
Abstract
Music performance anxiety (MPA) affects young musicians, and especially those in higher music education, due to the evaluation and performance demands of this context and their professional and personal expectations, with implications for health and wellbeing. This study investigates the following predictors of anxiety: gender, age, performance experience, health problems, coping strategies and medication use, among Portuguese higher education music students. The Portuguese Music Performance Anxiety Scale (PoMPAS) was used to collect data (N = 414). A Student’s t-test for independent samples was used to assess the extent to which MPA levels differ according to gender, and multiple linear regression was conducted to evaluate how age, performance experience, health problems, coping strategies and medication use influence the MPA levels of the sample. The results show that female participants display higher MPA scores than males. To varying degrees, all the factors above significantly impact participants’ MPA levels, as evaluated by the scale’s Behavioural/Emotional, Contextual/Physiological and Cognitive elements. The results of this study suggest that preventive orientation and health programmes could promote the wellbeing, and, consequently, decrease the MPA levels, of this group.
Fear, tension, panic, negative thoughts, shaky legs, trembling voice, altered breathing, stomach pain, rapid heartbeat, sweating, technical failures, nervousness, lack of strength and muscle control are some of the symptoms of music performance anxiety (MPA) that are commonly reported by musicians. MPA is generally understood as a psychophysiological manifestation that includes a range of cognitive, behavioural and physiological responses (Kenny, 2011) that lead to a sense of lack of control (Barlow, 2000) before, during or after a performance. These manifestations have a significant impact on musical performance, affect health and wellbeing and can even lead to a career break (L. S. Araújo et al., 2017; Barros et al., 2022; Orejudo et al., 2018). Moreover, MPA affects the abilities of instrumentalists (musicians/singers) regardless of aptitude, training, career stage – amateur, professional or student – and musical preparation (Salmon, 1990).
Studies on MPA in the context of higher music education (the focus of this research) are still insufficient to address all the anxiety predictors involved, such as gender, age, performance experience, health problems, coping strategies, flow state, situational factors, social perceptions, individual variables and others, as mentioned in the systematic review by Barros et al. (2022).
In order to obtain specific knowledge about predictors of MPA that affect higher education music students, the aims of this research are: (1) to investigate the extent to which the levels of MPA differ between male and female students in the Portuguese higher education context; and (2) to assess the extent to which the predictor variables of age, performance experience, health problems, coping strategies for anxiety and use of anxiety medication on the MPA levels of this population.
The following topics will expose a brief state of the art regarding the MPA predictors addressed in this research.
Gender
Regarding gender, most studies show that female university students present significantly higher levels of MPA than male students (Coşkun-Şentürk & Çırakoğlu, 2017; Dias, Veríssimo, et al., 2022; Dobos et al., 2019; Iusca & Dafinoiu, 2012; Orejudo et al., 2017; Sulun et al., 2017; Yondem, 2007), and that female music students display higher levels of trait anxiety (Barros et al., 2019), trait anxiety and total anxiety (Umuzdaş et al., 2019), and negative feelings related to MPA (Studer, Danuser, et al., 2011). Additionally, studies have also reported more worry and disturbing thoughts (Oudejans et al., 2016) and significantly higher levels of stress, helpless approach, submissive approach, guilt and shame (Coşkun-Şentürk & Çırakoğlu, 2017) among women. Contrarily, in the research of Otacıoğlu (2016), male students demonstrated higher levels of MPA than female students, and Paliaukiene et al. (2018) and Robson and Kenny (2017) found no significant differences in MPA levels between females and males.
Among the aforementioned studies pointing out that women experience greater anxiety, Coşkun-Şentürk and Çırakoğlu (2017) state that women are more exposed to gender discrimination in society and that this may contribute to higher levels of MPA, while Iusca and Dafinoiu (2012) argue that teachers should use different teaching approaches (but do not mention which), as MPA is experienced differently between genders. For Yondem (2007), biological, psychological and cultural factors may influence female students’ experience of MPA, making them a high-risk group that needs help.
Performance experience and age
With regard to performance experience and age, studies suggest that the number of years of musical training may influence MPA levels: the more years of musical experience, the lower the MPA. According to Hamann (1982), years of study or performance experience have a positive effect on MPA levels and the quality of performance in the presence of a judging panel. Other studies are consistent with this perspective; for example, Steptoe and Fidler (1987) negatively correlated stage fright with age and performance experience (the greater the age and experience, the lower the stage fright). Similarly, Paliaukiene et al. (2018) associated high levels of MPA with less performance experience, and Kenny et al. (2011) correlated performance experience with significantly lower levels of MPA.
In relation to age, according to Zarza et al. (2018) and Kirchner et al. (2008), the age at which one begins to learn the instrument is linked to anxiety levels, as students who begin their studies earlier have fewer anxiety symptoms. However, for Cox and Kenardy (1993), performance experience did not determine anxiety levels.
To reduce early-career MPA levels, the findings of Kenny et al. (2011) indicate that frequent public performances and playing in front of peers (since the environment in which these performances occur is friendly) help music students get used to performance situations. Hamann (1982) suggests that formalised instruction is needed for musicians experiencing MPA but does not specify how.
Health problems
Existing research has addressed the quest to improve the health and wellbeing of music students in higher education. According to Spahn et al. (2014), students show a low capacity to cope with health problems. L. S. Araújo et al. (2017) reinforce this statement pointing out that music students have potentially worrying perceptions, attitudes and behaviours in relation to health and wellbeing.
The physical and mental effort required for the daily practice of instrumentalists/singers may exacerbate these issues. In addition, the excessive practice effort can lead to various types of musculoskeletal injuries, such as muscle, tendon and shoulder pain, resulting from excessive practice and repetitive movements. Thus, the damage is likely to remain throughout the professional career.
In a study by Sousa et al. (2017), almost two-thirds (62.5%) of the musicians interviewed from a professional orchestra in northern Portugal presented musculoskeletal problems related to their instrumental practice. According to Jääskeläinen et al. (2020), excessive instrumental practice is the strongest predictor of stress among university students, suggesting high levels of MPA.
Considering the need to improve health and wellbeing, Perkins et al. (2017) state that health promotion should be adopted in educational institutions’ daily practices and routines. In this sense, according to Ginsborg et al. (2009) and Kreutz et al. (2008), preventive health programmes for musicians in conservatoires and universities can improve the quality of musical performance, and students’ health and wellbeing. However, an understanding of the profiles of music students is needed to identify and prevent problems, including MPA.
Coping strategies for anxiety
Music teachers and students have widely used coping strategies (a set of skills used in adverse and stressful situations) to improve health and wellbeing indices and, consequently, reduce levels of MPA. According to Sinico (2013), the choice of strategy is closely related to the symptoms that each musician experiences; more than one strategy may be required to alleviate the sensations of MPA, and they do not always work. Recent research by Barros, Marinho et al. (2024) lists some of the most commonly used strategies: physical exercises, breathing exercises, conversations with positive reinforcement, technical preparation, recordings, mental simulation of performance (or mental rehearsals) and use of medication, among others. Similarly, research in higher education contexts mentions the following coping strategies: breathing exercises, relaxation techniques and instrumental practice (Zakaria et al., 2013), breathing techniques, self-control techniques, use of natural substances (mostly homoeopathic) and use of medication (Studer, Gomez, et al., 2011), deep breathing, positive thinking, muscle relaxation and medication (Liu, 2016). In Tahirbegi’s (2021) research, all students report using coping strategies to deal with MPA, including musical and technical preparation as the most used coping strategy to gain confidence and self-efficacy. In addition, they use strategies to manage both the physiological symptoms (e.g., tremors) and the cognitive aspects of learning and performing music.
Studies focussing on the Portuguese higher music education context are scarce, with no publications addressing the predictors of MPA and its impact on students at national level. Most studies focussing on MPA and professional musicians or music students in Portugal are unpublished master’s dissertations (Amorim, 2015; J. M. P. Araújo, 2013; Barros, 2018; Correia, 2012; Mendanha, 2014; Pinto, 2019; Pires, 2015; Quinta, 2014; Silva, 2022; Trigo, 2015), doctoral theses (Facchini, 2014; Tempera, 2018) and some journal articles (Barros et al., 2019; Dias, Batista, et al., 2022; Dias, Veríssimo, et al., 2022; Sousa et al., 2016, 2017; Zanon et al., 2016). Most of these studies were developed within music education, predominantly addressing case studies with limited sample sizes that do not comprehensively describe the Portuguese context.
Considering that MPA impacts young musicians during their studies due to the assessment and performance demands involved and their professional and personal expectations, problems arising from MPA throughout this period can significantly affect their health and wellbeing.
Method
Participants and sample characteristics
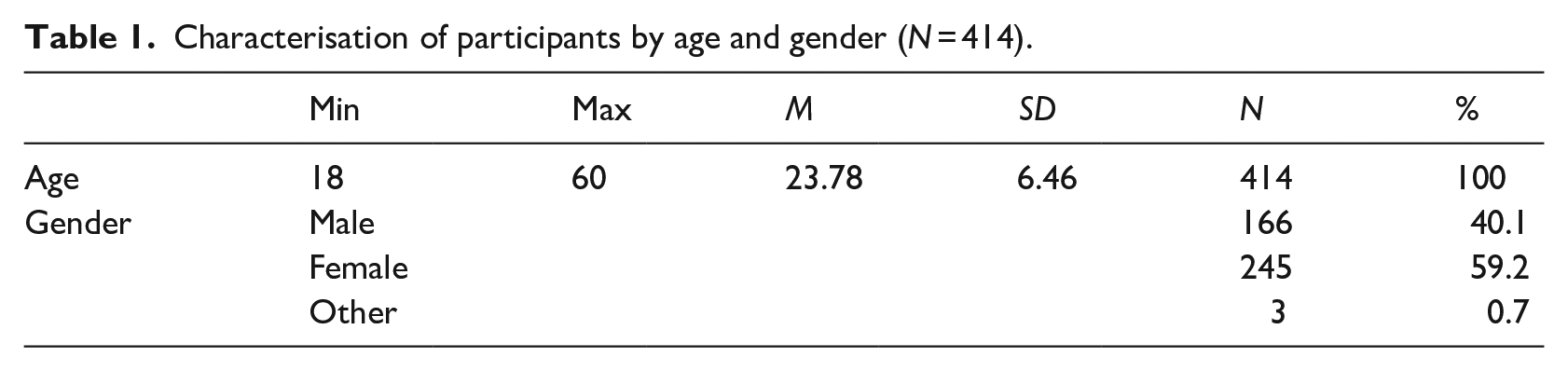
A total of 703 higher education students (bachelor, master and PhD levels) from public and private higher education institutions in Portugal participated in this study. However, only 414 (Table 1) provided complete answers to the questionnaire. Of this valid total, 166 identified themselves as male (40.1%) and 245 as female (59.2%); three did not wish to specify their gender (0.7%). The ages ranged from 18 to 60 years (M = 23.78; SD = 6.46).
Characterisation of participants by age and gender (N = 414).
Instruments
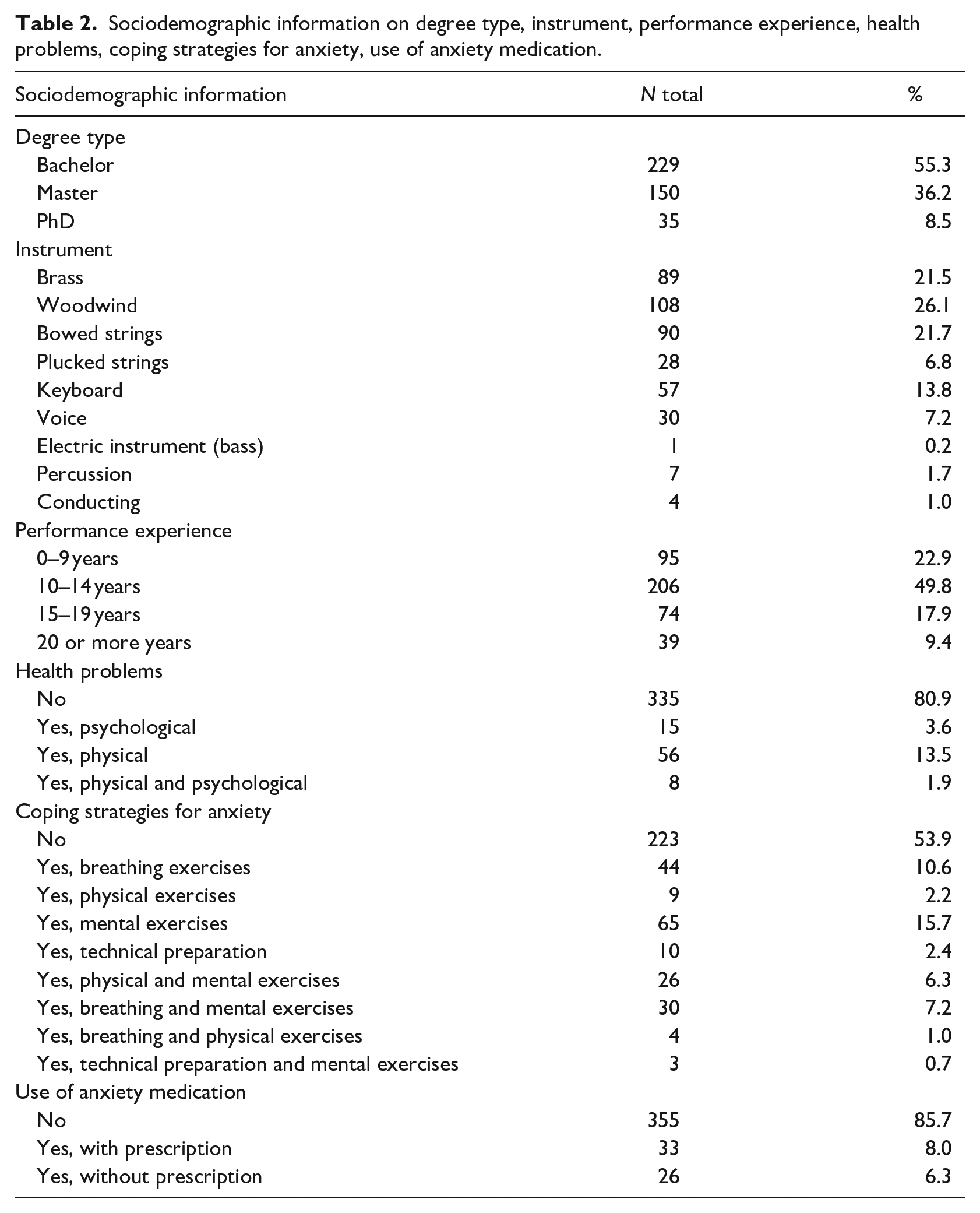
Data was collected from the participants using a sociodemographic questionnaire, mainly to obtain information about their degree type, instrument, performance experience, health problems, coping strategies and medication use for anxiety (Table 2).
Sociodemographic information on degree type, instrument, performance experience, health problems, coping strategies for anxiety, use of anxiety medication.
The Portuguese Music Performance Anxiety Scale (PoMPAS; Barros, França et al., 2024) applies a Likert scale with five response options, ranging from 1 (completely disagree) to 5 (completely agree). The scale comprises a total of 27 items and has been designed for higher music education in Portugal to understand, confirm and identify the global characteristics of Portuguese students’ MPA, experienced before and during the performance.
The PoMPAS is divided into three dimensions: Factor 1 – Behavioural/Emotional (F1 – BE) composed of 13 items (e.g. ‘Before a performance, I create expectations about how it will go’.); Factor 2 – Contextual/Physiological (F2 – CP) composed of 11 items (e.g. ‘The formalities of the performance context cause me anxiety’.) and Factor 3 – Cognitive (F3 – C) composed of 5 items (e. g. ‘During a performance, I feel sensations of threat or panic’.). It shows reliable internal consistency with good Cronbach’s alphas ranging between α = .81 and α = .90. Additionally, McDonald’s Omega also demonstrated good consistency, ranging between ω = .81 and .90. The values of the AVE (Average Variance Extracted) were adequate (Factor 1: 0.52; Factor 2: 0.52; Factor 3: 0.62).
Procedures
The sociodemographic questionnaire and scale were available online via the LimeSurvey interface at https://forms.ua.pt/ from December 2021 to September 2022 under ID 488167.
Participants were invited through institutional emails, personally by the first author of this study, and via social media, such as Instagram, Facebook and WhatsApp, to reach a broad and diverse number of participants and institutions.
The criteria for participation in this study were: (1) being enrolled in a higher education institution in Portugal, attending bachelor’s, master’s or doctoral courses and (2) answering all items of both questionnaires.
Ethical and deontological considerations
Research procedures were carefully selected and rigorously applied to ensure the ethical principles of respect for persons, beneficence and justice, based on the guidelines of the Declaration of Helsinki and Portuguese University Guidelines for Research. Furthermore, this research was conducted in compliance with the General Data Protection Regulation (GDPR) of the European Union and received approval from the Ethics and Deontology Board of the University of Aveiro (certificate 02-CED/2020).
No harm related to participating in the study was identified. Prior informed consent was obtained, and confidentiality and anonymity were assured.
Analysis procedures
A Student’s t-test for independent samples was performed to determine the extent to which PoMPAS scores differed between male and female participants. The assumption of homogeneity of variance was assessed using Levene’s test. Bootstrapping procedures were performed (1,000 resamples; 95% CI BCa) to correct deviations from the normality of the sample distribution (Field, 2018; Haukoos & Lewis, 2005). The effect size was calculated using Cohen’s d (d = 0.2, 0.5 and 0.8, corresponding to small, medium and large effects, respectively).
A multiple linear regression was performed to investigate the extent to which the predictor variables of age, performance experience (up to 9, 10–14, 15–19 and 20 years or more years), health problems (yes; no), coping strategies for anxiety (yes; no) and use of anxiety medication (yes; no) influenced the levels of Behavioural/Emotional, Contextual/Physiological, Cognitive factors and the total score of the PoMPAS. The predictors were entered into the regression model using the ‘enter’ method. This approach simultaneously includes all specified predictors in the model without any stepwise selection or exclusion.
The following hypotheses were tested: (1) independence of residuals (Durbin-Watson coefficient – between 1.5 and 2.5); (2) standardisation of residuals by Z-score (up to 5% of the sample with a standardised residual greater than 2) and (3) collinearity statistics (VIF – less than 2). Data was analysed using Jamovi statistical software (version 2.3.21).
Results
Independent samples Student’s t-tests were performed to determine how much the PoMPAS scores differed between the two groups (male and female). Tables 3 and 4 show the descriptive statistics of the subtests per group and Levene’s test, respectively. It should be noted that the gender category ‘other’ (Table 1) is not included in the results due to its low representativeness.
Descriptive statistics with the respective confidence intervals of the subtests per group.
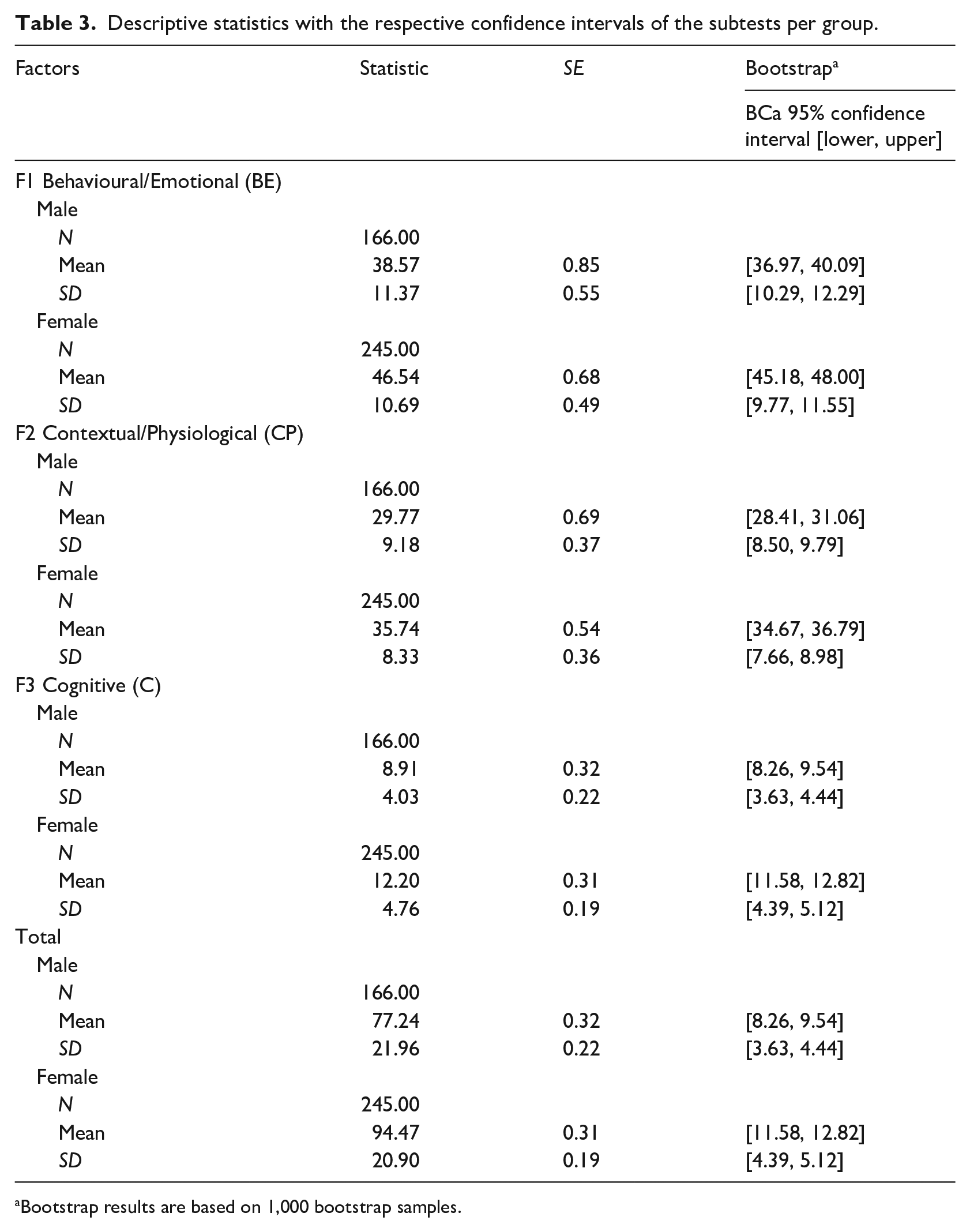
Bootstrap results are based on 1,000 bootstrap samples.
Levene’s test with independent samples.
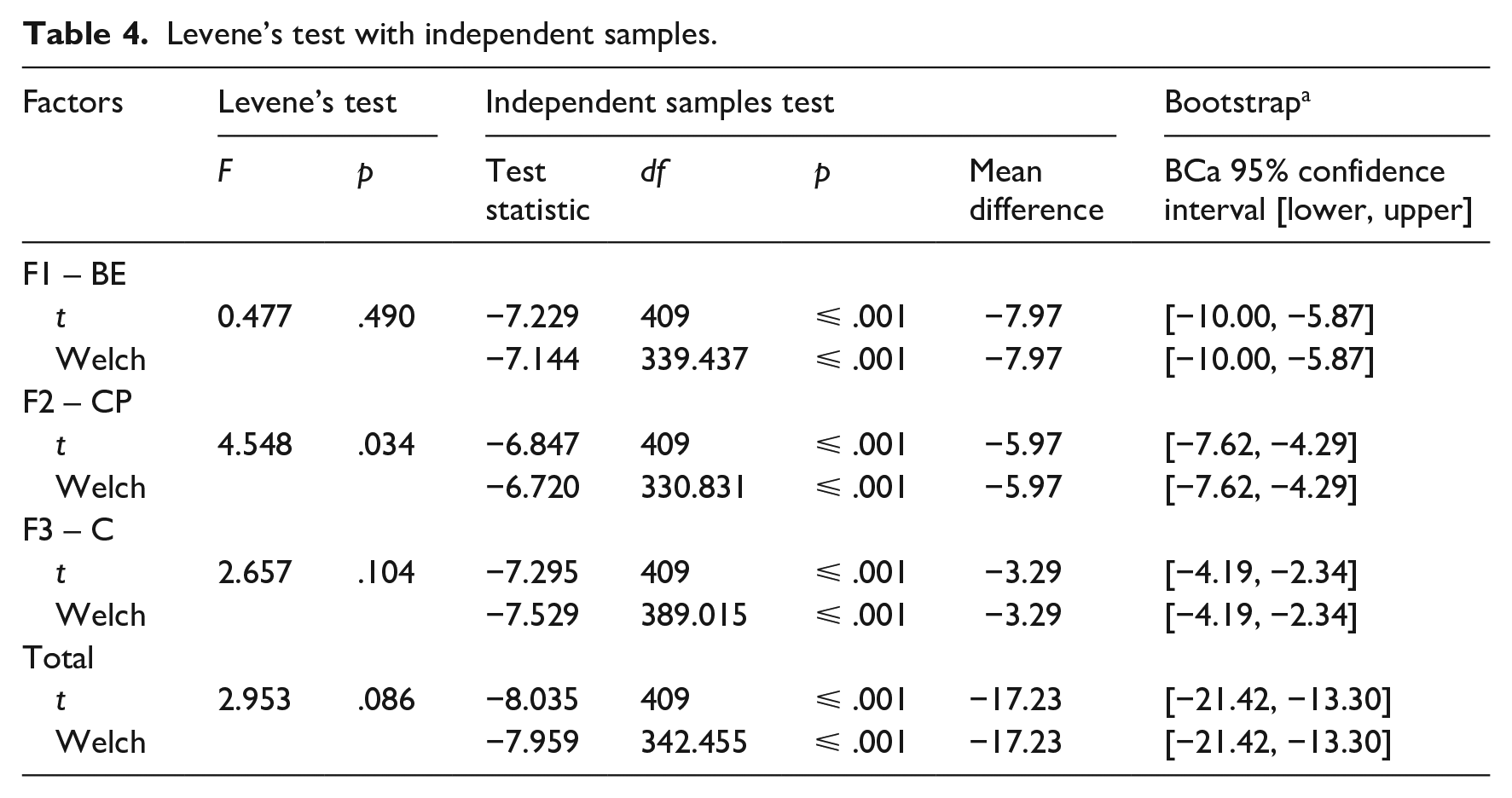
The results show that the assumption of homogeneity of variance was not met only for Factor 2. However, for the purposes of analysis, the results relevant to Welch’s statistics were used to ensure a more robust approach when testing groups (Delacre et al., 2017). Regarding the subtest of Factor 1 (Behavioural/Emotional), the results showed that males scored statistically lower (M = 38.57; SD = 11.37) than females (M = 46.54; SD = 10.69; t(339.437) = −7.144, p ⩽ .001). The effect size of the difference was medium (Cohen’s d = 0.73).
Results for the subtest of Factor 2 (Contextual/Physiological) showed that male participants scored statistically lower (M = 29.77; SD = 9.18) than female participants (M = 35.74; SD = 8.33; t(330.831) = −6.720, p ⩽ .001). The effect size of the difference was medium (Cohen’s d = 0.69).
For the subtest of Factor 3 (Cognitive), the results showed that male participants remained with a statistically lower score (M = 8.91; SD = 4.03) than the female participants (M = 12.20; SD = 4.76; t(389.015) = −7.529, p ⩽ .001). The effect size of the difference was medium (Cohen’s d = 0.73).
Finally, the subtest of the total factor (sum of factors 1, 2 and 3) showed a statistically significant difference between male (M = 77.24; SD = 21.96) and female (M = 94.47; SD = 20.90) participants (t(342.455) = −7.959, p ⩽ .001), with a large effect size of the difference (Cohen’s d = 0.80).
In the case of multiple linear regression, preliminary analyses were carried out to ensure that the assumptions of the test were not violated. The results showed that there was a significant influence of the predictor variables on MPA levels (Table 5).
Summary of the multiple linear regression analysis.
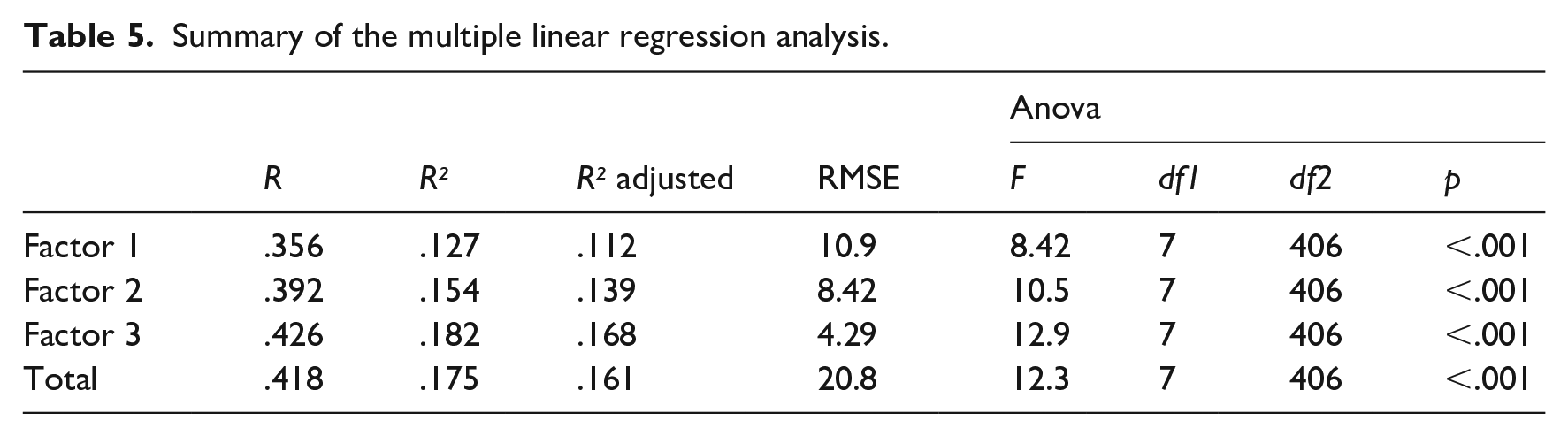
Considering the results (Table5), all factors (1, 2, 3 and the total factor) significantly predicted the outcome, with adjusted R² values indicating a moderate amount of explained variance. Tables 6, 7, 8 and 9 present the coefficients for all predictors.
Model coefficients – factor 1 – behavioural/emotional.
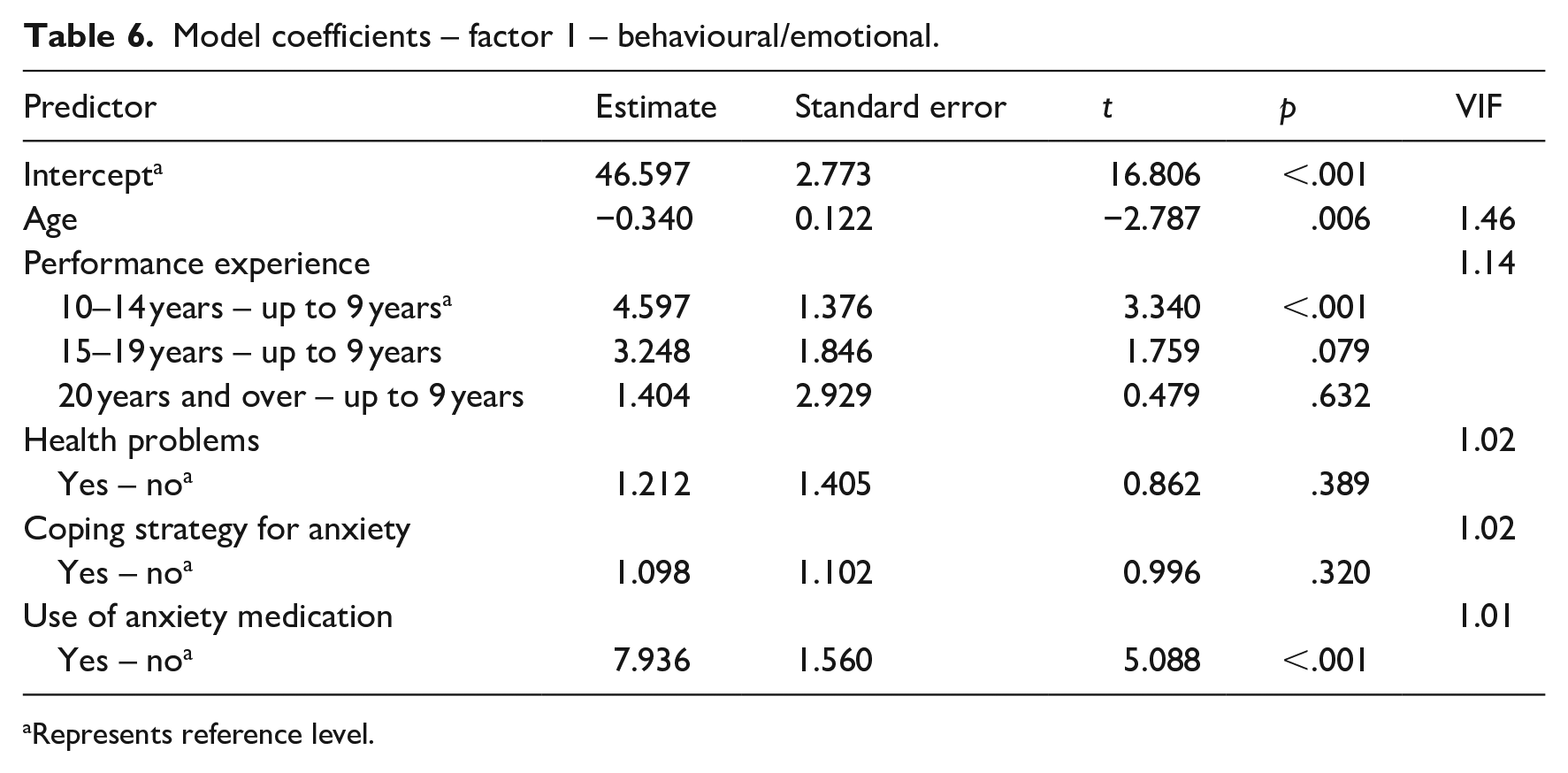
Represents reference level.
Model coefficients – factor 2 – contextual/physiological.
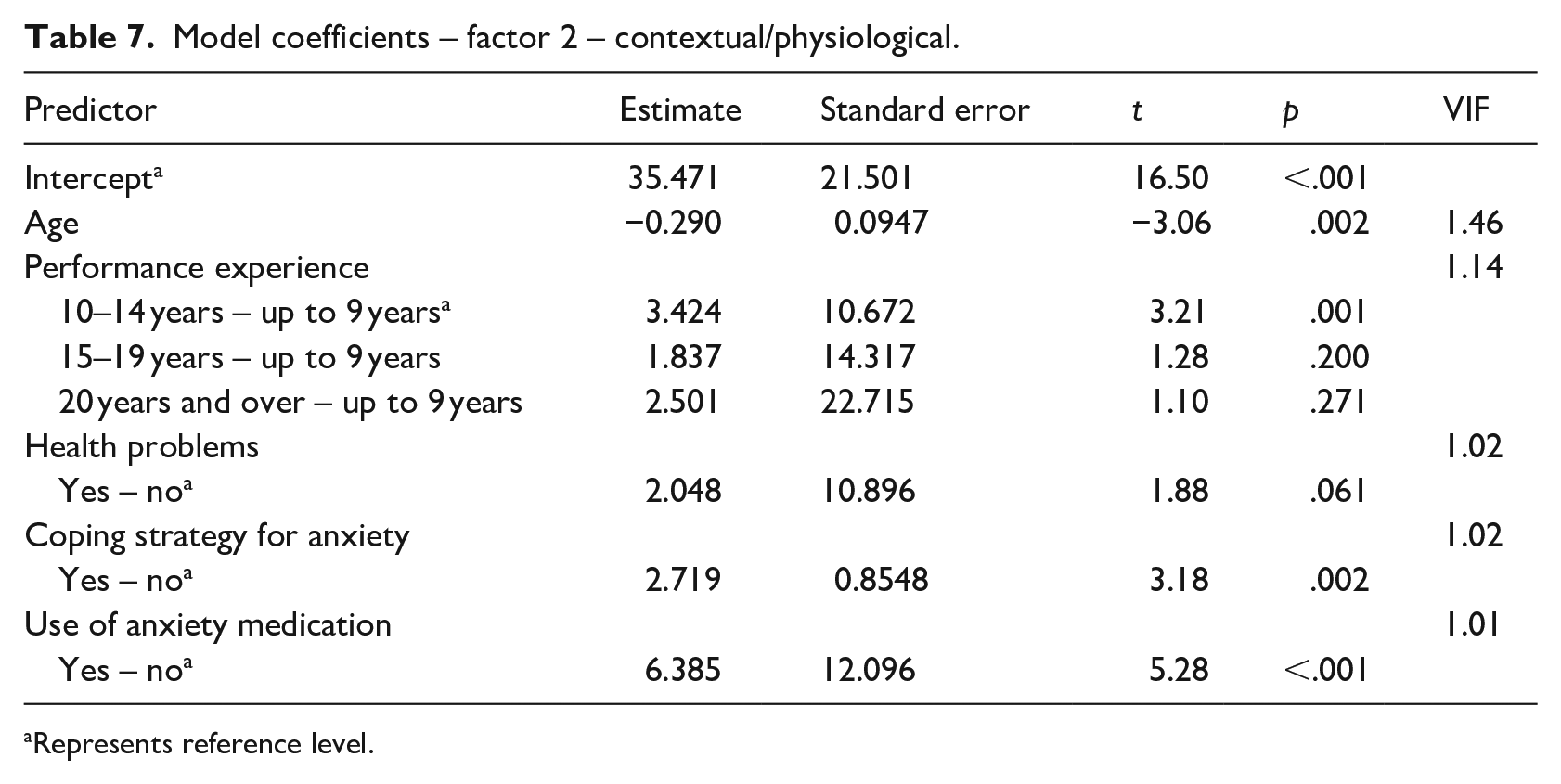
Represents reference level.
Model coefficients – factor 3 – cognitive.
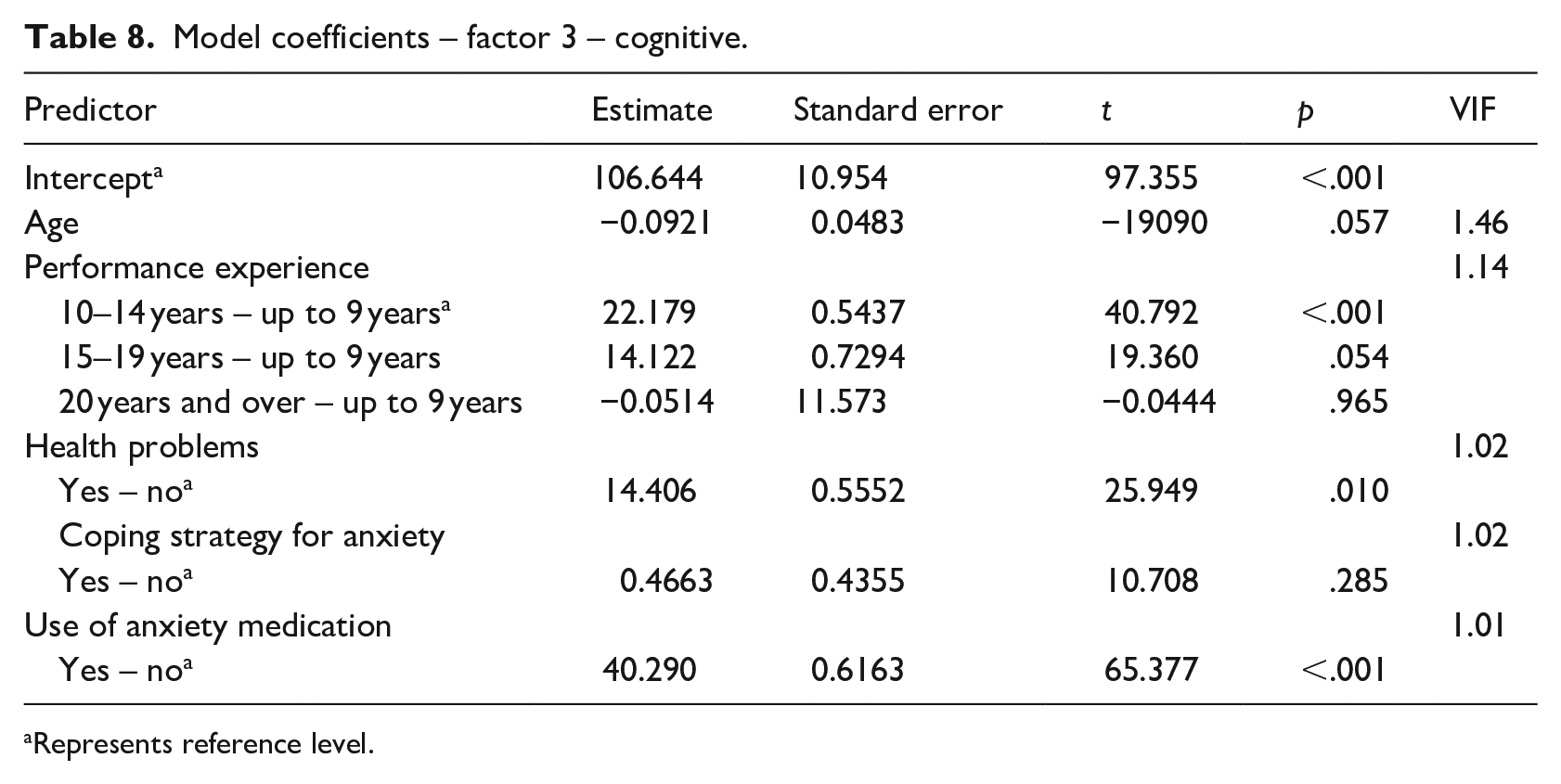
Represents reference level.
Model coefficients – total factor.
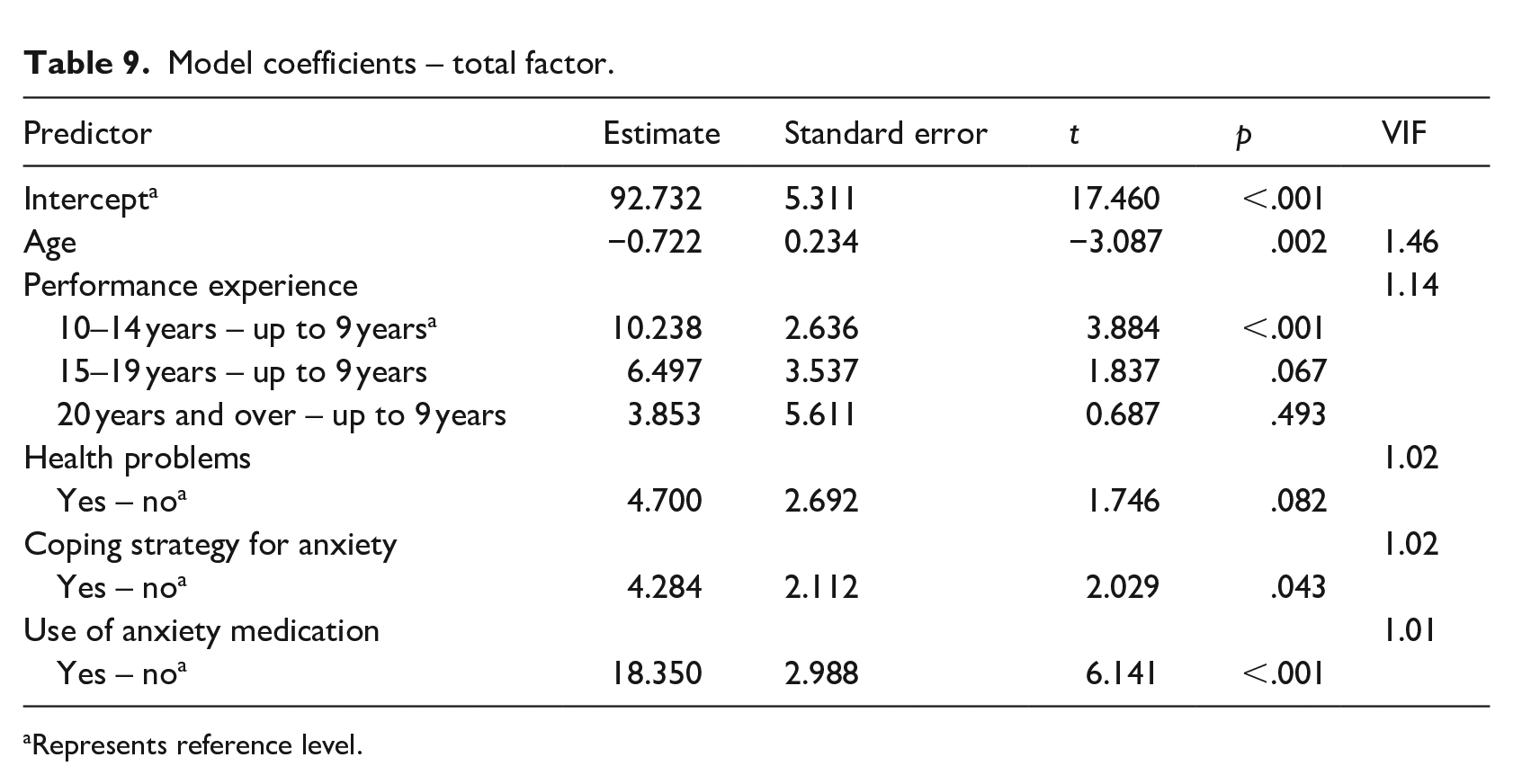
Represents reference level.
There are three statistically significant variables in the model. Age significantly affected the score of Factor 1 (β = -.340; p = .006). In terms of performance experience, changing the category ‘up to 9 years to 10 to 14 years’ had a significant effect on the score of Factor 1 (β = 4.597; p < .001). The use of anxiety medication significantly influenced the score of Factor 1 (β = 7.936; p < .001).
There are four statistically significant variables in the model. Age had a significant impact on the score of Factor 2 (β = -.290; p = .002). Regarding performance experience, changing the category ‘up to 9 years to 10 to 14 years’ impacted the score of Factor 2 (β = 3.424; p = .001). Concerning coping strategies for anxiety, the category change from ‘no to yes’ significantly affected the Factor 2 score (β = 2.719; p = .002). The use of anxiety medication significantly influenced the Factor 2 score (β = 6.385; p < .001).
There are three statistically significant variables in the model. The change in performance experience from the category ‘up to 9 years to 10 to 14 years’ has a substantial impact on the score of Factor 3 (β = 22.179; p < .001). Similarly, the shift from ‘no to yes’ in health problems has a significant effect on the score of Factor 3 (β = 14.406; p = .010). The use of anxiety medication significantly impacts Factor 3 (β = 40.290; p < .001).
There are four statistically significant variables in the model. Age shows a significant result on the total factor score (β = -.722; p = .002). In terms of performance experience, changing the category ‘up to 9 years to 10 to 14 years’ significantly affected the total factor score (β = 10.238; p < .001). Regarding coping strategies for anxiety, the category change from ‘no to yes’ significantly impacted the total factor score (β = 4.284; p = .043). The use of anxiety medication significantly influences the total factor score (β = 18.350; p < .001).
Discussion
Regarding gender, the results of this research showed that female participants displayed higher statistical MPA scores than male participants. The same was true for all three dimensions of the subscales (Behavioural/Emotional, Contextual/Physiological and Cognitive factors) and the total factor score of the PoMPAS. The results suggest that, in this study, women reported a greater impact of the symptoms and sensations associated with MPA, potentially influencing the quality of musical performance. Furthermore, this finding is in line with most of the previously mentioned research, which indicates that women experience higher MPA levels than men (Coşkun-Şentürk & Çırakoğlu, 2017; Dias, Veríssimo, et al., 2022; Dobos et al., 2019; Iusca & Dafinoiu, 2012; Orejudo et al., 2017; Sulun et al., 2017; Yondem, 2007), including other predictors associated with MPA such as trait anxiety, negative feelings, worry, guilt and shame. The systematic review by Barros et al. (2022) discussed patriarchal societal structures, which have a direct impact on social and cultural experience norms and can be a stressor for women, affecting interpersonal issues related to music performance anxiety. According to Coşkun-Şentürk and Çırakoğlu (2017), women have been affected by conservative social relations, and are more exposed to the pressure of moral and social norms. Thus, it is likely that women may feel more vulnerable to MPA. However, further studies should be conducted to better understand this variable in the Portuguese context.
Regarding age as a predictor of anxiety, only factor 3 of the subscales showed no significant impact (factors 1, 2 and total were significant). On the other hand, the predictor performance experience (years of performance experience according to the category ‘up to 9 years to 10 to 14 years’) had a significant impact on all dimensions of the scale, including the total factor. In summary, the greater the age and performance experience, the lower the MPA levels associated with the Behavioural/Emotional, Contextual/Physiological and Cognitive factors of the PoMPAS. Other publications similarly confirm these findings (Hamann, 1982; Kenny et al., 2011; Paliaukiene et al., 2018; Steptoe & Fidler, 1987), which indicate that MPA is inversely proportional to years of study, with higher MPA associated with less performance experience. Steptoe and Fidler (1987) also negatively correlated age with stage fright (the lower the age, the higher the MPA and vice versa). Similarly, Zarza et al. (2018) and Kirchner et al. (2008) reinforce that students who start their studies at an earlier age have fewer anxiety symptoms.
Concerning health problems, although 79 participants reported physical and psychological issues, only the factor 3 was significant, correlating it to the cognitive thoughts. However, in other studies, it is possible to identify health problems in music students related to perceptions, attitudes and harmful behaviours (L. S. Araújo et al., 2017), and musculoskeletal problems, as reported by Sousa et al. (2017). The latter, despite the professional context, may occur due to excessive instrumental practice while still in the higher education environment (Jääskeläinen et al., 2020).
With regard to the use of antianxiety medication, this issue can be seen as both a health problem and a coping strategy to deal with MPA symptoms. In this study, the predictor ‘use of anxiety medication’ had significant values in all dimensions of the PoMPAS and the total factor. This means that all participants who answered ‘yes’ (59 in total – 33 with a prescription and 26 without a prescription) to taking medication may have high levels of MPA, which justifies taking medication to reduce the associated Behavioural/Emotional, Contextual/Physiological and Cognitive factors. Beta-blockers are commonly referred to as a strategy adopted by music students in higher education. Likewise, in our article on contextual factors, perceptions and strategies (Barros, Marinho et al., 2024), we also mentioned beta-blockers as a strategy. According to Kenny (2005), using beta-blockers as a strategy is common but, according to Nube (1991, 1994), their use in high doses can have negative effects. Furthermore, their use may not be the best option, as they may impair fine motor control, an essential aspect of high levels of musical performance (Nascimento, 2013).
Regarding the use of ‘coping strategies for anxiety’, this predictor was significant for both factor 2 and the total factor of the PoMPAS, suggesting that strategies contribute to lower anxiety levels in the contextual/physiological factors and the PoMPAS total scores. The most commonly used strategies were mental and breathing exercises, consistent with other studies (Liu, 2016; Studer, Gomez, et al., 2011; Zakaria et al., 2013) and our recent study (Barros, Marinho et al., 2024). This study also shows different strategies used to a greater or lesser degree, indicating that the choice of strategy is individual and related to the experienced symptoms. A more conscious and appropriate strategy use may promote the health and wellbeing of this population. It may even prevent the use of illicit substances and subsequent dropout. According to Orejudo et al. (2018), 33.9% of music students in higher education use substances to alleviate MPA, with a high probability of dropping out of their careers.
The limitations of this research should be considered. Firstly, it is a non-randomised convenience sample, which means that the results should be treated cautiously. Regarding performance experience, 49.8% of the participants are in the ‘10 to 14 years’ category and only 9.4% in the ‘20 or more years’ category. It is likely that the categories with longer experience time were not significant, probably due to an unbalanced sample, so we suggest balanced samples in future studies. Another limitation is that the model has to explain a considerable percentage (R2 adjusted) of the result. On the other hand, it is a complex outcome, suggesting the need for new studies to test additional predictors.
We emphasise the importance of a more holistic vision in the training of higher education students, with preventive counselling and health promotion programmes designed for this context. For example, it may be useful to implement health and psychology courses and workshops for musicians, incorporating coping strategies to deal not only with daily practices, but also before, during and after musical performance presentations. Knowing the profiles and individual needs of students, evaluating and introducing changes in behaviour are some of the challenges that will help to reduce MPA and promote the health and wellbeing of music students.
Footnotes
Author contributions
Samuel Barros: Conceptualisation; Data curation; Formal analysis; Investigation; Methodology; Project administration; Visualisation; Writing – original draft; Writing – review & editing. Helena Marinho: Funding acquisition; Resources; Supervision; Visualisation; Writing – review & editing. Alex Bacadini França: Data curation; Formal analysis; Software; Validation; Writing – review & editing. Anabela Pereira: Supervision; Visualisation.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by FCT – Fundação para a Ciência e Tecnologia, I.P., through the project UIDB/00472/2020, with the DOI identifier. ![]() , and financial support through the individual research grant Ref. SFRH/BD/144883/2019.
, and financial support through the individual research grant Ref. SFRH/BD/144883/2019.