
Abstract
In a world afflicted by COVID-19, many people consult doctors through a digital interface or over the phone, as face-to-face consultations are almost impossible during a lockdown. The Medical Council of India and the NITI Aayog, a policy think tank, formulated new guidelines to empower medical practitioners to practice telemedicine in India in March 2020. Even before the COVID-19 pandemic gripped the world and made digital consultations a necessity in specific cases, academic studies located within a health promotion framework in Western contexts indicated that patients have been very much interested in using social media tools to communicate with their physicians. Previous studies have also highlighted the advantages of information and communication technologies for patient–doctor interaction.
Since changes introduced by digital health technologies have primarily been analysed from such health promotion perspectives that often adopt a ‘techno-utopian’ lens (Lupton, 2013), it becomes imperative to critically interrogate how such changes construct specific subjectivities and shape our understandings of health and normative healthcare practices. Specifically, scholars have highlighted how social media platforms and apps act as ‘performative devices’ (Johnson, 2014) that influence ‘everyday management of illness and health’ and help create the ideal of the ‘digitally engaged patient’ (Lupton, 2013).
In the Indian context, media reports highlight a growing trend in the use of social media platforms and apps by physicians and patients. However, academic research on such emerging phenomena in this country is still scarce. This exploratory study examines why some Indians connect with physicians on a social media platform such as Facebook, the nature of communication between them and their understandings of health. It uses in-depth interviews and draws upon neoliberal governmentality as a theoretical anchor.
The findings show how the internalization of neoliberal values and assumptions are associated with participants’ search for lifestyle and medical advice in everyday digital spaces such as Facebook. This study strives to extend the concept of neoliberal governmentality to performances in everyday digital spaces such as Facebook. In terms of practical implications, the results of the study highlight the critical need for policies that regulate the medical content available in social media spaces. Most importantly, some of the issues highlighted by the participants in this study can help policymakers take adequate precautions while formulating guidelines on digital consultations, especially during pandemics and their aftermath when there is tremendous pressure to promote telemedicine.
INTRODUCTION
Moreover, physicians, especially in Western settings, have often expressed their discomfort in connecting with patients on the platform (Chretien, 2010; Jain, 2009). In the case of India, media reports highlight a growing trend in the use of social media platforms and apps by physicians and patients. However, academic research on such emerging phenomena in this country is still scarce. This study strives to explore this nascent area of research.
Overall, the study seeks to contribute to the existing literature in critical health communication and healthcare management, especially in the case of online interface usage. It extends the Foucauldian concept of neoliberal governmentality to understand and interpret the health-related practices and performances of individuals in social media spaces such as Facebook in the Indian context. The following sections include a brief account on healthcare in India followed by a review of literature on the usage of information and communication technologies (ICTs) in healthcare. A section on the concept of governmentality and its theoretical relevance ensues, followed by an account of the research methods. Analysis of the findings and their implications follow.
CONTEXTUAL BACKGROUND: THE HEALTHCARE SECTOR IN INDIA
The Indian healthcare sector comprises both government-run hospitals and private establishments. While the public healthcare sector continues to perform poorly due to insufficient funds and overall neglect (Chakravarthi et al., 2017), private medical care remains expensive (Kumar & Gupta, 2017). The country’s healthcare system also suffers from multiple contradictions. Its healthcare expenditure is amongst the lowest in the world. It comprised just 1.41% of its GDP in 2017–2018 (Press Trust of India, 2018). Around 71% of health spending in India is met by people’s own savings called ‘out-of-pocket’ expenses, which contributes to increasing poverty (Hooda, 2017). Apart from inadequate health insurance (Ghosh, 2017), other challenges include a low doctor–patient ratio, concentration of doctors in big cities (McIntyre, 2017) and the double burden of coping with both communicable and non-communicable diseases (The Lancet, 2018) apart from a burgeoning population of 1.3 billion people.
While deep inequalities mark the Indian medical landscape in access to healthcare, many amongst the educated middle class in India have improved access to health information and demonstrate high levels of biomedical literacy (Broom et al., 2017). Many in India connect with their doctors on social media platforms and apps such as Facebook and WhatsApp (McIntyre, 2017). In 2018, India had 483 million Internet users (Statista, 2019c). Facebook, specifically, has 281 million users in India (Statista, 2019b) with a male-to-female gender ratio of 77:23 (Statista, 2019a). With more Indians getting access to the Internet, the current Indian government has repeatedly emphasized that it intends to use ICTs to improve healthcare facilities (Indo-Asian News Service, 2018). It has made health an important aspect of its ‘Digital India’ campaign (Mills & Hilberg, 2018) with the goal of transforming India into ‘a digitally empowered society and knowledge economy’ by using information technology in the field of public services (Government of India, n.d.). Digital technology is often perceived as a panacea for health issues in India today, and the government has launched various apps in this regard, including the Aarogya Setu app in April 2020, with the reported purpose of tracking COVID-19 infections in the country (Banerjea, 2020).
LITERATURE REVIEW: ICTs AND HEALTHCARE
While the review of literature did not yield any academic studies on Indians using Facebook to connect with doctors, Indian news media regularly carry reports on patients using social media platforms and apps to connect with them (Chandna & Dubey, 2016; Dhar, 2015; Fristpost, 2015). Academic literature located within a health promotion framework in Western contexts highlights that a patients’ interest in using social media tools to communicate with physicians remains strong (Andreassen et al., 2006; Jiang & Street, 2017; Lee et al., 2015; Rice & Katz, 2006). In the U.S. context, Jiang and Street (2017) found that younger, more educated and wealthier patients with easier Internet access were more likely to communicate online with doctors. However, Jacobs et al. (2017) observe that since people with less-privileged backgrounds are more dependent on traditional media and medical practitioners for health information than on the Internet, reliance on digital health technologies alone to provide health information is likely to perpetuate inequalities in terms of accessibility. Of course, advocates of the usage of digital technologies in healthcare highlight the advantages of ICTs for patient–doctor interaction, such as greater access and flexibility for patients in their interactions with physicians, the possibility of getting a quick response from a physician and overall improvement in the doctor–patient relationship (Baptist et al., 2011; Roter et al., 2008).
Since changes introduced by digital health technologies have primarily been analysed from preventive care and health promotion perspectives that often adopt a ‘techno-utopian’ lens, Lupton (2013) argues that it is imperative to also examine such changes from a critical perspective (p. 257). Specifically, Lupton (2013) emphasizes the need for examining how digital technologies operate to ‘construct various forms of subjectivities and embodiments and participate in the configuring and reproduction of power relations’ (p. 257).
Lupton (2013) uses the term ‘digitally engaged’ patient to refer to the highly proactive and participative patient who uses digital devices to track various health parameters. While advocates of digital health technologies highlight how self-tracking apps facilitate day-to-day management of health and medical decision-making, critics draw attention to concerns about loss of autonomy and control. In such a context, Sharon (2017) emphasizes the need to link our understanding of the role of self-tracking apps in health and lifestyle management to the experiences of not just those who voluntarily use them but also to the observations of those who stop using them after some time, perspectives of those who do not have the means or the technological fluency to use them and those who refuse to use them.
To understand the deep impacts of digital health technologies on people, it is important to understand the far-reaching changes in meanings and subjectivities associated with their usage. For example, in a study on self-management of pregnancy and social media platforms, Johnson (2014) observed:
apps format motherhood and pregnancy in a new way, instituting new rules into new devices and offering templates which actively shape meanings and practices....They create new social relations and valuing practices, such as ‘likeability’ on Facebook, which have the potential to alter our understandings of health and identity. (p. 346)
As people begin to self-manage various aspects of their health and lives, it is important to explore their assumptions and perspectives in this regard. The following section offers a brief account of the theoretical underpinnings of this study.
THEORETICAL FRAMEWORK: NEOLIBERAL GOVERNMENTALITY AND HEALTHCARE
Operating within a constructivist grounded theory framework, later grounded theory proponents (Charmaz, 2006; Dey, 1999; Kelle, 2007; Lempert, 2007; Thornberg, 2012) acknowledge the influence of existing theories on a study. As Thornberg, in his oft-cited article on ‘Informed Grounded Theory’ argues: ‘Empirical observations could never be totally free from theoretical influence because seeing is already a “theory-laden” undertaking’ (p. 246). In keeping with the fact that constructivist grounded theorists ‘advocate recognizing prior knowledge and theoretical preconceptions’ (Charmaz, 2008, p. 402), this study draws upon neoliberal governmentality as a theoretical anchor to understand the practices of the participants of the study.
While the omnipresence of market rationality in all aspects of life is considered a critical aspect of neoliberalism, ‘actually existing neoliberalism’ in different countries defies uniformity and assumes different permutations and combinations (Brenner & Theodore, 2002). Advocating a view of neoliberalism as a ‘discourse’ that takes into account both its Marxian roots and Foucauldian post-structuralist leanings, Simon Springer (2012) categorizes neoliberalism ‘as a mutable, inconsistent, and variegated process’ (p. 135). Since neoliberalism involves contradictory and diverse processes, examining various aspects of people’s lived experiences can be highly illuminating. In the Indian context, the self-regulated individual striving towards self-development forms an integral aspect of the ubiquitous ‘enterprise culture’ prevalent in the country today (Gooptu, 2013).
The concept of ‘governmentality’, which was originally formulated by French philosopher Michel Foucault, combines the two terms ‘government’ and ‘rationality’ (Huff, 2020). It refers to the way people willingly engage in their own ‘self-governance’. Several scholars (Crawford, 2006; Lupton, 1995; Petersen, 1996; Rose, 2001) have highlighted the relationship between Foucault’s works on power, discipline, and governmentality, on the one hand, and that of neoliberal health practices characterized by ‘self-governance’, on the other (Pond et al., 2010, p. 735).
Nike Ayo (2012) argues that the concept of governmentality helps to demonstrate the way health promotion works. Instead of focusing on ‘social and structural changes which impede upon the health and wellbeing of the population’, it incites ‘the desire within autonomous individuals to choose to follow the imperatives set out by health promoting agencies, and thus, take on the responsibility of changing their own behaviours accordingly’ (p. 100). The imperatives of neoliberal governmentality require citizens to be proactive and responsible for their health. It is viewed as an individual project to be run with little state assistance. Specifically commenting on how social media platforms and apps introduce new dimensions of self-care, Johnson (2014) states:
Digital health technologies are largely consistent with preceding modes of neoliberal governmentality, but their most significant feature is that they extend these modes of responsibilization into new spaces and practices and forms of calculation (p. 334).
As new aspects of self-care emerge, it becomes important to identify contemporary understandings of health that inform such practices. Drawing upon the above contextual background and existing literature, this study will explore the following research questions:
RQ1: Why do Indian men and women connect with physicians on Facebook?
RQ2: What is the nature of communication between people who follow physicians on Facebook and their physicians?
RQ3: What does ‘health’ mean to individuals connected with physicians on Facebook? What measures do they take to keep healthy?
METHODS
This study comprises the second part of a larger project on Facebook usage in the healthcare sector in India. Findings of the first study based on interviews with physicians connected with patients on Facebook showed that physicians were using the platform to communicate their brand and spread health awareness, especially after tailoring the messages to the socio-cultural context of their audience (Mishra, 2018). The current study explores the other side of the issue by analysing the perspectives of people who choose to connect with physicians on Facebook.
In-depth interviews of 30 men and women who are connected with physicians on Facebook were conducted between September 2018 and December 2019. Snowball sampling was used to identify participants for this study. Initially, the researcher attempted to identify people who were either ‘friends’ with physicians on Facebook and/or ‘followed’ their Facebook pages in the Facebook networks of physicians after taking their permission. The author had gained access to several physician Facebook profiles and pages during her first study (Mishra, 2018). However, contacting people on Facebook for interviews did not yield good results due to poor responses and difficulty verifying the identity of participants. Then the author used her offline networks and inquired about people who were either ‘friends’ with a physician on Facebook or ‘followed’ their Facebook page. Soon, one referral led to another and interview dates were set up. Consent was obtained from the participants before the interviews.
While several interviews were conducted face to face, many were also conducted over the telephone as the respondents live in various parts of India, including New Delhi, Kolkata, Bangalore, Pune, Bhubaneswar, Jaipur, and Ahmedabad. Here it may be pointed out that telephone interviews facilitate interviewing participants from diverse geographical locations and gives them the opportunity to talk from the comfort of their surroundings (Novick, 2008). The interviews followed a semi-structured format, and the average duration of the interviews was around 35 minutes. The interview guide included questions on motives for connecting with a physician on Facebook, the nature of communication with the physician on Facebook, the meaning of health for them and what, if any, measures they took to maintain their health. While some interviews were completed in one session, a few others led to follow-up sessions.
There were 20 women and 10 men in the sample. The majority of the participants (18) were in the age group 26–35, while 9 were in the age group of 36–45. The fact that the majority of participants were relatively young may be explained by the fact that more than 70% of Facebook users in India belong to the 18–34 age group. Additionally, one of the reasons for the predominance of women in the sample (even though more than 75% of Facebook users in India are men) may be traced to the gendered societal expectations that place the responsibility of maintaining the health of the entire family on women. The method of snowball sampling may have also contributed to it. It may also be pointed out that a Pew Research Center study (Fox, 2011) in the United States found that women (86%) are more likely than men (73%) to pursue health information online, although corresponding data for India is not yet available.
Further, all the participants in this sample were highly educated, including 19 with master’s degrees and above, 9 with bachelor’s degrees and 2 with high school degrees. The sample comprised IT professionals, media professionals, academicians, businessmen, a chartered accountant, a retired civil servant, and homemakers. The majority of the participants reported an annual household income of INR 10 lakhs and above. All the participants have been given pseudonyms to protect their identities.
The interview techniques and the subsequent analysis of the data followed elements of Charmaz’s (2014) constructivist grounded theory framework. The study followed an iterative approach whereby data collection and analysis were conducted simultaneously by the author. The data were analysed following the constant comparative method (Charmaz, 2014). After initial coding, preliminary themes were ascertained, following which similar themes were grouped. Initial coding was followed by ‘focused coding’, which requires selecting those initial codes that ‘make the most analytic sense’ to categorize data (Charmaz, 2014, p. 138). At this stage, the theoretical and conceptual relevance of the selected codes was examined with the goal of facilitating analysis. Finally, the emergent patterns were conceptually explicated.
RESULTS
The interviews showed that three major categories of people are connected with doctors on Facebook: current and former patients, current and former caregivers, and healthy individuals who seek lifestyle and fitness information. The participants were connected on Facebook with primary caregivers and specialists, including gynaecologists, cardiologists, psychiatrists, endocrinologists, neurologists, nephrologists, and orthopaedics. The following themes emerged from an analysis of their motivations for connecting with doctors on Facebook.
Seeking ‘Credible’ Health Information for Individual Consumption and Sharing
An important motivation for connecting with doctors on Facebook was to get access to preventive healthcare information. Participants also pointed out that doctors do not usually give enough information about the prevention of diseases during face-to-face interactions. Such perspectives reveal a gap between the amount and nature of preventive healthcare information sought by some people and what is provided by physicians in face-to-face interactions in hospitals and clinics. Further, participants sought health information for their individual use and were also keen on ‘sharing’ such information with their online networks in social media spaces, thereby indicating that posting health awareness information on one’s online profile possibly helps them cast a better impression.
Many participants also believed that information posted by doctors on their Facebook pages and profiles was more credible than information discovered through queries on online search engines. They claimed that physicians were unlikely to post wrong information online as their professional reputation was at stake. Interestingly, participants also said Facebook pages and profiles of doctors were a good source of culture and religion-specific health information. For instance, Nafeesah, a 29-year-old online media professional in Delhi, narrated her experience on this issue:
The Nipah virus outbreak in India happened in 2018 during the month of Ramzan [Ramadan]. Muslims all over the world break their fasts with dates. But with the Nipah virus outbreak, people were scared of having dates in India. I remember this particular Muslim doctor on Facebook posted that there was no problem in having dates unless a bat has bitten into it. One could have also Googled the information but it was more authentic coming from him.
Nafeesah’s response highlights how individuals depend on medical practitioners for credible healthcare information, especially during a public health crisis considering the explosion of fake news during such times.
Offers an Opportunity to Consult Doctors Discretely about Diseases that Carry a Social Stigma
According to several participants, online consultations offer an opportunity to seek medical advice discretely, especially when the disease is stigmatized in Indian society. For instance, one of the participants, Ira, a 26-year-old school teacher in Kolkata, said she felt comfortable contacting a psychiatrist on Facebook about her ailment rather than meeting him at the hospital due to the stigma associated with mental health:
I was suffering from mild depression. But I could not get myself to tell him face to face in the OPD. Online, I could say things more easily because I did not have to look at him and speak. There’s so much stigma around depression. I feel online contact is a good first step in the case of mental health issues.
In a country such as India, where stigma against mental health issues is rampant, avenues that help people connect discretely with practitioners can prove to be a big advantage. Apart from mental health ailments, contagious diseases also carry a tremendous social stigma in India’s rural and urban areas, and online consultations can help protect people not only from ostracization but also help in containing the spread.
For Psychological Assurance, Personal Connect, and a Sense of Community
The study showed that participants connected with doctors on Facebook for psychological assurance and a sense of personal connect. For instance, Supriya, a young media professional who lost her father a year ago after he developed neurological and cardiological problems, said she ‘felt safe’ being connected with doctors on Facebook. In fact, she continues to gather information on neurological and cardiological ailments:
Even after you lose somebody, that curiosity is still there. You want to know how to prevent it…You re-live that time again and again. You wonder what could you have done differently. You need more details to support whatever you are thinking.
Participants also pointed out that connecting with a physician on Facebook helped to know the latter in a non-medical context, facilitating interaction in medical settings. They were able to keep in touch with the physician even after the medical crisis was over. Being connected to a particular physician on Facebook also gave them access to a network of physicians who they believed they could access in times of need.
Further, the process of seeking health information on Facebook also facilitated interaction with people who were facing similar health issues. For instance, Nupur, 28, a housewife in Kolkata, mentioned that connecting with a physician on Facebook gave patients and caregivers a sense of community:
I had 3 miscarriages and felt depressed all the time. When I started reading posts on my gynaecologist’s Facebook profile, I realized there were many women who managed to have children despite having several miscarriages. That motivated me. I did not give up, and I had a baby girl 5 months back.
After the birth of her daughter, Nupur continues to follow the Facebook posts of her gynaecologist. She also follows a nutritionist on Facebook and watches lifestyle videos posted by her. Such practices indicate that patients are often interested in maintaining some form of connect with their doctor even after the immediate need for it has ended, and social media spaces appear to meet that need well.
However, not all participants believed that connecting with a physician on Facebook helps establish a sense of personal connect. Aman, 23, a graphic designer in Ahmedabad, who follows a cardiologist for fitness and wellness information, was more critical: ‘When we are connected on Facebook, we feel that if we want, we can meet the doctor in the future as they will remember us from Facebook. The truth is it’s an imagined relationship just like we have with celebrities.’
It is possible that healthy individuals such as Aman, who primarily seek wellness information in a physician’s Facebook post, are less likely to look for a psychological connect with the physician than a patient or a caregiver who may be more eager.
Using the Information Posted on a Facebook Page/Profile to Select the Right Doctor
Participants claimed that the testimonials written by patients and caregivers on doctors’ Facebook pages and profiles served as a valuable source of information for those in the process of selecting a doctor. For instance, Sinu, a 32-year-old HR professional in Delhi, justified such an approach of choosing a doctor:
Do you buy anything these days or visit a restaurant without reading reviews online? Similarly, why would we visit a doctor without reading reviews about him and his work on the Internet?
Sinu’s remark highlights the transformation of the individual from a patient to a health consumer. Choosing a doctor based on information available on the Internet introduces additional complications. There always remains the possibility of blurring information between advertising material and health information published in the public interest (Dutta, 2015). Furthermore, since participants also used information available on a physician’s Facebook profile and Google reviews to determine whether he was well-versed with the latest technological developments, it introduces the risk of privileging a specific type of knowledge over other forms of medical expertise. Not every ailment may have a technology-centric solution. However, as Mills and Hilberg (2018) emphasize, health issues in India are often presented today as problems with technological solutions.
Technologically Connected but Rarely Interacted Individually with Physicians
Most of the respondents said they did not interact one on one with doctors on Facebook. Instead, their online activity was limited to liking, sharing, and occasionally commenting on the physicians’ posts. Interestingly, the participants did not express resentment against the physicians for the lack of individual interaction with them on Facebook and instead attributed it to the latter’s busy lifestyle. Furthermore, participants still believed that having access to health information posted by a physician on Facebook created the possibility of future offline interaction about that topic. For instance, 29-year-old Nafeesah said, ‘When a doctor posts something new on, say, heart disease, the patient will read it. He may not ask a question to the doctor on Facebook. But he might ask that question to the doctor during his next visit to the clinic.’
Participants also pointed out that whether a doctor interacted individually with his contacts on Facebook often depended on their field of specialization and their personality type. While a surgeon may not want any contact, a mental health professional might be open to interaction on Facebook as they might consider it important to spread awareness.
Making the Right Lifestyle Choices and Keeping Stress under Control
Most participants emphasized that health implied making the right lifestyle choices such as doing regular exercises, eating a balanced diet, and remaining updated with preventive health information. Overall, their understanding of health reflected the internalization of neoliberal rationalities. Finding ways for coping with stress emerged as an important concern amongst many participants. Meditation, counselling, positive thinking, listening to motivational talks on YouTube, and exercise were considered effective strategies to cope with stress. Overall, participants emphasized the importance of individual effort in controlling stress and anxiety.
Gooptu and Krishnan (2017) argue that while the rise of stress levels among people in India can be interpreted ‘in terms of the affective cultures of self-making that are emerging in the context of neo-liberal transformation in India,’ socio-economic inequalities that contribute to it are often ignored even as relief from stress is framed ‘as a matter of self-control and self-development’ (p. 406). Thus, the Indian government launched a ‘No More Tension’ app in 2016, which claims to calculate stress levels of individuals and helps them manage stress as well (National Health Portal, n.d.).
While most participants in this study highlighted the need to be positive, Anita, a 26-year-old resident of Kolkata, said she was trying to resist the pressure to remain positive all the time: ‘There’s so much false positivity all around...I don’t have the freedom to say I am feeling sad. There’s no such thing as facing one’s emotion and going through it anymore.’
In this context, Youll and Meekosha (2011) point out that ‘the ideology of positive thinking reflects broader neo-liberal, capitalist culture and is therefore an example of “technologies of the self” through which individuals and populations self-regulate so as to preserve health and maintain demographic norms’ (p. 22). Moreover, ‘positive thinking’ can also have adverse consequences since it puts the responsibility of finding a solution or a cure on the individual: ‘This can be empowering if things go well, but it can also lead to a sense of failure or guilt if things do not go well’ (McGrath et al., 2006, p. 667).
Using Diagnostic Tests to Deal with Anxiety about Health
Many participants also expressed anxiety about their health and attempted to cope with it by getting regular diagnostic tests. For instance, 26-year-old Srijit from Kolkata expressed his anxiety in the following way:
I go for full body check-up just for the sake of it although everything is normal. I know a 33-year-old who used to be very fit but just had a kidney transplant recently. Both his kidneys failed. If he had done body check-ups twice a year, it could have been avoided. I want to do check-ups so that any disease can be caught early.
Participants believe the reason people are more anxious about their health today is because the level of threat from diseases has increased. Seema, a 30-year-old resident of Bhubaneswar, explained:
The problems we face today did not exist before. Cancer today has creeped into our homes. We did not hear of so many people dying of cancer before. If you are ill for 3-4 months continuously, the C-word automatically comes up in your thoughts. After a certain age, doctors advice you to first do an oncological checkup if you have any health problem. That is why we are all anxious about our health.
The excerpt as mentioned above from Seema’s interview, highlights the increasing anxiety and concern people feel about their health and their need to control it. Cossman (2013) pointed out that ‘anxiety governance’ which involves ‘taking action and self-governing to alleviate one’s anxiety’ is pervasive amongst neoliberal subjects (p. 900). Anxiety about one’s health creates the desire to follow medical advice as an everyday practice. In the process, anxiety becomes a ‘technique of governance’ or a via media for the regulation of conduct (Cossman, 2013, p. 915). Further, the market also plays a role in facilitating ‘anxiety governance’ as people today can avail discount packages on diagnostic tests, get their samples collected from home, and get the test results delivered to their email accounts. However, it must be pointed out that despite the overdependence on diagnostic tests, a few participants also resisted the neoliberal belief that one’s health can be predicted and controlled by lifestyle choices and timely diagnostic tests alone.
DISCUSSION
The narratives of the participants in this study reflect the internalization of neoliberal subjectivities and healthcare practices. The participants follow the neoliberal practice of getting access to available online sources of health and lifestyle information from the physicians’ Facebook profiles and pages and adopting some of the espoused practices. Remaining connected with physicians, conducting regular diagnostic tests, and listening to speakers on positive thinking and ways to control stress also helped them manage health-related risks in a neoliberal society where the individual takes proactive steps to manage their health even as the state takes a backseat.
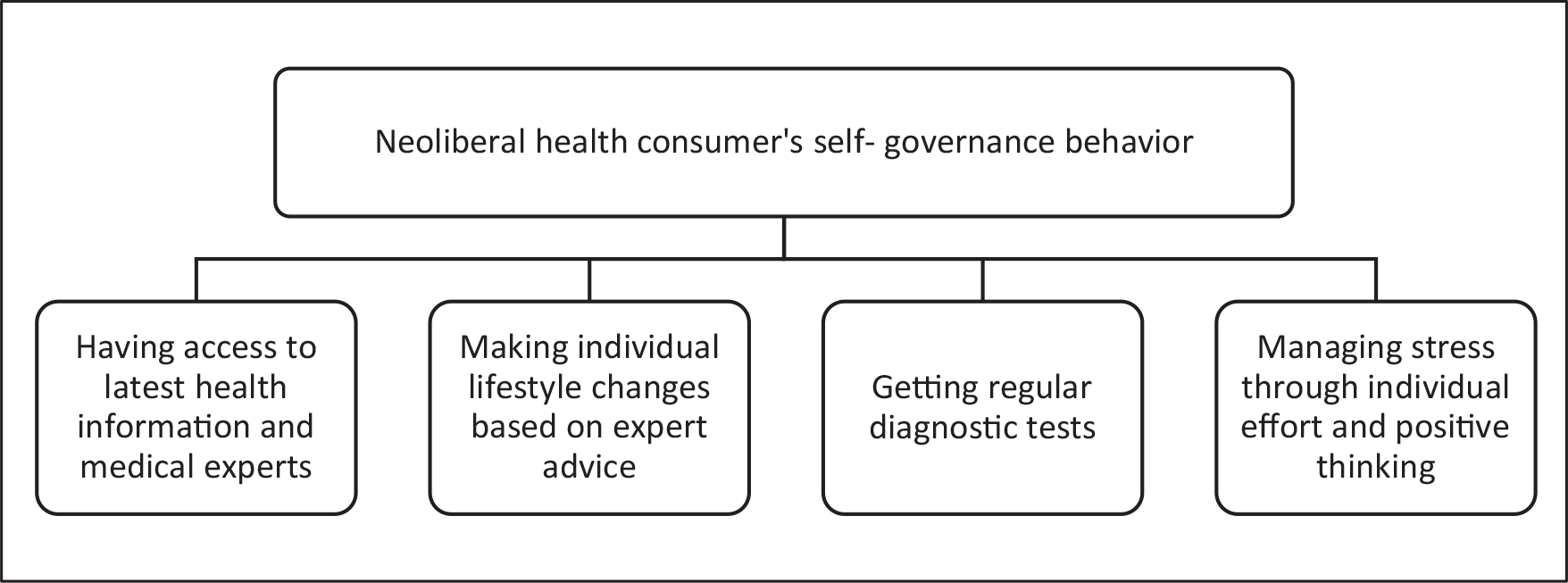
Foucault’s concept of governmentality, which refers to the consensual governance of one’s conduct, helps explain how the participants regulate their behaviour and ensure that they exhibit neoliberal values and norms as a part of their everyday lived experience. Viewing health as an aspect of life that can be controlled at the individual level, the participants took proactive measures to stay informed and ensure that they were healthy and safe. Using the theoretical lens of neoliberal governmentality, this study sought to understand the self-reported behaviours of socio-economically privileged Indians who connect with medical practitioners on Facebook (see Figure 1).
Neoliberal Health Practices and Foucauldian Self-Governance.
In a related study of urban, upper-middle-class Indian women’s dieting practices, Jaita Talukdar (2014) argues that both neoliberal values and biotechnological knowledge are popular among the urban elite in India and ‘induce an inward gaze, in a Foucaultian sense, that aims to detect and improve upon the functioning of the minutest part of the human body’ (p. 143). Meanwhile, Johnson’s study on the usage of pregnancy apps showed how ‘apps format motherhood’ in new ways and highlight the development of neoliberal subjectivities. Similarly, this study shows how neoliberal assumptions are associated with the usage of specific health-management apps and a search for medical advice in everyday digital spaces such as Facebook.
Of course, the purpose of this article is not to dismiss the social media affordances highlighted by the participants but to explore how neoliberal rationalities render it commonsensical for some men and women in urban India to connect with physicians on Facebook. Connecting with physicians on Facebook is a unique development since the platform has not been traditionally associated with patients, caregivers, and ordinary citizens seeking medical information. However, the need to access health information posted by medical experts on any online platform, including Facebook, seems to draw upon the neoliberal belief that healthy individuals and not just patients should adopt expert medical advice to live an optimal life (Sugarman, 2015). Additionally, this study showed that most participants found health-related information posted on the Facebook profile of a doctor more reliable, personalized, and culture-specific than the results of a generic online search.
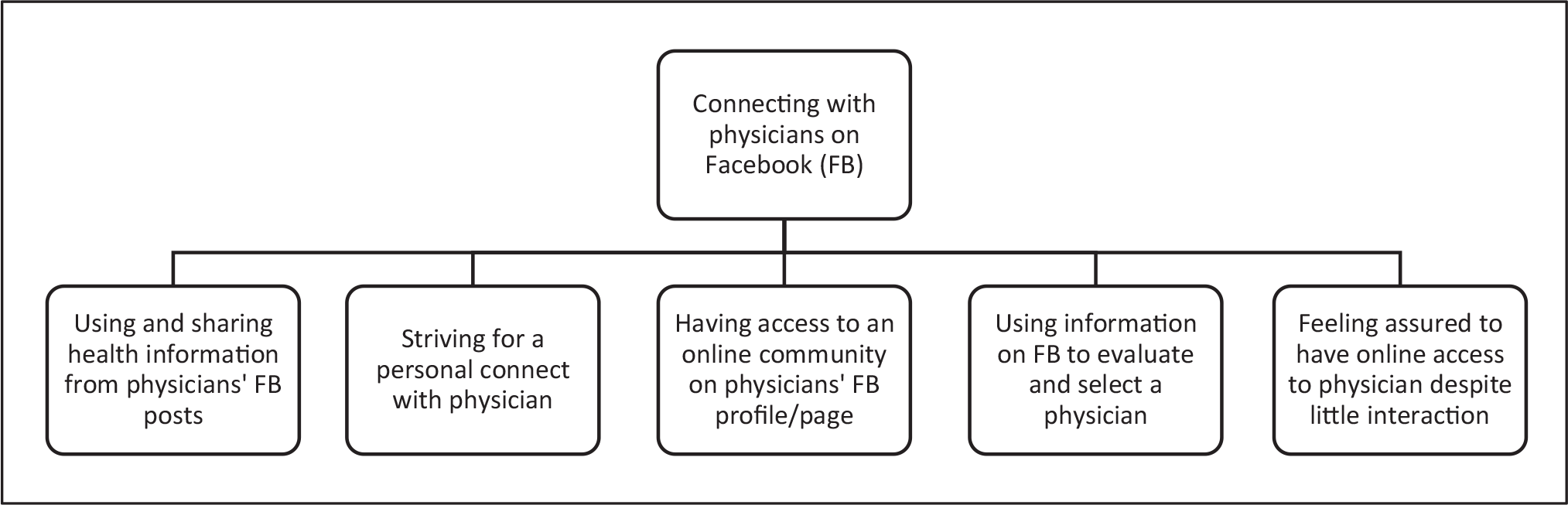
Interestingly, despite the limited nature of communication between participants and physicians on Facebook, many said they felt relieved to have online access to a physician (see Figure 1 for the web of neoliberal health practices adopted by the participants). Many participants also claimed to benefit from becoming a part of the online communities formed on the Facebook profiles and pages of physicians. It helped them connect with others with similar health issues and gain from their experiences (see Figure 2). These findings resonate with the principles of the self-verification theory, which claim that people usually seek suggestions from those with similar beliefs and experiences (Swann & Read, 1981; as cited in Sillence et al., 2007).
Participant Perspectives on Connecting with Physicians on Facebook.
However, being connected with physicians on social media platforms such as Facebook carries several implications. First, it introduces medical advice into everyday digital spaces and practices. Referring to the impact of digital health technologies on people’s lives, Lupton (2013) argues that the ‘clinic and the normalizing and assessing gaze of healthcare providers are incorporated into the everyday domestic spaces and practices of the lay person via these technologies’ (p. 261). Furthermore, to borrow a term from governmentality scholars, Rose and Novas (2005), all these developments facilitate the construction of ‘biological citizens’ who have heightened awareness about their own health based on exposure to expert medical knowledge (pp. 445–446). According to Rose (1996), such neoliberal health practices also sustain entire bodies of knowledge and expertise systems:
In the name of social and personal wellbeing, a complex apparatus of health and therapeutics has been assembled, concerned with the management of the individual and social body as a vital national resource, and the management of ‘problems of living’, made up of techniques of advice and guidance, medics, clinics, guides and counsellors. (Rose, 1996, p. 37)
This study also showed that many participants relied on regular diagnostic testing to alleviate health-related anxieties. Here, it may be pointed out that risk operates as a ‘neoliberal tool, a technology of government’ that warns citizens of possible harm, thus ‘stimulating a sense of panic, a sense of urgency, and a sense that action must be taken now’ (Ayo, 2012, p. 103). Furthermore, a neoliberal orientation towards healthcare positions ‘laypeople as ready and willing to actively engage in their own healthcare and promote their own health, in the attempt to shift the burden of such responsibilities from the state to the individual’ (Lupton, 2013, p. 266).
Participants’ understandings of health also revealed the importance they gave to individual lifestyle choices. While this study does not discount the advantages of following healthy lifestyle practices such as exercise and diet, it highlights how neoliberal subjectivities may prioritize individual lifestyle choices based on advice from physicians over other social determinants of health and indigenous forms of knowledge. More importantly, such a lifestyle approach to health obfuscates socio-economic and structural factors contributing to illness and privileges status quo over interventions at a macro level (Dutta & Zoller, 2008; Zoller, 2008).
Another implication of people connecting with physicians on Facebook is the potential for creation of new forms of digital divide as those from socio-economically disadvantaged sections of society are unlikely to have the socio-cultural capital to gain access to the Facebook profiles of physicians. While anyone can follow a physician’s Facebook page as it does not require prior permission of the account holder, it is unlikely that people from disadvantaged backgrounds will be able to leverage it. In fact, a study on perspectives of physicians in India who are connected with their patients on Facebook showed that many physicians with Facebook profiles accepted ‘friend’ requests only from patients they considered ‘safe’ to communicate with (Mishra, 2018). Overall, by making health an individual enterprise, participants reinforced ‘the privatization of the struggle for generalized wellbeing’ (Crawford, 1980, p. 365).
Finally, it must be mentioned that this study has several limitations, which introduce avenues for future research. Since the study uses a non-probability sample, generalizations cannot be drawn across large populations. This limitation also makes it difficult to ascertain the influence of variables such as age and gender on a person’s decision to follow a physician on Facebook and other social media platforms. Future studies may address these pertinent questions through large-scale quantitative studies. Future studies could also explore if the meanings of ‘health’ change during major epidemics. For instance, do people continue to believe that health is an individual-lifestyle-choices project during a pandemic? Or do their views change, taking into account the role of the state during a public health crisis?
CONCLUSION
To conclude, this study provides insights into how social media platforms such as Facebook serve as a site of neoliberal governmentality as they facilitate regulation of individual conduct related to healthcare. Specifically, this study showed that men and women in urban India who send ‘friend’ requests to physicians or ‘follow’ their Facebook pages primarily seek health information for individual consumption or sharing with their online network. The participants’ need to locate healthcare information in everyday digital spaces possibly emerges from their understanding of health as primarily about making the right lifestyle choices. The participants also believed that healthcare information found on the Facebook account of a physician would be more reliable and culture-specific than the results of a generic online search. Moreover, they also used the information available on physicians’ Facebook accounts along with Google reviews for selecting physicians.
Such findings imply the critical need for a policy regulating the medical content available in social media spaces. Furthermore, a view of ‘health’ as an individual enterprise with little consideration of socio-economic and structural factors may render people more vulnerable to commercial information presented online as unbiased preventive healthcare information posted in the public interest. Finally, although the participants said they rarely interacted individually with physicians on Facebook, the practice of connecting with them in social media spaces presents a slippery slope in terms of privacy and other medico-legal issues. Policymakers, medical practitioners, and hospital management need to pay attention to such complexities associated with the usage of social media platforms in healthcare, especially in a society in the throes of large-scale digitization. More importantly, some of the issues raised by the participants of the study such as the dependence on medical practitioners for credible health information during disease outbreaks when fake news abounds, the need to consult doctors discretely about a disease that carries social stigma, and the need for psychological assurance from doctors during a crisis hold special relevance for policymakers engaged in managing a public health crisis such as the current COVID-19 pandemic and its aftermath.
Footnotes
DECLARATION OF CONFLICTING INTERESTS
FUNDING
Data collection for this article was supported by an internal grant provided by the Indian Institute of Management Calcutta during the author’s tenure there.