
Abstract
Introduction
Purposeful soccer heading is unique to soccer and a skill routinely used by players during gameplay. However, soccer heading is a mechanically induced neurophysiological disruption (MIND) that, when repeated frequently, may negatively affect a player's brain health (Lavender et al., 2022). Soccer heading frequencies are associated with microstructural alterations in brain white matter and cognitive abnormalities (Lipton et al., 2013). Furthermore, soccer heading frequencies are associated with more microstructural alterations in women than men (Rubin et al., 2018). Thus, heading frequencies during soccer participation may indicate potential alterations in player brain health, with higher frequencies reflective of possible brain injury and inflammation, particularly in women.
Omega-3 polyunsaturated fatty acids (PUFAs), docosahexaenoic acid (DHA), and eicosapentaenoic acid (EPA) have anti-inflammatory properties (Gabbs et al., 2015). These properties are potentially neuroprotective against brain injury from repeated head impacts in contact sports populations (Heileson et al., 2021; Raikes et al., 2022). When the brain is mechanically injured, omega-3s are released from neuronal membranes and metabolized to help reduce inflammation and promote injury recovery (Dyall, 2015; Lust et al., 2020). This response to head impacts can reduce omega-3 content in brain tissue (Wu et al., 2014). The red blood cell (RBC) content of PUFAs and Omega-3 Index, defined as the percentage of EPA + DHA to the total RBC fatty acid content, are biomarkers for omega-3 tissue status, including brain tissue (Létondor et al., 2014). During a competitive soccer season, Omega-3 Index declines with increased training loads (Huggins et al., 2019). However, these measured training loads have not accounted for soccer heading frequencies. Thus, it is unknown if higher heading frequencies correlate with reductions or lower RBC omega-3 status. Such an association would support examining RBC omega-3 status and its role in the brain health of soccer players. Therefore, this preliminary study explored if there is an association between soccer heading frequencies and RBC omega-3 status in collegiate women soccer players during a competitive season.
Methods
Participants
Sixteen participants from a single National Collegiate Athletic Association (NCAA) Division-1 (D-1) women's soccer team completed the study. Inclusion criteria for study enrollment included being on the current team roster, physically healthy, and being able to participate in all sport-related activities, according to the team's sports medicine staff. Exclusion criteria included any player recovering from a physician-diagnosed concussion or not medically cleared to participate in all activities. Players were also excluded from the study if, during the competitive season, they were diagnosed with a concussion, suffered a season-ending injury, or had injuries that resulted in missing more than 14 days of sport-related activities. Players were also excluded if they did not record gameplay minutes or correctly complete the bi-weekly HeadCount questionnaires. During the competitive season, two players were diagnosed with a concussion, three experienced season-ending injuries, three did not record gameplay minutes, and two did not correctly complete all HeadCount questionnaires. Therefore, out of the 26 players initially enrolled in this study, only 16 players met all respective inclusion/exclusion criteria and were included in this study.
Experimental design
A prospective cohort study design was used with data collection for omega-3 status at two-time points (i.e., pre/postseason) and header frequencies at seven-time points (i.e., bi-weekly) throughout a fall (August-November) competitive season. Bi-weekly electronic surveys using the HeadCount questionnaire were completed during the season to quantify header frequencies. Gameplay stats like games played and cumulative gameplay minutes were collected following the season. The study protocol received approval from the investigator's institutional review board at the University of Kansas Medical Center (number. 00147365). Participation in this study was strictly voluntary. This study has been conducted according to the Declaration of Helsinki; each player provided their written informed consent before study participation.
Omega-3 status: RBC and diet
RBC omega-3 status and the Omega-3 Index were analyzed using dried blood spot supply kits and collection instructions from OmegaQuant Analytics, LLC, a Clinical Laboratory Improvement Amendments-certified laboratory that provides RBC fatty acid content profiling and Omega-3 Index testing (Sioux Falls, SD). Dietary assessment of habitual omega-3 dietary intake was completed using a targeted seven-question food frequency questionnaire (FFQ) to assess DHA and EPA intake and grouped foods based on respective content (Kuratko, 2013). This brief FFQ was used to ensure dietary omega-3 consumption, including supplementation, was accounted for when examining a player's RBC omega-3 status, given the diet's known influence on this biomarker (McDonnell et al., 2019). Furthermore, this FFQ was utilized because it correlates with RBC EPA and DHA content in the general population and women soccer players (Kuratko, 2013; Essman et al., 2022).
Headcount questionnaire
Study participants completed a previously validated self-report measure, HeadCount, to quantify gameplay header frequencies throughout the competitive season (Catenaccio et al., 2016). HeadCount is a web-based, structured, self-administered two-week recall questionnaire that assesses soccer heading exposures during competitive gameplay and practice. The questionnaire was electronically administered bi-weekly throughout the competitive season via REDCap; a secure web application for building and managing online surveys.
Gameplay stats and anthropometrics
Following the competitive season, gameplay stats specific to games played and cumulative gameplay minutes were collected for each study participant. These gameplay stats were obtained from the University's athletic department website. This website is available to the public and provides cumulative and game-by-game statistics for each player on the team during each competitive season. In addition, player anthropometrics specific to height (cm), weight (kg), and body mass index (kg/m2) were collected and calculated, respectively, from the team's preseason assessment.
Statistical analysis
Descriptive statistics for study participants, omega-3 status (i.e., RBC and dietary consumption), gameplay header frequencies, games played, and gameplay minutes are summarized as frequencies, means, standard deviation (SD), median (interquartile range), and range (min−max). Since data did not satisfy the normality assumption, a non-parametric approach was used for data analysis. A Wilcoxon signed-rank test compared the study participants’ RBC and dietary omega-3 status before and after the competitive season. A Spearman's rank correlation analysis examined the relationship between omega-3 status, gameplay header frequencies, and gameplay minutes. A simple linear regression was used to predict RBC omega-3 status measures using gameplay header frequencies. A p-value of less than 0.05 was considered statistically significant. Data were analyzed using SPSS statistics software (SPSS Statistics; IBM).
Results
Table 1 contains the descriptive characteristics, including omega-3 and gameplay characteristics of the study participants. No study participants reported taking omega-3 supplementation throughout the competitive season. Median omega-3 dietary intake (i.e., DHA + EPA) was low and not significantly different: preseason, 93 (104) mg/d; postseason, 96 (78.1) mg/d. The mean pre/postseason Omega-3 Index was low at 3.95 ± 0.44%. Study participants averaged 16 ± 6.5 games played, 47 ± 36.5 cumulative gameplay headers, 2.7 ± 1.5 headers per game, 696 ± 513 cumulative gameplay minutes, and 37.3 ± 22 min per game.
Descriptive characteristics of participants (n = 16).
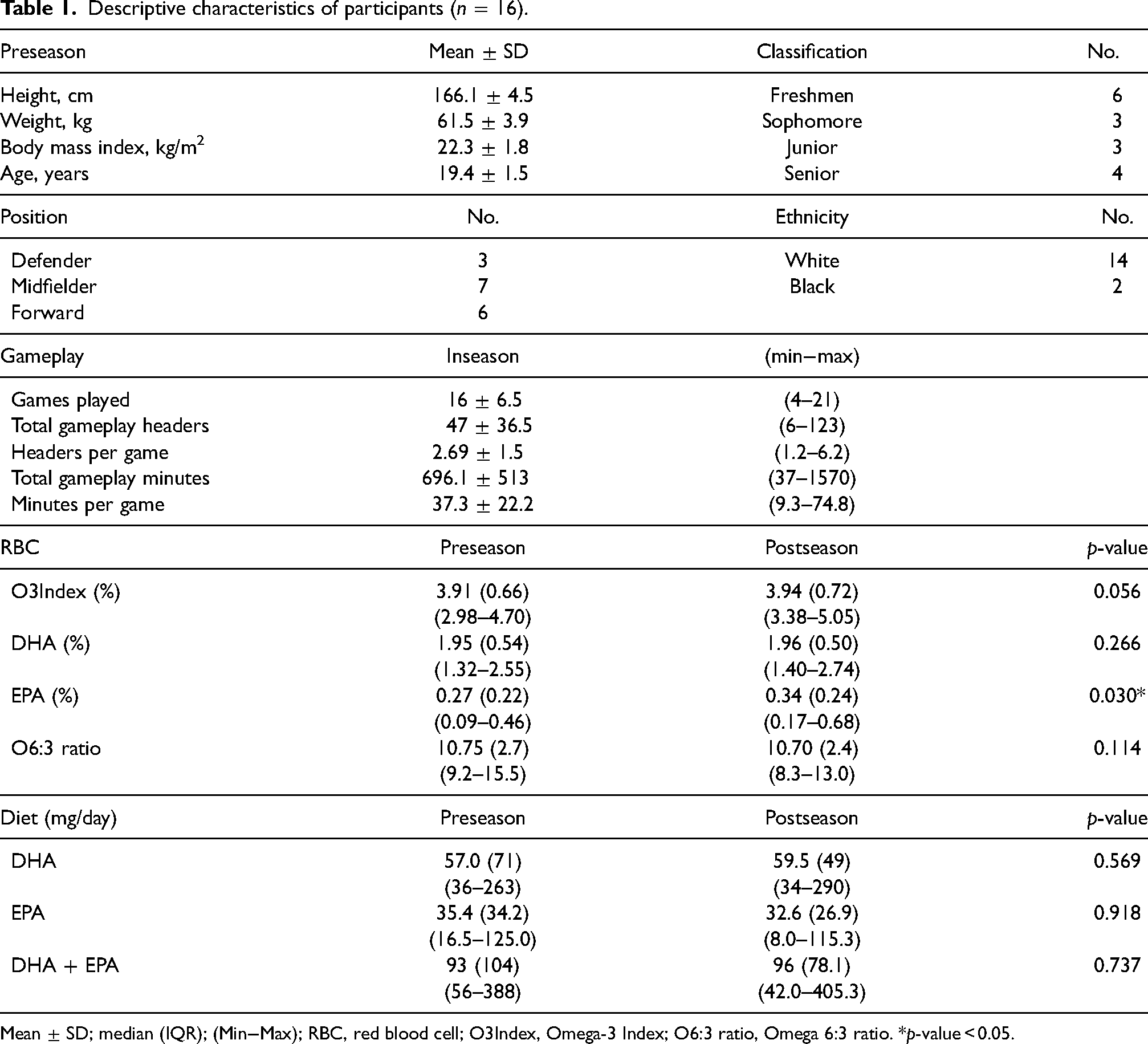
Mean ± SD; median (IQR); (Min−Max); RBC, red blood cell; O3Index, Omega-3 Index; O6:3 ratio, Omega 6:3 ratio. *p-value < 0.05.
Table 2 shows the correlation matrix between RBC and diet omega-3 fatty acids at preseason and postseason and between postseason and change (i.e., post-preseason) in RBC omega-3 status and in-season gameplay characteristics. At preseason, diet and RBC omega-3 were positively correlated. However, at postseason, no correlation was observed. Cumulative gameplay headers negatively correlated with postseason Omega-3 Index (r = −0.545, p = 0.029) and positively correlated with postseason omega 6:3 ratios (r = 0.719, p = 0.002). Average headers per game negatively correlated with change in Omega-3 Index (r = −0.663, p = 0.005) and near statistical significance with change in RBC DHA content (r = −0.494, p = 0.052). Cumulative gameplay minutes and minutes per game did not correlate with postseason Omega-3 Index and RBC DHA content. Likewise, seasonal changes in Omega-3 Index, including RBC DHA and EPA content and omega 6:3 ratio, did not correlate with cumulative gameplay minutes and minutes per game.
Omega-3 fatty acids (blood,diet) and inseason gameplay correlation table (n = 16).
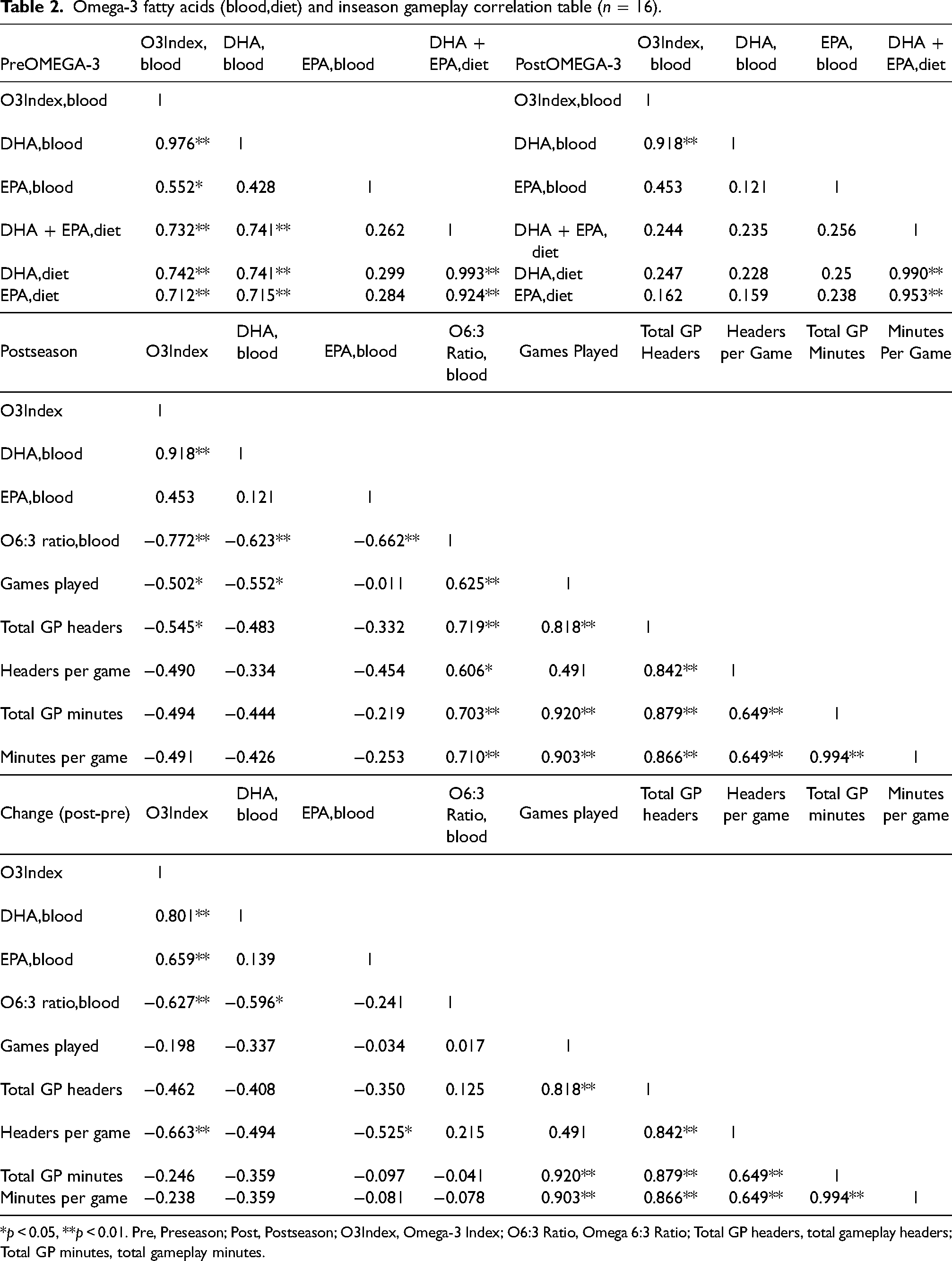
*p < 0.05, **p < 0.01. Pre, Preseason; Post, Postseason; O3Index, Omega-3 Index; O6:3 Ratio, Omega 6:3 Ratio; Total GP headers, total gameplay headers; Total GP minutes, total gameplay minutes.
Figure 1 shows gameplay header frequencies prediction of postseason and change in RBC omega-3 status using simple linear regression. The fitted regression model for cumulative gameplay header frequencies prediction of postseason RBC omega-3 status were near statistical significance for Omega-3 Index (r = 0.459, p = 0.074) and significant for omega 6:3 ratio (r = 0.629, p = 0.009). The fitted regression model for average headers per game prediction of change in RBC omega-3 status was near statistical significance for Omega-3 Index (r = 0.457, p = 0.075) and RBC DHA content (r = 0.460, p = 0.073).
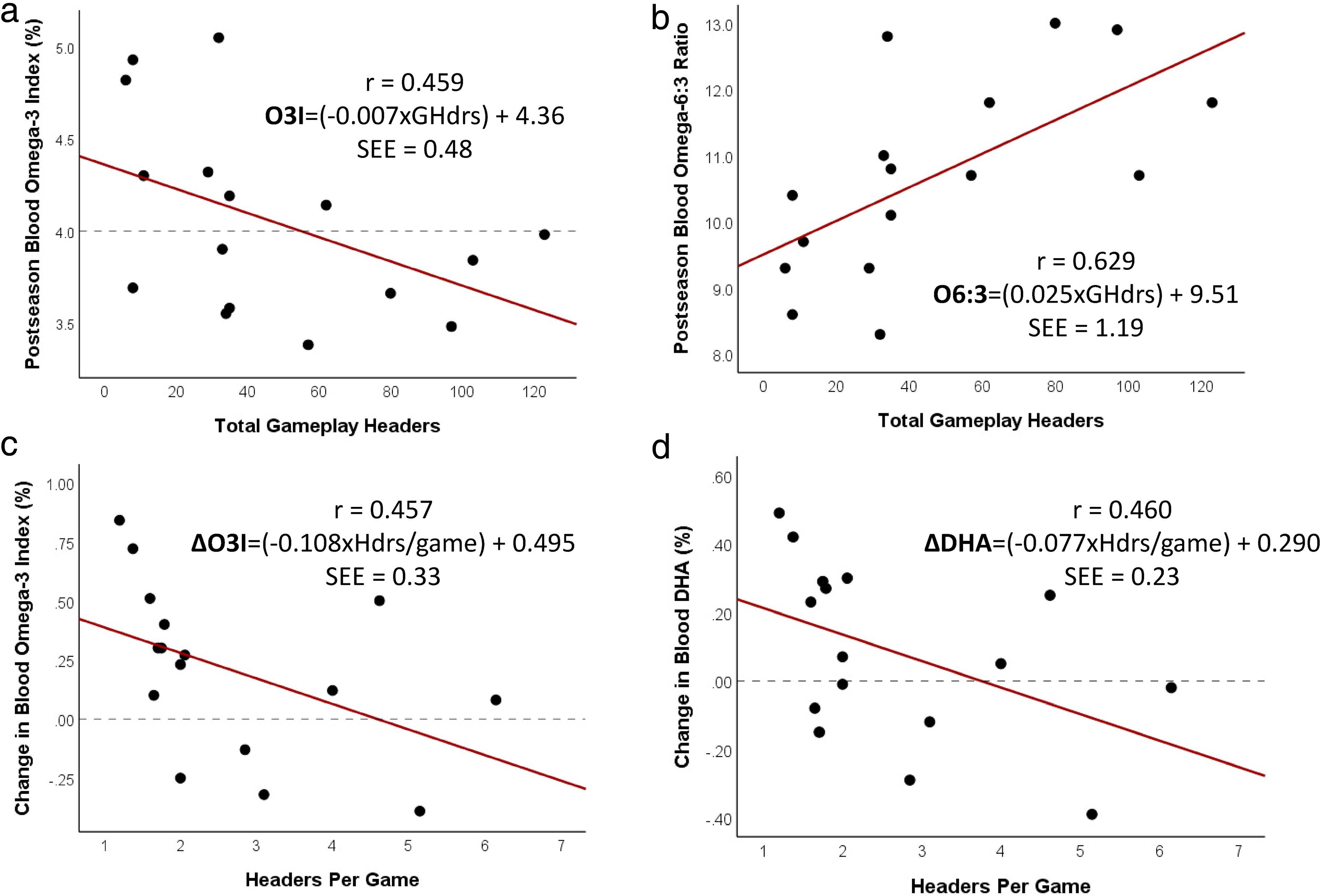
The relationship between blood omega-3 fatty acids (postseason and change [postseason−preseason]) and gameplay header frequencies (total and headers per game). Graphs showing results of simple linear regression analysis including r-value and SEE to predict blood omega-3 status (a) Omega-3 Index, (b) Omega-6:3, (c) Change in Omega-3 Index, and (d) Change in DHA. Data below (—) lines are undesired values or changes in blood omega-3 fatty acids. O3I, omega-3 Index; GHdrs, total gameplay headers; Hdrs/game, headers per game played; Δ, change (post-preseason).
Discussion
This study is the first to explore the relationship between RBC omega-3 status and heading frequencies in soccer players. In a sample of collegiate women's soccer players, we observed that RBC omega-3 status following a competitive season was negatively associated with header frequencies and not associated with gameplay minutes or dietary omega-3 intake. These findings suggest that higher gameplay heading frequencies during a competitive season may negatively influence omega-3 status. Therefore, these preliminary findings provide new implications for altered dietary requirements for soccer players and concerning implications for player brain health if omega-3 status is not addressed during a competitive season of frequent soccer heading.
The primary findings were RBC omega-3 status and Omega-3 Index negatively associated with gameplay header frequencies. Omega-3 Index is a stable biomarker resistant to artificial changes and has low within-subject variability compared to plasma fatty acid measurements (Harris, 2013). Data collection of RBC omega-3 measures pre/postseason aligned with Omega-3 Index test-retest recommendations according to OmegaQuant to ensure RBC membrane composition reaches a new steady state. Thus, the RBC omega-3 values presented here reflect the players’ new steady state following the season, which concerns players with lower RBC omega-3 status and more frequent heading. In collegiate American football players, higher RBC omega-3 status from omega-3 (DHA + EPA) supplementation blunts a rise in blood neurofilament light (NfL) concentrations, a sensitive blood biomarker for brain injury, throughout a competitive season of repetitive helmet impacts (Heileson et al., 2021). In addition, higher RBC omega-3 status in American football players improves brain functional connectivity (Raikes et al., 2022). These findings highlight the importance of higher RBC omega-3 status for player brain health in contact sports populations exposed to repeated head impacts. Therefore, the negative associations observed in this study and soccer may reflect undesired alterations in player brain health for those with higher header frequencies and lower RBC omega-3 status. However, more clinical research is needed to confirm these preliminary findings.
Our findings also observed no associations between RBC omega-3 status and omega-3 intake or soccer gameplay minutes following the competitive season. These findings differ from previous research reporting reductions in Omega-3 Index in male soccer players during higher exercise training loads (Huggins et al., 2019). However, the measured soccer training loads did not include header frequencies. Thus, based on our findings, the previously reported reductions may be due, in part, to frequent soccer heading, which can occur during higher soccer training loads given in our sample gameplay minutes associated with heading frequencies, see Table 2. Also, previous research reports that non-contact chronic exercise does not alter RBC fatty acid composition (Nikolaidis and Mougios, 2004). Dietary omega-3 intake does, however, influence RBC fatty acid composition (McDonnell et al., 2019). In collegiate women's soccer players, we have previously observed preseason omega-3 intake associated with the Omega-3 Index (Essman et al., 2022), like our current preseason study findings. However, despite no change in intake, postseason RBC omega-3 status did not associate with omega-3 intake, suggesting that soccer-related factors like heading frequencies may influence the known relationship between diet and RBC omega-3 status.
Gameplay characteristics during the competitive season included high, mid, and low-minute players with self-reported gameplay header frequencies like measured header frequencies previously reported in an NCAA D-1 women's soccer team (Press and Rowson, 2017). Also, the observed low Omega-3 Index levels and low omega-3 intake are like other male and female collegiate athlete populations (Ritz et al., 2020), with intake well below the Academy of Dietetics and Nutrition (AND) recommended intake of 500 mg/d (Vannice and Rasmussen, 2014). Thus, our reported gameplay and omega-3 characteristics reflect expected values in this collegiate athlete and sports population.
This study is not without its limitations. First, our sample size was small and included a single D-1 team of female athletes. Therefore, the findings in this study cannot be generalized to other sports and athlete populations. However, this study does provide team-specific insight into potential sport-related health changes during a competitive season. A second limitation is that gameplay header frequencies were self-reported and not directly observed or measured. A final limitation is that this study did not quantify training loads or capture the menstrual cycle phase, which may be confounding variables.
In conclusion, findings from this preliminary study highlight the potential negative role gameplay soccer heading frequencies may have on RBC omega-3 tissue status despite already low omega-3 dietary intake and omega-3 status. These findings have implications for altered dietary requirements and a need to emphasize omega-3 dietary intake among soccer players, particularly women, during competitive play. They also provide concerning implications for undesired alterations in brain health when exposed to higher frequencies of soccer heading. Thus, future research is needed to examine the relationship between soccer heading frequencies, omega-3 status, and measures of brain health. Furthermore, since RBC omega-3 status can be influenced by estrogen and progesterone, there is a need to examine this relationship separately for men and women in the future.
Footnotes
Acknowledgments
The authors would like to Amanda Ralton, the coaching staff, and the athletes who participated in the study for their time, commitment, and support of this research project. The authors would also like to thank Dr. Michael L. Lipton and his lab for their time and assistance in providing us with the HeadCount questionnaire.
Data availability
The raw data supporting the conclusions of this article will be made available by the authors without undue reservation.
Authors' contributions
AC: conceptualization, methodology, project administration, investigation, data curation, formal analysis, writing—original draft, and writing—review and editing. LDS: conceptualization, methodology, and writing—review and editing. All authors approved the submitted version.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study involving human participants was reviewed and approved by the University of Kansas Medical Center Institutional Review Board (number. 00147365). The participants provided their written informed consent to participate in this study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded through startup funding from the Department of Dietetics and Nutrition to AC within the School of Health Professions at the University of Kansas Medical Center.