
Abstract
This study aims to provide an overview of visually impaired cyclists’ difficulties with independent cycling in the Netherlands. Normally sighted cyclists (n = 109) and visually impaired cyclists (n = 197) and former cyclists (n = 22) completed an online questionnaire on potential cycling difficulties related to visual function, bicycle control, and contextual factors. The former cyclists were asked to what extent these difficulties were crucial for them to stop cycling. Overall, the visually impaired cyclists reported having most difficulties with light–dark transitions, crossing intersections without traffic lights, and other traffic participants’ bad visibility. The former cyclists’ determinants to stop cycling were similar to the difficulties reported by those who still cycle. The nature and the origination of the visual function limitations may induce specific difficulties in cycling. However, the ability to cycle does not depend on the visual functions alone, but also on the ability to compensate sufficiently for the visual function limitations. In conclusion, using minimal vision requirements for cycling unnecessarily excludes many visually impaired people from independent cycling. Mobility trainers are recommended to give cycling training and advice based on a practical test of the client’s individual ability to compensate for the visual limitations.
Introduction
Bicycle use for daily transport is being promoted around the world as it has economic, environmental, and health-related benefits (e.g., Bonham & Johnson, 2015; Danish Ministry of Transport, 2014; Tour de Force, 2017; Transport Canada, 2011; UK Department for Transport, 2017; US Department of Transportation, 2014). In the Netherlands, cycling is the most popular means of transport for distances up to 7.5 km (Dutch Ministry of Transport, Public Works and Water Management, 2009). The ability to cycle independently is important for mobility and social participation as the bicycle is commonly used for commuting, to go shopping, and for other activities of daily living (Centraal Bureau voor de Statistiek, 2016). The popularity of cycling in the Netherlands can be partly explained by circumstances that facilitate bicycle use. For example, the Dutch landscape is mostly flat and there is a high-quality cycling infrastructure; many cycle paths are separated from fast motorised traffic and can be recognised by a contrasting red colour. Cycling is also important for the independent mobility and social participation of visually impaired people, especially to those who are not able to control faster vehicles.
People with permanent reduced vision may experience difficulties with independent cycling for a number of reasons. The International Classification of Functioning, Disability, and Health ([ICF] World Health Organization [WHO], 2001), which is a commonly used framework in rehabilitation (Douglas, Pavey, Corcoran, & Clements, 2011; Jaarsma, Dekker, Koopmans, Dijkstra, & Geertzen, 2014) describes health conditions as interactions between body structures or functions, activities, and participation. According to the model (Figure 1) each of these domains is subject to contextual factors, which are classified into personal and environmental factors. Environmental factors make up the individual’s physical and social environment, whereas personal factors relate to internal features that are not part of the health state. Very limited information is available regarding the cycling difficulties encountered by visually impaired people, and the extent to which these difficulties are decisive for some of them to cease independent cycling.
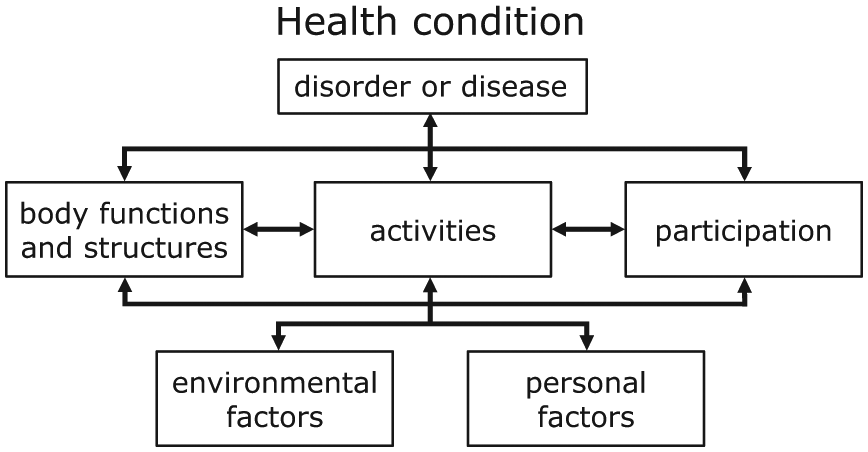
The International Classification of Functioning, Disability, and Health (ICF) (WHO, 2001).
Visual functions
The nature of the visual function impairment may partly determine which difficulties are experienced in cycling. Connor (1992) describes a number of cycling difficulties, based on his personal experiences as both a visually impaired cyclist and a rehabilitation counsellor. He states that particularly persons with peripheral field loss have difficulties in cycling. They consciously need to make the right eye and head movements to see stationary objects, such as the road surface and overhanging trees, resulting in difficulties with maintaining a straight line of travel. In contrast, people with central field loss may respond to stationary objects automatically.
In the Netherlands, there are no formal minimum vision requirements that impose restrictions on independent cycling other than a general law prohibiting road users to endanger themselves or others (Wegenverkeerswet 1994 artikel 5 [Article 5 of Dutch Road traffic act of 1994]). In essence, this allows visually impaired people to cycle, irrespective of the nature of the visual function limitations. Nevertheless, mobility instructors in Dutch rehabilitation centres for visually impaired people use informal guidelines based on visual functions. The instructors aim to optimise the independent mobility of visually impaired people while protecting the clients’ and other traffic participants’ safety. To be on the safe side most Dutch mobility trainers currently use a binocular visual acuity (BVA) below 0.1 (decimals; Snellen notation: 6/60 or 20/200) and a horizontal visual field less than 60 degrees as absolute contra-indications for independent cycling. These informal guidelines are partly based on Wilhelm and Endres (2004), who found increases of accidents in people with such visual functions. In practice, however, there are people whose visual performance clearly meets these guidelines but stop cycling anyway, whereas others with visual performance below the guidelines continue cycling without accidents (e.g., Schepers & Den Brinker, 2011). The latter suggests that some visually impaired people are able to compensate for their visual limitations in such a way that it enables them to cycle independently in a safe manner.
Activity of cycling
During the cycling ‘activity’ cyclists take numerous decisions to control their vehicle. Compensation strategies may be applied while taking these decisions. Michon’s model of driver behaviour (Michon, 1985) considers three levels of decision-taking in vehicle control: the strategic, tactical, and operational level. The strategic level concerns general plans of the trip, including selecting the vehicle or the route and departure time. Typically, there is no time-pressure while making decisions at this level. At the tactical level, the cyclist controls general manoeuvres in the prevailing circumstances, such as choosing the road position or following distance. These decisions are made under moderate time-pressure, within seconds. The operational level describes decisions related to controlling the bicycle, including pedalling, steering, and braking. All actions at this level are conducted under high time-pressure. Experienced cyclists make these decisions automatically. Visually impaired people particularly have problems with tactical and operational decisions, since these are mainly driven by visual input and made under time-pressure. Cyclists can compensate for shortcomings at a certain level by making the right decisions at another. As described in Connor (1992), visually impaired cyclists who experience difficulties with acquiring an overview in dense traffic (operational) may compensate by maintaining a lower speed (tactical) or by selecting a quiet-traffic route or time (strategic). During decision-taking at each level, visually impaired cyclists may also attune their eye or head movements to their visual condition (Connor, 1992; Piper, 1997).
Contextual factors
Connor (1992) suggests that lighting conditions, variations in the street surface, obstacles, and additional auditory limitations may be important environmental factors for independent cycling with vision impairment. Based on a sports study (Jaarsma et al., 2014), social factors, such as a lack of friends, may also obstruct cycling. Professionals involved in the mobility of visually impaired people considered the ‘traffic situation’, ‘characteristics of the infrastructure’, and ‘weather and light circumstances’ the most important environmental factors for low-vision cycling (Jelijs, Heutink, de Waard, Brookhuis, & Melis-Dankers, 2018). They regarded ‘personality’, ‘traffic experience’, and ‘personal background’ the most important personal factors.
Aim of the study
In summary, at present, it is difficult for mobility trainers to assess whether a visually impaired person is able to cycle independently in a safe and responsible manner. Nevertheless, they have to give advice on whether a client is able to cycle safely. In Dutch vision rehabilitation centres, mobility trainers use informal guidelines based on visual functions. However, there are indications that visual functions alone are not pivotal for the ability to cycle (Schepers & Den Brinker, 2011). Using these guidelines results in mobility trainers providing too conservative cycling advices that unnecessarily discourage visually impaired people from cycling. Instead, mobility trainers could assess whether a client compensates sufficiently for the difficulties experienced due to the visual limitations. However, more insight into these difficulties and compensation strategies is necessary to support mobility trainers in giving cycling advice and training. More knowledge on this topic may also explain which factors lead to visually impaired people ceasing cycling.
The present study aims to provide an overview of the difficulties that visually impaired cyclists and former cyclists experience with regard to independent cycling. For comparison purposes, normally sighted cyclists were also invited to participate. Respondents indicated in an online questionnaire which cycling difficulties they experience or experienced regarding visual functions, bicycle control and contextual factors. In addition, group comparisons were made based on visual acuity, on peripheral field loss, and on whether the participant cycles independently on a regular basis. In this way, insight is provided into the relation between the nature of visual function impairments, cycling difficulties, and cycling cessation. More specifically, this study provides insight into the appropriateness of the visual acuity guideline currently used, which suggests that independent cycling is unsafe with visual acuity below 0.1. Assuming this guideline is accurate, respondents with visual acuity below 0.1 would be more likely to have ceased cycling, cycle less kilometres, and be discouraged from cycling by friends and relatives, compared to respondents with visual acuity slightly above 0.1.
Method
Respondents
Between February 2016 and July 2017, both visually impaired and normally sighted people were invited to complete an online questionnaire. Recruitment occurred through newsletters, websites, and social media of Dutch vision rehabilitation centres and patient organisations. Visually impaired respondents were asked to invite one or two normally sighted peers, in an effort to obtain a matched control group. The respondents needed to be able to understand Dutch and have experience with independent cycling. Independent cycling is defined as traffic participation without the support of someone else, on a single-seat bicycle with at least two wheels. There were no restrictions regarding age, gender, or education. For ethical reasons, children under 12 years of age were not allowed to participate. Instead, a parent or caregiver could complete the questionnaire on his or her behalf. Respondents aged 12–16 years needed permission from a caregiver to participate. The University of Groningen Psychology Ethics Committee provided approval for this study, and the respondents did not receive financial compensation.
Questionnaire
The questionnaire was constructed and administered using Qualtrics software (Qualtrics, 2015). The questions were presented in Dutch using a sans serif font, a high-contrasting background, and large tick boxes to optimise the visual accessibility. The respondents accessed the questionnaire through the public website of Royal Dutch Visio, a Dutch centre of expertise for blind and partially sighted people. The goal of the study was explained and participation took approximately 25 minutes. Respondents gave informed consent by continuing. The questions concerned independent cycling during daytime and focussed on barriers to cycling due to eyesight despite wearing optimal correction.
Sixty-three closed-ended questions were clustered into four themes based on the ICF (WHO, 2001): (1) body structures and functions, for example, visual conditions, visual acuity and field, and physical and mental issues; (2) activity of cycling, for example, vehicle control and compensation; (3) participation, for example, the importance of the cycling ability; and (4) contextual factors, for example, environmental and personal factors. The questionnaire concluded with demographic and general questions, for example, about recent accidents, features of the respondent’s bicycle, and the use of cycling aids.
Respondents indicated to which extent they experience or experienced difficulties with theme-related aspects of cycling, which had been identified in Jelijs et al. (2018). For example, the respondents were asked, ‘Please indicate to what extent the following issues make it difficult for you to cycle independently’, followed by a contextual factor such as ‘bumps in the road surface’ or ‘cycling skills’. They answered this question on a 5-point Likert-type scale, ranging from ‘Not difficult at all’ to ‘Very difficult’. Similarly, former cyclists indicated to which extent these factors were decisive for them to cease cycling.
Analysis
A key distinction was made between respondents who reported that they no longer cycled independently (‘former cyclists’) and those who cycled regularly in the 12 months before participation (‘cyclists’). Furthermore, the visually impaired respondents were grouped based on both their self-reported binocular visual acuity and peripheral field loss. Respondents with acuity below the Dutch informal cycling guideline of 0.1 were classified as having ‘very low acuity’. Those with acuity slightly above the guideline (0.1 ⩽ BVA < 0.2) were classified ‘low visual acuity’. Respondents with a BVA ⩾ 0.2 were categorised as ‘moderately impaired to normal visual acuity’. In addition, a group with ‘unknown acuity’ was created. For the purpose of this study, different types of peripheral field loss (e.g., hemianopia and tunnel vision) were converted into a dichotomous variable (yes versus no)
Potential relationships were studied between the independent variable ‘cycling’ and dependent variables based on visual functions and circumstances not directly related to vision loss. The appropriateness of visual acuity of 0.1 as critical for cycling was examined by inspecting whether most respondents with very low visual acuity, but without peripheral field loss, had ceased independent cycling. Based on the visually impaired cyclists’ responses, per theme an overall top-five of most frequently reported issues was generated. These overall top-five items were compared to the scores of the normally sighted control group as well as to the scores of cyclists with either visual acuity loss (BVA < 0.2) and no peripheral loss or peripheral field loss and moderately impaired to normal visual acuity. Finally, comparisons were made between the visually impaired cyclists’ top-fives and the former cyclists’ five most frequently mentioned determinants of ceasing cycling.
The data were analysed using IBM SPSS Statistics 23 and Microsoft Excel 2010. Nominal variables were analysed through Pearson’s chi-square tests, Fisher’s exact tests, and non-parametric point biserial correlation (rspb). Mann–Whitney U-tests were used when parametric test assumptions were not met, for example, regarding the Likert-type-scale items.
Results
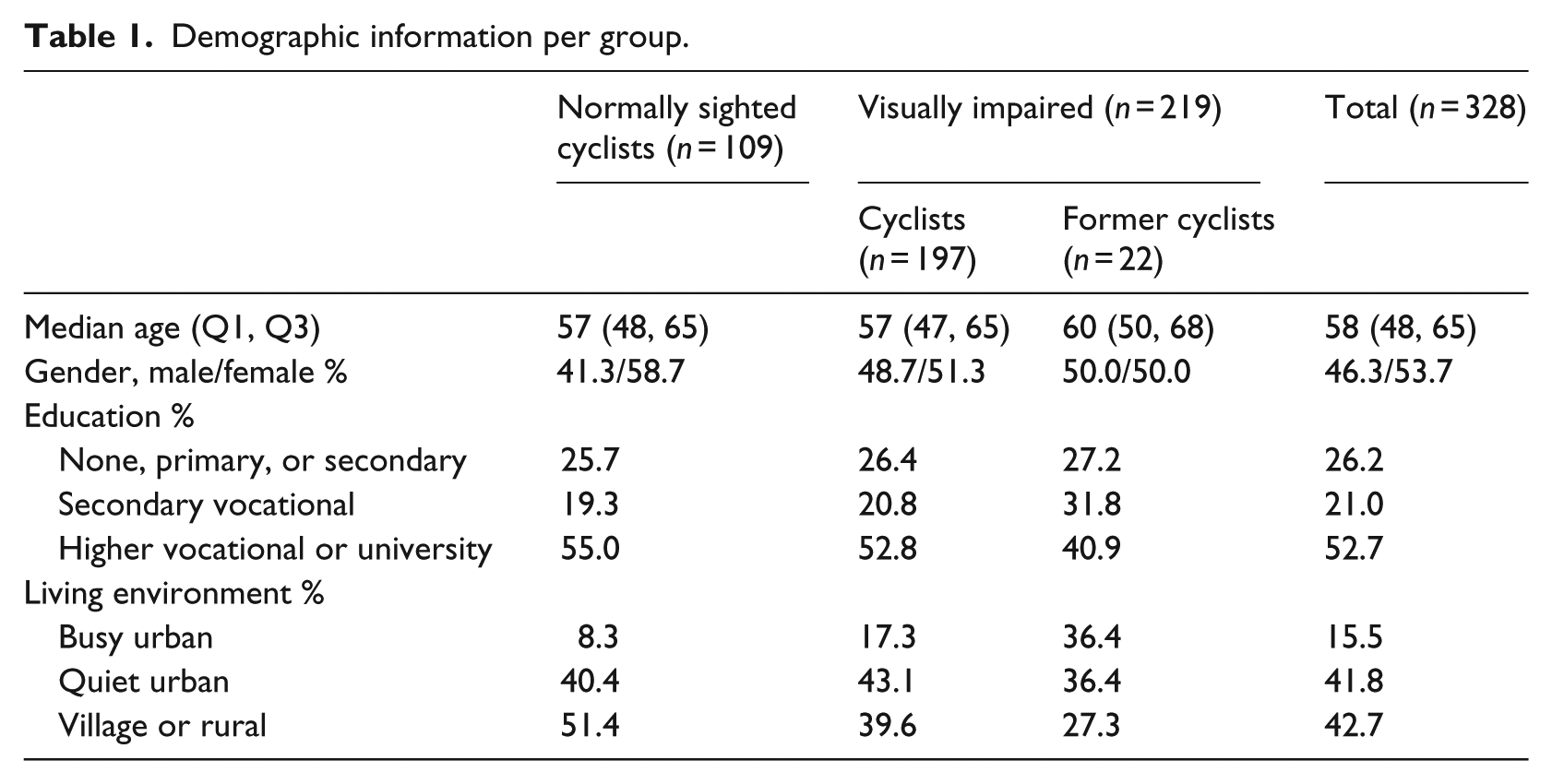
In total, 342 questionnaires were completed. Nine were excluded because of unusable or contradictory answers with regard to the functional impairment. Remaining respondents were 109 (33%) normally sighted and 224 (67%) visually impaired individuals from the Netherlands (n = 330) and Belgium (n = 3). The visually impaired group consisted of 197 cyclists and 27 former cyclists. Five respondents in the former cyclists group were excluded from further analyses because physical or mental limitations were at least as decisive for ceasing independent cycling as visual limitations. Table 1 presents the demographic information of the respondents. There were no differences between the groups regarding age, χ2(2) = 0.196, p = ns; gender, χ2(2) = 1.692, p = ns; and education, χ2(4) = 2.100, p = ns. With regard to living environment a difference between the three groups was found, χ2(4) = 14.117, p = .007, representing that relatively many former cyclists lived in an urban area. Figure 2 shows the frequencies of the visually impaired respondents’ visual conditions.
Demographic information per group.
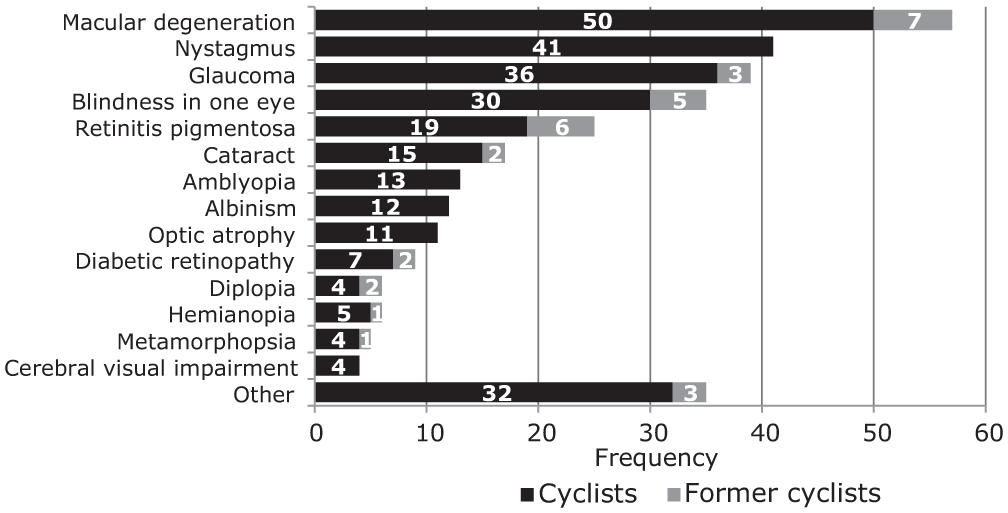
Frequency of visual function impairments experienced by the visually impaired cyclists (black, n = 197) and former cyclists (grey, n = 22). Respondents were allowed to enter multiple options.
Visual functions
Visual acuity
Respondents with peripheral field loss (n = 95) or unknown visual acuity (n = 8) were excluded from the low visual acuity analyses. No difference was found between the proportion of former cyclists in the group with visual acuity below 0.1 (n = 23) versus above or equal to 0.1 (n = 93; p = ns, two-tailed Fisher’s exact test). Table 2 shows that among the very low visual acuity respondents (n = 23), 3 (13%) reported they no longer cycled versus 20 (87%) who reported they still cycle. The low visual acuity group (n = 41) contained 2 former cyclists (5%). This difference in former cyclists proportion was not significant (p = ns, two-tailed Fisher’s exact test).
Grouping of visually impaired cyclists and former cyclists based on binocular visual acuity and peripheral field loss.
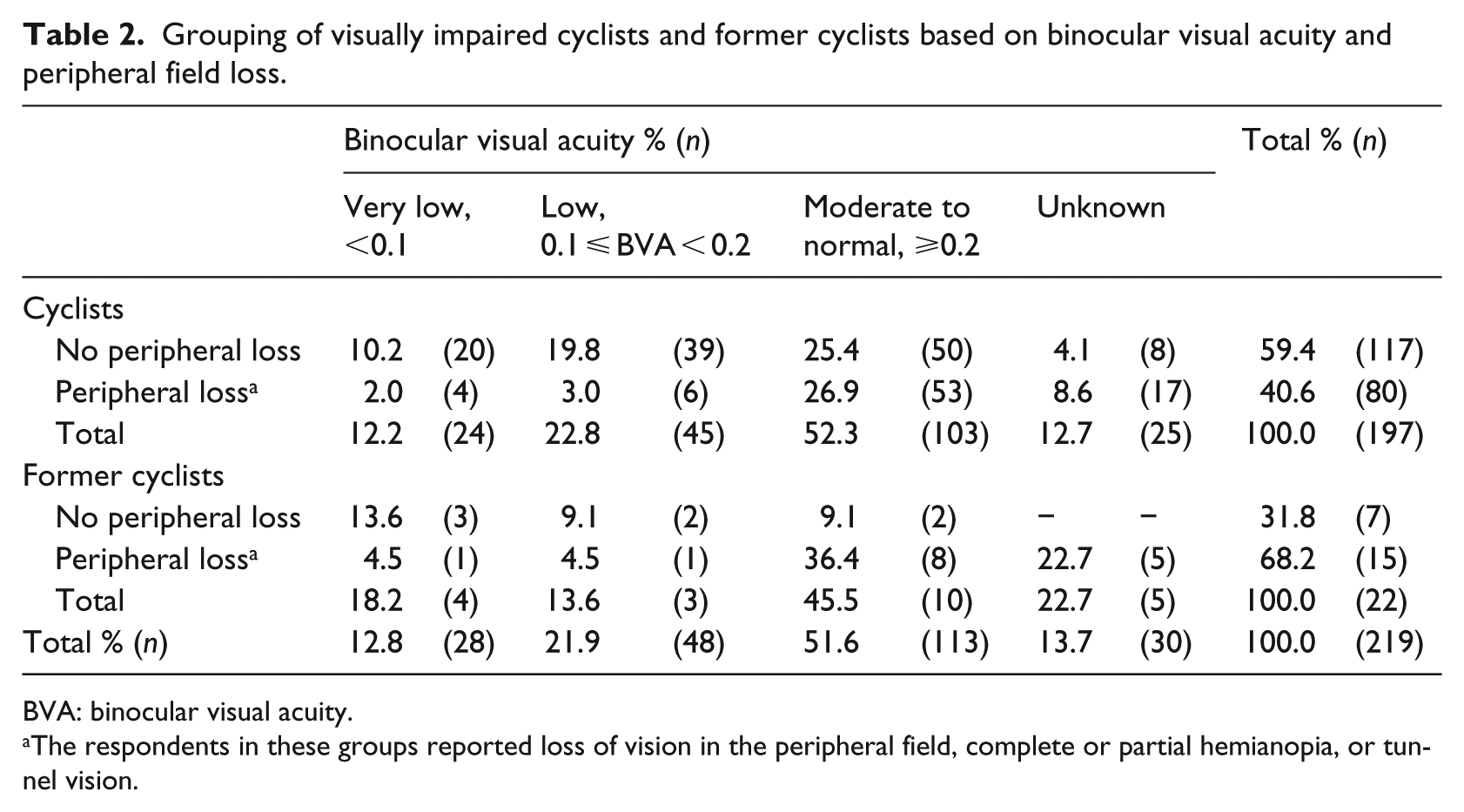
BVA: binocular visual acuity.
The respondents in these groups reported loss of vision in the peripheral field, complete or partial hemianopia, or tunnel vision.
The median self-reported weekly cycling distance in the normally sighted cyclists (n = 109) was 25 km. No difference was found (U = 283, z = –1.72, p = ns, r = –.22) regarding the estimated weekly cycling distance in the low visual acuity cyclists (n = 39, Mdn = 25 km) versus the very low visual acuity cyclists (n = 20, Mdn = 42.5 km). Very low visual acuity cyclists did not cycle less kilometres than low visual acuity cyclists. In fact, 85% of the very low visual acuity cyclists reported they cycle on a daily basis, while 67% of the cyclists in the low visual acuity group cycled daily (compared to 56% in the normally sighted cyclists, 75% with unknown BVA, and 70% with BVA ⩾ 0.2).
The frequency in which the very low visual acuity cyclists considered to cease independent cycling in the previous 12 months did not differ from the low visual acuity cyclists (U = 355.5, z = –0.79, p = ns, r = –.10). The majority of very low visual acuity cyclists (85%) and low visual acuity cyclists (77%) had not considered to cease cycling at all. No difference was found regarding the frequency in which friends or relatives of cyclists in these groups discouraged them from independent cycling (U = 294, z = –1.72, p = ns, r = –.22). Among the very low visual acuity cyclists, 80% indicated that friends or relatives at least occasionally discouraged them from independent cycling in the previous 12 months (vs 62% of low visual acuity cyclists).
With regard to reporting accidents and near-accidents no difference was found between the low visual acuity versus the very low visual acuity cyclists (U = 383.5, z = –0.12, p = ns, r = –.02). Figure 3 shows that most cyclists in the low visual acuity (59%) and very low visual acuity (55%) groups reported they had not experienced any accidents or near-accidents in the previous 3 months. In addition, no difference in reported accidents or near-accidents was found between cyclists with visual acuity loss (BVA < 0.2) versus cyclists with moderately impaired to normal visual acuity (U = 1214.5, z = –1.92, p = ns, r = –.18). Among the normally sighted respondents, 79% reported they had not experienced any accidents or near-accidents in the previous 3 months.
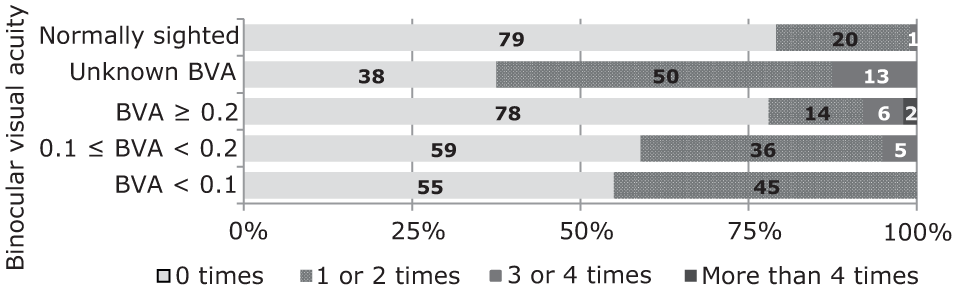
The self-reported frequency of accidents or near-accidents experienced in the previous 3 months by normally sighted cyclists (n = 109) and cyclists (without peripheral loss) with unknown visual acuity (n = 8), moderately impaired to normal visual acuity (n = 50), low visual acuity (n = 39), and very low visual acuity (n = 20).
Peripheral field loss
Respondents with very low (n = 28) or unknown (n = 30) visual acuity were excluded from the peripheral field loss analyses. A relationship was found between cycling and whether or not the respondent reported having peripheral visual field loss, n = 161, χ2(1) = 4.24, p = .046. Based on the odds ratio, this association represents that the odds of independent cycling are 3.39 times higher if a person does not experience peripheral field loss than if a person does. However, the association between these variables is small (φ = –.16, p = .046).
A difference was found in the number of accidents or near-accidents reported by cyclists without (n = 89) versus with (n = 59) peripheral field loss (U = 1597.5, z = –4.51, p < .001, r = –.37). Figure 4 shows that 31% of those without peripheral field loss versus 69% of cyclists with peripheral field loss reported they had experienced at least one accident or near-accident in the previous 3 months. The effect size (r = –.37) represents a medium association between peripheral field loss and the reported number of accidents or near-accidents.

The self-reported frequency of accidents or near-accidents experienced in the previous 3 months by low to normal visual acuity cyclists without (n = 89) versus with (n = 59) peripheral field loss.
Cyclists with peripheral field loss more frequently considered to cease cycling in the previous 12 months than those without peripheral field loss (U = 2206, z = –2.218, p = .027, r = –.18). In the cyclists without peripheral field loss 17% reported they had at least occasionally considered to cease cycling in the previous 12 months, while in cyclists with peripheral field loss 34% reported this. No difference was found in the frequency in which friends or relatives of cyclists in these groups discouraged them from independent cycling (U = 2243, z = –1.659, p = ns, r = –.14). Among the cyclists with peripheral field loss, 64% indicated that friends or relatives at least occasionally discouraged them from cycling (vs 54% in the cyclists without peripheral field loss).
Difficulties related to visual functions
The top-five of in total 13 issues related to visual functions that visually impaired cyclists mentioned were related to light–dark transitions, seeing obstacles or other traffic participants, excess of light, and seeing objects that are far away. Figure 5 shows the extent to which the respondents experienced difficulties with the according items.
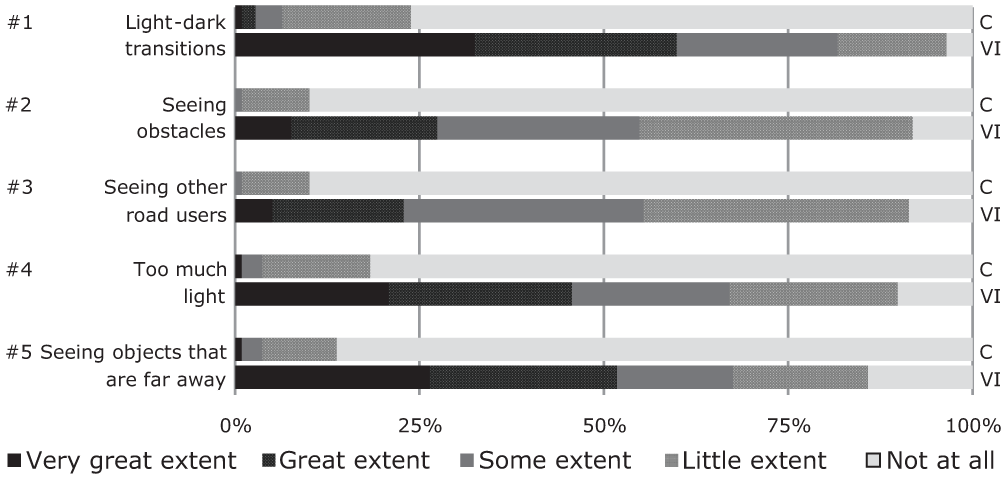
The visually impaired cyclists’ ([VI]; n = 197) top-five of issues related to visual functions that impede cycling. The upper bars represent the responses of the normally sighted control group ([C]; n = 109).
The top-five of the cyclists with visual acuity loss (BVA < 0.2) and no peripheral field loss (n = 59) is identical to the overall visually impaired cyclists’ top-five. Cyclists with peripheral field loss and moderately impaired to normal visual acuity (n = 53) indicated having most difficulties with seeing other road users and obstacles. Their top-five included ‘seeing contrasts’ instead of ‘objects that are far away’. The issues presented in Figure 5 were also mentioned by former cyclists as the five most pivotal issues related to visual function to cease independent cycling.
Activity of cycling
Difficulties related to bicycle control
The respondents indicated to which extent they experience difficulties with 24 aspects of bicycle control. Figure 6 shows that visually impaired cyclists indicated experiencing most difficulties in: crossing intersections without traffic lights, overviewing the traffic situation, anticipating to other traffic participants or the road’s trajectory, and finding the correct route.
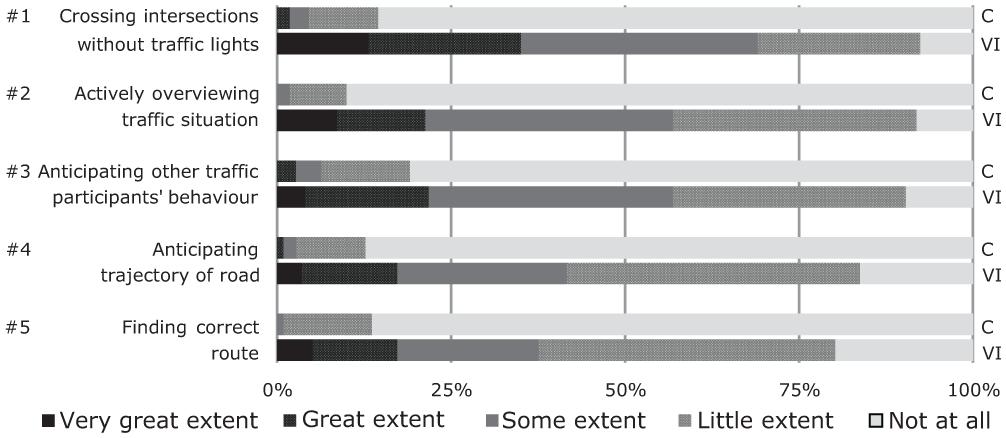
The visually impaired cyclists’ ([VI]; n = 197) top-five of issues related to bicycle control that impede cycling. The upper bars represent the responses of the normally sighted control group ([C]; n = 109).
The difficulties presented in Figure 6 are included in the top-five of the cyclists with visual acuity loss (BVA < 0.2) and no peripheral field loss (n = 59). Likewise, this applies to cyclists with peripheral field loss and moderately impaired to normal visual acuity (n = 53), except ‘finding the correct route’. Instead, their top-five included difficulties with ‘merging into traffic’. They also indicated having more difficulties with ‘noticing they are being overtaken’ and ‘choosing the distance between other traffic or the kerb’ than finding the correct route. In addition to the first four issues presented in Figure 6, the former cyclists indicated ‘passing static objects along the road (e.g., parked cars)’ and ‘merging into traffic’ as the most pivotal issues related to bicycle control in their decision to cease cycling.
Compensation
Among the visually impaired cyclists, 81% (n = 160) reported they avoid specific manoeuvres or circumstances (e.g., by dismounting the bicycle or taking a different route) versus 14% (n = 15) in the normally sighted cyclists. The visually impaired cyclists particularly avoided cycling when the roads are slippery (62%), cycling in the dark (59%), and cycling in dense traffic (56%) versus 12%, 4%, and 8% in the normally sighted cyclists, respectively.
Five visually impaired cyclists (3%) indicated they most frequently rode a bicycle with three or more wheels in the previous 12 months versus one normally sighted cyclist (1%). There were 40 visually impaired cyclists (20%) versus 19 normally sighted cyclists (17%) who reported they most frequently rode a pedal electric bicycle (pedelec), which gives pedal-support up to 25 km/h. The three cycling aids most frequently used by the visually impaired cyclists were as follows: glasses to improve the ability to see details (47%), glasses to protect against light (47%), and visors to protect against light (14%) versus 47%, 3%, and 2% in the normally sighted cyclists, respectively.
Contextual factors
Difficulties related to contextual factors
The respondents were asked to which extent 23 contextual (i.e., environmental and personal) factors made independent cycling more difficult. The five most obstructing factors according to the visually impaired cyclists were as follows: other traffic participants’ bad visibility and unpredictable behaviour, obstacles, bumps in the road surface, and the amount of traffic in their immediate vicinity (see Figure 7).
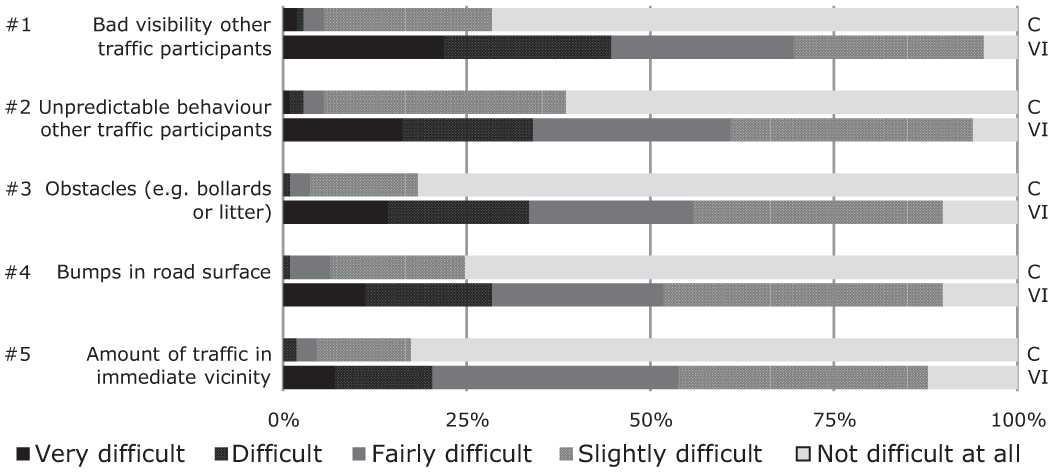
The visually impaired cyclists’ ([VI]; n = 197) top-five of contextual factors that impede cycling. The upper bars represent the responses of the normally sighted control group ([C]; n = 109).
Cyclists with visual acuity loss (BVA < 0.2) and no peripheral field loss (n = 59) mentioned having most difficulties with the first four issues shown in Figure 7. This group mentioned ‘unfamiliarity with the route’ as more obstructing than the ‘amount of traffic in the immediate vicinity’. The top-five of cyclists with peripheral field loss and moderately impaired to normal visual acuity (n = 53) included each of the issues shown in Figure 7. In addition, ‘unfamiliarity with the route’ tied for the fifth place. The former cyclists’ top-five determinants of ceasing cycling included the first four issues presented in Figure 7. They mentioned ‘precipitation’ more frequently as determinative for ceasing cycling than the ‘amount of traffic in the immediate vicinity’.
Cycling and respondent characteristics
No associations were found between whether or not the visually impaired respondents still cycle and the availability of alternative means of transport (p = ns, two-tailed Fisher’s exact test) or the respondents’ age (rspb = –.06, p = ns), gender, χ2(1) = 0.01, p = ns, education level (p = ns, two-tailed Fisher’s exact test), living environment (p = ns, two-tailed Fisher’s exact test), or household composition (p = ns, two-tailed Fisher’s exact test).
An association was found between cycling and whether or not the respondent was born with the vision impairment, χ2(1) = 4.80, p = .040. Among the respondents with a congenital vision impairment (n = 98) 95% (n = 93) reported they cycle independently versus 86% (n = 104) of those who acquired the vision impairment in later life (n = 121). Based on the odds ratio, this association represents that if the person has a congenital vision impairment the odds of independent cycling are 3.04 times higher than when the person acquired the visual condition at a later age. However, this association is small (φ = –.15, p = .040). Differences were found between cyclists with congenital versus acquired vision impairment in the cycling difficulties related to visual functions, bicycle control, and contextual factors. Compared to cyclists with congenital impairments, cyclists with acquired impairments reported having more difficulties with light–dark transitions, distorted vision, and seeing objects that are nearby. With regard to bicycle control, they indicated having more difficulties with taking left turns, choosing the distance between others or the kerb, overtaking, noticing timely that they are being overtaken, and mounting, stopping, and dismounting the bicycle. They indicated having more difficulties with contextual factors, namely: obstacles, bumps in the road surface, and hearing. The only aspect that was more impeding for cyclists with a congenital vision impairment was having a bad quality bicycle. The test statistics of these issues are presented in Table 3.
Mann–Whitney U-test results of cycling issues in cyclists with congenital (n = 98) versus acquired (n = 121) vision impairment.
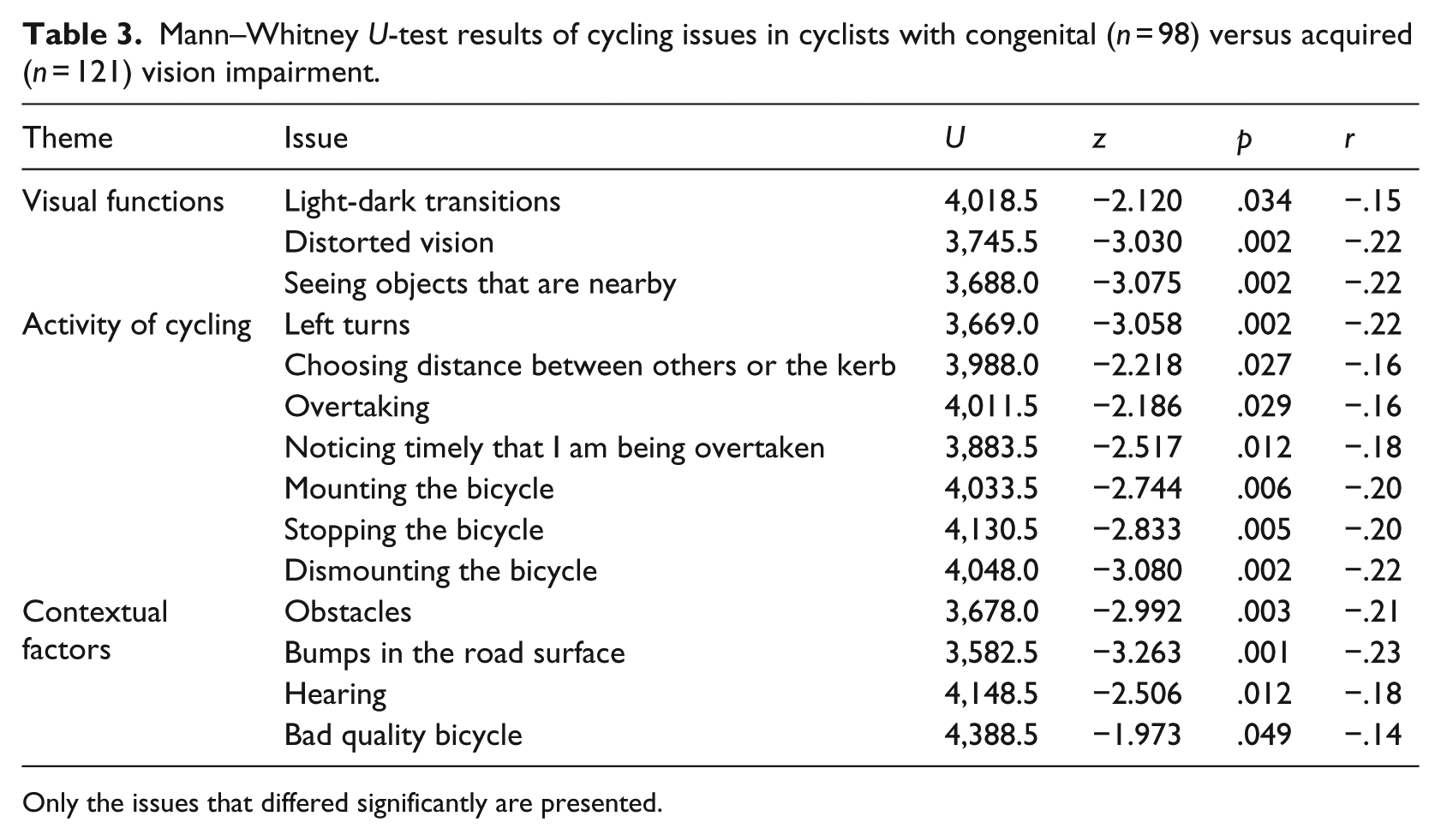
Only the issues that differed significantly are presented.
Discussion
The present study aimed to give an overview of the difficulties that visually impaired people experience regarding independent cycling. Visually impaired former cyclists indicated the extent to which difficulties were decisive for them to cease cycling. In addition, the current study examined the appropriateness of the informal visual acuity guideline for cycling used in most Dutch vision rehabilitation centres. This guideline suggests that independent cycling is unsafe with visual acuity below 0.1.
Visual functions
Cycling difficulties experienced specifically by the cyclists with visual acuity loss (BVA < 0.2) and no peripheral field loss were seeing objects that are far away and route-planning. The present findings do not support using visual acuity below 0.1 as an absolute contra-indication for independent cycling. The appropriateness of this guideline appears to be low as the vast majority of the respondents with both very low visual acuity (BVA < 0.1) and no peripheral field loss indicated that they cycle on a regular basis. The cyclists in this group did not cycle less kilometres per week than those with low visual acuity (0.1 ⩽ BVA < 0.2). Our finding contradicts the findings of Wilhelm and Endres (2004) who concluded that visual acuity below 0.1 is not sufficient for cycling. Wilhelm and Endres (2004) also suggested that the occurrence of accidents increased in participants with visual acuity below 0.2. The results of the present study do not confirm such a relationship between visual acuity and the occurrence of accidents or near-accidents. This discrepancy may be partly explained by differences in bicycle habits and facilities between Germany and the Netherlands (see Hellmann, 2016), as the relative number of cycling accidents is lower in countries with a higher bicycle use (Dutch Ministry of Transport, Public Works and Water Management, 2009).
An association was found between experiencing peripheral field loss and whether or not the respondent cycles. The odds of cycling are approximately three times higher in individuals without peripheral field loss than in those with peripheral field loss. Cyclists with peripheral field loss reported that they more frequently (1) experienced accidents or near-accidents and (2) considered to cease independent cycling, compared with cyclists without peripheral field loss. They specifically reported having difficulties seeing contrasts, merging into traffic, noticing they are being overtaken, and choosing the distance to others or the kerb. The detrimental effect of peripheral field loss is in line with the personal experiences of Connor (1992), who argued that particularly persons with peripheral field loss have greater difficulties operating a bicycle. Based on Cordes et al. (2017), the negative impact of peripheral field defects also applies to operating other vehicles, such as mobility scooters.
The current results suggest that peripheral field loss is a better predictor for safe cycling than visual acuity. Similar to the respondents with visual acuity loss (BVA < 0.2), however, the vast majority of the respondents with peripheral field loss indicated they cycle regularly. Although the nature of the visual condition may induce specific difficulties with cycling, visual functions alone should not be used as predictors of the ability to cycle independently.
Activity of cycling
Route planning appears to be a crucial element of cycling in visually impaired people. The main difficulties with bicycle control they reported were crossing intersections without traffic lights and overviewing the traffic situation. The majority of these issues as well as light–dark transitions difficulties can be remedied by defining a route that meets the cyclist’s abilities and limitations. The vast majority of the visually impaired cyclists indicated they avoid specific situations or manoeuvres (e.g., by dismounting the bicycle or taking a different route). For example, they reported avoiding cycling when the roads are slippery, when it is dark, or when there is dense traffic. The importance of route planning is also recognised in Connor (1992) and in a study that primarily included participants professionally involved in low vision cycling (Jelijs et al., 2018).
As described above, the nature of the visual impairment may partly determine the difficulties experienced with bicycle control. Mobility instructors could examine the visually impaired individual’s difficulties with bicycle control, for example, by conducting an individual practical cycling test. Visually impaired persons who wish to cycle may be trained in taking strategic, tactical, and operational decisions in cycling that complement their (visual) limitations. The mobility instructors’ advice on cycling could depend on an individual practical test of the client’s ability to compensate for the difficulties induced by the visual limitations. The current findings acknowledge the importance of taking strategic decisions, including selecting a suitable route. Future research should point out how visually impaired cyclists compensate at each level of vehicle control. For example, they may also create more time to react to unexpected events by maintaining a larger distance to other road users or the kerb (tactical) or by reducing speed (operational).
Contextual factors
An important finding is that the five most impeding contextual factors reported by the visually impaired cyclists were all environmental factors. These factors concerned the other traffic participants’ bad visibility and unexpected behaviour and the quality and maintenance of the road. In contrast, in Jelijs et al. (2018), participants rated factors related to ‘personality and temperament’ as the second most important (72%). This discrepancy can be explained by the attribution theory (Heider, 1958). This theory concerns the individuals’ tendency to emphasise internal circumstances when describing others’ behaviour, whereas they emphasise external circumstances when describing their own shortcomings (Campbell & Sedikides, 1999).
Special attention should be paid to persons who acquired vision impairment in later life. An association was found between using the bicycle and whether or not the respondent was born with the visual condition. The odds of independent cycling are approximately three times higher in persons with a congenital visual condition compared to persons who acquired the visual condition in later life. Cyclists with acquired vision impairment indicated having more difficulties with aspects of bicycle control at both the operational level (e.g., mounting, stopping, and dismounting the bicycle) and the tactical level (taking left turns, overtaking, and maintaining distance between others or the kerb). This finding conflicts Connor (1992), who argued that congenitally visually impaired children encounter more cycling difficulties as they have more limitations in visual memory. However, congenitally visually impaired adults may be more used to their visual limitations than adults who acquired vision impairment in later life.
Determinants to cease cycling
The former cyclists’ determinants to cease cycling were similar to the visually impaired cyclists’ most frequently mentioned difficulties. With regard to controlling the bicycle, however, the former cyclists indicated that passing static objects and merging into traffic were more pivotal than finding the correct route. Regarding the contextual factors they indicated that precipitation was more decisive than the amount of traffic in the immediate vicinity.
It is difficult to determine how many respondents in the former cyclists group would be able to compensate sufficiently to enable themselves to cycle independently in a safe manner. Based on the current results, it is expected that especially people with congenital vision impairments without peripheral field loss might be able to compensate sufficiently enabling them to cycle.
Study strengths and limitations
To the extent of our knowledge, this is the first study that identified the difficulties experienced by a large sample of visually impaired cyclists and former cyclists. Furthermore, this study provides crucial insight into the necessity of using guidelines for low vision cycling that are not based on visual functions alone. The difficulties identified in this study can be useful for mobility trainers of vision rehabilitation to provide clients who wish to cycle with a more tailored advice, for example, by designing and conducting individual practical cycling tests.
There were a number of limitations to the present study. First, this study focused on the Dutch cycling situation and the results may not be entirely generalizable to other countries. The present findings are important for independent mobility, particularly in countries with a relatively high cycling-accessibility and popularity. In counties with lower cycling accessibility, on the other hand, visually impaired people may choose more consciously to use the bicycle as a means of transport. The present results could provide useful guidance when they consider to cycle.
Despite the effort to optimise accessibility, the sample used may be biased. It cannot be ruled out that there were people who could not complete the questionnaire due to visual or digital inaccessibility. Compared to the number of visually impaired cyclists, there were fewer normally sighted and visually impaired former cyclists included. Possibly, there is a relationship between the ability to participate and the ability to cycle. The present study was possibly less in the interest of these groups. For this reason, the visually impaired respondents invited the normally sighted respondents, so they were not selected randomly. Furthermore, a difference in living environment was found between the three groups. Possibly, some differences in cycling issues may be related to this group difference regarding the living environment.
The reliability of the grouping of respondents is uncertain as the grouping was partly based on the respondents’ self-reported visual acuity and visual field limitations. Some respondents possibly did not have correct or recent information about these visual functions. The groupings of peripheral field loss and congenital visual impairment were simplified substantially by converting them into dichotomous values. In theory, respondents missing 10 degrees and 120 degrees in their peripheral field were grouped together. The fact that some congenital visual conditions are degenerative or develop in later life was not taken into account.
It is unclear to what extent the present results apply to cycling in the dark as this study was limited to cycling during daytime. Future studies could also focus on bicycle-specific difficulties as the present study made no distinction between riding a conventional bicycle, pedelec, or tricycle.
Conclusion
The present results suggest that the visually impaired people’s ability to cycle independently in a safe manner does not depend on visual functions alone. Most respondents who did not meet the cycling guidelines currently used in Dutch vision rehabilitation compensate sufficiently for their limitations, which enables them to cycle independently. This implies that using guidelines based on visual functions alone unnecessarily reduces the independent mobility of many visually impaired people.
Instead, mobility instructors in vision rehabilitation could give their cycling training and advice based on an individual practical test of the client’s ability to compensate for the cycling difficulties induced by the vision limitations. The present identification of cycling difficulties could assist mobility trainers in developing cycling tests and training programmes. Overall, the visually impaired cyclists indicated having most difficulties with light–dark transitions, crossing intersections without traffic lights, and other traffic participants’ bad visibility. The nature and origination of the visual function impairment may induce specific difficulties in cycling. For example, cyclists with low visual acuity indicated having difficulties with seeing objects that are far away and route-planning. Cyclists with peripheral field loss reported having particular difficulties, including merging into traffic, noticing they are being overtaken, and choosing the distance to others or the kerb. Furthermore, respondents with an acquired vision impairment indicated having specific difficulties, including mounting, stopping, and dismounting the bicycle. The former cyclists’ determinants to stop cycling were very similar to the difficulties reported by those who still cycle. Future research should focus on the compensation strategies that visually impaired cyclists use to remedy their difficulties in cycling.
Footnotes
Acknowledgements
The authors thank all participants who took part in this study, Else Havik for her support regarding the questionnaire’s lay-out, and Anselm Fuermaier for assisting with data analysis.