
Abstract
Stereotyped and repetitive behaviours are characteristics of autism spectrum disorder (ASD) but also occur in individuals with combined intellectual and sensory disabilities. This article looked at the differences in type, frequency, and duration of stereotyped behaviours between individuals with and without ASD in this population. The study included 59 individuals with intellectual disabilities and sensory impairments. The presence of ASD was assessed using Observation of Autism in people with Sensory and Intellectual Disabilities (OASID). Separate from these assessments, video recordings were scored by observers naive to the ASD status of participants for stereotyped and repetitive behaviours. Stereotyped and repetitive behaviours were more prevalent in participants with ASD, though a large proportion of participants without ASD showed them too. Participants with ASD showed, on average, more frequent and in duration longer stereotyped and repetitive behaviours, especially self-injurious behaviours. No differences were found for vocal, motoric, and stereotyped behaviours with objects. The mean duration of each episode of stereotyped behaviour did not differ between groups. Cluster analysis revealed a distinct group of individuals without ASD who showed a high number of stereotyped behaviours.
Keywords
Introduction
Autism spectrum disorder (ASD) is characterized by two major components: (1) deficits in social communication and social interaction, and (2) restricted and repetitive behaviour patterns, interests, or activities (American Psychiatric Association, 2013). In people with a combination of sensory and intellectual disabilities, the same deficits and atypical behaviours are also present (de Vaan et al., 2013; Hobson, 2005; Hoevenaars-van den Boom et al., 2009). Both people with ASD and people who have a combination of sensory and intellectual disabilities show autistic features. The biggest overlap may be found in the domain of repetitive and stereotyped behaviours. This is not surprising, because stereotyped behaviours occur very frequently in individuals with both sensory and intellectual disabilities (Murdoch, 1997). The question presents itself whether the presence of repetitive and stereotyped behaviours is a differentiating characteristic, of ASD in people with a combination of intellectual and sensory disabilities. The current study will focus on this question by looking at the occurrence and severity of stereotyped and repetitive behaviours in people with a combination of sensory and intellectual disabilities with and without ASD.
The Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) describes four different expressions of stereotyped behaviour that are part of ASD, namely (1) stereotyped and repetitive movements, objects, or speech, (2) insistence on sameness and adherence to routines, (3) restricted and fixated interests, and (4) different reactivity to sensory input (American Psychiatric Association, 2013). Though these behaviours are described as being typical for ASD, they are also often seen in people with sensory or intellectual disabilities. As such, a relationship has been found between stereotyped behaviours and developmental level (Militerni et al., 2002). Research also showed that individuals with ASD and an intellectual disability perform more stereotyped behaviours than individuals with an intellectual disability without ASD (Bodfish et al., 2000; Goldman et al., 2009). Research by Richards et al. (2012) further suggested that for people with intellectual disabilities the prevalence of self-injurious behaviours is high when someone has ASD as well and the amount of stereotyped behaviours is correlated with ASD severity (Militerni et al., 2002).
Though there seems to be a relationship between ASD and stereotyped and repetitive behaviours, the underlying cause of the behaviours may be different, depending on a person’s impairments. Andrews and Wyver (2005) suggest that the stereotyped behaviours found in people with sensory impairments may be due to completely different causes and serve different functions than the ones found in people with ASD, even though the behaviours may express themselves in an identical way. Turner (1999) suggests that some specific behaviours may be due to ASD while others are caused by something else. Certain behaviours may indeed be specifically correlated to a person’s visual impairment, such as eye poking or eye pressing which occurs frequently in blind children (Tröster et al., 1991). Another option is that intellectual disabilities, sensory impairments, and stereotyped behaviours are due to the same cause. Mukaddes and colleagues (2007) found that persons with blindness and ASD often have greater neurological impairments, such as lower intellectual levels or cerebral palsy. They suggest the possibility that the neurological damage that is responsible for the visual impairment or intellectual disability is also the cause of ASD typical behaviours such as repetitive and stereotyped behaviours.
Regardless of the cause of stereotyped and repetitive behaviours, earlier research findings indicated that stereotyped and repetitive behaviours are indeed frequently seen in people with sensory and/or intellectual disabilities, but also in people with ASD. The prevalence, frequency, and severity of stereotyped and repetitive behaviours are known to be a differentiating factor between people with and without ASD (Lord, 1995; MacDonald et al., 2007; Szatmari et al., 1989; Turner, 1999; Watt et al., 2008). At the same time, people with both sensory and intellectual disabilities show a high prevalence of stereotyped and repetitive behaviours, caused by their sensory disabilities and not necessarily by ASD (Gal et al., 2010; Poppes et al., 2010; Tröster et al., 1991). This raises the question whether stereotyped and repetitive behaviours are characteristic factors for ASD and can serve as differentiating behaviours or clinical markers for the assessment of ASD in people with a combination of intellectual and sensory disabilities. In fact earlier studies have indicated that in people with both sensory and intellectual disabilities the persons with ASD versus the ones without ASD show more impairments in the social domain and less in the domain of stereotyped and repetitive behaviours (de Vaan, Vervloed, Peters-Scheffer, et al., 2016; Hoevenaars-van den Boom et al., 2009). This could mean that stereotyped and repetitive behaviours are of no or limited use in diagnosing ASD in people with both sensory and intellectual disabilities.
The present study takes a closer look at stereotyped and repetitive behaviours in people with a combination of sensory and intellectual disabilities with and without ASD. What types of stereotyped behaviours are seen and how do they differ between people with and without ASD? First, a possible underlying structure of stereotyped and repetitive behaviours is examined. Second, differences between people with and without ASD within this target population are assessed. The focus will be on the type, duration, and frequency of stereotyped behaviours. Finally, we will cluster participants with comparable stereotyped and repetitive behaviours to see if behavioural profiles can be made regardless of the combination of disabilities.
Method
Participants
Participants were recruited from four residential institutions and three schools for people with multiple disabilities. Information about disabilities and impairments was obtained from personal files kept at their school or institution and were determined by licenced psychologists, psychiatrists, physicians, ophthalmologists, and audiologists in the past independently of this study. A contact person from each institution recruited potential participants and asked legal representatives for written consent. For privacy reasons, the authors did not receive information about clients that did not want to participate, so the non-response rate is unknown.
Participants were 59 individuals (41 male, 18 female) with a mean age of 31.32 years (SD = 14.92, range = 6–55 years). All participants had a moderate to profound intellectual disability and a visual impairment, ranging from moderate visual impairment to blindness without light perception. A total of 16 individuals had an additional auditory impairment and were thus deafblind (following the definitions of Ask Larsen & Damen, 2014; Dammeyer, 2012). The presence of ASD was assessed using Observation of Autism in people with Sensory and Intellectual Disabilities (OASID; see de Vaan, Vervloed, Peters-Scheffer, et al., 2016). OASID scores normally lead to an interpretation of No ASD, Mild ASD, Severe ASD, or Profound ASD symptoms (De Vaan et al., 2018), but for the purpose of this study two groups were created: No ASD (n = 27) and ASD (n = 32). The latter group consisted of people with Mild, Severe, and Profound ASD symptoms. See Table 1 for an overview of participant characteristics in both groups. An independent samples t test showed that age did not differ between groups. Chi-square tests showed that the distribution of levels of visual and auditory impairment were equal between groups. Only the distribution of level of intellectual disability was not the same between groups, χ2(2, n = 59) = 20.48, p < .001. The level of intellectual disability was more severe in people with ASD. This is not uncommon, because level of intellectual disability and autism were frequently found to be related (e.g., Matson & Shoemaker, 2009; O’Brien & Pearson, 2004).
Participant Characteristics.
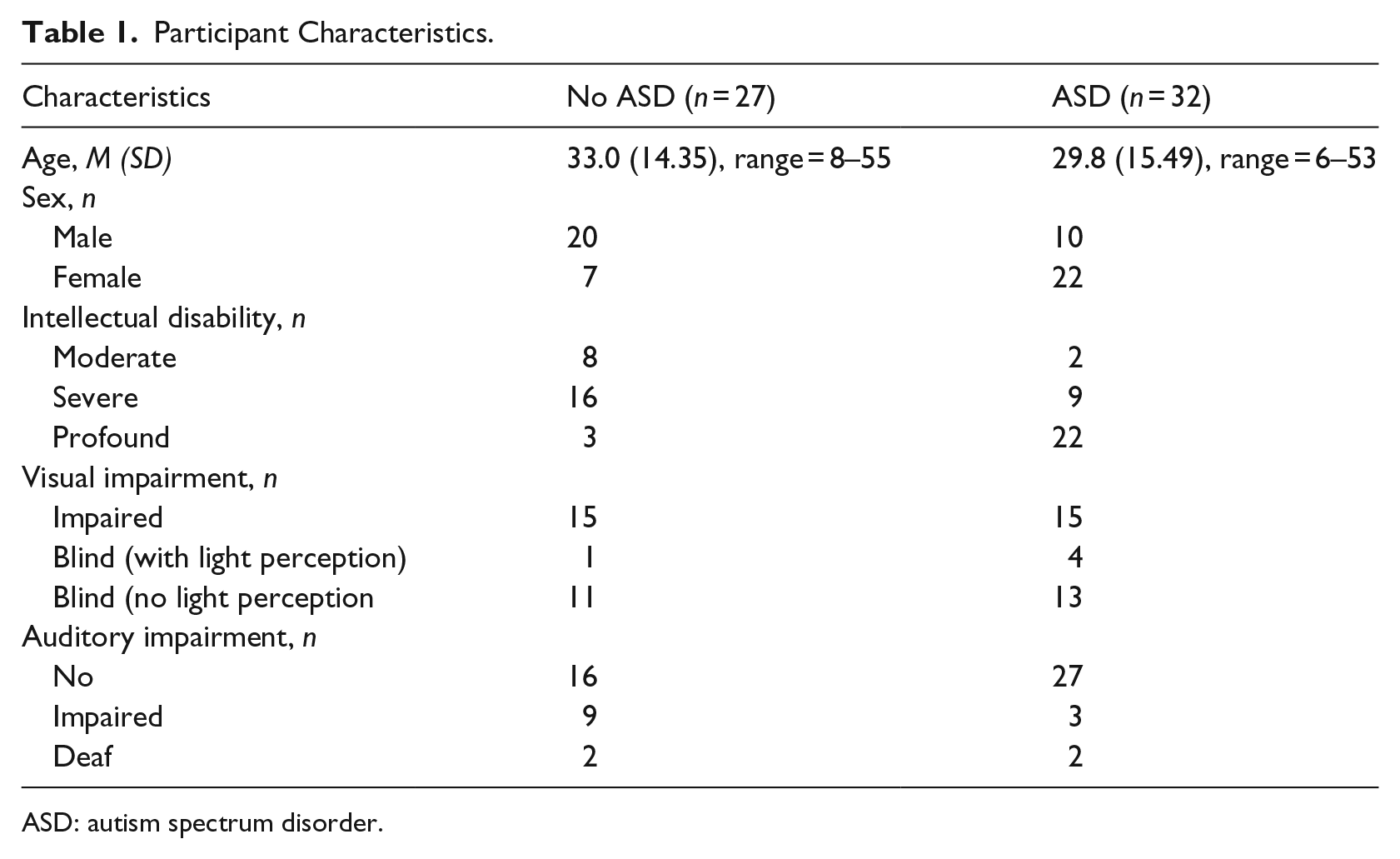
ASD: autism spectrum disorder.
Materials
OASID
OASID is a semi-structured observational assessment tool, designed to diagnose ASD in people with intellectual disabilities combined with sensory impairments (de Vaan, Vervloed, Peters-Scheffer, et al., 2016). The first author and two experimenters, trained in the assessment of OASID by the first author, played five tasks with the participants in order to trigger ASD typical behaviour, using toys and interaction games adjusted to the participants’ abilities. This play session lasted between 20 and 55 min and was recorded on video. The video of each session was observed afterwards and scored for autistic behaviours using 40 items scored on a three-point Likert scale. A total score was calculated for two scales, namely ‘Social Interaction and Communication’ and ‘Stereotyped and Repetitive Behaviours’. Both scales conform to the DSM-5 criteria for ASD. The combination of the two scales leads to a final score indicating ASD severity: no ASD, mild ASD, severe ASD, or profound ASD. OASID was found to be both a valid and reliable measure of ASD in people with sensory and intellectual disabilities (de Vaan et al., 2018; de Vaan, Vervloed, Peters-Scheffer, et al., 2016).
Observation
In order to assess the presence, frequency, and duration of stereotyped behaviour, four behavioural categories were created based on the literature: motor, self-injurious, and vocal stereotyped behaviour and repetitive behaviours with objects (eg. Moore & Magyar, 2012; Singer, 2009; Weiss, 2002). Each category comprised one or more stereotyped or repetitive behaviours (see Table 2). Behaviours within each category were mutually exclusive, but behaviours from different categories could overlap.
Observed behaviours and definitions.
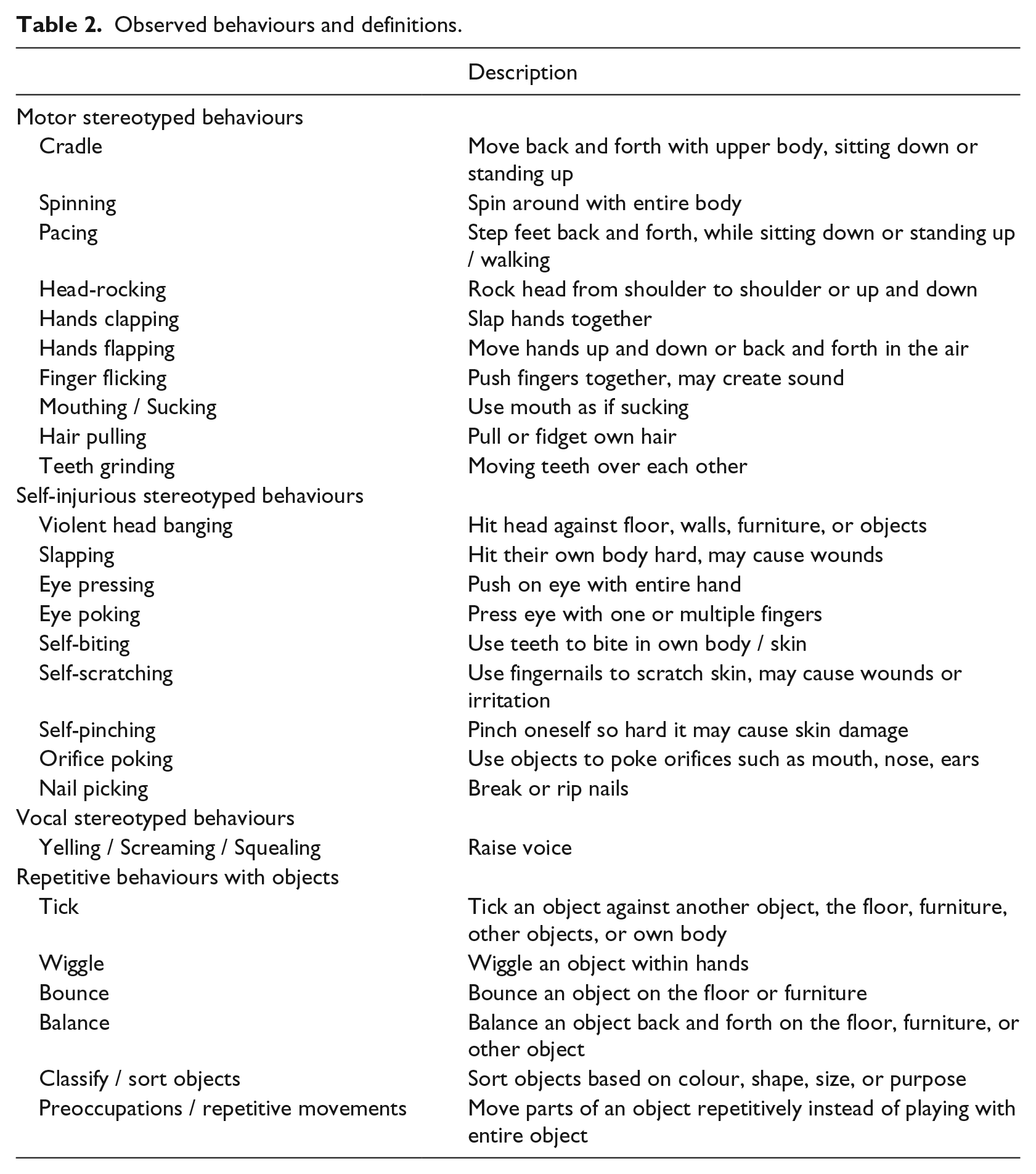
For this study, we observed a 10-min session from the OASID assessment. As described above and more elaborately in de Vaan, Vervloed, Peters-Scheffer et al. (2016), this assessment consisted of a play session that was similar for each participant. Examples of tasks that were played are physical interaction games with song and movements and solving a puzzle. Because the assessment was unfamiliar to the participants the first 10 min served as a warming up for the participant to get acquainted with the situation and experimenter. Stereotyped behaviours during these first 10 min were therefore disregarded. Observations were performed with The Observer XT software (Noldus, 2015). The Observer software allows for the design of a coding scheme and to code behaviour accordingly. While watching the video a rater coded on- and offset times of behaviours. The time in between start and stop defined an episode of stereotyped behaviour. This provided information about which behaviours occurred, how many episodes there were (frequencies), and how long each episode lasted (duration). The coding scheme is shown in Table 2. When a behaviour appeared to be starting but ended within less than three bouts, the raters were instructed not to take this behaviour into account as repetitive attempts were not scored.
A 10-min fragment of the OASID assessment was analysed, starting after 10 min in the assessment and ending at the end of the 20th min. Videos were scored independently by two student assistants, who had previously received training by the first author in the use of the Observer XT and the coding scheme. Both raters completed all video fragments. The Observer XT interrater reliability analysis revealed an overall Kappa of 0.98, indicating excellent inter-rater reliability.
Procedure
This study was approved by the local Committee on Research Involving Human Subjects and conformed to the Ethical Principles for Medical Research Involving Human Subjects of the World Medical Association Declaration of Helsinki (World Medical Association, 2013). Parents or legal representatives gave informed consent prior to participation. First, the OASID assessment was performed, which lasted between 20 and 55 min. This session was recorded on video and scored afterwards for the whole session by means of the OASID questionnaire. After the assessment, four behavioural categories were created to assess the presence of stereotyped and repetitive behaviour. These categories and corresponding behaviours were the result of a literature study on stereotyped and repetitive behaviours . Second, a 10-min fragment of each OASID video recording was selected. For each participant, the 11th until the 20th min were analysed with the Observer XT software. Since categories could overlap each video had to be scored in four separate runs, one run for each behavioural category, in order to guarantee observation accuracy. Both OASID and the 10-min fragments were scored for stereotyped behaviour using observations. However, the OASID assessment only included questions about the mere presence of stereotyped behaviour, whereas the observations with The Observer XT zoomed in on the types, frequency, and duration of these behaviours.
Statistical analyses
First, a principal component analysis using oblique rotation was performed to check if our a priori categories of stereotyped behaviour could be confirmed based on our data. Second, groups (ASD vs. no ASD) were compared. To compare proportions, we used chi-square tests, and to compare differences in duration, frequency, and duration per episode, we used non-parametric Mann–Whitney U tests, because assumptions regarding normality and equal variance were violated. Corresponding effect size r was calculated using the formula of Pallant (2010).
We made comparisons between groups on the types and total number of stereotyped behaviour, and compared duration, frequency, and duration per episode. Duration was defined as the total duration in seconds that participants engaged in stereotyped behaviour. Frequency was the number of separate episodes of stereotyped behaviour that were observed. Duration per episode was the average duration of each episode of stereotyped behaviour, calculated by dividing duration by frequency. In case of planned multiple comparisons, a more conservative statistical significance level of .01 was used, to avoid capitalization on chance and control for familywise error rate. Finally, clusters of participants were made using the durations of the different stereotyped behaviour categories. This was done using a hierarchical cluster analysis according to the procedure described by Yim and Ramdeen (2015).
Results
Principal component analysis on categories of stereotyped behaviour
Prior to this study, we created four categories of stereotyped and repetitive behaviour based on the literature (see Table 2). An exploratory principal component analysis was performed. This was done to see if our data led to the same categories that were created a priori. The variables that we inserted were the total duration of each separate behaviour. For six of these 26 variables there was no variance, so these were excluded from this analysis. These variables were spinning, mouthing/sucking, teeth grinding, violent head banging, nail picking, and classify/sort objects. The principal component analyses were performed on the remaining 20 variables. We chose to use eigenvalues of 1.0 as a cutoff for number of factors. Ten factors were extracted accordingly, explaining 78.6% of the total variance. This is a large number of factors considering the number of variables (an average of two variables per category) and does not comply with the categories that were found in the literature. The results showed that based on the data, stereotyped and repetitive behaviours could not be reduced to clear latent structures. This is why we will perform our calculations on individual variables and the a priori categories.
Proportion of people with stereotyped behaviour
The first column for each group in Table 3 shows the number and percentage of people in this group that showed each type of stereotyped behaviour. Within the ASD group, 100% of the participants showed stereotyped behaviour as opposed to 85.2% of people without ASD, a significantly higher proportion, χ2(1, n = 59) = 5.07, p = .024.
Prevalence, duration, and frequency of stereotyped behaviours.
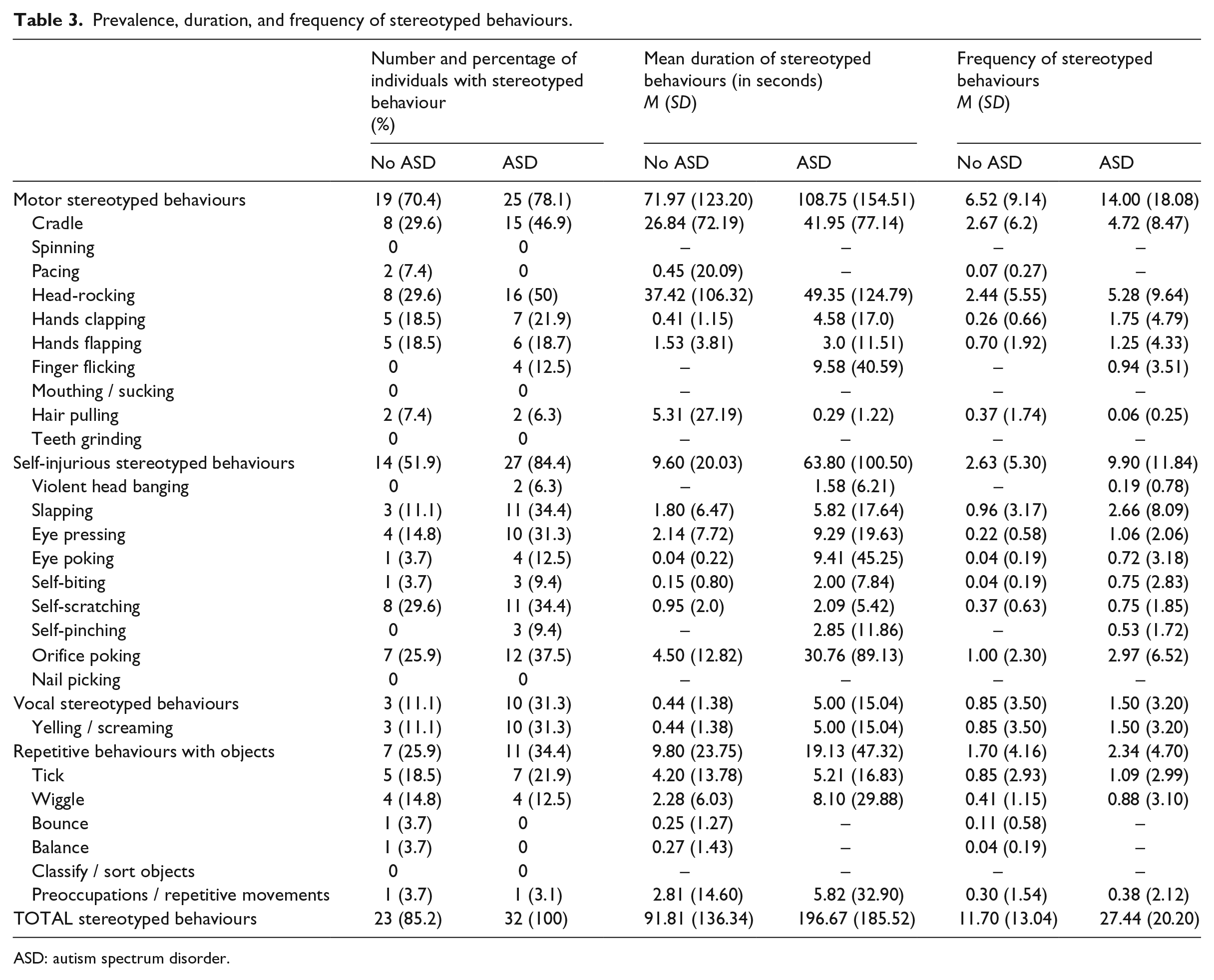
ASD: autism spectrum disorder.
For the different categories of stereotyped behaviours, differences in proportions of people were found for injurious stereotyped behaviour, χ2(1, n = 59) = 7.31, p = .007, where 84.4% of participants with ASD showed self-injurious behaviour, versus 51.9% of participants without ASD. For the other categories no significant differences in proportions were found.
Types of stereotyped behaviour
As can be seen in Table 3, some types of stereotyped and repetitive behaviour did not occur at all in our sample, including spinning, mouthing/sucking, teeth grinding, nail picking, and sorting or classifying objects. Furthermore, pacing and bouncing and balancing of objects only occurred in the no ASD group, whereas finger flicking and violent head banging was only observed in people with ASD.
In addition, persons with ASD showed significantly more types of stereotyped behaviour than persons without ASD, respectively, 4.00 (SD = 2.08, Mdn = 3.5) types of stereotyped behaviour versus 2.56 (SD = 2.23, Mdn = 2.0) types, U = 250.000, p = .006, r = .36.
Differences in duration of stereotyped behaviour
Differences in duration of stereotyped behaviour (see Table 3) between people with and without ASD were tested with Mann–Whitney U tests. Differences were found for the total duration of stereotyped behaviour, U = 232.000, p = .002, r = .40, (ASD Mdn = 120.13, No ASD Mdn = 29.66) and for the duration of the category injurious stereotyped behaviours. U = 225.500, p = .001, r = .41 (ASD Mdn = 23.57, No ASD Mdn = 1.67). In general, people with ASD showed longer mean durations of stereotyped behaviour than people without ASD. Differences in duration were not found for the categories motor and vocal stereotyped behaviours or repetitive behaviours with objects, and any of the discrete stereotyped behaviours.
As can be seen in Table 3, a large proportion of participants did not show certain types of stereotyped behaviour at all. This affected the group mean, and possibly caused differences as the proportion of people without stereotyped behaviour is larger in the no ASD group. The analyses were repeated with participants with no stereotyped behaviour treated as missing, so only participants with stereotyped behaviours were taken into account. Mann–Whitney U tests revealed no differences on any of the categories of stereotyped behaviour between people with and without ASD, only the total score differed significantly between ASD (M = 196.68, SD = 185.52, Mdn = 120.13) and no ASD (M = 107.77, SD = 142.0, Mdn = 37.07), U = 232.000, p = .02, r = .31. There is no longer a difference for self-injurious behaviours. On the discrete stereotyped behaviours, no significant differences were found.
Differences in frequency and duration per episode of stereotyped behaviour
Differences between groups in frequency (see Table 3) of stereotyped behaviour episodes were assessed with Mann–Whitney U tests. This revealed differences between the ASD and no ASD groups for the total frequency of stereotyped behaviour. The ASD group showed a higher frequency (Mdn = 21.5) than the no ASD group (Mdn = 6.0), U = 198.500, p < .001, r = .46. Also on self-injurious stereotyped behaviour, people with ASD (Mdn = 6.00) showed a higher frequency of stereotyped behaviour than people without ASD (Mdn = 1.00), U = 203.000, p = .001, r = .45.
The total duration of stereotyped behaviour was divided by the frequency of stereotyped behaviour, finding the mean duration of each episode. Mann–Whitney U tests revealed no differences between people with and without ASD for episode length.
Clustering participants by stereotyped behaviour patterns
An hierarchical cluster analysis was performed to search for clusters of participants among the categories of stereotyped behaviour (Yim & Ramdeen, 2015). The duration of motor stereotyped behaviour, self-injurious stereotyped behaviour, vocal stereotyped behaviour, and repetitive behaviour with objects were used as cluster variables. The agglomeration schedule and dendogram revealed three clusters of participants on these variables. See Table 4 for a comparison between clusters on these variables, as well as on total duration of stereotyped behaviour, age, and OASID score.
Mean values on stereotyped behaviour, age, and OASID scores for each cluster.
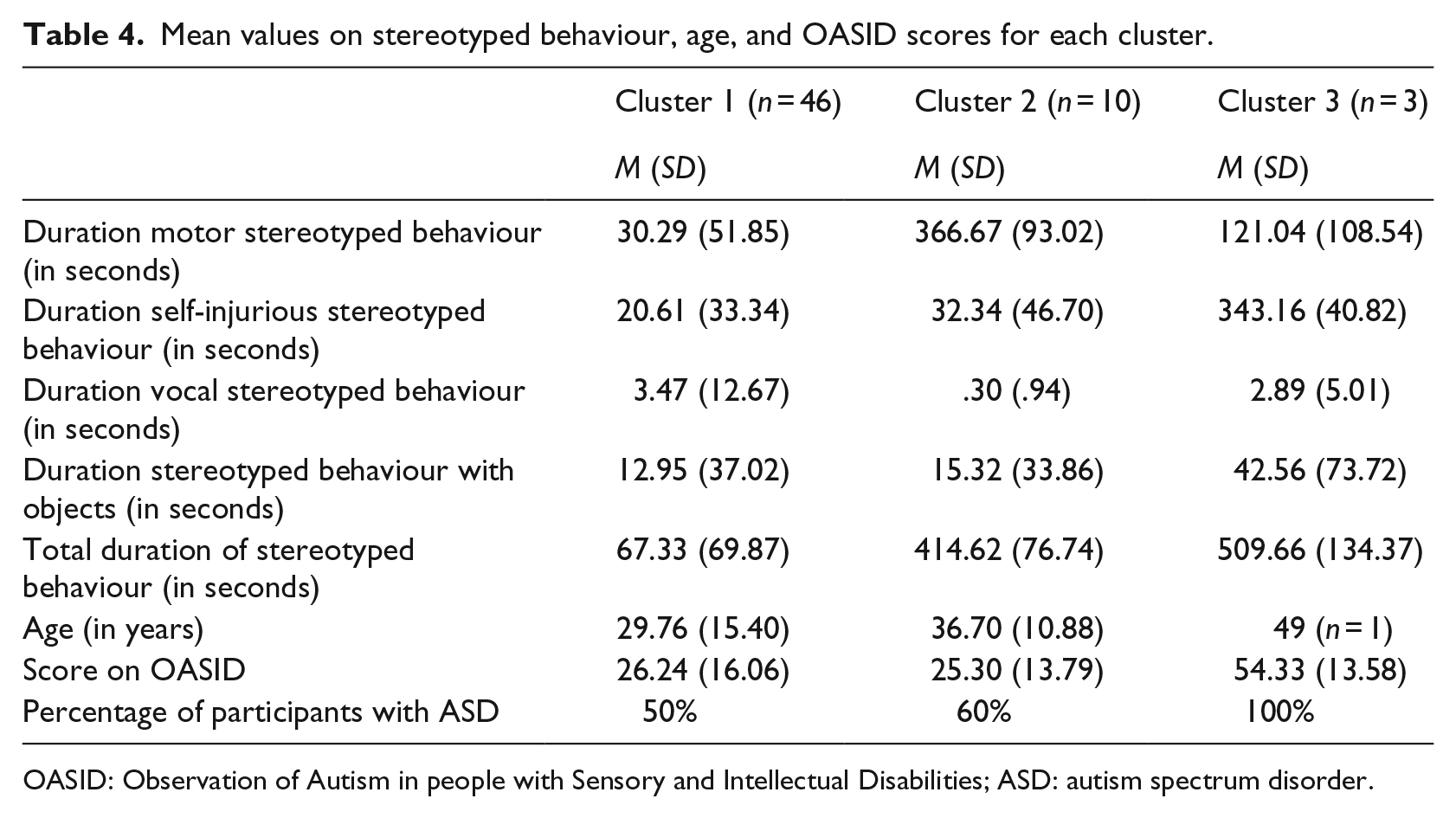
OASID: Observation of Autism in people with Sensory and Intellectual Disabilities; ASD: autism spectrum disorder.
As can be seen in Table 4, Cluster 1 consists of people with a relatively low total duration of stereotyped behaviour, reflected in all categories of stereotyped behaviour. Cluster 2 consists of people with a relatively high score on stereotyped behaviour, mostly in the category of motor stereotyped behaviours. Cluster three is a small cluster consisting of people with a high duration of stereotyped behaviour, especially seen in self-injurious stereotyped behaviour.
First we analysed differences on the variables used for clustering. Significant differences between clusters were found for motor stereotyped behaviour, where Cluster 2 (Mdn = 333.67) scored higher than Cluster 1 (Mdn = 6.37; U = 0, p < .001, r = .66) and Cluster 3 (Mdn = 125.92; U = 0, p = .01, r = .70). On self-injurious stereotyped behaviour, Cluster 3 (Mdn = 343.05) scored higher than Cluster 1 (Mdn = 4.29; U = 0, p = .004, r = .41) and Cluster 2 (Mdn = 2.19; U = 0, p = .01, r = .71). The other variables used for clustering did not differ significantly between groups.
Then we analysed differences on the total duration of stereotyped behaviour. This was shorter in Cluster 1 (Mdn = 36.74) than in Cluster 2 (Mdn = 434.31; U = 0, p < .001, r = .66) and Cluster 3 (Mdn = 477.64; U = 0, p = .004, r = .41). On OASID scores, persons in Cluster 3 (Mdn = 47.00) scored higher than people in both Cluster 1 (Mdn = 23.00; U = 12.0, p = .03, r = .34) and Cluster 2 (Mdn = 24.50; U = 2.0, p = .02, r = .61), indicating more autistic symptoms in Cluster 3. Based on OASID results, Cluster 3 consisted of people with ASD only, when only about half of participants have ASD in Clusters 1 and 2. No differences between clusters were found for duration of vocal stereotyped behaviour and stereotyped behaviour with objects, for age, visual impairment, auditory impairment, or level of intellectual disability.
Discussion
The current study focused on stereotyped and repetitive behaviours in individuals with both an intellectual disability in addition to sensory impairments with or without ASD. Besides measuring the mere presence and type of stereotyped behaviour, this study zoomed in on the intensity of stereotyped behaviour, measured by its frequency and duration. People with sensory and intellectual disabilities show many topographical overlaps in behaviour with people with ASD (de Vaan et al., 2013). Though for other populations stereotyped and repetitive behaviours are differentiating factors for the presence of ASD, it might be not for people with sensory and intellectual disabilities who seem to show stereotyped behaviour regardless of the presence of ASD (Poppes et al., 2010; Tröster et al., 1991). This study focused on the question whether stereotyped and repetitive behaviours are indeed characteristics of ASD and are differentiating factors for ASD and no ASD in people who have sensory and intellectual disabilities.
First, we made categories of stereotyped behaviour based on the literature. Four categories were created, namely motor stereotyped behaviour, self-injurious stereotyped behaviours, vocal stereotyped behaviour, and stereotyped behaviour with objects. A principle component analysis did not find the four a priori categories as the best factor solution but a solution with 10 factors. The analyses did not reveal clear latent structures in the stereotyped and repetitive behaviours. However, in our short session, we found an average of only two to four stereotyped behaviours per individual. This means that the remaining behaviours were not seen on an individual level. Possibly, the frequency of stereotyped behaviours and sample size was too low to find any underlying structure.
Second, we analysed the prevalence of stereotyped behaviour in our groups of ASD and no ASD and the average number of different stereotyped behaviours each person showed. The groups were created based on a relatively new assessment instrument, OASID (de Vaan et al., 2018; de Vaan, Vervloed, Peters-Scheffer, et al., 2016). This is a new test instrument and has not been studied extensively, so it is possible that some of our participants were unjustly classified as having ASD or no ASD. However, the personal files of our participants did not always provide sufficient information to classify participants as having ASD or not, and other existing instruments have proven to be inappropriate for diagnosing ASD in this population (see de Vaan, Vervloed, Hoevenaars-van den Boom, et al., 2016, for a review). Creating groups using OASID therefore appeared to be the best choice for our study.
In the ASD group, all participants showed stereotyped behaviours and in the no ASD group 85% of the participants showed stereotyped behaviours as well. Though still a very large proportion, it was significantly less than in the ASD group. This is in line with earlier findings from a study by Bodfish et al. (2000) who compared individuals with and without ASD with intellectual disabilities. Although stereotyped behaviour was present in both groups, it was more frequent in participants with ASD than in participants without ASD (Bodfish, et al., 2000). On a categorical level, there was only a significant difference for self-injurious stereotyped behaviour, which is in line with Richards et al. (2012) who showed that self-injurious behaviour is more frequent among people with ASD and intellectual disability than in people with ASD alone. In addition, we found that people with ASD showed a larger number of different types of stereotyped behaviour than people without ASD. This is in line with earlier research that showed that in persons with intellectual disabilities, persons with ASD showed more stereotyped behaviours than without ASD (Bodfish, et al., 2000; Richards, et al., 2012; Rojahn et al., 2010). Specifically, we found that violent head banging and finger flicking occurred exclusively in people with ASD, whereas pacing and bouncing and balancing of objects was only observed in people without ASD. Some other behaviours that we selected were not seen at all in our observations. This could be due to the limited observation time or because some higher order behaviours, such as classifying objects, are only seen in individuals with higher developmental levels (Militerni et al., 2002). Other behaviours, such as nail picking and finger flicking, might not have been seen because they require fine motor skills that are often not well developed in people with multiple disabilities (Tröster et al., 1991).
Earlier studies indicated that the intensity of stereotyped behaviour is more severe in people with ASD as opposed to people without ASD (Turner, 1999; Watt et al., 2008). We tested if this was also the case in people with sensory and intellectual disabilities, by looking at duration, frequency, and mean duration per episode. We found that the duration and frequency of stereotyped behaviours was indeed higher for people with ASD; this was found for total duration and self-injurious stereotyped behaviours. However, this difference could have been biased by the lower proportion of people who showed stereotyped behaviours in the no ASD group. It was therefore important first to see if the results could be replicated if only participants that showed stereotyped behaviours were analysed. Second, we had to take a closer look at the duration of each episode. Our results revealed that when people without stereotyped behaviours were excluded from the analyses, people with ASD only scored higher than people without ASD on total duration and not on self-injurious stereotyped behaviours anymore. In fact, no differences between ASD and no ASD were found for the duration of each stereotyped behaviour episode. Based on our data, no conclusions about the presence of ASD can be drawn from the length of an episode.
On average, people with ASD showed more types of stereotyped behaviours, they had a higher frequency of stereotyped behaviours, and on average they showed stereotyped behaviour of longer durations. However, even in participants without ASD, stereotyped behaviours were observed frequently. So, though a high frequency and long duration of stereotyped behaviour can be alarming, especially when it is self-injurious, it does not necessarily indicate the presence of ASD.
Our findings raised the question which factors were involved in the occurrence of stereotyped and repetitive behaviours in people with sensory and intellectual disabilities. To answer this final question, a cluster analysis was performed to search for clusters among participants who showed similar patterns of stereotyped behaviour. Our analysis revealed three clusters, consisting of one cluster with people showing stereotyped behaviour of limited duration, and two clusters with people showing long lasting stereotyped behaviours. Participants in Cluster 3 clearly had higher ASD scores and also more self-injurious stereotyped behaviours than persons in the other two clusters. The persons in Cluster 2 showed many stereotyped behaviours but they scored the same amount of other ASD characteristics as the persons in Cluster 1 who showed limited numbers of stereotyped behaviour. Apparently in people with both sensory and intellectual disabilities, there is a distinct group of people without ASD who show high amounts of stereotyped behaviours, especially in the category of motor stereotyped behaviours. Our further analyses revealed that these clusters did not differ for different levels of intellectual disability, visual impairment, auditory impairment, or age. As a result, these variables cannot explain the number of stereotyped behaviours. Other factors than ASD or sensory and intellectual disabilities must be related to the occurrence of stereotyped behaviours, such as level of communication, amount of social reinforcement (Janssen et al., 2002), level of stimulation that proceeds the behaviour (Hall et al., 2003), or stress and anxiety (Leekam et al., 2011; Rodgers et al., 2012).
The study has several limitations that have to be taken into account. A first limitation of this study is that for the principal component analysis the sample size might be too small. A larger number of participants than in this study is normally recommended (Pallant, 2010). The small number of participants could have played a part in not finding clear latent structures among our variables. A second limitation is that OASID assessments were used in both the observations of stereotyped behaviour and in assessing the presence of ASD. This could have resulted in overlap between both measures, because stereotyped behaviour is also one of the criteria for ASD (American Psychiatric Association, 2013) that was also observed in the OASID assessment (de Vaan, Vervloed, Peters-Scheffer, et al., 2016). However, OASID only observed whether stereotyped behaviour was present, whereas in the current observations, we zoomed in on the types, duration, frequency, and duration per episode. Finally, only a brief period of time was selected from each participant video to observe stereotyped and repetitive behaviour. This was done to guarantee that for each participant a similar session over the same period of time was observed. However, the specific activities that occurred during this session varied between participants, so it is possible that some activities, transitions, or periods of downtime could have affected the prevalence of stereotyped behaviour. A longer period of time for each participant would have provided us with more information about stereotyped behaviour. For future studies, it is therefore recommended to observe longer periods of time so that not only the prevalence and duration of stereotyped behaviour can be observed but possible causes can also be assessed.
The current study showed that, on average, in people with both sensory and intellectual disabilities, the persons with ASD show more stereotyped behaviours than persons without ASD, especially self-injurious stereotyped behaviours. However, as this behaviour also occurs in people without ASD and the duration of each episode does not differ between people with and without ASD, the mere occurrence of stereotyped behaviour cannot be used as a differentiating factor for ASD. In fact, there was a distinct group within our population that do show stereotyped behaviours, but have a low number of autistic symptoms. Hence, the assumed over-diagnosis of ASD in people with sensory and intellectual disabilities can be understood (Andrews & Wyver, 2005; Hoevenaars-van den Boom et al., 2009). Future research should look at factors that cause stereotyped behaviour in people with sensory and intellectual disabilities, so that over-diagnosis of ASD is prevented and treatment can be aimed at reducing stereotyped behaviours, especially the types that harm the individual.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by ZonMW (grant number 60-00635-98-0081), Royal Dutch Kentalis and the Behavioural Science Institute of Radboud University.
Compliance with ethical standards
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This study was approved by the local Committee on Research Involving Human Subjects, CCMO region Arnhem-Nijmegen.