
Abstract
Arguably, individuals living with deafblindness are among the hardest hit by the effects of the corona virus disease of 2019 (COVID- 19), given the importance of the sense of touch for their ability to interact with the world. To address this challenge, it is imperative to facilitate the implementation of evidence- and experience-based recommendations, and to improve knowledge translation on a global scale. Deafblind International organized a webinar to provide a platform where participants could exchange experiences and solutions to overcome the challenges created by the arrival of COVID-19, in order to facilitate information exchange among stakeholders in deafblindness during this pandemic. We present an overview of its content here and place the summarized themes in context with existing research literature. Abstract submission was open for 4 weeks in May 2020, resulting in 30 submissions from 13 countries across 5 continents. Of the 26 presenter teams, 9 (35%) had a co-presenter that was living with deafblindness themselves. The number of individual participants across all sessions ranged from 55 to 140 (M = 98), with a total of 3709 session registrations overall, and the organizers estimate a total attendance of around 400 participants. Based on extensive field notes taken during the webinar, and repeated viewing of the recordings, qualitative description allowed the team to synthesize eight principal themes across the event: access to information, communication, service accessibility, adaptations to service delivery, online safety and security, physical distancing, mental health and research. The first Deafblind International webinar was able to fill an important gap by bringing together a variety of stakeholders in deafblindness across the globe. The event created a sense of group membership and peer support, brought the participants, researchers, the professionals as well as their service agencies closer together and generated a sense of hope and collaboration.
‘Keep calm and carry on being deafblind!’
The international research response to the corona virus disease of 2019 (COVID-19) has been remarkable, launching international efforts in the development of treatments, vaccines and multiple other related avenues to improve our ability to cope and overcome this pandemic. An increased risk for marginalized subgroups of the population, for example, older adults (Jordan et al., 2020), various ethnic groups (Khunti et al., 2020) or individuals with pre-existing health conditions (Zhou et al., 2020), disabilities (Armitage & Nellums, 2020) or patients with mental health disorders (Pereira-Sanchez et al., 2020) has been investigated. Mainstream media have paid specific attention to individuals living with deafblindness: In an article in The New Yorker, Robin Wright (2020) explored how the lives of persons living with deafblindness are being touched by the COVID-19 pandemic. Intuitively, the concept of physical distancing is difficult to consolidate with persons living with deafblindness, given that their ability to communicate with the world around them primarily depends on the sense of touch. The sense of touch is the optimal form of providing support, security and togetherness. Simcock (2020) pointed at the importance of considering the specific needs of the deafblind population where touch is concerned during a time when physical contact of any kind creates a risk of infection, including their ability to access information, whether in person or on-line (Recite Me, 2020).
Interestingly, the effects of COVID-19 created unique communication barriers at multiple levels between the deafblind community and the individuals that provide professional or non-formalized care for them. Inter-personal interaction and information exchange required immediate adjustments, such as the wearing of gloves during the use of tactile sign language, the need to disinfect shared assistive devices, or the necessity to make clear-window masks available to facilitate communication with individuals who depend on speech and lip reading (Mendel et al., 2008; Reed et al., 2020). In addition, exchange of health information with and access to professionals became challenging, given that the lockdown closed the offices of many service providers, and virtual information exchange was neither readily available nor accessible as a tele-health tool for this vulnerable population during a time of uncertainty, misinformation and physical and social distancing.
There were immediate research and knowledge translation responses within and about the culturally Deaf, the audiologically deaf, as well as the blind community, with focus on uni-sensory impairment priorities and COVID-19-specific adaptations. For example, health care workers who interacted with persons living with hearing impairment reported that sound attenuation and the barrier to lip- and speech-reading were recognized early on by patients as main barriers to communication (Trecca et al., 2020). These findings were mirrored by two health care workers as well who self-described as deaf and discussed the implications for the D/deaf community (Grote & Izagaren, 2020). Furthermore, in-person sign language interpreters were being switched to remote interpreting roles due to COVID-19 (Mckee et al., 2020). Hearing services were soon centre-stage in a discussion about whether they are essential services, specifically in the context of speech-rehabilitation with children where language development would otherwise be threatened (Pattisapu et al., 2020).
To bring the importance of adaptations for persons living with vision loss to the forefront during the pandemic, the American Foundation for the Blind led the launch of the survey on the effects of COVID-19 (Rosenblum, 2020). It is interesting to note that the survey sample contains a considerable number of respondents that live with combined vision and hearing impairment; therefore, the forthcoming results will be of great interest to the deafblind community as well. As a response to the needs of home schooling, peer-reviewed work focused on the challenges that emerged early on when implementing videoconferencing for the purpose of educating children with visual impairment (Lewis, 2020). The needs of engaging parents in a new role increases both their confidence and competence, and challenged traditional viewpoints on what is or is not possible remotely. Similar barriers and facilitators have been discussed in the context of persons with visual impairment working remotely (Ginley, 2020), whereby it comes as no surprise that on-line accessibility of software, website and apps emerged as the main concern. However, the authors acknowledge the high level of accessibility of several videoconferencing software, such as Microsoft Teams, Google Meets and Zoom. While these and other sources present the situation of persons living with singly sensory impairment, the effect of COVID-19 has not been specifically examined for people with congenital or acquired deafblindness in the peer-reviewed literature yet, aside from being briefly mentioned as part of the disability considerations published by the World Health Organization (2020) who state that public health information and publications should be made accessible for persons with deafblindness.
To facilitate the implementation of such recommendation, to improve knowledge translation on a global scale and to bridge the distance between individuals living with deafblindness and the persons who care and work for and with them, Deafblind International organized a webinar to provide a platform where participants could exchange experiences, solutions and approaches to overcome the challenges created by the arrival of COVID-19. The webinar was specifically focused on facilitating independence, participation and quality of life for persons living with deafblindness. We present an overview of its content here and place the summarized themes in context with existing research literature while highlighting main outcomes and recommendations that are of shared relevance for the community of persons living with deafblindness and their allies.
Methods
Under the leadership of Deafblind International, the organizing committee was composed of Frank Kat, President of Deafblind International (DbI), at SintLucas, Netherlands; Mirko Baur, Vice-President of DbI, at Tanne, Switzerland; Jude Nicholas, at Statped & Haukeland University Hospital, Bergen, Norway; Saskia Damen, Vice-Chair of the DbI Research Network, at the University of Groningen & Royal Dutch Kentalis, Netherlands; Michelle Borton, at Sensity, Canada, and Walter Wittich, Chair of the DbI Research Network, at the University of Montreal, Canada. Wittich and Damen also operated as the scientific committee. The creation of the webinar was motivated by the cancellation of the World Blindness Summit in Madrid, Spain, and was held during Deafblind Awareness Week from June 22 to 26, 2020, using the Zoom Webinar platform (Zoom Video Communications, Inc.; https://zoom.us/webinar). Abstract submission was open for 4 weeks in May 2020 and was promoted using social media (e.g., Facebook, Twitter) as well as deafblind-specific email list-serves and the website of Deafblind International. The call for proposals, entitled ‘Living with Deafblindness in a New Reality’, resulted in 30 submissions from 13 countries across five continents, including Australia, India, the United Kingdom, the Republic of Ireland, Finland, the Netherlands, Germany, Norway, Sweden, Mexico, Brazil, the United States and Canada (see Table 1 for complete programme overview, titles and speaker names). The 26 selected live presentations each lasted 45 min, to allow the live international sign language interpreters to take 15-min breaks between presentations. Presenters were encouraged to present their content in teams of two, whereby the primary presenter would provide the content and share their screen and their PowerPoint presentation, while the secondary presenter would be able to follow the chat option in Zoom, and the Question & Answer feature, to facilitate interaction with the audience and to focus the primary presenter to answer relevant questions. Attendees were muted and their camera feed was disabled. Of the 26 teams, 9 (35%) had a co-presenter that was living with deafblindness themselves. Four teams utilized the co-presenter as a translator, whereby the presentation was held in Portuguese or Spanish and was then simultaneously translated by the co-presenter into English. All sessions were moderated by the lead author of this article who also acted as a discussant, allowing for the identification of continuities and commonalities among the presentations. The programme was organized to accommodate the time zones of the presenters as best possible; therefore, the first speakers would present during the evening Australian time, which would translate into early morning in the Americas, mid-day in Europe and afternoon across parts of Asia. Given the free registration for the event and the limited financial support that was available (see acknowledgements), live captioning was not possible during the webinar. The number of individual participants across all sessions ranged from 55 to 140 (M = 98), with a total of 3709 session registrations overall. It was not possible to identify the exact total number of individuals that attended the event, given confidentiality reasons for email protection; however, the organizers estimate an attendance of around 400 participants. The sessions across each day were recorded and are available for free online (https://www.deafblindinternational.org/webinars/).
Complete program overview for the Deafblind International Webinar, including titles and speaker names.

Note. Underlined names indicate presenters living with deafblindness.
Results
The lead author who also acted as conference host took extensive field notes during the webinar, for the purpose of summarizing common and priority themes that emerged across the 5 days of presentations. Using qualitative description (Sandelowski, 2000), he presented the co-authors with an initial draft of these themes, based on the field notes and repeated viewing of the recordings. The co-authors then edited these themes and their summary presentation until a consensus was reached that best represents the content overview of the webinar. These themes are as follows: access to information, communication, accessibility of services, adaptations to service delivery, online safety and security, physical distancing, mental health and research.
Access to information
Given what is well established as a main barrier for persons living with deafblindness (Wittich et al., 2016), it comes as no surprise that the most dominant theme for the webinar was access to information about COVID-19. Concerns were expressed about access to important daily updates that are presented via TV without live captioning or sign language interpretation. This topic varied widely across countries and reflected access to such services and the required resources to make such daily briefings accessible. Several speakers elaborated on the accessibility of videoconferencing. The webinar was held using Zoom, specifically to facilitate visual access to sign language interpretation; however, many participants criticized the absence of live captioning, a service that was beyond the budget possibilities of the organizers (but within the technical possibilities of using Zoom).
Communication
The barriers included not just technology accessibility, but speakers across all participating countries commented on the challenges of communicating COVID-19-related vocabulary and terminology through tactile and visual sign language. One presenter pointedly summarized this with the statement ‘Assume nothing and simplify whenever you can’ when describing optimal communication approaches for persons with deafblindness. Often neither clients nor service providers or interpreters were initially familiar with the necessary terms and signs to communicate concepts such as physical distancing or flattening the curve. The difference in terms between social and physical distancing is also worth mentioning in this context. This subtle yet important distinction has already been acknowledged in the context of care provision for persons with hearing impairment (West et al., 2020), but takes on even more importance for persons with deafblindness that rely on tactile communication, given that physical distancing automatically becomes an experience of social isolation. However, several speakers acknowledged the opportunity to be creative and to take advantage of the opportunity to advocate for the need to improve communication under current and future circumstances.
Speakers in the webinar repeatedly recognized the communication difficulties that arise from communication partners wearing face masks (one speaker demonstrated her clear mask during her presentation). A speaker with deafblindness mentioned the added challenge that is created by the combination of distancing and mask-wearing, whereby ‘In a store, if I ask a question a 6 feet distance, can’t ask a question, because I won’t hear the answer’. Several deafblind speakers wore masks while presenting because their communication supporters or sign language interpreters were in the same room for an extended period of time. Immediately, the importance of speech cues became obvious for all participating sighted audience members, given that cues from the lips and face greatly contribute to audio-visual speech perception (Legault et al., 2010; Summerfield, 1992).
The topic of tactile communication raised an interesting philosophical discussion about ‘touch as a right’ in opposition to some of the policies that were enacted in response to COVID-19, thereby further isolating vulnerable individuals of all ages. The presenters referred to the concept of the dignity of risk, that has previously been discussed in the context of persons with mental and physical disabilities (Perske, 1972; Schloss et al., 1993). According to this principle, all individuals have the right to decide the risks they are willing to take, as an expression of their ability to choose, as well as their autonomy and control over their lives (Nay, 2002). Such a view of dignity and autonomy also aligned with the view of older adults with deafblindness through the lens of the United Nations Principles for Older People which clearly acknowledge the importance of independence and dignity (Simcock & Wittich, 2019). However, the reality of COVID-19 removed the decision of taking the risk of touch from many persons with deafblindness. In part, this decision was made for them by other persons who were unwilling to engage in haptic interactions; in part, safety policies limited touch without considering the choice of persons with deafblindness to engage in tactile interaction.
Accessibility of services
A large number of presentations included reports on how services were adjusted to accommodate the safety and security regulations that were put in place to protect both persons with deafblindness, their family and informal care givers, as well as their service providers. Tele-service provision became the standard for most presenters, and was widely presented as highly successful in many circumstances. However, various challenges were described that will require additional attention as the pandemic will unfold. For example, not all service recipients have access to WIFI or an internet connection with sufficient bandwidth to make videoconferencing viable. Those clients that depend predominantly on tactile communication are unable to benefit from tele-services; however, not all service providers were able or legally allowed to be physically close enough to communicate directly. Several speakers impressed with creative solutions, including WIFI-sharing among neighbours, or the use of accessible social media platforms for communication. All the while, questions of confidentiality and online security were being considered, where guidelines and regulations had not yet been developed or distributed, and the quality and accuracy of information available through such channels was questioned.
Adaptations to service delivery
This need for tactile and haptic interaction was also highlighted in presentations about accommodations to service provision. Researchers at the University of Groningen and Royal Dutch Kentalis, Netherlands, presented their work on communication coaching for parents (Damen et al., 2015), but now using more online video-feedback. Rorije explained that in her PhD study, the purpose of online video-feedback was to facilitate the involvement of parents in a communication intervention for persons with deafblindness. Hagen explained that the ability to support parents via video and the provision of online coaching became especially useful in a time of COVID, when children with deafblindness were not able to visit the Kentalis early intervention centre or school, and stayed home with their parents. The researchers are now evaluating whether this online coaching is indeed effective. Several of the presenters based in Canada mentioned the progress that was made at the policy level, whereby intervenor services are now recognized as an essential service through an Ontario Provincial Announcement. Service access entitlement was increased from 3 to 24 h per week; however, some of the intervenors expressed concerns about levels of work–life blend, given that remote working from home resulted in difficulties separating personal and professional time. Still, several speakers acknowledged a certain organizational resilience, complimenting their staff and management on their ability to focus on health and wellness, peer-to-peer and supervisor support.
Online safety and security
Researchers as well as service providers mentioned some of the barriers that need to still be addressed around authorship rules for sharing materials online and considerations around online privacy. Concerns about online safety were echoed by the director of the Youth Network of Deafblind International, Simon Allison, who was forced to cancel a networking event. He presented his work on developing an online alternative aimed at engaging youth with complex sensory needs. He used the Zoom waiting room feature to screen attendance, and to give parents a brief break at home while their youth could participate in safe team activates online. Several participants specifically acknowledged their inexperience with online tools, and their concerns about ‘breaking the rules’ unintentionally. One presentation team specifically discussed this topic in the context of communication needs with a remote client. While email communication was accessible, it was not recommended as a communication tool for confidential information; however, the decision to adhere to such regulations during a pandemic may not always be possible. Therefore, difficult choices need to be made between the communication needs of a client and the feasibility of service provision remotely.
Physical distancing
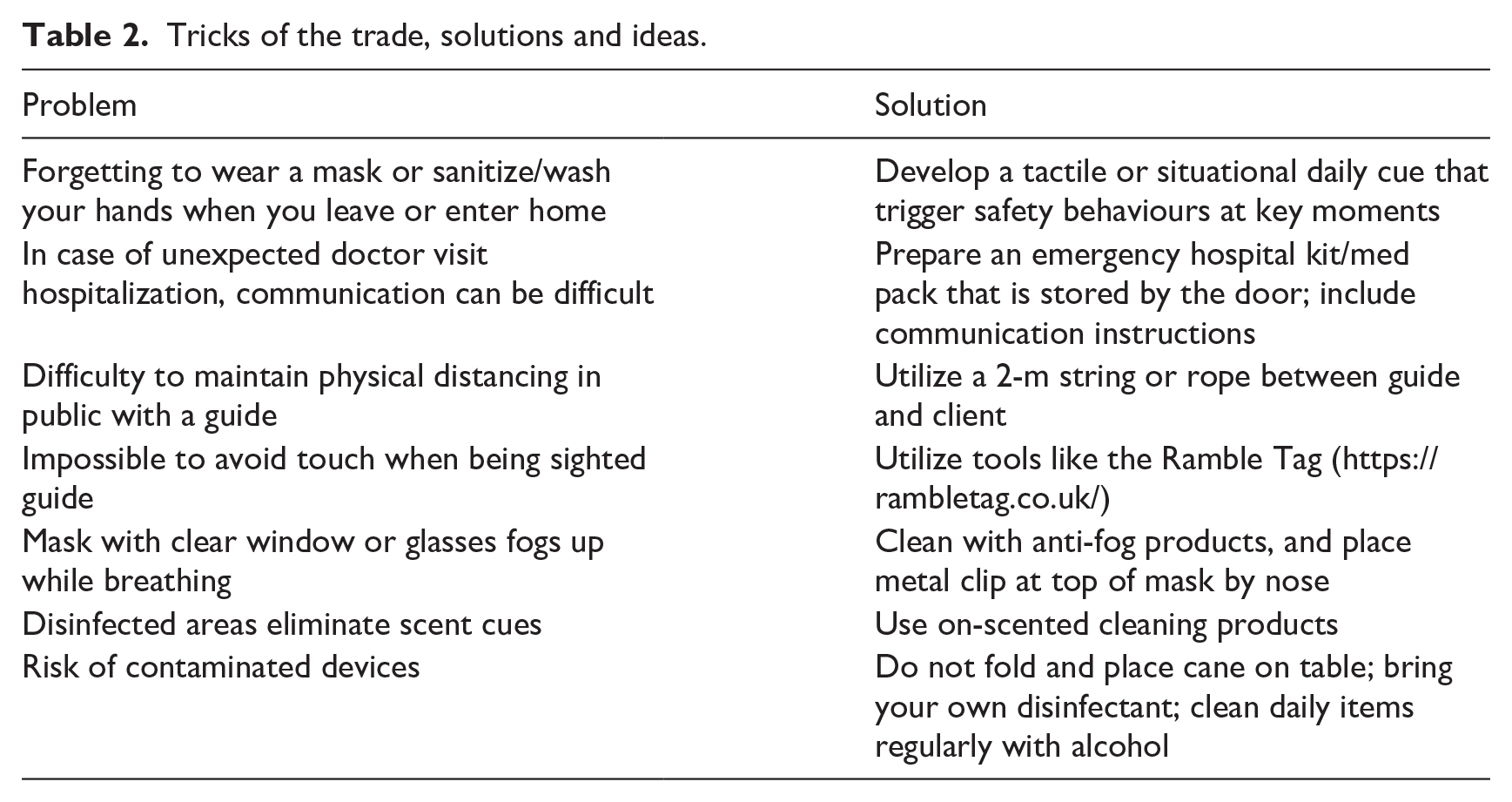
Most presenters mentioned the challenges associated with physical distancing, giving a variety of example, including guide dogs that are incapable of respecting distancing. However, facilitators that were mentioned included the use of gloves and personal protective equipment during tactile communication, ropes of 2-m length that are used between sighted guide and client during travel in open spaces, and family members that are now more engaged in the care of persons living with deafblindness. In addition, participants shared several ideas and solutions for specific problems (see Table 2).
Tricks of the trade, solutions and ideas.
Mental health
Loneliness and social isolation are well documented as a central problem for persons living with deafblindness (Lieberman & MacVicar, 2003; McInnes, 1999). Lockdown meant further isolation of residents in group homes for the deafblind. Several participants mentioned efforts to overcome these challenges. Zoom visits were scheduled to connect people, providing iPads in cases where technology was missing in home of DB persons. Webinars were developed on topics such as art therapy and mental health maintenance. Person-centred support was and is ongoing in a new way. All parties involved have acquired new technology skills, with special focus on those with limited communication skills and lack of access to technology. Stress management was frequently discussed by all participants, independent of their connection to deafblindness. Themes such as worry about the future, finance, home and health have previously been presented in the context of aging with deafblindness (LeJeune, 2010). Lockdown also meant changes in the routine for children with congenital deafblindness. Parents of children with congenital deafblindness may experience considerable amounts of stress and impaired emotional well-being due to disruptions to the schedules at home during the pandemic. Previous research also acknowledged the distress that is often accompanied by deafblindness, at the level of the affected individual and/or their family members (e.g., Dammeyer, 2014; Wulffaert et al., 2009); however, the stress caused by COVID-19 obviously takes on a different dimension that yet needs to be further explored.
Research
Some of the presenters took a research perspective on the pandemic, pointing at facilitators, barriers and priorities that need to be considered. Based on his previous work in social participation and deafblindness (Jaiswal et al., 2018, 2020), Jaiswal presented a collaborative possibility for citizen engagement and international team building. The goal of this proposal was to identify common research priorities that may now emerge as a result of the pandemic and that can be addressed globally in collaboration. Luiselli and Bruce presented their education research framework, rooted in previous work on education with the deafblind (Grisham-Brown et al., 2018), to take task analysis to the next level. They focused on examples such as active listening, eye contact during zoom, or informing people in real time about ongoing activities such as typing in the chat option, to increase engagement. Again, privacy concerns were at the forefront of the discussion, in addition to concerns about Zoom overload, stress and fatigue. The presenters provided strategies to create as well as break up routines, facilitate family engagement during on-line learning and creating structure for optimal home schooling. They proposed that their framework has the potential of becoming an eventual research tool. The sessions with a research focus also included representation of graduate students completing their work even in the face of necessary adaptations due to the pandemic. Weber and Choudhary discussed how they discovered that research on deafblindness requires flexibility and creativity as the ongoing pandemic demands. Weber carried out online expert hearings about good practices in hearing assessment of people with congenital deafblindness. Choudhary took a proactive participatory action approach (including two young adults living with deafblindness as co-presenters) to explore his original topics of peer relations between people with deafblindness of different ages, and explored communication activities (e.g., through WhatsApp) in new ways. Finally, all researchers agreed that access to and availability of research funding remains a challenge, making the visibility and unique requirements of persons living with deafblindness and ongoing priority.
Discussion
The first Deafblind International webinar ‘Living with Deafblindness in a New Reality’ was able to fill an important gap by bringing together a variety of stakeholders in deafblindness across the globe. This event allowed us to move the process of knowledge translation forward during an unprecedented time of pandemic. In response to the concerns of family members and support professionals, one participant highlighted an important insight, whereby he pointed out that he is ‘OK with this, this is normal life for me’. Persons living with deafblindness are experienced with living in isolation, having reduced ability to venture out independently, and being limited by living within a rigid system of restrictions. Suddenly, here is an opportunity for the able-bodied community to learn from their experience, and adopt their coping strategies. It is a powerful message and a unique chance to gain an understanding about the reality of persons living with any form of disability.
There is no doubt that the situation for persons with deafblindness magnifies the challenges of COVID-19, specifically in the context of touch and tactile access. This problem forces us to view touch as a right versus touch as a topic that is regulated through safety policies that are currently enacted and that further isolate persons with deafblindness. It remains unclear to which level the dignity of risk (Nay, 2002; Wolpert, 1980) is a sufficient justification for a person with deafblindness to judge for themselves, to make choices and to experience the consequences, without causing risk to others. The challenge of developing policies and procedures that can maintain the rights of persons with deafblindness, and balance them with health and safety responsibilities is ongoing and will need to consider, fundamental needs, risks and benefits as the pandemic unfolds. All stakeholders in deafblindness need to continue their advocacy efforts to ensure full access for the community to information and service. The example of making intervenors in Ontario, Canada, now fully recognized essential workers is a positive milestone in this process. Information access through public media (e.g., daily briefings on TV) was initially not accessible to those living with visual impairments and relied heavily on graphics and visual presentation (Holloway et al., 2020). Sign language interpreters and captions were added later on in many countries and across multiple languages. Such advances will further ensure equity for people living with disabilities in the age of COVID-19 (Jumreornvong et al., 2020).
The webinar was held early on in the pandemic, with ‘only’ 9,455,953 infections on the last day of the webinar. This number had multiplied by almost a factor of 10 at the time this manuscript was submitted. Different countries found themselves at different stages of severity, and for most the second and third waves had not yet hit, leading to further lockdowns and safety measures later on. Being the first webinar of this kind organized by Deafblind International, and scheduled early on in the pandemic, several technological glitches and the absence of captions rendered parts of the event inaccessible to persons with sensory impairment. In addition, the nature of a webinar did not allow for direct tactile participation of persons living with deafblindness themselves. However, it was interesting to observe how around the globe the barriers, enablers and solutions for persons with deafblindness and their allies were remarkably similar. The event created a sense of group membership and peer support, brought the participants, researchers, the professionals as well as their service agencies closer together and generated a sense of hope and collaboration. Deafblind International aims to make this an annual event that improves and expands over time, much like other already existing on-line knowledge translation and peer-support tools for deafblindness (Gavouyère et al., 2019).
Footnotes
Acknowledgements
The authors would like to acknowledge the financial and in-kind support of Deafblind International, the Fonds de recherche du Quebec–Santé Vision Health Research Network and Tanne Schweizerische Stiftung für Taubblinde.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: W.W. serves as the editorial board member of this journal; he is supported by a Fonds de recherche du Quebec – Santé chercheur boursier junior 2 career award # 281454. The other authors declare no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received financial support from Deafblind International for the publication of this article.