologists, occupational therapists, and social workers. As highlighted in the Canadian Patient Charter for Vision Care (2015), successful comprehensive VR care is dependent on patients’ timely referral, access to the full spectrum of care from assessment to rehabilitation, and collaboration among rehabilitation professionals in the development of personalized VR therapy. Two different models proposed for comprehensive VR in Canada are the SmartSight model (Jackson, 2006) and the three-tiered model for optometry (Leat, 2016; 2020). The American Academy of Ophthalmology (AAO) included the SmartSight model in the United States Preferred Practice Pattern (AAO PPP) guidelines that is widely accepted by US and Canadian ophthalmologists to encourage appropriate referrals (S. N. Markowitz, 2016). The three-tiered model of optometry is adopted in the Low Vision Clinical Practice Guideline for Canadian Optometrists by the Canadian Association of Optometrists (Leat, 2020).
However, no further pilot or evaluation studies based on these models have been reported in the literature in the Canadian or US context. More efforts are needed to compare and validate these models on a province-by-province basis and examine their effectiveness in providing care to clients with vision loss (CAO, CCB, CNIB, TFFB, 2017; Eye Health Council of Ontario, 2015). Considering the existing ways in which VR services are currently delivered in Canada (CNIB/VLRC sites, university-based centres, and independent low-vision service providers, and multidisciplinary rehabilitation centres in Quebec), it is imperative to conduct implementation studies using the two proposed models to determine which service delivery model is best suited for each of the provincial jurisdictions.
Overall, the quantity of research evidence on VR is limited. Most studies were descriptive and/or qualitative and were focused on the provision of service delivery; only a few studies measured the effectiveness of service delivery. For example, a systematic review of VR for children reported lack of studies and limited evidence in the Canadian context that could inform clinical practice and policy decisions (Chavda et al., 2014). Within the included studies, there were only a few that discussed the VR service provision at a national level. Except for Ontario and Quebec, only a few studies included provinces of Alberta, Manitoba, and Saskatchewan while no studies were found for the other provinces and territories. However, it is important to note that lack of evidence does not mean that there are no VR services in these regions. Instead, there is a lack of published reports/studies that document the services and their effectiveness. This evidence gap could be attributed to the lack of prioritization of vision health on a population health agenda and lack of dedicated government funding for vision health and rehabilitation research in Canada (Access Economics Pty Limited, 2009; Dennis, 2017; National Coalition for Vision Health, 2010).
Two of the included studies in this review addressed the need for VR services for people with additional health-related conditions (Simpson-Jones & Hunt, 2019; Yoo et al., 2020). The Canadian Survey on Disability (CSD) (2017), a nation-wide survey of Canadians aged 15 and over who experience limitations in everyday activities, indicates that 85.70% (approximately 1.3 million) of Canadians with vision loss live with additional disabilities (CNIB, 2021). Particularly for aging Canadians with vision loss, the prevalence of co-morbid conditions is extremely high (>90%) and vision loss itself is a strong predictor of falls, cognitive decline, depression, mobility difficulties, injuries, and mortality (Meyniel et al., 2017). Interestingly, only a few studies examined or discussed VR services for those with vision loss in addition to other comorbidities such as those with brain injury (Simpson-Jones & Hunt, 2019; Yoo et al., 2020). This evidence gap may be the result of the fragmentation between VR (often delivered in the community) and other health care services and the consequent limitation in communication between providers in the health care and VR settings (National Academies of Sciences, Engineering, and Medicine, 2016). Nevertheless, the impact of comorbidities on the VR plan needs to be considered by service providers and supports the need for multidisciplinary and collaborative modes of care (Leat, 2020; Simpson-Jones & Hunt, 2019; Yoo et al., 2020).
Implications for research, policy, and practice
Based on gaps identified in this study, early referral to rehabilitation by eye care practitioners and better awareness among professionals and clients with vision loss about VR services are needed to improve referral patterns and timely access to care (Adam & Pickering, 2007; Basilious et al., 2019; Dennis, 2017; Gold et al., 2006; Lam et al., 2015; Mwilambwe et al., 2009; Overbury & Wittich, 2011). Research also suggests that access to care can be improved by better provincial health coverage of vision loss services including optometry and other VR services, and better communication between VR providers and consumers to facilitate access to VR services (Gold et al., 2006; Lam et al., 2015; Southall & Wittich, 2012).
A stronger research evidence base is needed to better understand the VR-specific needs of all Canadians and to reach a consensus on the most-suited service delivery model of VR that is equitable and accessible for all Canadians – regardless of age, class, gender, ethnicity, indigeneity, socio-economic status, geography, and other factors (National Collaborating Centre for Determinants of Health and National Collaborating Centre for Healthy Public Policy, 2016). This research needs to incorporate diversity in perspectives and socio-demographic characteristics of Canadians with vision loss to include under-represented groups and those with vision loss and comorbidities.
Limitations
One limitation of this study is its generalizability beyond Canada. A second limitation is that studies available in scientific databases other than those searched or material in the grey literature may have been omitted. The review, also, did not capture studies on VR among the veteran population as these services are provided separately from general health care services. Finally, although recommended, we did not confirm our study results with experts and other stakeholders, that is, stage 6 of scoping review. Doing this would have provided further validation to our findings.
Conclusion
This is the first review to systematically identify literature on VR in Canada, understand its current status, and identify gaps in service delivery to inform delivery of care and future research. Access to care is inconsistent in Canada and services are fragmented. To attain the goals of VR as outlined in the Canadian Patient Charter for Vision Care (2015), it is critical to overcome the service gaps by improving collaboration and communication among VR providers, and dedicating provincial government funding for services, including multidisciplinary team interventions to meet rehabilitation needs of Canadians with vision loss.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Two authors (M.A.S. and T.P.) have affiliation with the CNIB and/or Vision Loss Rehabilitation Canada.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Mitacs through the Mitacs Accelerate program.