
Abstract
Background
Food insecurity is associated with an increased risk of hypertension.
Aim
The aim of this study was to evaluate the role of dietary sodium and potassium intake in the setting of food insecurity on hypertension risk.
Methods
We performed a cross-sectional analysis of data from 17,015 adults aged 18–65 years who participated in the National Health and Nutrition Examination Survey (2011–2018). We examined the associations between food insecurity, hypertension, and dietary sodium and potassium levels using multivariable logistic regression. Mediation analysis was conducted to explore the potential influence of dietary sodium and potassium intake on the relationship between food insecurity influenced hypertension.
Results
Individuals experiencing food insecurity had a significantly lower mean potassium intake (2.5 ± 0.03 g) compared to food-secure counterparts (2.74 ± 0.02 g). Food insecurity status was significantly associated with an increased likelihood of a higher dietary sodium-to-potassium ratio, an established predictor for hypertension.
Conclusion
Adults with food insecurity and hypertension were more likely to have lower dietary potassium intake. Increasing access to healthy foods, particularly potassium-rich foods, for individuals facing food insecurity may contribute to reducing the hypertension prevalence and improving cardiovascular outcomes.
Introduction
Hypertension is a significant public health issue, affecting 116 million adults in the United States (CDC, 2023). Various social determinants of health associated with lower socioeconomic status, such as lower income level, educational attainment, employment status, and opportunities, and adverse environmental factors contribute to the risk of hypertension and cardiovascular disease (CVD) (Schultz et al., 2018). Individuals in low-income areas experience higher rates of hypertension, uncontrolled hypertension, and an elevated risk of fatal CVD complications (Shahu et al., 2019), highlighting the impact of social determinants of health on hypertension prevalence and outcomes.
Food insecurity, the inconsistent access to nutritious food for a healthy life, is one of many social determinants of health and is a growing public health concern (USDA ERS, 2025). It is linked to increased hypertension risk and adverse health outcomes (Banerjee et al., 2024; Nagata et al., 2019; Royer et al., 2025; Tian et al., 2025). US adults living below the federal poverty level exhibit a higher prevalence of food insecurity (Shahu et al., 2019). Alarmingly, 84% of households served by the food banks in the Feeding America network experienced food insecurity, with 58% of them having a family member with hypertension (Feeding America, 2014). Studies reveal that individuals with food insecurity are less likely to have their hypertension under control (Oladele et al., 2025; Palakshappa et al., 2021; Sacks et al., 2001; Shahu et al., 2019).
Several pathways link food insecurity to hypertension (Seligman et al., 2010), including stress response to poverty (Rasmusson et al., 2018), suboptimal dietary quality (Brown et al., 2019; Leung et al., 2014), and obesity (Li et al., 2020). Studies indicating an association between poor diet quality, chronic disease risk, and cardiovascular health in individuals with food insecurity suggest a potential connection (Micha et al., 2017; Nagata et al., 2019; Oladele et al., 2025; Rasmusson et al., 2018). Food-insecure households often face challenges in paying bills, making trade-offs between food and other financial obligations (Feeding America, 2014; Gundersen et al., 2017; NCHS, 2024). This situation often results in unhealthy eating patterns, characterized by inexpensive and highly processed foods that are high in sodium and nutritionally deficient (Brown et al., 2019; Gundersen et al., 2017; Leung et al., 2014). Excessive sodium intake is a well-established risk factor for hypertension, while potassium plays a crucial role in counterbalancing sodium's effects and promoting healthy blood pressure (Kim et al., 2024; Newberry et al., 2018). The combination of high sodium and low potassium intake, commonly observed in processed foods prevalent among food-insecure populations, creates an optimal environment for hypertension development. Despite the clear relationship between poor diets and hypertension, limited studies have explored the impact of food insecurity on hypertension.
This study aims to examine the relationship between food insecurity, hypertension, and dietary sodium and potassium intake in a nationally representative sample of adults. We hypothesize that individuals experiencing food insecurity and hypertension will exhibit higher dietary sodium and lower potassium intakes compared to those who are food secure and have normal blood pressure.
Methods
Study population
We conducted a cross-sectional secondary analysis using data from the National Health and Nutrition Examination Survey (NHANES) from 2011–2018. NHANES is a nationally representative survey assessing the nutrition and health condition of noninstitutionalized individuals through interviews and physical examinations, conducted by the National Center for Health Statistics (NCHS) (Whelton et al., 2018). We excluded pregnant women and participants with incomplete blood pressure and food security screening data. Ethical approval was exempted for this study because we used publicly available, de-identified data.
Blood pressure status: Blood pressure was classified into normal BP, elevated BP, and hypertension based on the 2017 American College of Cardiology (ACC)/American Heart Association (AHA) Task Force guidelines (USDA Survey Tool). Participants who reported use of antihypertensive medications were categorized as having hypertension.
Food security status: Food security was determined using the 18-item USDA's Food Security Module and categorized into one of four food security categories (i.e., high, marginal, low, and very low) based on NHANES documentation (NCHS 2015-2016, 2023).
Dietary recall data: Dietary intake of sodium and potassium was evaluated via two 24-hour dietary recall interviews. We calculated sodium-to potassium ratios (Na:K), which have been established to be a good predictor of hypertension risk. Detailed information on 24-hour dietary recall procedures can be found elsewhere (Bauman et al., 2006).
Demographics and social factors: Demographic information included age at the time of the interview, sex, and self-reported race/ethnicity. The income-to-poverty ratio variable was utilized to assess participants’ socioeconomic status adjusted for family size, as established by the US Census Bureau, and divided into four distinct categories: Family income ≤1.3 (poorest); between 1.3 and 1.85; >1.85 of the poverty threshold and N/A, missing or incomplete data.
Physical Activity: We estimated the weekly number of minutes spent performing moderate and vigorous physical activities. Using the Physical Activity questionnaire, participants were categorized into three groups (high or recommended, intermediate, and low physical activity) based on the CDC's recommended level of physical activity (Diaz et al., 2021).
Statistical analyses
Descriptive data were reported as proportions and 95% confidence intervals for categorical variables, and as mean (±standard error, SE) for continuous variables. Patient characteristics were compared among blood pressure status (normal, elevated, or hypertension) and food security status, considering sample weights, using the chi-squared test for the categorical variables, the t-test for two groups of continuous variables, and Wald's test for three or more groups of continuous variables. To address missing data and imbalances in the categories, high food security and marginal food security were merged as one category of food security; low and very low food security were merged to classify food insecurity. Age was categorized into 5-year intervals (Diaz et al., 2021).
Participants aged 18–29 years were grouped together, considering the lower prevalence of primary hypertension in individuals under 30.
Outcome measures included food security status and hypertension, with each serving as a predictor and outcome variable, depending on the analysis. Predictor variables included race/ethnicity, sex, food security status, body mass index (BMI), diabetes, kidney disease, sodium and potassium intake, Na:K ratio, age, physical activity, and family income. Separate logistic regression models for survey data were fitted to identify risk factors associated with hypertension or food insecurity. We performed mediation analysis to evaluate the direct and indirect effects of food insecurity on blood pressure mediated by dietary sodium and potassium intake and Na:K ratio. All analyses were conducted using R version 4.3.1 (R Core team, Vienna, Austria). All tests were two-sided, and a P-value <.05 was considered statistically significant.
We presented results as unweighted counts (actual numbers of participants sampled) and weighted estimates. The NCHS sample weights in NHANES account for the complex survey design (including oversampling), survey non-response, and post-stratification adjustment to match total population counts from the Census Bureau, ensuring representative estimates of the US civilian noninstitutionalized population (NCHS 2015-2016, 2023).
Results
Participant characteristics
During the study period, 39,156 individuals completed the NHANES surveys. The final dataset for our analysis included 17,015 adults aged 18–65 years (Figure 1). Of these, 15,633 participants completed the 24-hour dietary recall.
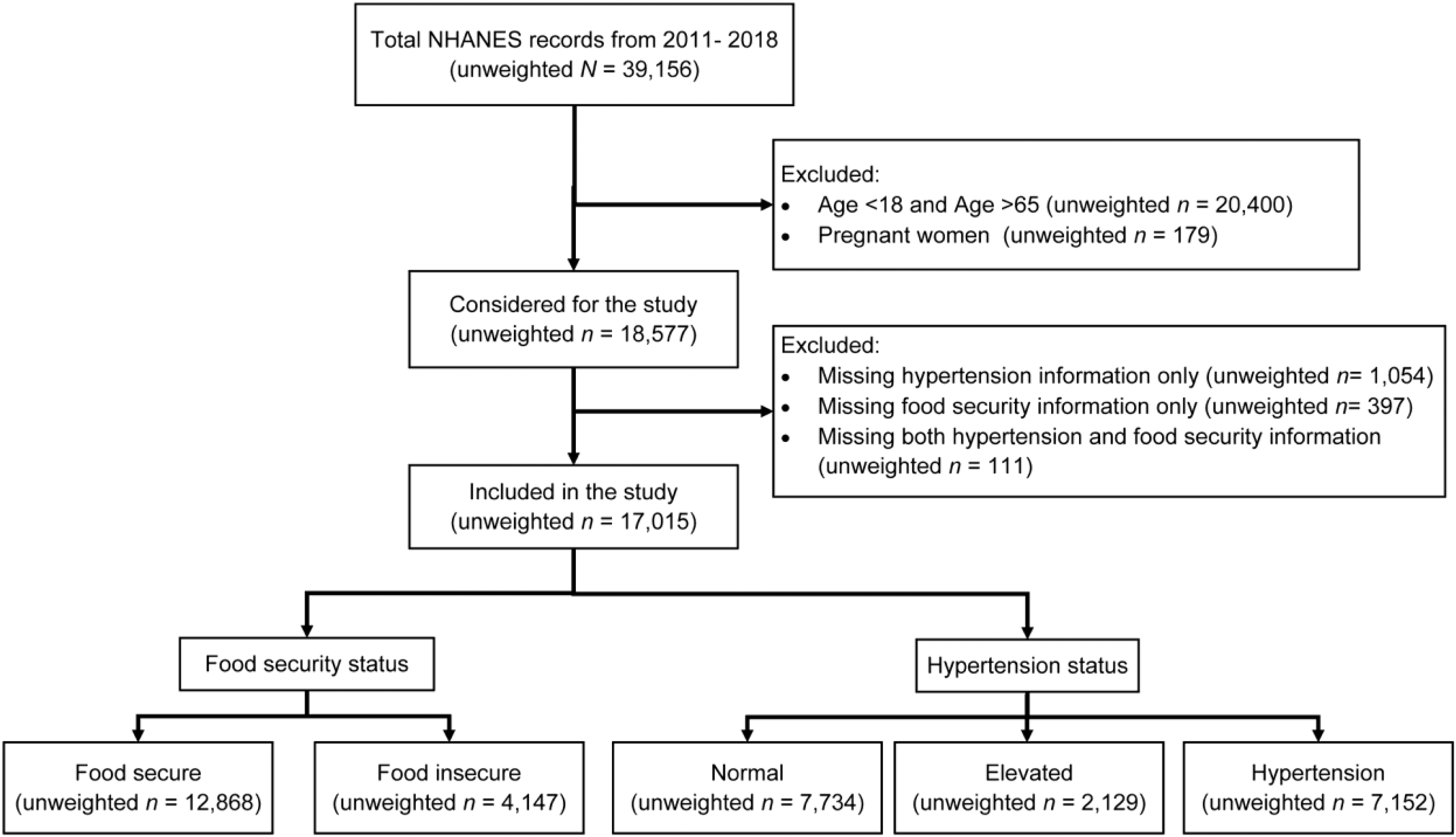
Participant selection.
Hypertension as an outcome
Weighted estimates revealed distinctive characteristics between participants with hypertension and those with normal blood pressure. The hypertension group was significantly older, more likely male, and obese and had a significantly higher dietary sodium intake compared to the normal blood pressure group (Table 1). The prevalence of hypertension in US adults across different time periods, and in age, sex, and race–ethnicity subgroups is presented in Table S1.
Characteristics by hypertension status for NHANES 2011–2018 participants.
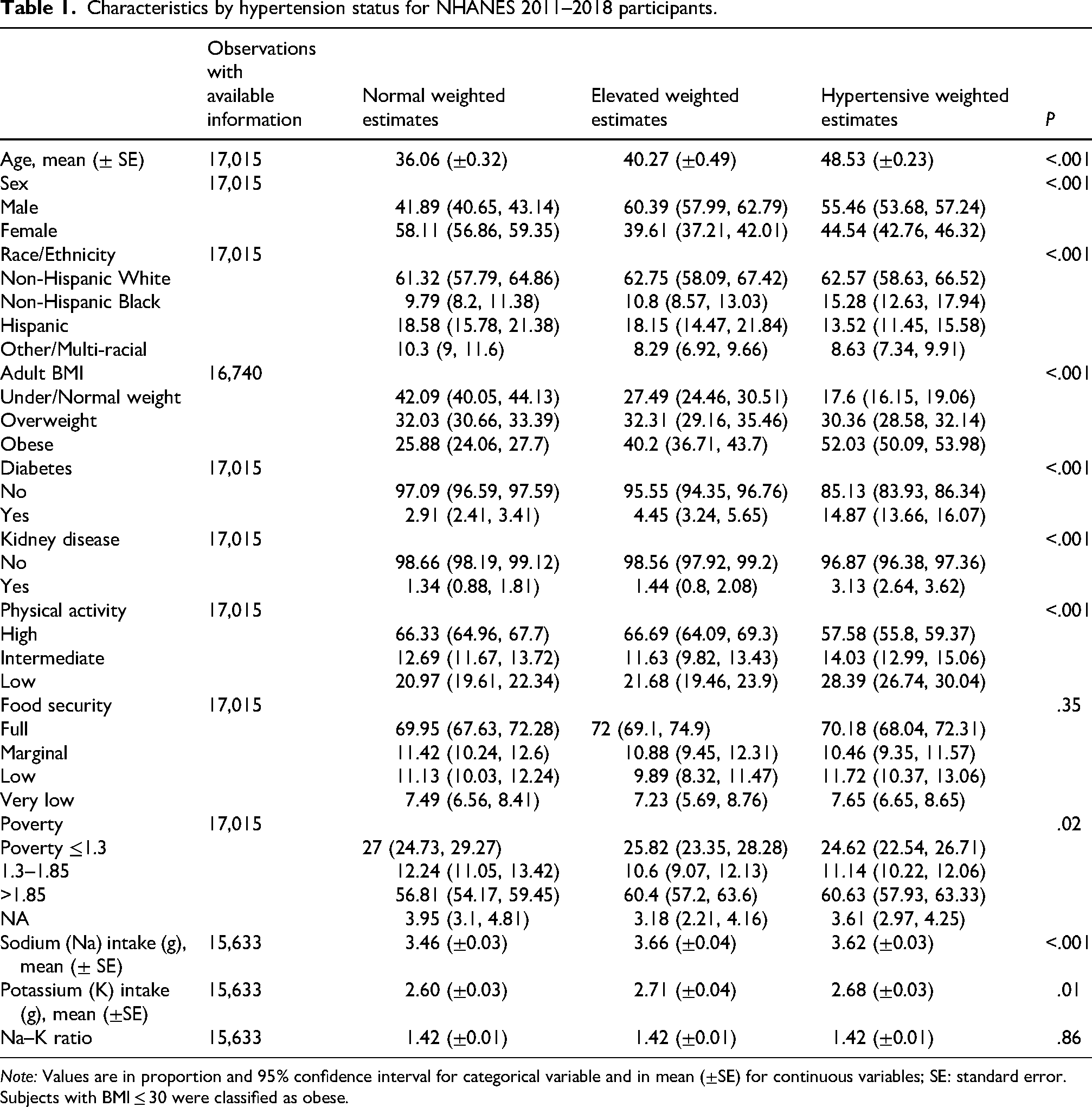
Note: Values are in proportion and 95% confidence interval for categorical variable and in mean (±SE) for continuous variables; SE: standard error.
Subjects with BMI ≤ 30 were classified as obese.
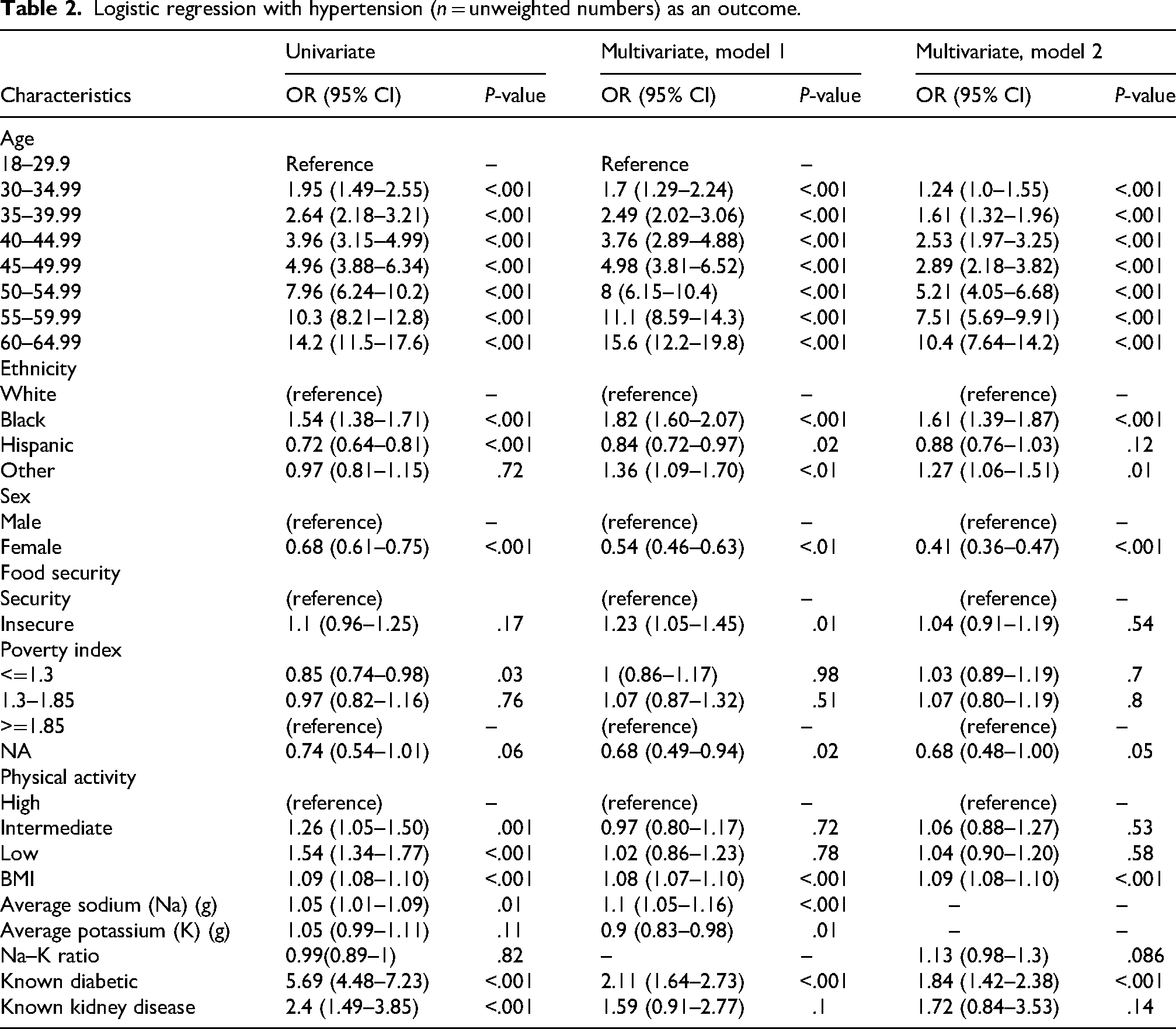
Several factors, including sex, age, race/ethnicity, and food security status, were significantly associated with an increased likelihood of hypertension (Table 2). Non-Hispanic Blacks had higher odds of hypertension compared to Non-Hispanic Whites (OR = 1.82, 95% CI: 1.60–2.07, P < .001). Participants reporting food insecurity also had higher odds of hypertension (OR = 1.23, 95% CI: 1.05–1.45, P = .01).
Logistic regression with hypertension (n = unweighted numbers) as an outcome.
Differences in sodium and potassium intake were statistically significant between the different blood pressure status groups (P < .001 and P = .01, respectively). The normal blood pressure group, on average, reported lower sodium and potassium intake (3.46 g, SE = 0.03 and 2.60, SE = 0.03, respectively) while those with elevated blood pressure reported the highest (3.66 g, SE = 0.04 and 2.71, SE = 0.04, respectively) sodium intake. There was no difference in Na:K ratio between the different blood pressure status groups (Table 1).
The study highlighted the positive associations between higher dietary sodium intake and hypertension (Table 2). Although a higher Na:K ratio was associated with an increased likelihood of hypertension, this association did not reach statistical significance in multivariate analysis (P = .09). For every 1-g increase in dietary sodium intake, the odds of hypertension increased by 10% (P < .001). Conversely, with every 1-g increase in dietary potassium intake, the odds of hypertension decreased by 10% (P < .001). The model's AUC values of 0.81 suggest a relatively strong discriminative ability between the hypertensive and non-hypertensive groups (Table 2).
Food insecurity as an outcome
Significant differences in demographic, lifestyle, and health factors were observed between the food-secure and food-insecure groups. Participants reporting food insecurity were younger than food-secure participants (average age of 39.29 ± 0.35 years vs. 42.10 ± 0.27 years) (P < .001) based on weighted estimates. Additionally, food-insecure participants were predominantly female (52%) and obese (45%) compared to food-secure counterparts (Table 3).
Characteristics by food security status for NHANES 2011–2018 participants.
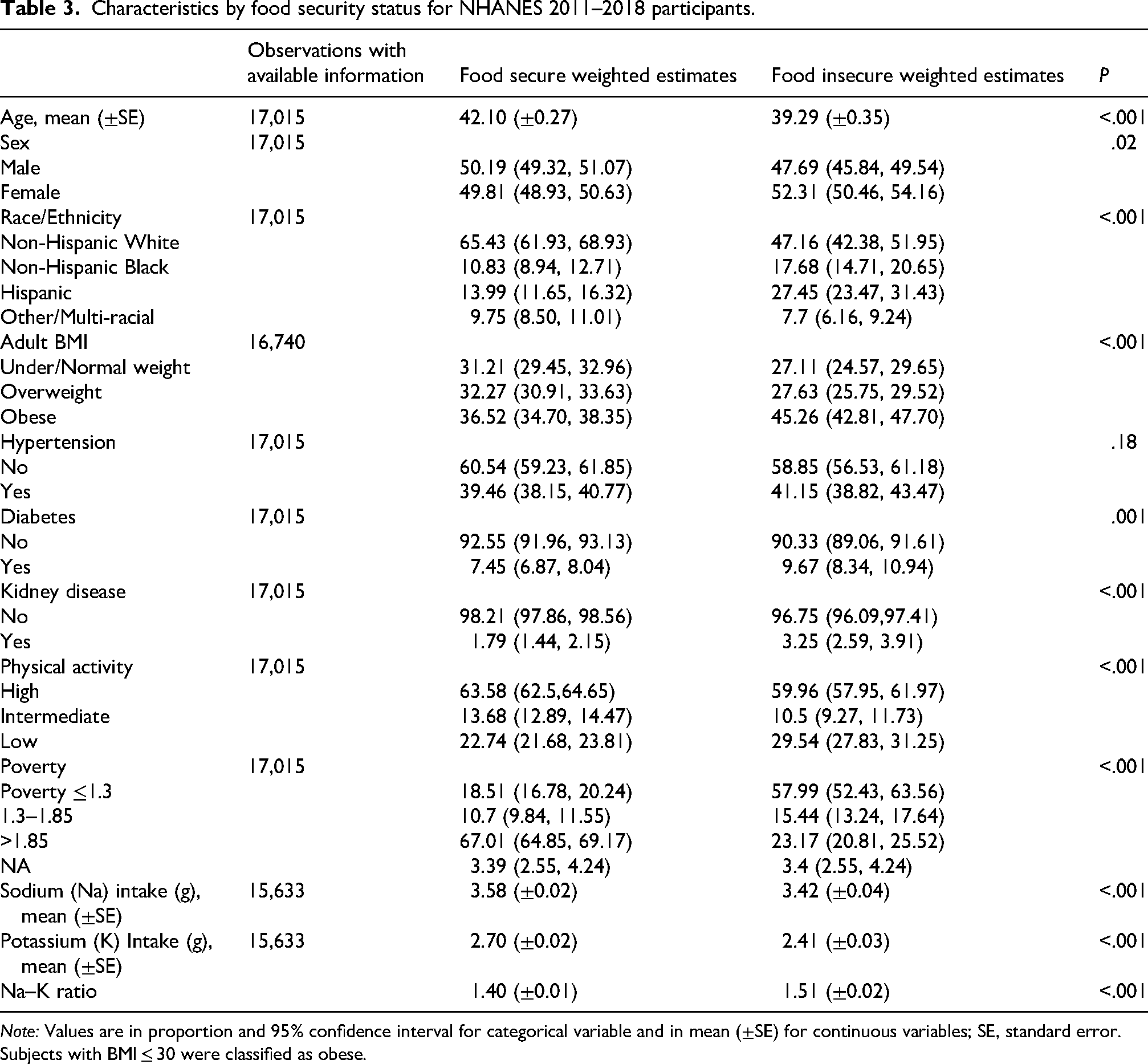
Note: Values are in proportion and 95% confidence interval for categorical variable and in mean (±SE) for continuous variables; SE, standard error.
Subjects with BMI ≤ 30 were classified as obese.
Ethnic/racial minorities were overrepresented in the group experiencing food insecurity. In multivariate analysis, Non-Hispanic Black (OR = 1.33; 95% CI: 1.05–1.68, P = .02) and Hispanic (OR = 1.78; 95% CI: 1.37–2.17, P < .001) participants were significantly more likely to experience food insecurity compared to their White counterparts (Table 4).
Logistic regression with food insecurity as an outcome.
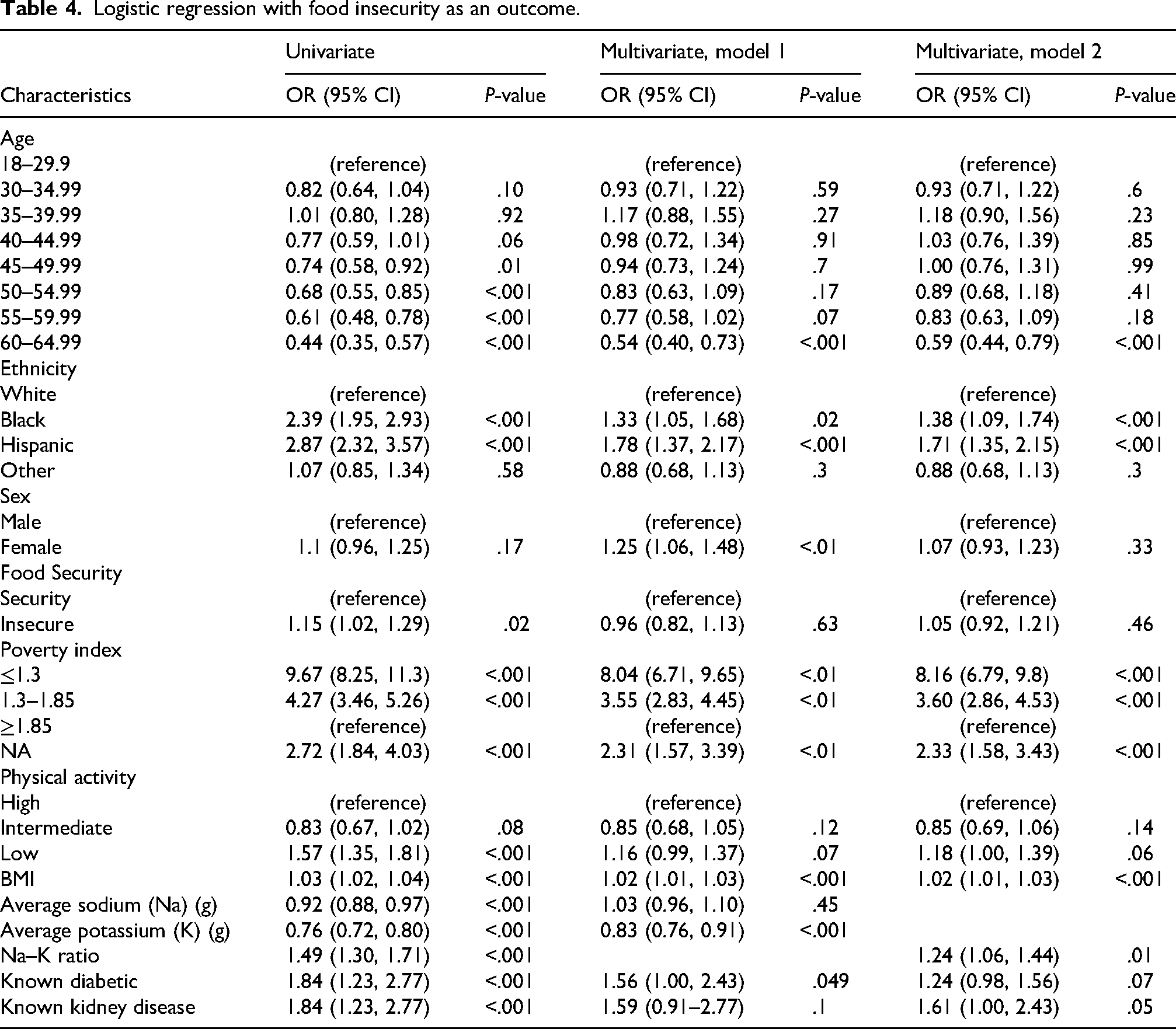
Participants reporting food insecurity exhibited a significantly lower intake of dietary potassium (2.41 ± 0.03 g) compared to food secure individuals (2.79 ± 0.02 g); P < .01). Although we found that participants with food insecurity had significantly lower mean intakes of sodium (3.42 ± 0.04 g) compared to food secure individuals (3.58 ± 0.02 g; P < .001), we found a significantly higher Na:K ratio, a hypertension risk in participants who reported food insecurity (Tables 2 and 4).
With respect to health characteristics, participants reporting food insecurity had a higher prevalence of obesity (45.26%) compared to the food secure group (36.52%; P < .01). For each unit increase in BMI, the odds of food insecurity marginally increased in both univariate (OR = 1.03; 95% CI: 1.02–1.04, P < .001) and multivariable (OR = 1.02; 95% CI: 1.01–1.03, P < .001) analyses (Table 4).
While no statistically significant difference in the prevalence of hypertension between the food secure and food insecure groups, multivariable analysis revealed that participants with hypertension were more likely to experience food insecurity (OR = 1.25; 95% CI: 1.06–1.48, P < .001) (Table 4).
Furthermore, participants with low socioeconomic status, defined by a poverty index ≤1.3 (OR = 8.04; 95% CI: 6.71–9.65, P < .001) and 1.3–1.85 (OR = 3.55; 95% CI: 2.83–4.45, P < .001), had significantly higher odds of experiencing food insecurity than those with a poverty index ≥1.85 in multivariable analyses. In addition, we observed that the level of physical activity appeared to influence food insecurity. In the multivariate analysis, participants who reported low activity levels demonstrated a higher likelihood of experiencing food insecurity (OR = 1.16; 95% CI: 0.99–1.37, P = .07) compared to participants with high levels of physical activity. The model's AUC values of 0.75 suggest a relatively moderate discriminative ability between the food-secure and insecure groups.
Mediation analysis
Finally, we applied mediation analysis to evaluate the direct effect of food insecurity, and its indirect effect mediated by dietary sodium and potassium intake on blood pressure (Figure 2). We observed that compared to individuals with food insecurity, individuals with food security had lower systolic blood pressure with a coefficient (coef.) −0.86 (CI −1.64, −0.07), P = .03 in univariable analysis. This effect was mostly from the direct effect of food insecurity, [coef. −0.94 (CI −1.70, −0.18), P = .02 and coef. −0.93 (CI −1.72, −0.15), P = .02] rather than the indirect effect mediated by daily potassium [coef. 0.08 (−0.01, 0.17), P = .07] or sodium [coef. 0.07 (0.02, 0.13), P = .01]. Meanwhile, the food security group appears to have slightly higher diastolic BP than the food insecurity group [coef. 0.66 (0.05, 1.26), P = .03 and 0.66 (0.05, 1.26), P = .03]. Again, this effect was mostly from the direct effect of food security rather than the indirect effect mediated by daily electrolyte levels. However, in the multivariable mediation analysis adjusted for other demographic factors, physical characteristics, and comorbidities (i.e., age group, gender, ethnicity, poverty index, physical activity, BMI, diabetes, and kidney disease), the results did not reach statistical significance (Table 5).
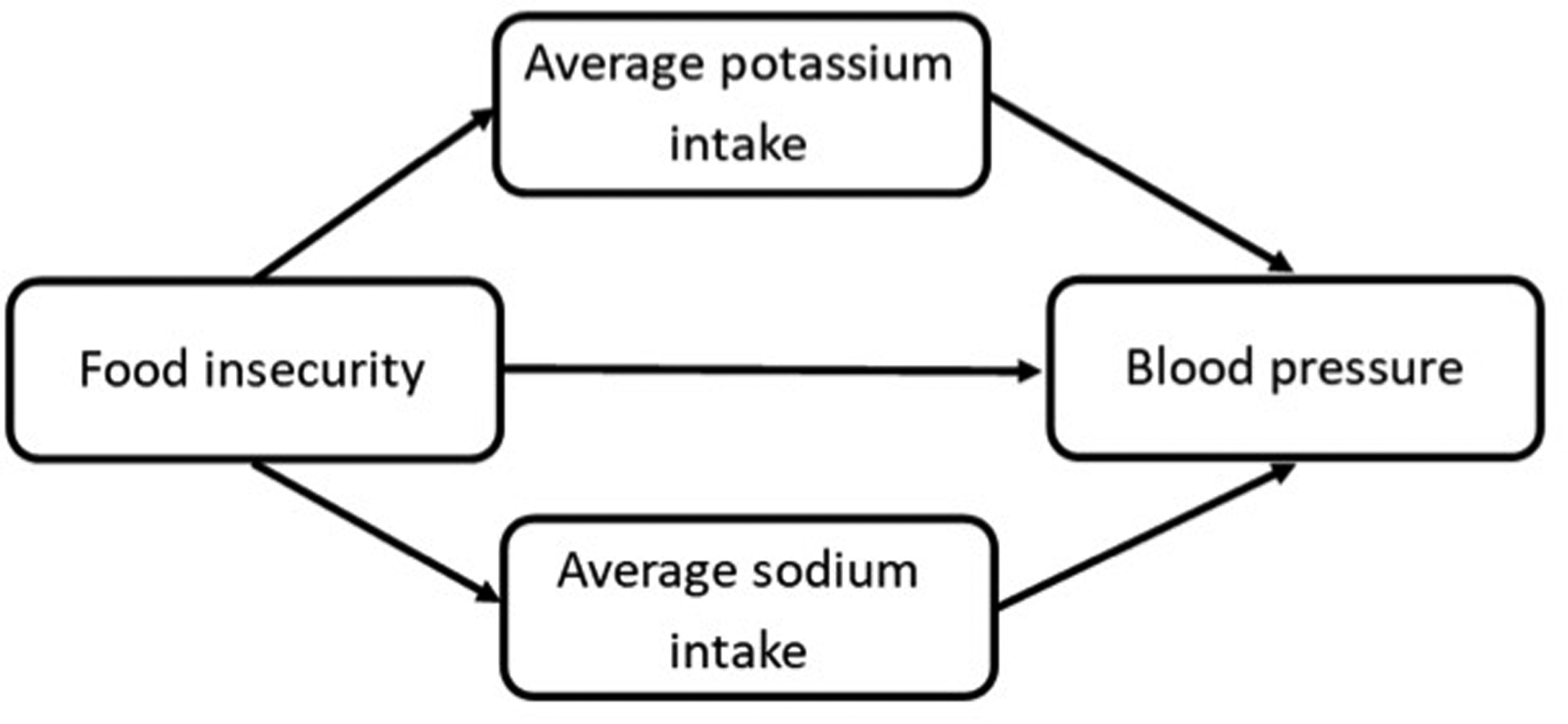
Mediation model path diagram.
Effects of food security on mean systolic and diastolic BP mediated by average sodium/potassium intake.
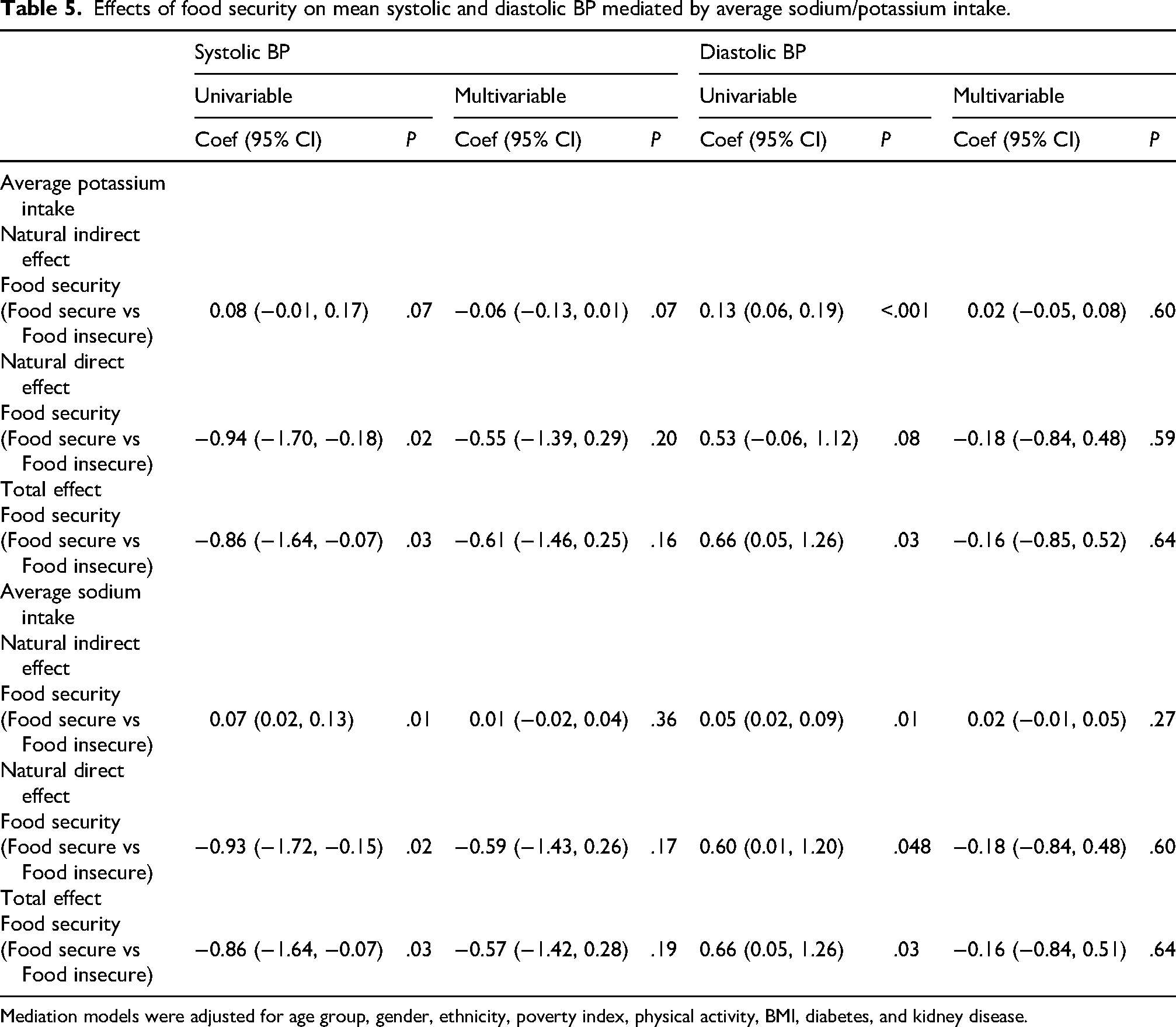
Mediation models were adjusted for age group, gender, ethnicity, poverty index, physical activity, BMI, diabetes, and kidney disease.
Discussion
This cross-sectional study investigated the relationship between food insecurity, dietary sodium and potassium intake, and hypertension risk. Our findings reveal a strong association between food insecurity and lower dietary potassium intake, likely due to lower intake of potassium-rich foods such as fruits, vegetables, and grains, which are main components of the DASH (Dietary Approaches to Stop Hypertension) eating plan (Palakshappa et al., 2021). A recent review by Arslan et al. highlights the benefits of plant-based diets on decreased risk of hypertension, improved cardiovascular health, and reduced cardiac and all-cause mortality (Arslan et al., 2024). This provides evidence supporting dietary interventions to decrease hypertension risk and aligns with models demonstrating reduced dietary intake of vegetables and fruits as leading risk factors for cardiometabolic mortality (Perez and Chang, 2014).
Prior research has shown that the Na:K ratio is a more reliable predictor of BP than sodium or potassium alone (Elmadfa and Meyer, 2010). However, our study found only a weak link between a high Na:K ratio and hypertension after adjusting for other factors. This result may be due to limitations in our data. The 24-h dietary recall method used can be inaccurate because of recall bias and errors in estimating portion sizes (Beltrán et al., 2020). It is also possible that other factors, like BMI, race/ethnicity, or physical activity, may have masked the true relationship. Despite these limitations, we still observed a high Na:K ratio in individuals who are food-insecure. This finding is important because it supports existing research linking the Na:K ratio to a higher risk of hypertension (Elmadfa and Meyer, 2010). Public health initiatives should therefore focus on increasing access to potassium-rich foods, especially among populations at risk of food insecurity (Palakshappa et al., 2021). Future studies using more precise measurement methods, such as 24-h urine tests, are needed to confirm the true effect of the Na:K ratio on BP.
While we observed a higher mean dietary sodium intake among individuals with hypertension, as has been previously established (Gundersen et al., 2017), the relationship between food security and sodium intake was less clear. This may be attributed to limitations in dietary recall methods; acknowledging the potential recall bias and the inherent variability in nutrient contents of foods in the food composition tables is important (Ing et al., 2023). For clinical and health-related research, exploring complementary methods (e.g. 24-h urine collection) may be necessary to enhance accuracy and address these limitations.
Our findings reinforce the established link between food insecurity and hypertension among US adults (Aggarwal et al., 2021; Banerjee et al., 2024; Hertz et al., 2005; Micha et al., 2017; Rasmusson et al., 2018; Royer et al., 2025; Tian et al., 2025). Understanding the mechanisms contributing to hypertension risk in food-insecure individuals, such as dietary changes chronic stress, and unhealthy coping mechanisms like smoking or reduced physical activity, can inform targeted interventions to effectively manage hypertension in vulnerable populations.
Our study supports prior research indicating a high prevalence of hypertension (Dhunna and Tarasuk, 2021; Fernandez et al., 2023) and food insecurity (To et al., 2014) in Non-Hispanic Black participants. In contrast, non-Hispanic White and Hispanic participants, despite having a high prevalence of food insecurity, did not exhibit a significant influence on hypertension risk. This complex interplay between ethnicity, food security, and health outcomes (Bateson and Pepper, 2023) requires further investigation to develop culturally sensitive interventions that address the broader social determinants of health that can promote more equitable health outcomes. Additionally, future research should investigate how sodium and potassium intake vary by sex and ethnicity to clarify the link between dietary patterns, food insecurity, and hypertension risk. Stratified analyses may help identify high-risk groups and inform targeted, public health efforts.
Predictably, we found a higher prevalence of obesity, a known hypertension risk factor, in individuals from food-insecure households. Our finding that food insecure adults were less likely to be engaged in physical activity aligns with a study by To et al. (To et al., 2014). This suggests a complex interplay wherein food insecurity may influence physical activity levels. These interrelated factors contribute to the increased burden of hypertension among food insecure populations.
It is important to acknowledge the study's limitations. Firstly, potential selection bias may exist, given the response rate to the food security questionnaire and missing information in the dataset, affecting generalizability. Secondly, dietary assessment methods for sodium and potassium intake may be influenced by self-report, challenges in quantifying salt, and failure to account for non-food sources of sodium such as supplements, and nutrient coding errors (Gibson et al., 2017). Thirdly, reliance on self-reported measures of food insecurity and dietary intake introduces potential recall bias or social desirability bias (Gittelsohn et al., 2022). Additionally, the cross-sectional design of NHANES limits causal inference, and the use of within-person mean instead of using generalized mixed methods for estimating nutrient intake simplifies the approach but may be more susceptible to errors (Herrick et al., 2018). Lastly, given the relatively simple mediation structure, we selected a traditional mediation analysis framework, which is well-suited for estimating and interpreting direct and indirect effects in this context. While more advanced statistical techniques such as structural equation modeling could be employed to analyze complex relationships and latent constructs, our primary objective was to evaluate the direct effect of food insecurity and its indirect effect on the outcome via dietary sodium and potassium intake. We prioritized interpretability and accessibility for a broader clinical audience.
In conclusion, the study underscores the critical role of social determinants of health, particularly food insecurity, in the prevalence of hypertension. Our findings highlight the need for comprehensive interventions targeting vulnerable populations to address disparities in hypertension prevalence. By improving food security, promoting access to nutrient-rich foods, and implementing culturally sensitive programs, we can significantly reduce the burden of hypertension. Further research is essential to elucidate the complex mechanisms underlying these relationships and to develop effective strategies for prevention and management. Addressing the root causes of food insecurity and its impact on dietary patterns, especially in low-income communities, can significantly contribute to lessening the burden of hypertension and achieving equitable health outcomes for all (Ziso et al., 2022).
Supplemental Material
sj-docx-1-nah-10.1177_02601060251410454 - Supplemental material for Dietary sodium and potassium patterns in adults with food insecurity in the context of hypertension risk
Supplemental material, sj-docx-1-nah-10.1177_02601060251410454 for Dietary sodium and potassium patterns in adults with food insecurity in the context of hypertension risk by Elizabeth A Onugha, Ankona Banerjee, D. Vimalajeewa Horahenage, Kenneth J Nobleza, Duc T Nguyen, Susan B Racette and J Dave in Nutrition and Health
Footnotes
Acknowledgments
The authors thank Victor Davila-Roman MD, Lisa de Las Fuentes MD, MS and DC Rao, PhD, the leadership of the PRIDE (Programs to Increase Diversity Among Individuals Engaged in Health-Related Research) program in Cardiovascular Disease Comorbidities, Genetics and Epidemiology (CVD-CGE) for the mentored research experience of the PRIDE program. We also acknowledge Linda Schreier, BS, the program manager.
Ethical approval
The Baylor College of Medicine Internal Review Board deemed this study exempt from review due to the use of publicly available, de-identified data.
Consent for publication
All participants provided informed consent upon enrollment into the NHANES study. The Baylor College of Medicine Internal Review Board deemed this study to be exempt from review because of the use of publicly available, de-identified data.
Authors’ contributions
EO and SR conceptualized and designed the study. AB, KN, and DN curated, analyzed, and interpreted the data. EO and AB drafted the manuscript. EO, AB, HV, KN, DN, SR, and JD critically reviewed and edited the manuscript. All authors have read and approved the final version of the manuscript for submission.
Funding
This work was funded in part by the National Heart, Lung, and Blood Institute (NHLBI) (Grant R25 HL105400) to Victor G. Davila-Roman and DC Rao. This work was also funded, in part, by federal funds from the USDA/ARS under Cooperative Agreement no. 58-3092-0-001 (J.M.D.). The contents of this publication do not necessarily reflect the views or policies of the USDA nor does the mention of trade names, commercial products, or organizations imply endorsement from the U.S. government.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.