
Abstract
Background:
Vision rehabilitation services are increasingly being delivered remotely (i.e., telerehabilitation); yet, limited research has explored practitioners’ attitudes towards this approach or considered the wider implications of re-designing services. This qualitative study investigates perspectives on delivering telerehabilitation among sight loss support organisations.
Methods:
Twelve participants from 9 sight loss charities in the United Kingdom took part in a semi-structured interview. Participants were professionals from large national rehabilitation service providers (n = 5), regional charities (n = 3), or local community organisations (n = 4). Qualitative data were analysed using thematic analysis.
Results:
Four themes were identified (1) Delivery of telerehabilitation; (2) Opportunities associated with telerehabilitation; (3) challenges associated with telerehabilitation; and (4) wider challenges in the vision rehabilitation sector. Greater utilisation of telerehabilitation was viewed positively; however, questions arose regarding cost-effectiveness and the appropriateness of this method of service delivery. Factors such as workforce decline, access to training, and understanding of vision rehabilitation were identified as wider problems affecting the future landscape of vision rehabilitation.
Conclusion:
Digital innovation has facilitated local and national organisations to provide largely successful and accessible telerehabilitation services. Wider challenges call for investment in strategies and policies to ensure people with visual impairment can continue to benefit from vision rehabilitation services.
Introduction
Vision rehabilitation is a key component in the eye care pathway wherein therapeutic or training interventions are used to reduce disability and optimise functioning in people with visual impairment. Interventions are traditionally aimed towards maintaining activities of daily living, safety, and social life to facilitate adaption to visual loss and prevent deterioration in the quality of life (Binns et al., 2012; Rees et al., 2010).
Growing demand for rehabilitation in the sight loss sector led to a range of health and social care policies being introduced to ease pressure on clinical services in the UK (Rabiee et al., 2016). The Care Act 2014 set out new responsibilities for local authorities concerning rehabilitation (Department of Health & Social Care, 2023), whereby registers of blind and partially sighted individuals were to be established and maintained, as well as planning the provision of services to meet needs for care and support. Under this new model, vision rehabilitation has extended beyond hospital-based low-vision services to include multidisciplinary programmes of support from charities, volunteers, local authorities, and in some cases, the private sector. Programmes are delivered in the community by a range of specialists such as technical instructors, social workers, and qualified therapists. A key role within the rehabilitation workforce is the ROVI (rehabilitation officer for the visually impaired), who is trained to work with people with visual impairment to assess their difficulties and areas of need and to identify solutions to enable an independent lifestyle as much as possible.
In the post-pandemic era, eye care providers have begun to embrace alternative strategies to vision rehabilitation, such as delivering services via remote and virtual approaches (i.e., telerehabilitation) (Aravich & Stants, 2022; Keilty et al., 2021; Patel et al., 2021:). Conventionally, for an individual to engage in vision rehabilitation would require a scheduled appointment in a face-to-face session; although new technology and innovation have increased opportunities to adopt telerehabilitation. Services may comprise a range of elements designed to assess, prevent, treat, educate, or counsel individuals living with chronic health conditions (Brennan et al., 2010). Our recent scoping review highlighted that charities and community organisations (i.e., third-sector organisations) had shifted aspects of their rehabilitation programmes virtually to continue supporting people living with visual impairment during the COVID-19 pandemic (Jones et al., 2022). For example, organisations reported using telerehabilitation for digital skills and assistive technology training, support with domestic and practical activities, well-being activities, physical exercise training, and telephone counselling. A recent systematic review identified only limited evidence to evaluate the benefits of vision telerehabilitation, calling for more studies to explore the potential for this approach in the sight loss sector (Bittner et al., 2023). In addition, little is known about how a rapid re-design and up-scaling of digital services has impacted the service provision from an organisational perspective. The aim of this study was to explore reflections on the changing landscape of delivering vision rehabilitation from charity organisations in the sight loss sector.
Methods
Study design
A qualitative study with professionals working in charities and organisations in the sight loss sector was undertaken. The study was conceptualised following a scoping review of telerehabilitation for people with visual impairment (Jones et al., 2022), which outlined the significant role of charities in delivering rehabilitation in practice; yet, highlighting a lack of research in this field. The study was approved as a service evaluation among sight loss services in the Visionary group (www.visionary.org.uk), a national membership organisation for local sight loss charities. The study adhered to the principles stated in the Declaration of Helsinki and informed consent was gained from each participant prior to the interview. The study was designed and reported following the guidance of the Consolidated Criteria for Reporting Qualitative Research (Tong et al., 2007).
Participants
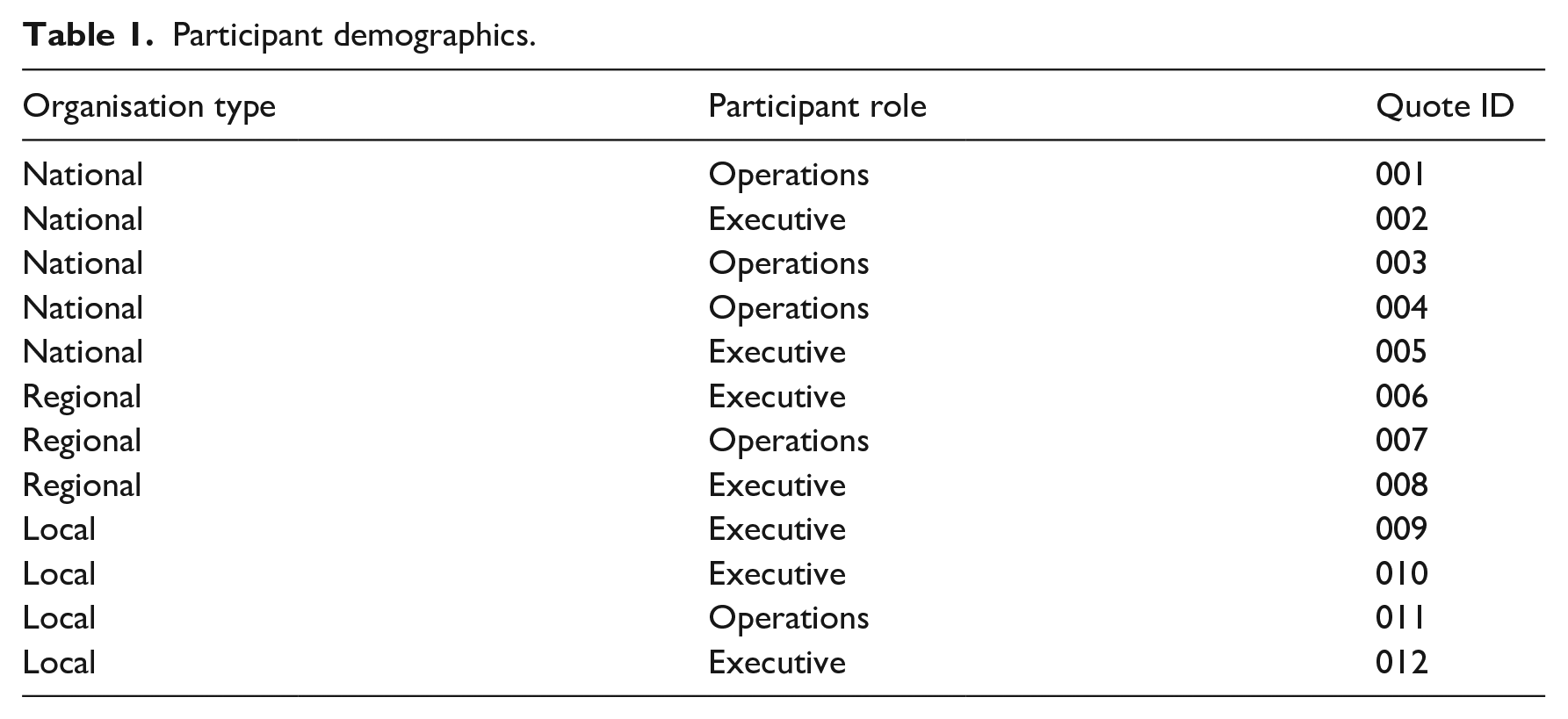
Purposive sampling was used whereby participants from sight loss organisations in the UK were invited to take part in the interview via email by the lead author (LJ). Eligible organisations were identified through the ‘VI Charity Sector Partnership’ at Visionary. The key criteria for recruitment were that the participant worked at an organisation in the sight loss sector which provided either a telerehabilitation service or offered information about, or access to such agencies. Local organisations providing vision rehabilitation were identified from the grey literature of the authors’ previously published scoping review (Jones et al., 2022). Local organisations were contacted about the study and were provided with the study information sheet. All organisations were based in the UK and there was no restriction on the size of the organisation. A summary of the type of organisation and participants’ role within the organisation are provided in Table 1.
Participant demographics.
Data collection
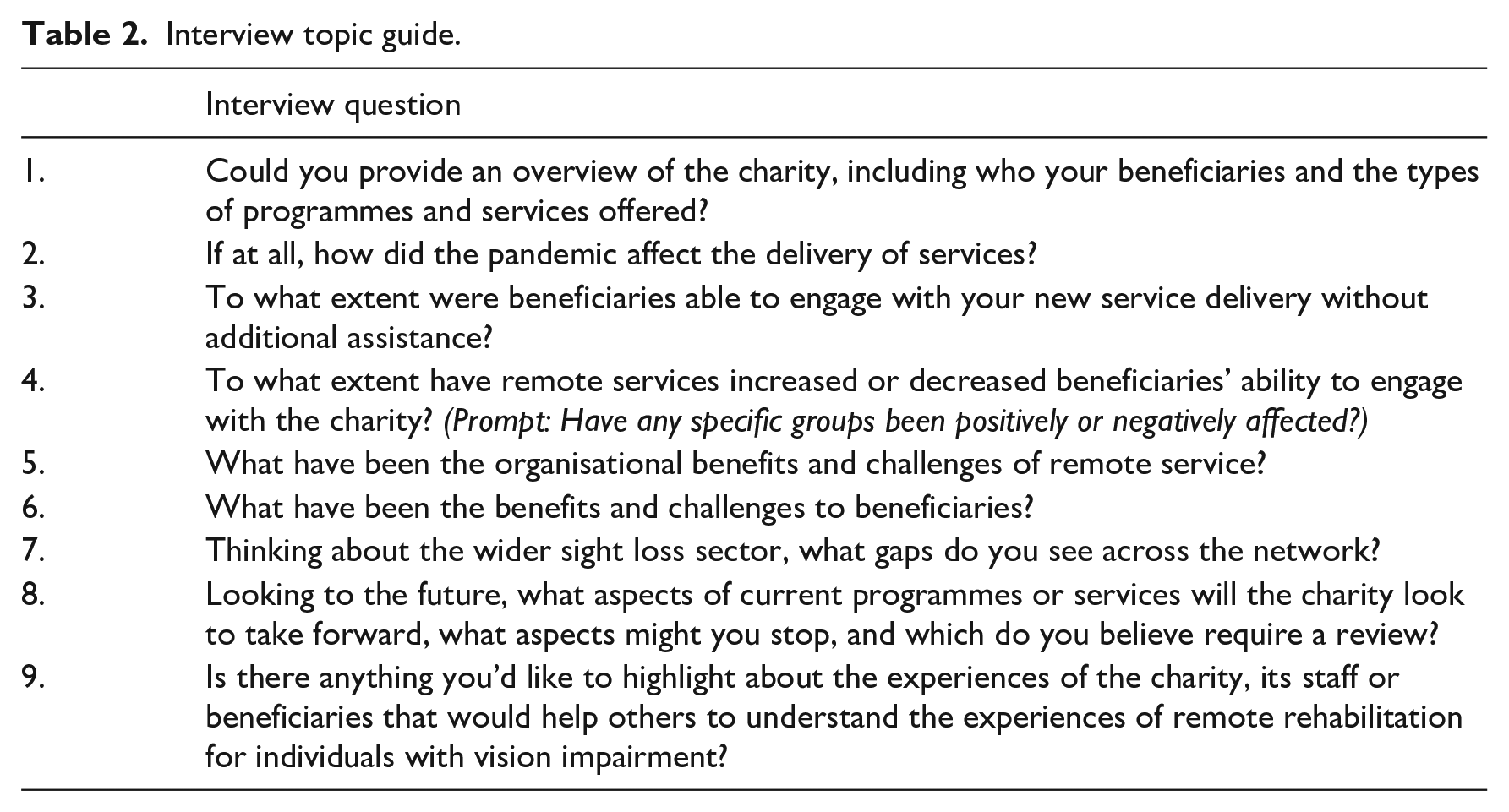
Online semi-structured interviews were conducted using Microsoft Teams V.1.3 with consenting participants meeting the recruitment criteria. Interviews were conducted by a male PhD trained researcher with a background in psychology (LJ). It was communicated to participants that the researcher was external to vision rehabilitation charities and that the reason for the study was to gain a real-world understanding of rehabilitation service delivery. No relationship was established between the researcher and participants prior to beginning the study. An interview topic guide was developed which included open-ended questions about the sight loss organisation and its beneficiaries, the changes to rehabilitation services during the pandemic, and reflections on the benefits and drawbacks of telerehabilitation. The interview topic guide is shown in Table 2. Interviews were audio-recorded and transcribed verbatim.
Interview topic guide.
Data analysis
Transcripts were analysed using thematic analysis (Braun & Clarke, 2006), whereby texts were read and re-read to ensure familiarity, and meaningful units were coded. Transcripts were coded at a semantic level, considering the explicit content of the data. Data were coded by one researcher (LJ) and the coding framework was discussed among the entire research team. After all transcripts were coded, themes were generated by identifying patterns within and across participant interviews and collecting relevant codes together. Themes were created using an inductive approach (i.e., driven by the content of the data). An inductive approach was used due to the limited previous research in the area, and therefore no specific theories were used to generate the themes. Finally, the overarching themes were created by collecting the subthemes together based on the aspects of vision telerehabilitation to which they related.
Data were analysed using NVivo v.13 (QSR International, Cambridge, Massachusetts, USA). Data saturation was defined as the point where no new information was coded during transcript analysis, which was based on the judgement of the research team and indicated further data collection or analysis was unnecessary. A member-check exercise was employed where the coding framework and the interpretation of the data were sent to all participants to provide an opportunity to clarify or elaborate on any aspect of how the data had been interpreted by the research team. This exercise allowed for an assessment of the credibility and authenticity of the final coding framework, and to determine interpretive validity (i.e., accuracy in determining meaning of quotes).
Results
Twelve participants took part in the study from a total of nine sight loss organisations in the UK between July and November 2022. Average interview duration was 41 (±12) minutes. The size of the organisations varied where some participants were from large national service providers (n = 5), some were from regional charities serving UK nations (n = 3), and others were local community organisations (n = 4). Four major themes were identified during analysis: (1) delivery of telerehabilitation, (2) opportunities associated with telerehabilitation, (3) challenges associated with telerehabilitation, and (4) wider challenges in the vision rehabilitation sector. Figure 1 provides an overview of the challenges, opportunities, and wider considerations described in this study. Direct quotations taken from the interview transcripts are italicised and used to illustrate the relevant themes.
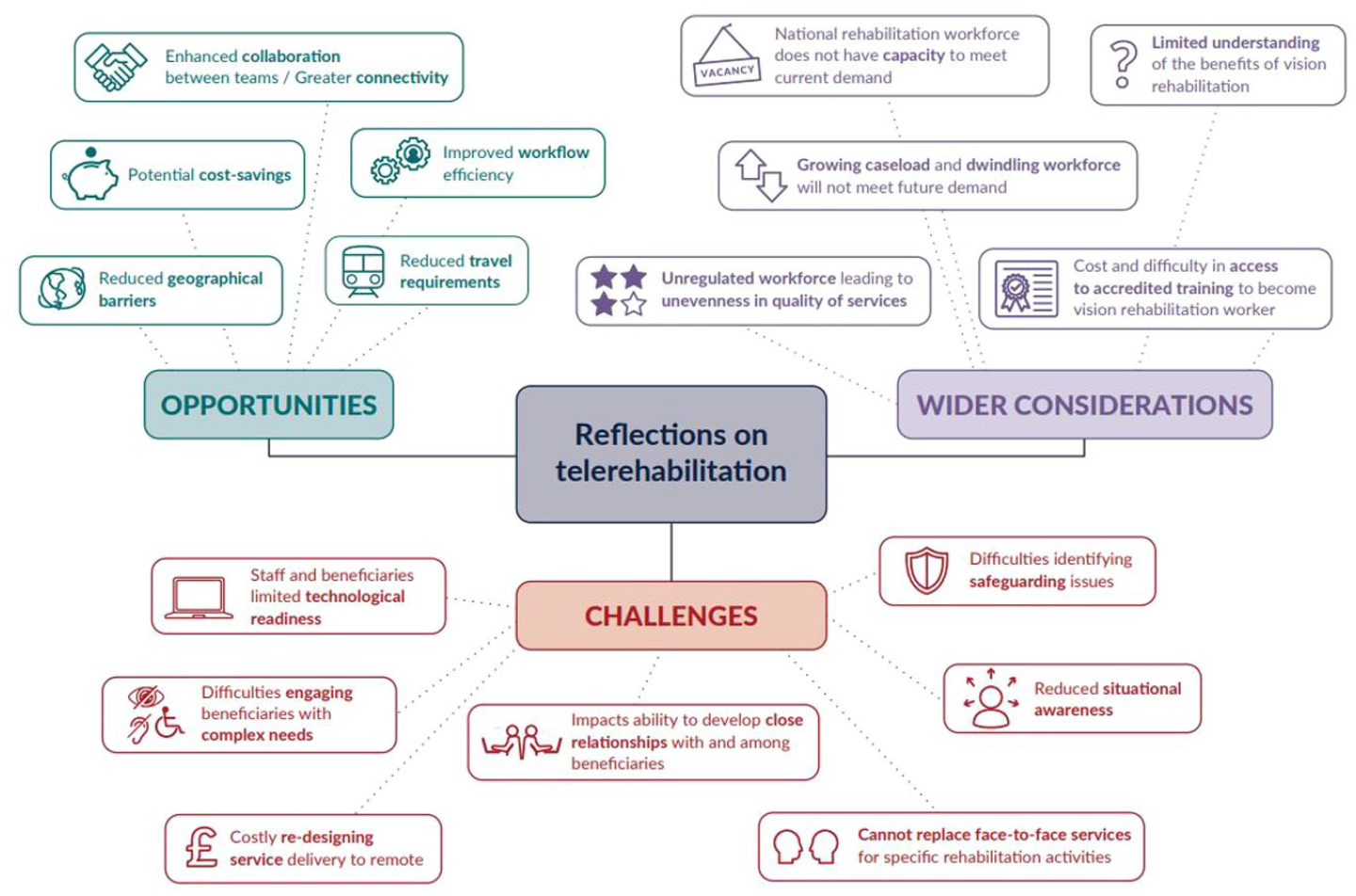
Diagram illustrating the opportunities, challenges, and wider considerations of vision telerehabilitation described by service providers.
Delivery of telerehabilitation
The organisations recruited in this study provided a broad range of vision rehabilitation programmes and services, including but not limited to digital skills training, mobility and navigation, maintaining routine hobbies, daily living skills, lighting assessments, and counselling. Prior to the pandemic, these services were largely delivered through face-to-face sessions, either during home visits or through sessions at rehabilitation centres. Most participants reported a halt to face-to-face sessions in the first wave of the pandemic; however, there were regional differences regarding recommencement of these services. For example, differences in restrictions meant that centre-based vision rehabilitation could restart earlier in Scotland than in England. In addition, there was some regional variation in the extent to which vision rehabilitation workers were classed as key workers, which affected whether services were delivered face-to-face or remotely. Participants reflected on the rising demand for vision telerehabilitation services necessitated by restrictions associated with the pandemic. The immediacy of these changes was highlighted in the interviews: We moved online almost overnight. We moved from community based into an entire telephone delivery. (003) Before COVID all our services would’ve been face-to-face. That was the way that we’d all been working, and then overnight we had to learn how to do things remotely. That’s been an incredible journey. (006)
Providers described making greater use of digital communication platforms and telephone services to deliver rehabilitation sessions virtually during the pandemic, including skills training and social networking We used video calls where the service user could manage that. We would be doing a rehab intervention, a piece of training or demonstration over a video call. (009) Largely, a lot of our remote groups were set up and we explored using different platforms with members. But I think the ones that have sustained are the ones that are telephone-based groups. (002)
Both audio and video communication modalities were adopted by charities to deliver remote sessions. There was a suggestion that video-based technology should not be overlooked simply because individuals may be living with reduced vision. For example, a video platform could be helpful for individuals who rely on speechreading: I’ve certainly done a one-to-one using a video camera because the member could lip-read. We absolutely do everything we can to include everybody. (003)
The urgency for working with service users to develop their digital literacy was emphasised given the growing need to use technology: Technology became even more important during the pandemic because suddenly everybody wanted to know how to use Zoom, everybody needed to do their online shopping, everybody needed to book their [vaccine] boosters online. Obviously for lots of our clients, that was very new. So, our assisted technology services were in quite high demand. (009)
Opportunities associated with telerehabilitation
Participants remarked on a broad range of benefits associated with delivering rehabilitation virtually, both in the context of opportunities for the organisation and the service users themselves. One particular benefit was a perceived wider geographical reach of services, removing geographic barriers between providers and recipients: When you think about how many people we can reach from rural locations, who would never have been able to come into cities and towns to do a face-to-face group and layer into that the fact that people might find it really difficult to navigate around a town or a city or a place that’s unfamiliar, so there are lots and lots of plus points. (003) Because the county is huge, there are still vast areas that places aren’t accessible. So there were definitely travel barriers before. (009)
In addition to providing a wider geographical reach, telerehabilitation was considered to improve reach to populations who traditionally had difficulties travelling to face-to-face sessions: For people who perhaps care for a relative or there’s some other reason that they can’t travel perhaps because of a physical disability, then actually having an online group is much easier for them. (009)
In the context of geographic reach, there was a reflection that organisations could extend their provision beyond the local authority for which they are responsible, creating opportunities for greater collaboration between organisations and authorities to provide a more equitable service: Obviously when you’re running a localised course, everybody’s trying to get support from the same therapist or from the same guide dog officer, that kind of thing, whereas for the first time, we had individuals hearing about what the services were like outside of their area. We didn’t have a postcode lottery. It didn’t matter where you were in the country. You could attend the course, and you’d come away achieving the same outcomes. (004)
Digitalisation of services was considered to have some internal organisational benefits, such as improving collaboration between teams within a national service provider. For example, greater connectivity across the organisation reduced tendency for individual teams to work in silos: One benefit we found internally was the way in which our teams were working together. Rehabilitation might occur in centres, and then rehabilitation staff sit in community teams, and before now how often did they really talk to each other when supporting a member, and while a member was moving around different elements of our service. We’re now actually working in a much more collaborative, integrated way. (002)
Although no formal cost-effective or cost-comparison evaluations were reported, it was generally regarded that telerehabilitation could be operated at a lower cost and requiring a smaller time commitment in some circumstances. For example, saving time and money by reducing the need to travel to centres or individuals’ homes: In terms of budget, there’s definitely been a cost saving in terms of our staff travel, the venue hire, the refreshments, having to pay volunteer expenses, et cetera. We’ve definitely saved money not having to travel. (004)
Besides reducing the need for travel, another cost-related benefit was the potential for delivering online group sessions to larger audiences, therefore maximising the number of recipients who could be reached in each session. Telerehabilitation may thus be more amenable to delivering services to multiple groups and arguably requiring fewer resources: I’ve heard organisations say is it can make it more cost-effective in that you can cover some of the stuff online without sending a worker out. As soon as you send a worker out, it becomes more expensive. (005)
With respect to perceived cost and time savings, there was an additional benefit of minimising the impact associated with non-attendance and cancellations of face-to-face sessions, which was considered to have significant cost and time implications: At times everyone has said they’re going to come, and then we have a heatwave or a really rainy day or it snows, and then just five people will turn up. It can be soul destroying. It’s a whole day that you’ve wasted. It’s expenses that you’ve claimed, et cetera. Whereas now, on a phone-based course, a course can still run with three or four people. (003) Sometimes we were sending one person out for an overnight stay out to some far-flung place. They had to take ferries and boats and it costs hundreds of pounds to send this worker, and when they’ve arrived, the client had forgotten and had gone out. (005)
One sentiment expressed during the interviews was that the pandemic served as a catalyst to address a long-standing need to re-design models of rehabilitation, and harnessing aspects of virtual service delivery beyond the pandemic was viewed positively in this respect: We knew that we needed to change before the pandemic. I think the nature of the pandemic, in terms of it being a necessity to do things differently catapulted us forward in terms of those different ways of working, particularly from how our beneficiaries received our services and their willingness to change and to do things differently. Had we done that without a pandemic, we’d still be on that journey of trying to go through those changes. It thrust us into a new way of doing things. (002) It gave us a kick up the backside for sure. We were saying before that we didn’t want to push people to have things like the Internet and so on. But my goodness it’s changed the world and it’s changed people’s lives. (012)
Challenges associated with telerehabilitation
Alongside the opportunities and benefits of telerehabilitation, organisations reflected on a broad range of challenges they had experienced with using this approach, as well as wider concerns regarding potential gaps in service provision.
A common difficulty was the need to upskill staff and service users’ digital skills to enable engagement with services: One of the barriers to engagement with remote delivery has definitely been the technology itself. That has been quite stressful at times. It’s one of those things that is largely out of our control. (003) We very quickly moved on to doing online, which was a very steep learning curve for the whole team as well. (012)
Particular challenges during the pandemic related to technical problems occurring during sessions, as well as inefficient processes: Sometimes we had complaints. One time it sounded like everybody was underwater. It’s very difficult to hold a call in that situation. (003) Initially, we were having to dial participants in. If they wanted to join, they had to enter in a nine-digit code, so there were some issues with that. (004) Working with service users with more complex needs living with dual sensory loss, such as a hearing impairment in addition to visual impairment, was reported as a challenge at times: A lot of our members who are quite elderly, they have hearing loss as well. So, for some people it was really difficult, and they weren’t able to engage in the telephone stuff as well. (007)
In addition, there was a sentiment that older adults in general tend to have a lower readiness to adopt the use of technology which was a challenge given the age-related characteristics of many eye conditions. However, it was also emphasised that individuals should not be excluded on the basis of age: It’s unfair and stereotypical to say older people don’t use tech. But I think it’s absolutely understandable that the older somebody becomes, they might be less confident using it, or it might just be too difficult. (003)
While there were discussions around the potential cost-saving aspects of telerehabilitation, there was also the recognition that organisations, particularly smaller charities, may not have the financial resources to be able to re-design their services to include technology: These organisations are often surviving hand to mouth each year . . . They need the money to buy the kit. They need the staff who are willing to learn how to use the kit, assuming they can buy the kit, so that’s a resource implication. (005)
Regarding the wider drawbacks associated with telerehabilitation, it was highlighted that delivering services virtually can impact the relationships between providers and recipients, and between recipients themselves within peer support networks: You don’t get to know people the same virtually as you do face-to-face. There’s not that same connection. You do get to know people, but it’s different. As soon as you meet somebody in a room, you’ve got their presence, their personality comes across strong. (006)
In addition, telerehabilitation was considered to go only so far in delivering interventions, and that many aspects of rehabilitation cannot easily or safely be achieved outside of face-to-face sessions: For route finding and getting out and about, nothing can replace face-to-face in my own view. I think online cannot replace face-to-face when it comes to route navigation. (005) It’s high-risk work because they’re asking people who can’t see to do things that are risky. Like crossing the road, using a sharp knife, getting things out of the oven, moving hot pans around. All those things are very, very high risk, and they’re teaching people to do that when they can’t see, or their field of vision is restricted a lot. (011)
Further concerns arose regarding reduced situational awareness (i.e., an understanding of the context that the individual and the rehabilitation provider are operating in). For example, home visits were considered essential to fully assess living conditions to provide an indication about how well an individual is coping and to effectively identify potential hazards: Sometimes, with the older generation, they can kind of put a mask on things and say, oh yeah, I’m absolutely fine, I’m coping absolutely fine. But then you go into the house, and you just think, oh my goodness, this is just an accident waiting to happen. (010) You are very reliant on what a beneficiary tells you. There is quite a lot to be said from being in someone’s home to be able to observe some of the stuff that’s going on, particularly around challenges to do with maintaining daily living tasks. That sometimes can be quite different to what they might tell you they’re able to do. (001)
Moreover, a virtual approach to rehabilitation could lead to greater difficulty in detecting safeguarding concerns and non-verbal cues regarding an individual’s well-being: From a safeguarding point of view, being in someone’s home and understanding family dynamics and observing, you will find out more than what someone may tell you. It’s quite unusual that someone would disclose a safeguarding issue to you. You’re more likely to observe things that lead you to a conversation where you explore something with a member or beneficiary, rather than relying on them picking up the phone to you and saying, do you know what, this is happening to me. (002)
Wider challenges in the vision rehabilitation sector
Reflections on the delivery of telerehabilitation generated broader discussions from organisations about wider challenges affecting the sector. There was a consistent narrative across interviews that aspects of vision rehabilitation were approaching a crisis point. For example, the national rehabilitation workforce does not have capacity to meet current demand, and the urgency of this problem was expected to be compounded by a growing caseload in combination with an aging and retiring workforce.
Certainly, right now, there’s a real crisis point. We have a shrinking workforce because many of the qualified professionals are now getting to the age where they’re close to retirement. (006) A lot of our ROVIs at the moment are just simply firefighting. They’re firefighting the waiting list that they’ve got. (008)
Scarcity of the workforce was also attributed to perceptions of rehabilitation and a lack of understanding about the role. For example, organisations reflected on difficulties recruiting to roles: We just can’t recruit because there are just no rehabilitation officers even available to appoint to those jobs. We’re always going to be on the backfoot with trying to recruit people. It’s such a niche market as well; it’s not something that loads of people will go into, so it is difficult. (011)
To address workforce-related issues, it was felt that perceptions about rehabilitation needed to change to highlight the value of the profession and the role practitioners have in the eyecare pathway: I am a qualified rehabilitation practitioner, but I was disappointed because I qualified feeling like I had gained a qualification that nobody understood. (006)
Poor awareness about the role of vision rehabilitation workers extended to commissioners and decision makers, where the lack of recognition was affecting the regulation and quality of services across the sector: They don’t understand the benefits of it. The commissioners don’t know what it is, and they don’t know, in my view, the kind of life-changing difference it can make at the point that you need it. You might get it, you might not get it. You might be dead before you get to the top of the waiting list. (005)
Further issues related to training associated with the profession. Several barriers to vision rehabilitation training were identified, including the ability to gain access to accredited training, the motivation to undertake training and the associated costs of courses: There’s no training for these people unless you’re prepared to go to a University where there’s only about 20 places. (005) You’ve got to take on a whole load of student debt to gain a qualification, and when you enter the workforce, there is limited career progression for you as a professional ROVI . . . you’re capped within a bracket. There isn’t a career pathway for you to proceed. (010) Local authorities are saying they haven’t got the money to fund the training. That’s been a barrier for us. It’s £12,000 for the two years and they just don’t have the budgets. (008)
Finally, a wider problem was identified that rehabilitation is not a regulated workforce unlike other care-related professions and therefore causing potential unevenness in the quality of services: One of the issues with the workforce is first of all, the regulation of the workforce. It’s not a regulated service. Rehab is not a regulated service . . . The actual training program doesn’t have tech in it. Probably by the time you taught somebody it would be out of date anyway, so there’s major issues. (005)
Discussion
As the prevalence of visual impairment increases in the population, rehabilitation will have an increasingly important role in the eyecare pathway providing early intervention and prevention to support independence and healthy longevity. Providers are utilising telerehabilitation approaches to ensure individuals can continue to access services, even at times when traditional face-to-face sessions are challenging. Overall, this study identified a range of factors at an organisational and service user level which may have implications for the future directions of telerehabilitation in the sight loss sector.
A common thread across interviews was that telerehabilitation could be used as a tool for increased inclusion and participation, due to overcoming geographical barriers and addressing the needs of traditionally harder-to-reach populations. People with disabilities, including those with visual impairment, may often have complex medical and health care access needs for which telehealth may be particularly well suited (Noel & Ellison, 2020). For example, limited access due to geographical barriers or a lack of resources to travel may prevent some individuals from fully engaging with, and benefitting from, rehabilitation. In terms of costs, previous economic modelling from the United States has indicated telerehabilitation (including adaptive skills training, orientation and mobility training, computer training, and training with vision-related activities) was associated with a significant reduction in the number of miles travelled and time spent travelling among a rural community of individuals living with conditions including age-related macular degeneration, glaucoma, and diabetic retinopathy (Ihrig, 2019). Overall, the median travel cost-saving per rural individual was US$65.29. The sentiment that vision telerehabilitation could have cost-saving implications for both beneficiaries and providers was expressed by participants in this study, suggesting this approach could be a practical, time-saving, and cost-saving alternative to traditional face-to-face sessions in some situations. Yet, the economic value from a provider perspective requires more research. For example, participants in this study described the need to re-design systems and purchase new technology, as well as upskilling staff with specialist training, all of which having a cost implication for the provider already working within a limited budget. This was particularly highlighted by small organisations funded through programmatic models of commissioning and grant funding.
In addition to creating opportunities for increased participation, there was discussion around the role of telerehabilitation in working with beneficiaries with more complex needs, such as those with dual sensory loss, or older individuals less familiar with technology. Delivering services virtually to individuals hard of hearing during the pandemic was at times referred to as a challenge; however, one strategy to address this was to use a video-based platform to allow for lip-reading. In relation to older adults, there was discussion around potential challenges associated with a lower technological readiness and confidence in using telerehabilitation systems among this cohort. Evidence suggests older people engage better with technologies that are considered to have value, such as technologies associated with health care and rehabilitation (Heinz et al., 2013). Older ophthalmic patients frequently use technology, for example, 88.5% of people aged 66–79 years attending a hospital eye clinic reported regularly using technologies to help with everyday tasks including desktop and laptop computers and smartphones; However, this proportion dropped to 58.6% for those over 80 years old (Ali et al., 2019). Moreover, at least a third of participants under the age of 80 cited being experts at using the internet. Individuals living with age-related eye conditions are generally motivated to use technology related to monitoring eye health (Jones et al., 2021). When considering this evidence together, it could be argued there may be significant variability in individuals’ readiness to adopt telerehabilitation; thus, requiring policymakers and service providers to avoid reinforcing stereotypes relating to older adults and technology. As suggested elsewhere, increased variation in physical and cognitive function as people age requires policies to consider beneficiaries on a more individual basis (Beard & Bloom, 2015). As such, an assessment of individual self-efficacy regarding aptitude for telerehabilitation or a blended approach to service delivery offering virtual and face-to-face sessions will help to stratify individuals where telerehabilitation is most likely to be tolerated and successful.
Alongside factors relating to potential cost and time savings, these benefits need to be balanced against the drawbacks of this approach. For example, delivering rehabilitation remotely was thought to potentially negatively impact the ability to create close working relationships between service users and providers, and among service users themselves in peer support groups, which could affect the quality of services. It has been suggested that virtual clinical consultations, either by telephone or video, are more difficult for both patient and provider in situations where the individuals have never met in person (Kilvert et al., 2020). Research relating to virtual mental health services identified disadvantages including feelings of less personal and awkward interactions, difficulty in building a rapport, and aversion to discussing sensitive issues (Hawke et al., 2021). The importance of the client–therapist relationship has been recognised in health and social care, including occupational therapy where studies have indicated a connection between the quality of this relationship and clients’ achievement of functional and meaningful outcomes (Bright et al., 2012; Cole & McLean, 2003). This connection may partly be explained by the importance placed on human characteristics in rehabilitation, such as a perceived sense of compassion, empathy, and active listening (Thorne et al., 2004), aspects of which may be experienced less clearly outside of a face-to-face context. Indeed, the relationship with the practitioner is central to individual experiences of rehabilitation as clients may attribute greater importance to the relationship with their service provider over factors such as the content and technical expertise of the service itself (Blank, 2004; Östlund et al., 2001). While the significance of this evidence is important when considering the potential impact on outcomes in vision rehabilitation, it is noteworthy that telerehabilitation (and wider telehealth) is a rapidly evolving field; thus, it can be expected that perceptions of this approach are also likely to change over time within this shifting landscape. For example, interest in telerehabilitation is growing, as evidenced by studies showing virtual consultations and low-vision services are acceptable among people living with visual impairment (Bittner et al., 2022; Kotecha et al., 2015).
Concerns arose during the interviews regarding a potential for reduced situational awareness associated with telerehabilitation. In other words, face-to-face rehabilitation, particularly within a beneficiary’s home, allows practitioners opportunity to personally assess the home environment and to gain a better understanding of the individual’s living arrangements. Participants described difficulties with accurately analysing rehabilitation needs virtually, which largely relies on self-reporting from the recipient themselves. Home assessments and adaptions represent an important component in rehabilitation concerning leisure activities and social participation. For example, evidence suggests that adaptions to lighting in the homes of people with visual impairment are related to improvements in completing everyday activities such as reading and enhances ability to contact friends and relatives, thereby increasing opportunities for social interaction (Brunnström et al., 2004). In addition, providing home-based problem-solving training has been found to reduce the likelihood of an individual living with visual impairment to relinquish a valued activity (Rovner & Casten, 2008). Similar concerns were raised regarding difficulty in detecting possible safeguarding issues when working with individuals remotely. Recommendations from a study on virtual consultations in diabetes care suggested techniques to mitigate vulnerability such as, communicating in advance to invite individuals to a conversation at a specified time to allow the individual options to accept or decline in principle, offering an option for a telephone rather than video consultations allows participants greater flexibility in choosing a safe location, and to begin each session by checking that privacy and confidentiality are in place and the individual is not vulnerable to anyone hearing their discussion (Kilvert et al., 2020).
Besides reflections on adopting and using telerehabilitation in practice, participants spoke more broadly about wider challenges in the field of vision rehabilitation. A shortfall in the workforce, such as an insufficient number of ROVIs to meet demand, was recognised as a growing problem for the sector. This issue was exemplified in a recent report commissioned to assess patterns in service provision and highlighted the scarcity of qualified ROVIs across local authorities in Wales, UK (Wales Council for the Blind, 2021). In particular, the report identifies the diminished capacity to meet the minimum standards set by the adult social services agency of one ROVI per 70,000 of the population. Workforce-related challenges are not a new concept in vision rehabilitation. For example, the projected shortfall in rehabilitation workers was described over 10 years ago in the UK Vision Strategy, a part of the VISION 2020 initiative, which set out a framework to improve access to these services (UK Vision Strategy, 2008). Indeed, forecasting indicates eye health services more broadly will also be affected by insufficient capacity, including clinical care (Resnikoff et al., 2020).
Shortages in the workforce can be linked to a range of factors identified in this study, including poor awareness about the scope and value of vision rehabilitation, limited opportunities for career development, as well as the availability and cost of training. Qualified practitioners are required to pass a specified qualification which has hitherto been delivered by a limited number of universities (n.b. at the time of interviews, just one) for a foundation degree, or via an apprenticeship route. Although significant efforts by the Scottish Visual Services Steering Group have since led to a graduate low vision rehabilitation course being reinstated at an additional UK university. Training requirements are contained within recommendations and guidance documents produced by the Association of Directors of Adults Social Services (ADASS) and the Royal National Institute of Blind People (RNIB), referenced within Care and Support Statutory Guidance (Department of Health & Social Care, 2023). The ADASS guidance refers to the need for competent and appropriately trained staff; however, neither the legislation nor the guidance is specific, and training for ROVIs is not part of the NHS Business Service Authority bursary funding programmes. There may be further related issues around differences between training and education. For example, concerns were raised around the limited relevancy of technology in the current educational model, suggesting this approach may not meet employer requirements, highlighting the need for practitioner development through ongoing training and continuous professional development to ensure technical skills are kept up to date. Finally, the lack of professional regulation in the rehabilitation workforce was identified as an issue. Unlike more regulated professions such as those in the health sector, the care sector has fewer regulatory bodies. Regulation can help to develop a highly skilled, knowledgeable, qualified, and competent workforce, and there are ongoing strategies to further professionalise the care workforce, although these efforts are caveated by costs associated with regulation (House of Commons Committee of Public Accounts, 2018).
It was apparent in the interviews that organisations offered a range of services described under the broad term ‘telerehabilitation’. During this study, the term telerehabilitation was used to refer to any aspect of rehabilitation delivered using a remote approach, including physiological, psychological, and social interventions. The purpose of this study was to understand organisations’ reflections on telerehabilitation more generally, and therefore, the findings have been discussed together, without disaggregating by these specific components of rehabilitation. There is general acknowledgement that remote delivery of services will remain an important aspect of routine practice within future health and social care systems, further demonstrating the need for training and guidance for telerehabilitation (Anil et al., 2021). When considering the role of telerehabilitation in the eyecare pathway beyond the pandemic era, a remote approach will likely be more amenable for certain interventions (e.g., social support and activities), and less practical in other cases (e.g., functional rehabilitation such as mobility training). As identified in this study, tasks such as route finding and navigating using a cane involve risks to health and safety, making these activities more suited to traditional face-to-face sessions. These findings align with evidence from physiotherapy telerehabilitation identifying an unmet need in accurate remote movement assessments (Aderonmu, 2020). Moreover, risk minimisation strategies are needed such as not performing sessions at home alone as well as the need for supervised baseline measurements to accurately understand individuals’ limitations (Caniça et al., 2021).
Conclusion
Pressures to harness digital innovation solutions to support delivery of rehabilitation in the sight loss sector have been growing, largely due to an increasing caseload and dwindling workforce. The pandemic necessitated health and social care services to review what is possible and adapt models of care to a rapidly changing situation (Wosik et al., 2020). Reflections from sight loss charities about the emerging role of telerehabilitation and wider considerations about the future landscape of vision rehabilitation led to a broad range of opportunities and challenges being identified in this study. The prospect of reducing geographical barriers and enabling wider engagement was attractive to many organisations. Cost-effectiveness remains an area of uncertainty given the short-term capital costs associated with re-designing systems and longer-term operations expenditure associated with training; however, these costs could be absorbed by time and resource savings in the longer term. Challenges remain regarding the appropriateness of telerehabilitation for specific aspects of vision rehabilitation and for different populations, as well as ensuring policies are in place to ensure safeguarding and assessments are not compromised. In addition to growing the rehabilitation workforce, addressing barriers to training and improving regulation of the profession, there is a need to consider the distribution and accessibility of support to help ensure equity of services so that vision rehabilitation needs are universally met. Telerehabilitation may go some way to closing gaps in services, but greater investment in organisations to develop their services and in research to understand the benefits of this approach in the longer term will help to answer increasingly important questions about what works well, in what places, at which times, and under which circumstances.