
Abstract
Background:
The study aimed to evaluate the effectiveness of a social skills training program provided at the occupational therapy unit of a tertiary care center in India.
Methods:
The study used a pre–post interventional design where 101 consecutive patients with a diagnosis of schizophrenia or bipolar affective disorder, between 18 and 60 years, who provided written informed consent, were assessed on the Vellore Assessment of Social Performance (VASP) during the first week of attendance (baseline). Subsequently, they were enrolled in a six-session social skills group training program for two weeks. They were assessed on the VASP after one week (midterm assessment) and at the end (posttest) of the intervention. A follow-up assessment was done two weeks after cessation of the intervention. The participants were also scored on the Brief Psychiatric Rating Scale (BPRS) at four time points.
Results:
Repeated measures ANOVA revealed significant differences in the VASP scores between time points, that is, F(baseline, midterm) = −4.34 and P = 0.001; F (baseline, postgroup) = −6.92 and P = 0.001; and F (baseline, follow-up) = −8.71 and P = 0.001. The correlation between the BPRS and VASP scores was also significant at each time point.
Conclusion:
The social skills group training protocol seems to be effective and feasible for the Indian population. Since conducting multicenter clinical trials might not always be possible in resource-constrained settings, this study might be considered preliminary evidence for context-specific, peer-/family-supported social skills training.
Keywords
Social skills training is an essential component of the psychosocial rehabilitation of people with severe mental illness. Family involvement and context specificity of training are needed for improved generalization of skills.Key Messages:
Social skills refer to behaviors that, when combined in appropriate sequences and used in appropriate contexts, enable an individual to have successful social interactions. 1 This success in social interactions is reflected by social competence, through the application of skills in real-life situations. 2 The skills include verbal, nonverbal, and paralinguistic behaviors and accurate perceptual and cognitive skills required for effective societal interactions. 3 The biopsychosocial stress-vulnerability model of schizophrenia postulates that cognitive and psychobiological vulnerabilities, exacerbated by stressors, lead to decreased social functioning. 4 In persons with schizophrenia, social functioning can also be further impeded by positive symptoms, negative affective states, neurobiological deficits, motivational factors, and adverse environmental conditions. 5 Studies have shown good social skills to be protective factors in schizophrenia 6 and impairment in social functioning to be a predictor of poorer outcome, relapse rates, illness course and unemployment. 7
Social skills training (SST) programs aim to address deficits in social skills that result in impaired social functioning and are among the psychosocial interventions recommended by the Schizophrenia Patient Outcome Research Team. 8 The interventions employ behavioral and social learning principles like behavioral goal setting, prompting, modeling, and shaping, combined with positive reinforcement and overlearning to teach skills. 9 Although SST has been adopted as an adjuvant to therapy and controlled studies have been done across continents, evidence is limited from developing countries like India. 10 A recent systematic review found significant differences in favor of social skills programs when compared to standard care; however, the data were limited with low-quality evidence. The reviewers suggested including the families in training, employing validated outcome measures used in routine clinical care, and conducting trials in multiple settings. Since generalization of skills into real-life situations is a concern with psychosocial interventions, it was also recommended to incorporate naturalistic environments, peers, and other stakeholders during the training process. 11
This study aimed to evaluate the effectiveness of a social skills group training protocol, which is used in routine clinical care, in improving the social functioning in persons with severe mental illness (SMI).
Materials and Methods
Design and Setting
The study used a pre–post interventional design and was carried out at the inpatient occupational therapy unit of the Department of Psychiatry, which is a 122-bedded facility, with an average daily footfall of around 500 outpatients, attached to a tertiary care center in South India. It has a residential care facility where persons with mental illness can stay with their families for an average of five weeks to receive psychosocial rehabilitation, including SST. This is one of the few centers in South India offering psychosocial rehabilitation facilities, and the majority of patients are from other states, who travel specifically for accessing healthcare. Since SST is already part of the standard care available at the center, it was not thought to be ethical to have a randomized control trial, where patients in the control group would be deprived of the intervention. Hence, the pre–post interventional design was decided as the most feasible one, considering the limited time duration of inpatient stay and ethical issues. There were no changes made to the method after the commencement of the study.
Participants
All inpatients are routinely assessed for functional deficits within one week of admission, and goals for the admission, including SST, are set by the therapists. Patients thus identified and who fulfilled the inclusion criteria of being diagnosed with schizophrenia or bipolar affective disorder according to ICD-10 diagnostic criteria, between 18 and 60 years of age, who provided written informed consent, were recruited for the study through convenience sampling. Those with comorbid physical or psychiatric illnesses and those with acute psychotic presentations were excluded. Those identified as eligible were explained about the study in the presence of their relatives, after which they read the written informed consent document and provided consent if they wished.
Intervention
The protocol for the SST group is based on the hierarchical model of verbal and nonverbal skills as building blocks of social competence, consisting of social perception, social cognition, and emotional perception. 6 There are six sessions occurring thrice a week, spanning 60–90 minutes. The group process is structured, based on learning principles, as a ten-step model: 1. Introduction—brief introduction of what skill is to be focused on; 2. Rationale—discussion of the importance of the skill in daily life; 3. Instruction—detailed information on various aspects of the skill; 4. Modeling—role-play by therapists to demonstrate the skill; 5. Review—discussion about observed aspects of role-play; 6. Supervised practice—role-play by participants; 7. Feedback—positive and corrective feedback of role-play to participants by therapists/peers; 8. Problem-solving ideas—difficulties encountered in the role-play discussed and suggestions provided by therapist and peers; 9. Generalization—supervised practice in real-life situations, accompanied by caregivers; and 10. Independent practice—participants try out the skills learned, in real-life situations, supervised by the caregivers (the following session starts with a review of this). 12 The consecutive sessions focused on (a) eye contact, social smile, and appearance, (b) facial expressions, gestures, and posture, (c) proximity and orientation, (d) initiating and terminating conversation, (e) maintaining conversation, and (f) putting them all together (Appendix 1, available as online-only supplementary file).
Outcomes
The primary outcome measure was the VASP, 13 which measures social functioning in 20 items across the following 5 domains: (a) nonverbal social skills, (b) verbal social skills, (c) receptive social competence skills, (d) processing social competence skills, and (e) expressive social competence skills. The scoring is done after observing performance in life situations, with a seven-point scoring system of “0” being not able to perform the skill, “1” and “2” being able to perform in test (role-play) situations, “3” and “4” being able to perform in familiar life situations, and “5” and “6” being able to perform the skill in unfamiliar life situations. This performance-based measure was developed and standardized 13 specifically among the patients attending the tertiary care center. The assessments were done in-person at four time points; before intervention (baseline), one week into SST (midterm assessment), end of SST (posttest), and two weeks after cessation of intervention (follow-up). The participants were also scored on the BPRS 14 at four time points to quantify psychopathology.
Sample Size
The sample size was calculated a priori comparing the pretest and posttest scores of another study on SST, assuming 0.280 effect size with 80% power, as 100. 15
Implementation
The third author recruited patients, obtained written informed consent, collected demographic data, and scored patients on the BPRS within ten days of admission. The SST sessions were conducted by the first author; the scoring on the VASP at all four time points was done by the second author. The first and second authors are senior occupational therapists with more than 5 years of experience in group therapy for persons with mental illness.
Statistical Methods
To describe the population, descriptive statistics (mean and standard deviation) were calculated for continuous data, whereas frequency distributions were obtained for categorical variables. A repeated measures ANOVA was performed to measure changes in the social skills scores over the four time points. While bivariate correlation, using Pearson’s correlation coefficient, was done to compare social skills and continuous variables, ANOVA was done to measure the difference in social skills between groups for categorical variables. Differences were considered significant at P < 0.05 for correlation and association tests unless otherwise specified. The statistical analysis was performed using SPSS 18.0 (SPSS Inc., Chicago, IL, USA).
Ethics Statement
This study was conducted in conformity with and after approval from the Institutional Review and Ethics Board of the Christian Medical College and Hospital, Vellore, Tamil Nadu, India.
Results
Participant Flow
Total 109 patients were recruited. Eight got discharged before completion of the program; hence the final sample size was 101. A total of 19 SST groups were conducted with an average of 6 patients per group. Data collection commenced in October 2017 and ended by April 2019 when the required sample size was reached.
Baseline Data
The majority of the patients were diagnosed with paranoid schizophrenia, male, young adults, unmarried, graduates, from middle socioeconomic status, and currently unemployed (Table 1). The descriptive statistics of social skills and psychopathology are shown in Table 2.
Descriptive Statistics of the Sociodemographic and Clinical Variables (
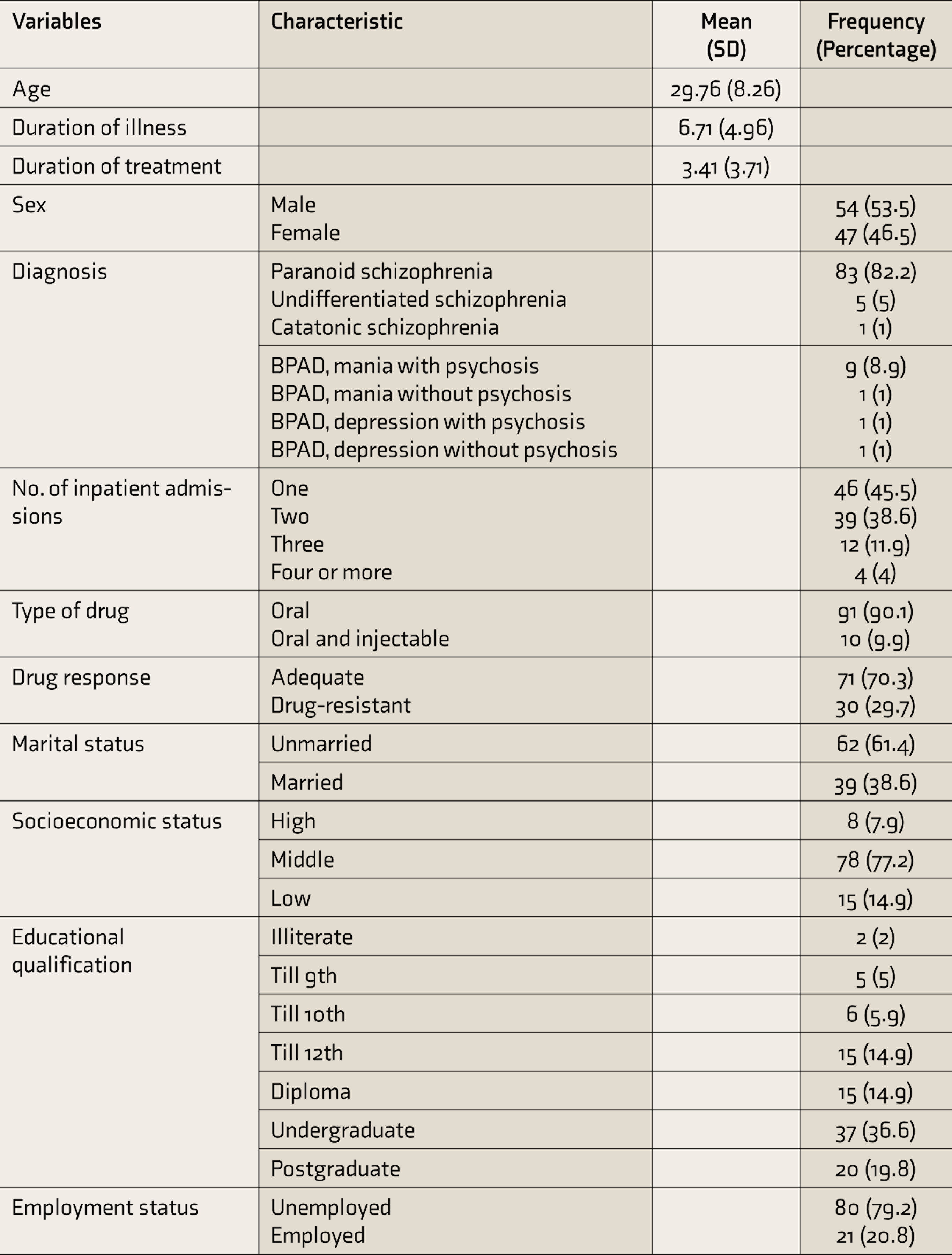
BPAD: bipolar affective disorder.
Descriptive Statistics of Social Skills and Psychopathology (n = 101)
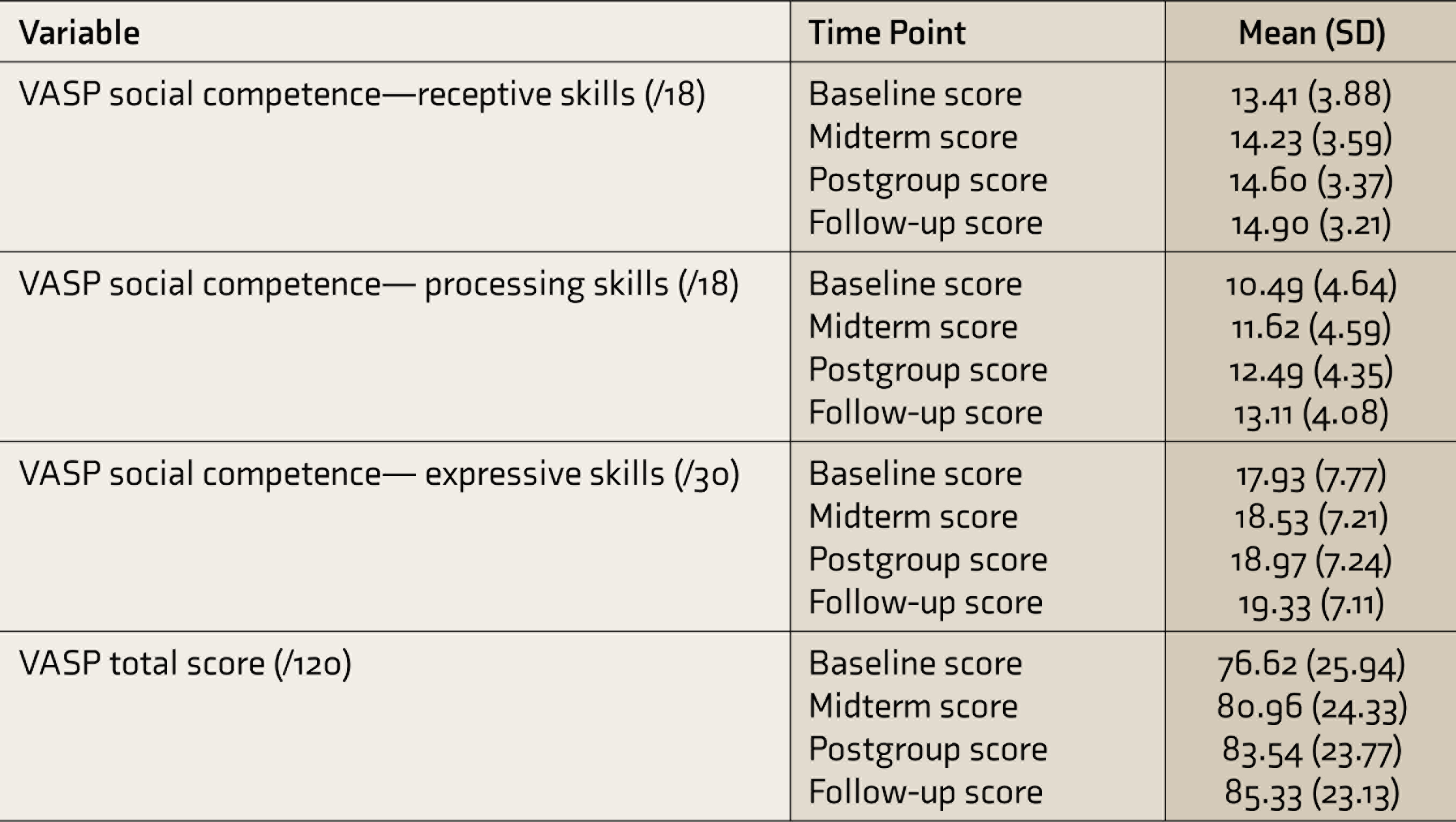
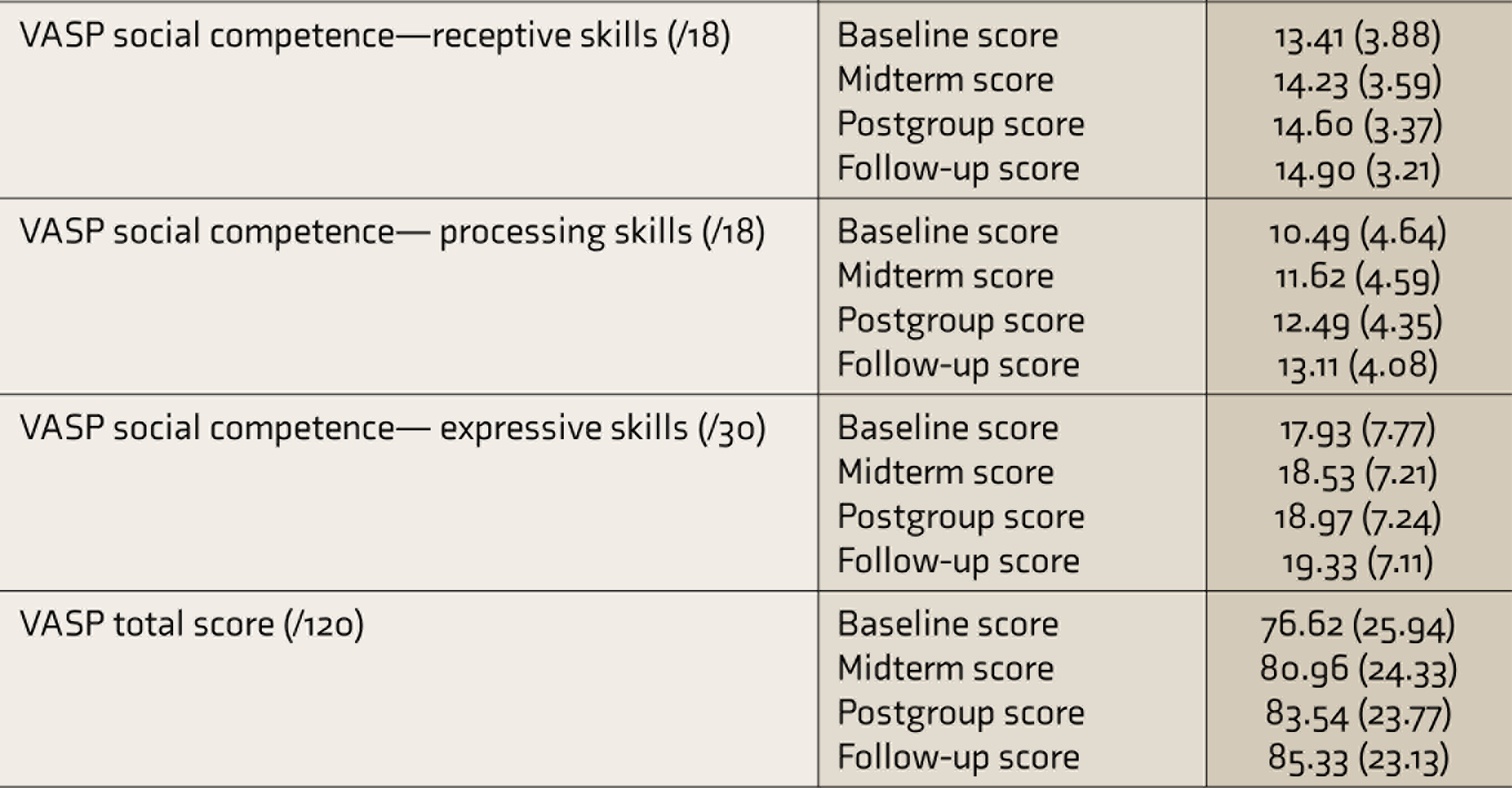
VASP: Vellore Assessment of Social Performance.
Effectiveness of SST
The repeated measures ANOVA was performed to compare the VASP scores across the four time points. The VASP scores were tested for normality and sphericity. Mauchly’s test of sphericity indicated that the assumption of sphericity had been violated, that is, χ 2 (5) = 317.348, P < 0.0005, and ε < 0.75, and therefore, the Greenhouse–Geisser correction was used. There were significant differences in the VASP scores between time points, that is, F (baseline, midterm) = −4.34, P = 0.001; F (baseline, postgroup) = −6.92, P = 0.001; and F (baseline, follow-up) = −8.71, P = 0.001.
Correlation Between Social Skills and Psychopathology
The details of the correlation between the scores of the VASP and the BPRS at the corresponding four time points are given in Table 3. Pearson’s correlation coefficient revealed a statistically significant correlation at each time point between the total VASP score and the BPRS. There was also a statistically significant correlation between all five subdomains of the VASP and BPRS at midterm, postgroup, and follow-up. There was also a statistically significant difference in social skills between groups when those who had only one inpatient stay were compared with those with multiple inpatient stays (F = 4.82, P = 0.001). There was no statistically significant association between social skills and response to drugs, type of drugs given, or duration of treatment.
Correlation Between BPRS and VASP Scores at Four Time Points
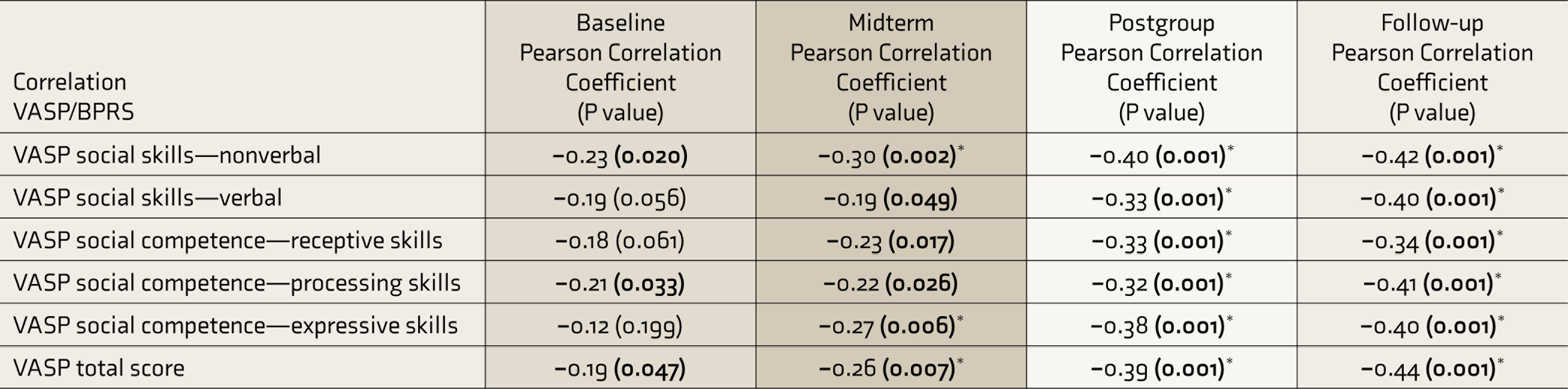
VASP: Vellore Assessment of Social Performance, BPRS: Brief Psychiatric Rating Scale. *Correlation significant at the 0.01 level. Bolded values: Correlation significant at the 0.05 level.
Comparison Between Social Skills and Clinical Variables
There was a statistically significant difference between diagnostic groups in overall social skills only at baseline (F = 4.54, P = 0.036) and not at the other three time points. When the subdomains of social skills were compared between diagnoses, the domain of social competence—expressive skills—had statistically significant difference between groups at baseline (F = 7.05, P = 0.009), midterm (F = 5.79, P = 0.018), postgroup (F = 4.91, P = 0.029), and follow-up (F = 4.47, P = 0.037). The subdomain of social skills—verbal—had a statistically significant difference between groups at baseline (F = 6.07, P = 0.015) alone. The other subdomains did not have statistically significant differences between the diagnostic groups.
Comparison Between Social Skills and Demographic Variables
There was a statistically significant difference in social skills when compared with the educational status of participants (F = 3.29, P = 0.006). There were no statistically significant correlations or associations between social skills and the characteristics of age, duration of illness, socioeconomic status, marital status, or employment status of the participants.
Discussion
This pragmatic study aimed to evaluate the effectiveness of an SST program conducted as part of routine clinical care. The protocol for the program has been modified over the years, based on clinical experience and available evidence. Group-based SST has been suggested as a cost-effective alternative to individual therapy in resource-constrained settings. 11 Group-based interventions also have the advantage of peer support and feedback, which has been shown to improve generalization of skills into real-life situations. 3 The component of generalization in the ten-step program enables therapists to empower caregivers to facilitate skills learnt in therapy to actual life situations. The final step of independent practice allows therapists to assess if the participant and caregiver have been able to implement the discussed strategies between sessions. In the absence of a community-based skills program, which necessitates the participants to travel out of state for accessing services, these strategies seem to partially bridge the gap between training and generalization. The provision of training in context-specific situations, with involvement of family, is also recommended for long-term maintenance of skills even after cessation of the intervention. 3 The outcome measure used to evaluate social performance is also a context-specific, performance-based measure routinely employed in clinical practice, which fulfills another recommendation from systematic reviews on SST. 11
The major target areas of the intervention were basic nonverbal and verbal social skills. Nonetheless, analysis reveals that participant scores improved across all five subdomains of the VASP: social skills—nonverbal and verbal; and social competence—receptive, processing, and expressive skills. We assume that the ten-step model of the sessions, using corrective feedback and discussion of problem-solving ideas within the group, followed by supervised practice in life situations, would have helped improve the cognitive processes underlying social competence. This is supported by systematic reviews that suggest that broad-based SST interventions can indirectly target and subsequently improve social-cognitive outcomes. 16
There was no statistically significant difference between those with schizophrenia and BPAD in overall social performance except at baseline. The subdomain analysis also revealed no differences in four of the five subdomains. There was a statistically significant difference between participants with schizophrenia and BPAD in the expressive domain of social competence, consistently, at four time points. It has been hypothesized that in people with schizophrenia, cognitive deficits added onto negative symptoms of affective disturbances and anhedonia can also limit the expression of social behavior. 3 There is also some evidence for greater benefit with SST when focusing on social cognitive domains 17 and for SST improving negative symptoms. 18 Since the number of participants with BPAD was less in the sample, we did not do further analysis. However, recent studies have found social cognitive deficits in persons with BPAD, even in remission, and have suggested early remediation programs. 19 This could explain the lack of statistically significant difference between diagnostic groups. Further studies comparing social skills deficits between schizophrenia and BPAD would have clinical implications in planning diagnosis-specific SST interventions.
The statistically significant negative correlation between psychopathology and social performance at all four time points is not surprising as there is good quality evidence for SST having a favorable effect on psychopathology.11,17 We also found statistically significant differences in social skills compared with the number of previous inpatient admissions, which can be a proxy indicator of the severity of illness. However, we did not find a statistically significant relationship between other clinical indicators like duration of illness, duration of treatment, type of drug taken, or response to drugs. This finding is contrary to findings from recent systematic reviews, which report a few studies concluding that SST can reduce relapse rates and rehospitalizations when compared with standard care. 11
Clinical and Research Implications
SST for SMI has evolved over the years from broad-based interventions to targeted interventions focusing on specific areas of social and neurocognition, with good quality supportive evidence.11,16,17 Given the culture-specific nature of social skills and the evidence base supporting SST, studies from India in this area are negligible. Our study shows not only that social skills deficits are prevalent in people with SMI, but also that the deficits can be mitigated with short-term, hospital-based training. The effect of other symptoms like cognitive deficits, motivational states, and psychotic symptoms also need to be considered while planning interventions, to optimize improvement with training. Recommendations for future research would also be to consider the effect of issues comorbid to SMI, like substance use, obsessive-compulsive traits, and intellectual disability, on social skills. Although we excluded people with acute psychosis, this is not an absolute contraindication for SST. 17 In resource-scarce settings, when waiting for the remission of psychotic symptoms is not feasible, initiating SST early on in the disease process could also be considered. The favorable effect of SST on long-term clinical outcomes like relapse and rehospitalization rates, which subsequently reduces disease burden and improves quality of life, is also a potential area of study.
Limitations
Owing to the pre–post design of this study, methodological limitations like lack of a control arm, lack of blinding, and issues related to confounders and cointerventions have to be considered while generalizing the results. The period of intervention is relatively less when compared with similar interventions that last up to months. The short follow-up period of two weeks during the inpatient stay itself is also a limitation as we could not assess how participants fared after going home. We did not look into premorbid characteristics, cognitive deficits, or negative symptoms, which could impact social skills. Since we could not find indexed publications on SST from India, we recommend similar studies across various cultural contexts with more robust designs.
Conclusion
This study supports the effectiveness of a hospital-based SST group protocol in improving the social performance of persons with SMI. We believe that this study demonstrates the feasibility of a multiple-stakeholder-involved program that can be implemented as part of routine clinical care and not just employed for research purposes. Since conducting multicenter clinical trials might not always be possible in resource-constrained settings, this study might be considered preliminary evidence for context-specific, peer/family supported SST.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
The authors would like to express their gratitude to all the participants for their time and willingness to be part of this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was approved and funded by the Institutional Review and Ethics Board, Christian Medical College, Vellore (IRB Min. No. 10901). The funding source had no further involvement in the conduct of the research or preparation of the article.