
Abstract
Background:
Patients with serious mental illness experiencing psychosis go through many challenges in their daily life activities. Despite the relevance of this issue, qualitative studies on this area from the Global South are scarce. This qualitative study aims to explore the impact of psychosis on functioning in patients with serious mental illness.
Methods:
Nine patients clinically diagnosed with serious mental illness, aged 18–60, identified through maximum variability sampling, were approached for written informed consent. Subsequently, they were invited for an in-person interview regarding the impact of psychosis on their daily activities and everyday functioning. Interviews were also conducted with seven primary caregivers and four healthcare professionals working in the field of mental health. The interviews were audio-recorded, transcribed, and thematically coded in Microsoft Word and Microsoft Excel. The data analysis was done using the Systematic Text Condensation (STC) strategy. Interviews were conducted until thematic saturation was achieved.
Results:
The key themes are presented as: Influence of psychosis on functioning, personal narratives of living with psychosis, and personal anecdotes from mental health professionals on psychosis and functioning. The results highlight the multidimensional nature of psychotic experiences, which reach beyond clinical manifestations and lead to significant emotional distress, reduced self-worth, and a diminished sense of personal identity.
Conclusions:
This study brings out the need for holistic, patient-centered approaches that recognize the complex lived experiences of individuals experiencing psychosis, emphasizing the importance of comprehensive support systems that address functional, social, and psychological dimensions of mental illness.
We aimed to explore how the lived experience of psychosis interferes with the daily activities and functioning of patients. Functional limitations caused by psychotic symptoms are chronic, dynamic, and pervasive. Despite this, patients can use various strategies to deal with the psychotic experiences. Psychosis and functioning are multidimensional concepts; the interplay between specific symptoms and areas of functioning needs to be studied in more detail.Key Messages:
Serious mental illnesses (SMI) are diagnosable mental, behavioral, or emotional disorders that cause severe functional impairment that substantially interferes with or limits one or more major life activities. 1 SMIs are long-term illnesses involving substantial functional impairment over multiple symptom domains. 2 Based on the International Classification of Functioning, Disability and Health (ICF), many authors have developed core sets of functioning and disability across three domains: Body functions and structures, activities and participation, and contextual factors. These core sets help to identify and assess areas of disability in a person. Core sets are available for bipolar disorder, depression, and schizophrenia.3–5 Authors have also aggregated the core sets for these three conditions and formed a brief core set for severe mental disorders. Out of the 11 common categories, three correspond to body functions, six refer to activities and participation, and two correspond to environmental factors. 6
Psychosis is a common feature of SMI and has a significant impact on daily functioning and quality of life. 7 Evidence suggests that deficits in even basic skills, such as oral hygiene, can significantly affect individuals with SMI. 8 It is well documented that disruptions or restrictions in activity engagement can negatively impact health and well-being, including both physical and mental health. 9 Individuals with SMI spend much of their time in passive, solitary activities, and less time in work or other productive occupations in the community. They also spend more time asleep. 10 Literature also tells us that poor sleep can be linked to psychosis, especially insomnia with paranoia.11,12 The maintenance of relationships with family, friends, and the broader community over the long-term is said to be challenging. 13 Studies show that people with SMI seek education, either for employment or as preparation for employment, indicating their willingness to work.12,14,15 However, their functional performance might be adversely affected by cognitive abilities, motivational deficits, and contextual factors. 16 Social stigma and discrimination frequently exacerbate the psychological burden, leading to social isolation, reduced quality of life, and challenges in maintaining employment and interpersonal relationships. 17
Even though much evidence is available on the impact of psychosis on functioning, there are limited qualitative studies narrating the lived experience of psychosis interfering with daily activities. Hence, we aimed to explore this impact from the perspectives of patients, their caregivers, and mental health care professionals. Given that India is a country with multiple, interlinked cultural practices, we hypothesized that personal narratives from various stakeholders would provide rich details of this experience. The insight from these experiences would help to understand individual and contextual factors that mediate the relationship between psychosis and functioning, and thereby facilitate tailored psychosocial interventions.
Methods
Ethical Considerations
The study was reviewed and approved by the Institutional Review and Ethics Committee.
Study Design
This was a descriptive qualitative study employing a phenomenological analysis. This method was chosen because it would allow the researcher to focus ideographically on each participant as the experiential expert, while also conducting comparative analysis to highlight the diversity of participants’ experiences. We used face-to-face interviews as they would enable in-depth exploration of personal experiences.
Study Setting
The study was conducted at the inpatient occupational therapy unit of the Department of Psychiatry at a tertiary care center in South India between June 2024 and February 2025. The setting employs a family-centered, multidisciplinary care model, with psychiatrists, nurses, occupational therapists, psychologists, and social workers comprising the treatment team.
Participants
The participants were recruited through purposive sampling from the inpatient care facility, where persons with mental illness stay with their primary caregivers for a few weeks to receive psychosocial rehabilitation. The authors are occupational therapists who oversee the rehabilitation process and work closely with patients and families throughout their hospital stay. We approached patients around two weeks into their admission, allowing enough time to assess mental status and occupational abilities. Persons aged between 18 and 60, on regular treatment, were approached for written informed consent if they met the International Classification of Diseases-11th Edition criteria for schizophrenia (6A20), schizoaffective disorder (6A21), or bipolar disorder (6A6). 18 We included persons with psychosis, but excluded those whose symptoms interfered with their ability to communicate their experiences, as judged by the treating psychiatrist. We also excluded patients with other psychiatric or physical comorbidities. We also interviewed a few primary caregivers and professionals with at least two years of experience in mental health care, who provided written informed consent. We used maximum variability sampling to ensure participation across age groups and sociocultural backgrounds.
Data Collection
Nine persons with SMI, seven primary caregivers, and four mental health professionals were interviewed in their vernacular language—Tamil, Hindi, Bengali, Malayalam, or English. Each author conducted interviews in the languages in which they were proficient. The interviews were conducted in a therapy room with only the participant and the interviewer present. The interviews typically lasted from 45 minutes to one hour. The interview guide questions were formulated using the ICF core sets for severe mental disorders as a reference. 3 Interview guides were developed separately for patients, caregivers, and professionals and translated as necessary (Supplementary Material). The questions were finalized after discussion with senior colleagues, who served as a critical reference group. The interviews were audio-recorded, and the interviewer also took field notes on nonverbal aspects. Each interviewer transcribed and translated the interviews into English using Microsoft Word. Data saturation was considered achieved when no new codes were generated after the seventh patient and sixth caregiver interviews. We conducted interviews with two more patients and one caregiver to ensure data saturation.
Data Analysis
The data were analyzed using the Systematic Text Condensation (STC) strategy, based on Giorgi’s psychological phenomenological analysis. STC prescribes analytic reduction with specified shifts between decontextualization and recontextualization of data, involving four steps of (a) total impression, (b) identifying and sorting meaning units, (c) condensation, and (d) synthesizing. 19 In all, we had 231 meaning units across 31 categories from patients, 170 meaning units across 36 categories from mental health professionals, and 154 meaning units across 13 categories from caregivers in the study. Initially, separate categories were given for the influence of psychosis on various domains of functioning. We decided to consolidate categories across domains and participants under the theme “influence of psychosis on functioning.” A sub-theme of patients’ personal experiences and coping strategies was also added to this theme. After synthesis, this theme had seven categories for the influence of psychosis on functioning and an additional sub-theme for personal experience of psychosis. We decided to develop a second theme, “personal anecdotes from health care professionals on psychosis and functioning,” with two categories, as these were able to provide additional insights into the intersectionality of sociocultural factors, psychosis, and functioning.
Trustworthiness of the Study
The validity of the analysis was ensured by adhering to the standards proposed by Morse et al. 20 Investigator responsiveness was maintained by all authors, who analyzed data from initial interviews and conducted inductive analyses to inform subsequent interviews. Methodological coherence was ensured by aligning the research question, sampling methods, data analysis, and interpretation. Ensuring sampling adequacy and appropriateness, and iterative data analysis until saturation, were also agreed upon by all authors as verification strategies.
Results
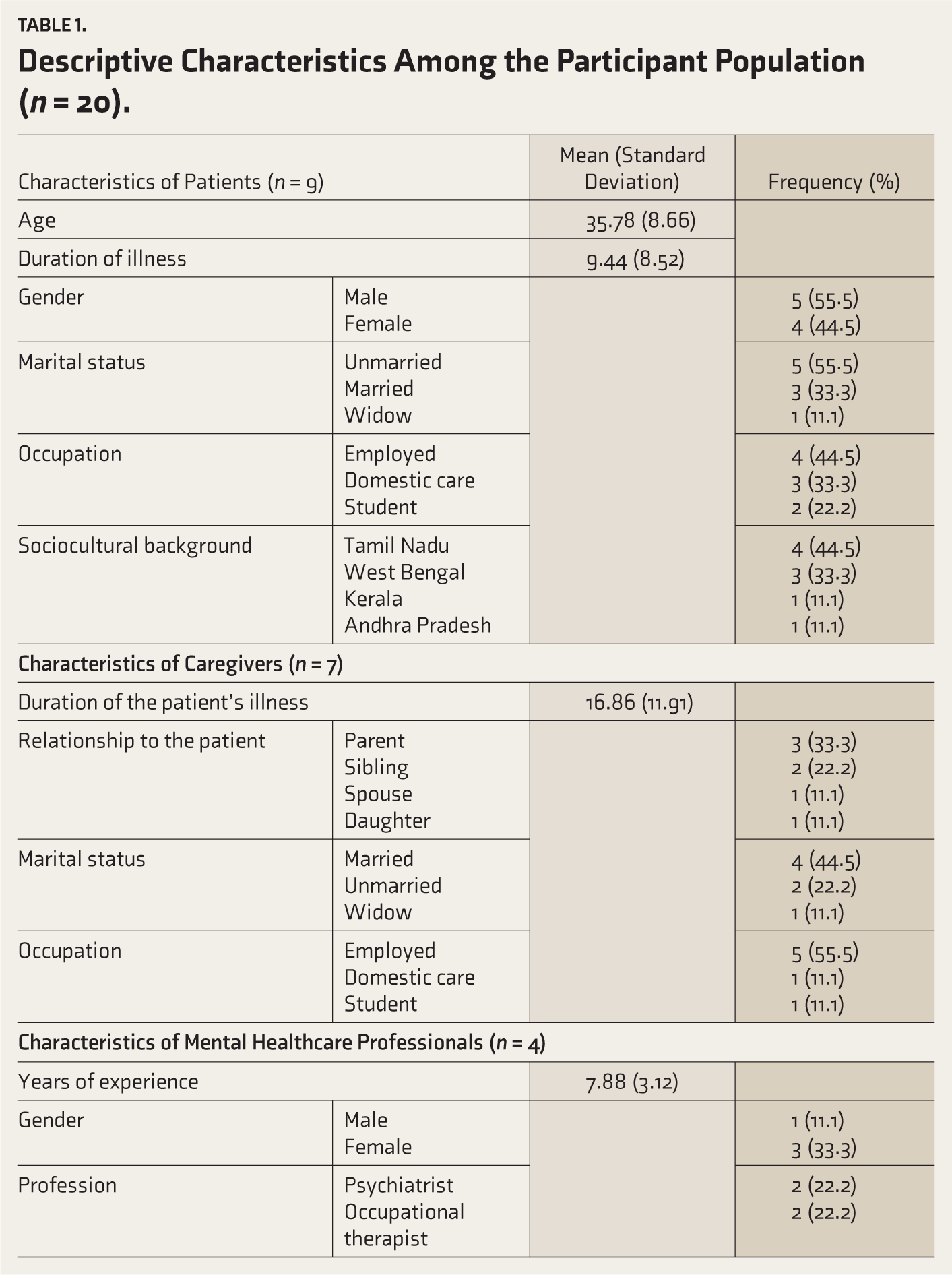
In all, we interviewed nine patients with SMI, seven primary caregivers, and four mental health professionals. The participants’ details are provided in Table 1. Our findings are presented in two themes: The first outlines the influence of psychosis on various areas of functioning, such as daily living activities, sleep, paid work, and social relationships; the second, a sub-theme, addresses the lived experience of psychosis. The second theme looks at the personal experiences of mental health professionals and the sociocultural influences on psychosis and functioning.
Descriptive Characteristics Among the Participant Population (n = 20).
Theme 1: Influence of Psychosis on Functioning
All participants were able to describe the adverse effects of psychosis across the functional domains of basic and advanced activities of daily living, paid work, sleep, interpersonal relationships, and social participation. Most patients reported that preoccupation with the content of symptoms, active engagement with psychotic experiences, negative mood states, and decreased motivation arising from psychotic beliefs were the main reasons for functional decline. P6 and P8 discussed how listening to voices and being preoccupied with them affected self-care activities such as brushing and bathing. P3 heard voices commanding him not to sleep and was unable to study. P7 was scared to go to work, thinking he would be killed, and P3 stopped socializing, believing that others were talking about her.
Most patients felt that active engagement in specific tasks, such as taking a walk, helped shift the focus from psychotic experiences. Nevertheless, a few patients also reported an increase in these experiences when attempting to focus.
“When the voices become louder, my focus shifts toward that, and I become quiet, and sit in one place, give my full concentration to the voices and forget the work I was doing” (P2).
The caregivers shared their experiences of how the dysfunction prevented patients from assuming expected roles, strained family relationships, reduced the family’s social involvement, and increased the time required for caregiving. C1 spoke about how her daughter feels unsupported when she, as the mother, did not share her daughter’s persecutory beliefs. C3 shared concerns about her mother’s safety, as she was prone to keep the gas stove on with the intention of dying. C4 reported financial strain from repaying debts and loans incurred by his ill son.
“So, there are times when he says, ‘Now I don’t want to bathe’. He wants to keep himself clean, but the very thought that people are watching him when he is bathing and doing his personal things makes him postpone things” (C7).
The mental health professionals also expressed similar themes; they generally believed that the intensity and frequency of symptoms, rather than the content, led to dysfunction. They were also of the opinion that even if the content of psychotic experiences was pleasurable, the time spent in engaging with the experiences subsequently led to reduced priority given to functional tasks. They were also able to highlight how gender-based and cultural factors contributed to unique patterns of dysfunction in a person. H4 highlighted the vicious cycle of symptoms leading to increasing social isolation.
“During conversations, due to delusions and hallucinations, he lost focus, said unrelated things, experienced a thought block, and struggled to maintain a continuous flow in conversation. This led his friends to feel upset and to ignore him. This caused him to feel left out, and his family, frustrated by the lack of response, eventually stopped making efforts to help him” (H4).
Sub-theme: The Lived Experience of Psychosis
All patients expressed distress and regret for the life roles they were unable to fulfill, the interpersonal issues brought about by the psychosis, and the overall adverse effect of the illness on their quality of life. These experiences were all the more distressing when the content included real-life situations such as the inability to work or study effectively. P6 reported hearing voices telling him he would not be able to meet deadlines; this prediction came to pass when he resigned from his developer position. P5 talked about “not wanting to go out and face the humiliation of others talking about her,” which ultimately led to family issues, financial crisis, and being “pushed to a corner of not wanting to live.”
They were also concerned that efforts to improve their skills would be accompanied by the risk of worsening symptoms due to added stress, and wanted to learn how to cope effectively. All of them reported internalized stigma, as well as accounts of external stigma, which impeded vocational opportunities and prospects of marriage and parenthood. We were also able to identify differential stigma within diagnoses, as participants felt that “depression” was a more acceptable diagnosis, whereas “schizophrenia” was considered more dangerous and disabling by society. P6 spoke about being overlooked for a leadership position after he disclosed his diagnosis of schizophrenia, and about how his father had instructed him not to mention that particular diagnosis to others.
On a positive note, participants were also able to describe various strategies that they had utilized to deal successfully with their psychotic experiences. P6 shared how a “key change happened when I understood logically how to distinguish between voices and real-life sounds. When I hear somebody speaking about me, I know it is a voice. When I hear somebody speaking about normal things, I know they are real.” A patient reported telling himself, “people are more interested in themselves than in you, nobody is speaking about you,” which helped reduce distress, and that writing down all his thoughts helped because “it looked silly on paper.”
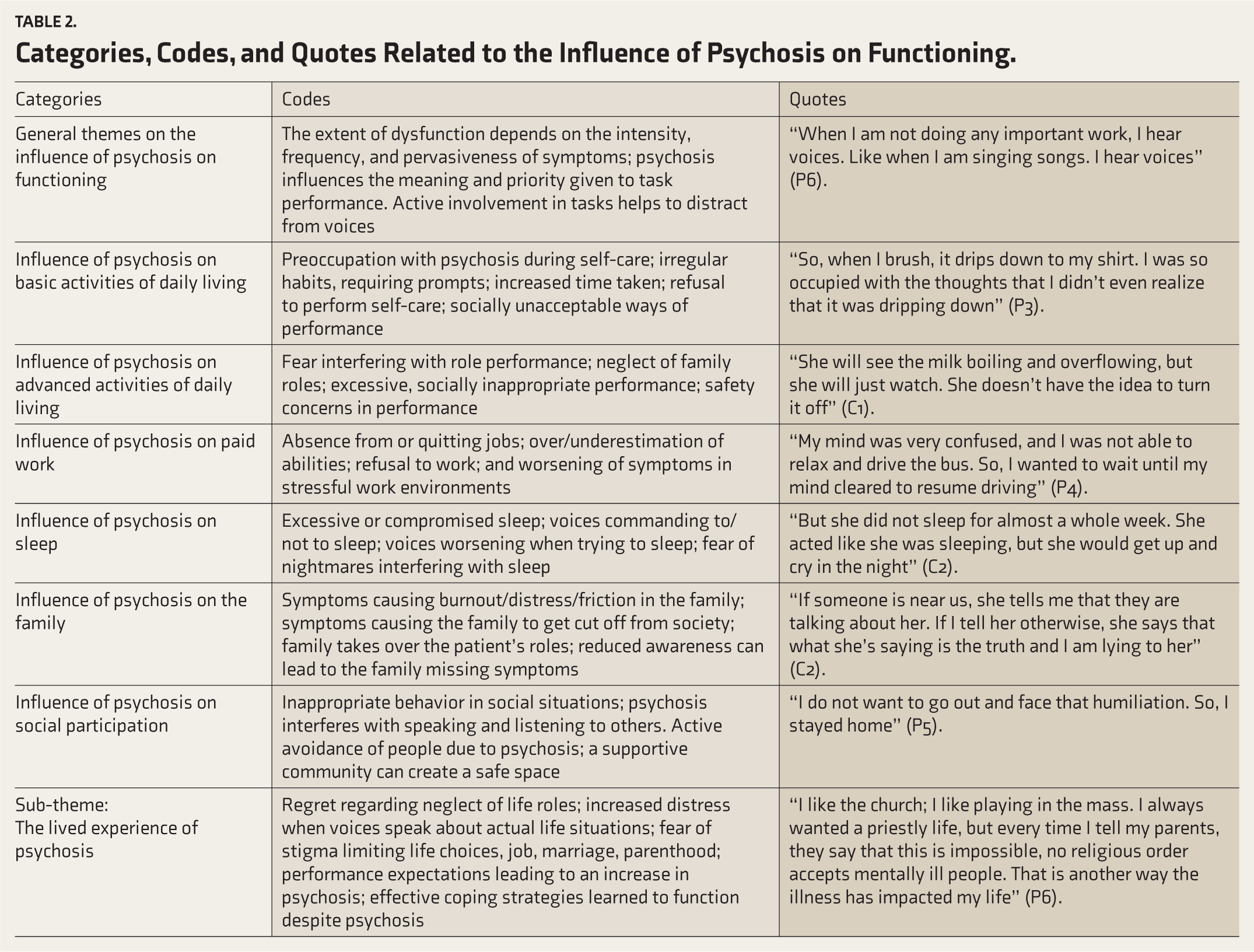
The details of the codes, categories, and quotes pertinent to this theme are given in Table 2. Figure 1 presents a graphic representation of the influence of psychosis on domains of functioning, including basic activities of daily living, advanced activities of daily living, sleep habits, paid work, and interpersonal relationships.
Categories, Codes, and Quotes Related to the Influence of Psychosis on Functioning.
Thematic Map Illustrating the Influence of Psychosis on Various Functional Domains.
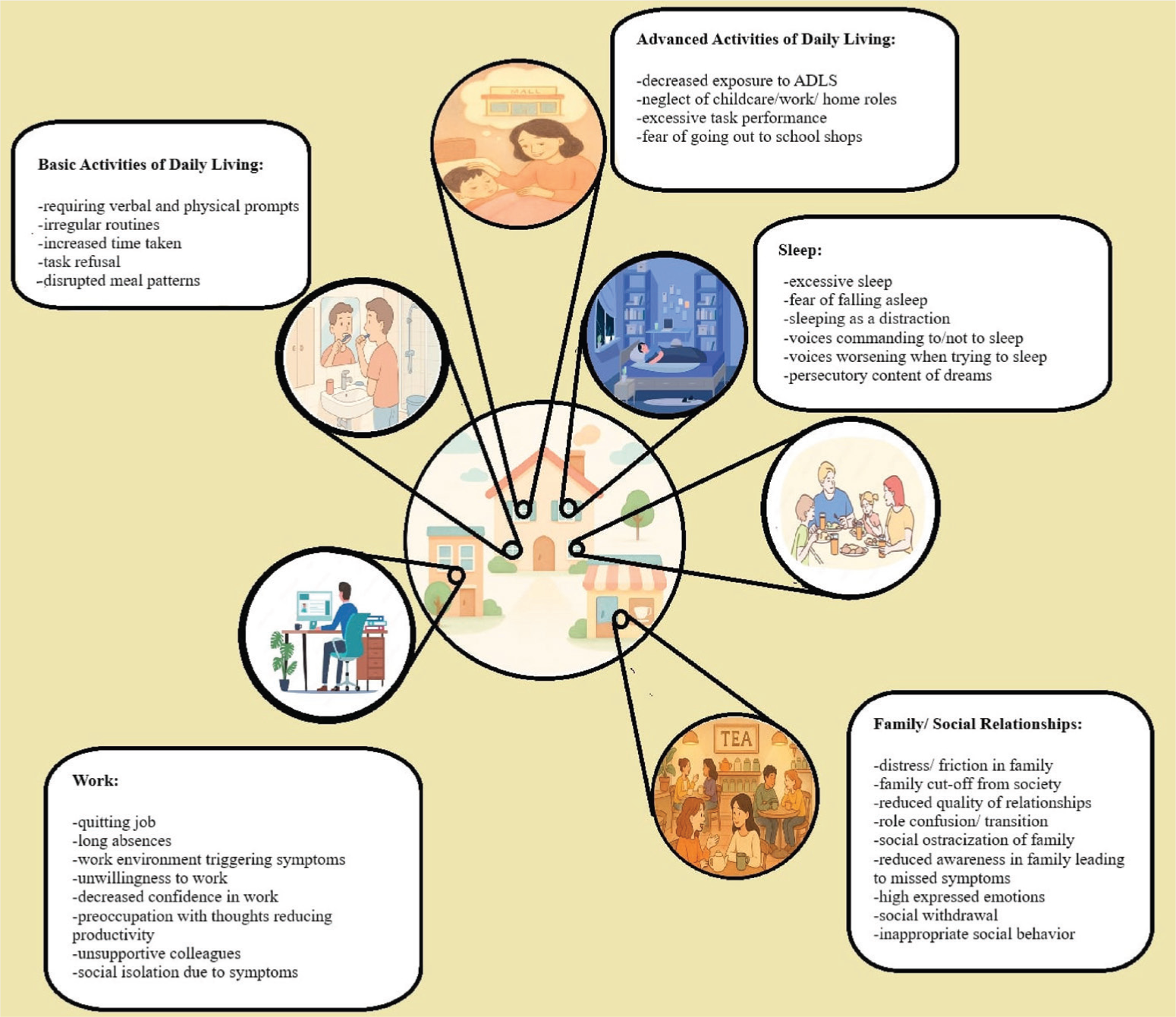
Created with Microsoft Paint (version 11.2402.32.0; Microsoft Corporation; 2024).
Theme 2: Personal Anecdotes from Mental Health Professionals on Psychosis and Functioning
All professionals reported that functional decline was often an indication of the extent of psychosis, and the crucial point at which families brought persons with behavioral changes to healthcare providers for assessment. They advocated functional recovery through pharmacological management to reduce symptoms, combined with skills training, and environmental accommodations to address contextual barriers. This was considered all the more important in persons with residual symptoms not fully controlled with medications alone. Professionals were also cognizant of the need to finely grade the therapeutic press to improve functioning so that the stress did not become overwhelming for patients. They felt that if a patient “has the capacity to understand the consequences of his actions, if he understands the risks,” then it was all right to “go abroad to work, to join a stressful course, or to get married.”
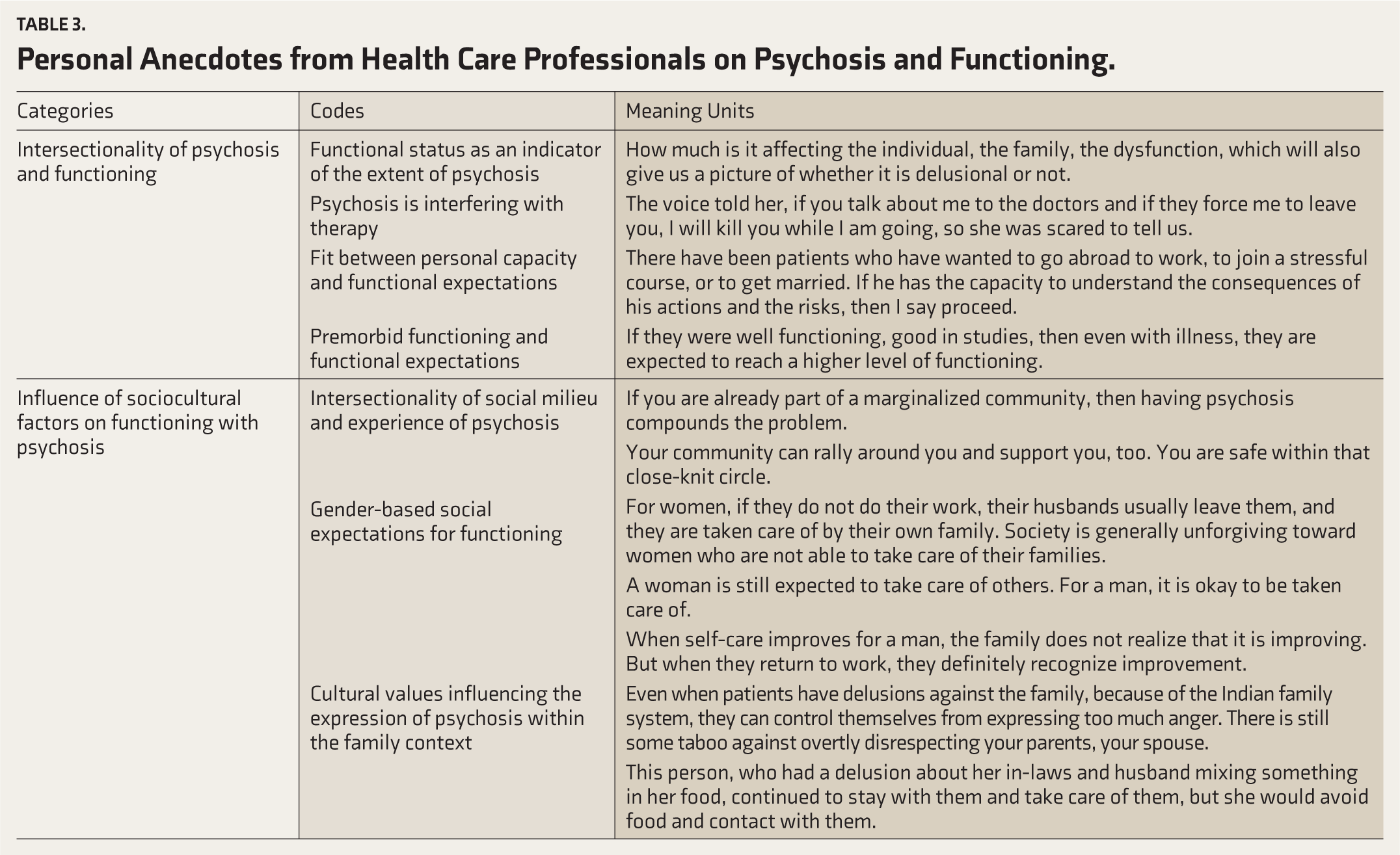
They provided various examples of facilitators, such as good family and community support, that mediate functional recovery in patients. They thought that the family-centered values of Indian communities facilitated emotional support to patients even when patients had delusional ideas against the family. They also identified barriers such as stigma, rigid gender-based role expectations, and cultural beliefs about mental illness and treatment, which impede the recovery process. Of particular note is the cultural expectation for a woman to be independent in home-making and childcare roles, and for a man to be engaged in paid work, irrespective of the illness. The details of the codes, categories, and meaning units relevant to this theme are given in Table 3.
Personal Anecdotes from Health Care Professionals on Psychosis and Functioning.
Discussion
Our study aimed to elicit personal experiences of patients living with psychosis, as well as experiences of caregivers and mental healthcare professionals who provide them care. We hoped to better understand the individual and contextual factors that mediate the relationship between psychosis and functioning.
The study results reveal an individual-specific profile of functional limitations based on psychotic symptoms. The adverse effects on functioning seem to be chronic, dynamic, pervasive across the functional domains, and may or may not be directly related to the characteristics of the psychotic experience. There is also considerable distress associated with these experiences and with their effects on functional roles in a person’s life. The experiences of the patients in our study are similar to a qualitative study from India, which explored desired functional outcomes from the perspective of patients with schizophrenia and their caregivers. Of the eleven outcomes that emerged, eight were related to functional recovery: Activity engagement, social functioning, education/employment, independent functioning, fulfillment of duties and responsibilities, self-care, medication-free management, and self-determination. 21
Beyond the experience per se, the reality of having a mental illness and the limitations that it poses in their personal lives, relationships with significant others, life events such as marriage, employment, and parenthood, have been described by our participants. Of particular note were the stigmatizing experiences that persons with illness reported, where just the label of being mentally ill was enough to exclude them from social and vocational participation. The increased stigma associated with a diagnosis of schizophrenia, as compared to bipolar disorder or depression, has been reported by authors from India and elsewhere.22–24 The exclusion from participation in social and vocational spheres solely due to stigma, despite functional recovery, has also been reported from India. 25 The narratives of internalized stigma, where patients reported reluctance to consider life tasks such as marriage and parenthood, also require targeted attention to improve the self-concept of persons with SMI.
Despite these adverse circumstances, the patients were also able to describe how they utilized behavioral, cognitive, and emotive strategies to overcome the psychotic experiences. The personal narratives of the patients in this study indicate the need for prolonged, consistent engagement by professionals with patients, actively discussing their experiences and management strategies as the illness evolves. The accounts remind us that functional recovery is often a process rather than an end, especially for diseases with a chronic, changing course, where the benchmark needs to shift as the impairments also move based on the psychopathology.
The results from our study also reveal the added burden on families, directly as a result of the negative mood states caused by psychotic experiences, and indirectly due to added household responsibilities, economic cost, and social exclusion. The caregivers’ accounts in our study of the significant time spent traveling, waiting for appointments, and accessing care are consistent with the concept of time toxicity. 26 The cumulative burden of time spent on treatment-related activities directly translates into lost wages and reduced time for other essential life roles for most caregivers. This finding points to the need to look beyond the person with illness, to consider the whole family as a functional unit in psychosocial rehabilitation, in other words, the emerging concept of “family centric rehabilitation.” 27 The Indian literature has also reported positive effects of family intervention programs in which family psychoeducation was provided to engage patients in functional activities such as household work, family-based employment, or vocational training. 28
The experiences of the mental health professionals in our study show that they often use functional recovery as a yardstick when complete symptom remission is not possible. They also consider the extent of functional decline as an indicator of the severity of psychotic symptoms. They were also mindful of the need to plan functional goals aligned with the patient’s personal capacity at any given point in time, continually adjusting them based on the illness trajectory. Similar to the other stakeholders, the mental health professionals were also able to identify sociocultural factors that influenced functional recovery, and also cited stigma as a major barrier to seeking mental health services.
There is good evidence that both psychosis and functioning are multidimensional concepts, and for optimal functional recovery, the interplay between specific symptoms and areas of functioning needs to be studied. However, most available studies have assessed both constructs using global score measures, which are inadequate to understand the complex intersectionality between psychosis, functioning, and contextual factors. One longitudinal study done on patients with first episode psychosis in Spain conducted network analysis to identify patterns between the different dimensions of functioning and psychopathology. They found various factors related to psychosis that interconnected and mediated domains of functioning such as self-care, social communication, and community participation. 29 Another longitudinal study done in Finland on persons with first episode psychosis found that at 18-month follow-up, fewer than half of them were functioning well. 30 A qualitative study from North India, which explored experiences of patients and caregivers with first episode psychosis, also identified impairments in functioning to be one of the reasons when caregivers sought treatment. They also identified occupational dysfunction across all domains of functioning, with caregivers reporting improvements in symptoms but not functional recovery. 31 This underscores the need for assessment and early intervention to support functional recovery during the initial phases of the illness. The interventions should consider the patient’s and family’s gender-based role expectations to ensure alignment with cultural values. Strategies to manage environmental factors that mediate functional recovery, such as reducing stigma and addressing negative societal attitudes, should also be implemented. There needs to be more targeted research on the various functional domains affected by psychosis, employing comprehensive, performance-based outcome measures.
Limitations
The sample size is relatively small and from the same center, which could limit the study’s generalizability. The exclusion of patients with psychotic symptoms that interfere with communication may have introduced systematic bias. We did not define inclusion criteria for patients based on illness characteristics such as level of psychopathology, duration of illness, or current pharmacological regimen. We did not assess caregiver-related factors, such as cognitive sophistication and disease knowledge, which could affect the quality of the information provided. We were able to include professionals from only two mental health streams. Collecting additional information from professionals such as psychologists, psychiatric nurses, and psychiatric social workers could have provided insight into other facets of functioning.
Conclusion
Our study highlights the complex, deeply personal experiences of persons with psychosis who are attempting functional recovery. The results call for looking beyond the diagnosis to understand the multidimensional effect of psychotic symptoms and study the interaction between environmental facilitators and barriers that mediate the recovery process. The personal narratives of those experiencing psychosis emphasize the need for holistic, client-centered care by providing support systems that address the psychological, social, and functional dimensions of mental illness.
Supplemental Material
Supplemental material for this article is available online.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
The authors would like to express their gratitude to all the participants for their time and willingness to discuss their experiences.
Appropriate Permissions from the Concerned Authorities
Written permission was obtained from the Head of the Department, Psychiatry and the Principal, CMC Vellore.
Data Sharing Statements
All relevant data have been added as tables. Additional individual participant data will not be made available due to ethical considerations.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
No part of this article was written or generated by a generative AI tool. The authors take full responsibility for the accuracy, integrity, and originality of the published article.
Ethics Committee Details
Name of the Institutional Ethics Committee/Independent Review Board: Institutional Review and Ethics Board, CMC Vellore.
Approval reference No.: 0624029 Date of approval: 5 June 2024
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent/Assent
Written informed consent was obtained from patients, caregivers, and healthcare professionals who fit the inclusion criteria.
Prior Presentations
Nil.
PROSPERO/CTRI Details
Not applicable.
Registration
Not applicable.
Trial registry name:
URL Registration number
Simultaneous Submission to Another Journal or Resource
Not submitted to another journal or resource.
Status of Your Study (for Study Protocol)
Not applicable.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.