
Abstract
Family accommodation (FA) is prevalent in obsessive-compulsive disorder (OCD). When patients refuse treatment, the impacts are more severe—with poorer clinical outcomes, greater FA, and more caregiver burden. In these cases, caregiver interventions are an essential clinical priority. However, clinical documentation of structured, culturally informed interventions for FA and caregiver burden for adults with OCD, in the absence of patient participation, remains limited. This case study describes an eight-session caregiver-focused intervention for a 26-year-old male experiencing burnout while accommodating his twin sister with OCD, who was refusing treatment. The intervention, grounded in cognitive–behavioral principles, targeted maladaptive caregiving patterns, reinforced boundary-setting, and facilitated shifts in caregiver behaviors and family routines. Post-intervention assessments indicated reductions in FA and emotional distress, with gains maintained at the one-month follow-up. This case highlights the feasibility and clinical utility of caregiver-directed approaches in adult OCD. It underscores the need for structured support for caregivers in collectivist cultures and suggests that even indirect interventions can disrupt symptom-maintaining cycles and promote systemic well-being.
Keywords
Obsessive-compulsive disorder (OCD) is a chronic and functionally impairing condition. First-line treatments, such as cognitive– behavioral therapy (CBT) with exposure and response prevention (ERP) and pharmacological interventions, are empirically supported. 1 However, many individuals remain resistant or ambivalent toward formal treatment. In such instances, the responsibility of managing symptoms often falls on family members, who are expected (implicitly or explicitly) to adapt to the individual’s evolving symptom patterns. The majority of family members report engaging in such behaviors, particularly in collectivistic settings such as India. 2 Family accommodation (FA), defined as the modification of routines or direct involvement in compulsions to reduce the individual’s anxiety, is highly prevalent and linked to poorer treatment response, symptom persistence, and increased caregiver burden.3,4
There is a subgroup of people who do not take treatment and whose behavior may be perpetuated and worsened by FA. 5 Caregiver-focused interventions are relevant here, particularly in sociocultural settings with blurred emotional boundaries, as in many Indian households. However, clinical documentation of structured, culturally informed interventions involving family members of adults with OCD, especially in the absence of patient participation, remains limited. 6 This article addresses that gap by presenting a caregiver-directed intervention focused on reducing accommodation within the Indian context, illustrating both its process and potential when direct treatment is not viable.
Case Context and Method
This study presents a sibling-focused case example from a tertiary care mental health setting in India, illustrating the application of a structured caregiver-directed intervention to address FA in OCD where the patient refuses treatment. The intervention was delivered over eight sessions, focusing on modifying malada-ptive caregiving patterns, reinforcing boundary-setting, and promoting observable changes within the family’s behavioral contingencies and caregiver responses within a collectivist cultural context.
Case Description
V, a 26-year-old male software engineer, presented with stress and caregiver burnout due to supporting his twin sister, W, who was diagnosed two years prior with OCD, as per the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM–5). 7 W had completed her MBBS degree under psychological strain, with extensive support from V. Her symptoms began after witnessing a patient’s death from an ICU-acquired infection, leading to obsessions with contamination and compulsions including ritualistic hand washing, cleaning, and avoidance. These behaviors intensified with time, impairing her academic and social functioning. She became essentially homebound, with minimal activity and little motivation for further study or employment. At initial contact, her Yale–Brown Obsessive-Compulsive Scale (Y-BOCS), 8 score was 28, indicating severe OCD, with poor insight and high avoidance. Though fluoxetine (40 mg/day) initially helped, adherence was inadequate, and she showed little motivation for therapy. She resisted both pharmacological and psychological treatments, citing a lack of perceived need.
Case Formulation and Treatment Plan
V presented for psychological consultation due to growing emotional exhaustion and a decline in his quality of life. He reported pervasive irritability and increasing difficulty in managing his personal and occupational responsibilities. While working remotely in the IT sector and residing with his family, V gradually assumed a central caregiving role for W. He provided reassurance, engaged in proxy rituals (e.g., cleaning), adjusted routines to avoid triggers, and deferred personal tasks to manage W’s distress. Over time, these accommodations caused family tension and interpersonal conflict. The family stopped attending social events due to self-stigma and fear of public incidents related to W’s condition.
Assessments
V did not meet diagnostic criteria for any mental disorder in the DSM-5 classification system. Still, he scored 32 on the Family Accommodation Scale - Interviewer Rated (FAS-IR), 9 indicating high levels of accommodation, and the Depression Anxiety Stress Scale (DASS-21) 10 suggested moderate emotional distress with the doubled subscale scores of 16 on Depression (moderate range), 6 on Anxiety (normal range), and 22 on Stress (moderate range). These findings indicated significant emotional dysregulation stemming from his caregiving role, in alignment with existing literature.11,12
Treatment Plan and Goals
Given W’s refusal to engage in treatment, a caregiver-focused intervention was developed for V and delivered across eight weekly, hour-long sessions. The protocol was informed by evidence-based approaches drawn from psychoeducation and accommodation-focused, CBT-informed caregiver intervention, with adaptations to suit the current context.13,14 The intervention was aimed at educating V about FA’s role in OCD maintenance, fostering healthier relational dynamics, and gradually reducing enabling behaviors, thereby enhancing his psychological and emotional functioning.
General Framework
Each session typically involved reviewing homework, discussing challenges, and recapping previously introduced skills to ensure that V understood the rationale. Feedback was encouraged to clarify therapeutic concerns and comfort.
The Course of Treatment and Monitoring of Treatment Progress
Session 1: Psychoeducation and Case Formulation
It focused on building rapport and orienting V to the structure and goals of therapy. History was clarified, and psychoeducation was provided on OCD using a cognitive–behavioral model tailored to W’s symptom profile. V’s accommodative behaviors were labeled as such, with discussion on how they can act as a maintaining factor in the OCD cycle. V’s responses, previously viewed as supportive, were reframed as neutralizing behaviors that reinforced W’s contamination fears. The lack of distinction between supporting W through her difficult times and “accommodating” was noted. Homework included reflecting on these concepts, articulating therapy goals, and summarizing his understanding of the OCD-accommodation feedback loop.
Session 2–3: Mapping Accommodation Patterns
A detailed behavioral chain analysis was conducted to deconstruct typical episodes of accommodation. V identified antecedents, specific accommodative behaviors, and their short- and long-term consequences. A self-monitoring log was introduced to track instances of FA and associated triggers. The following week’s session built upon his entries in this log to identify both internal cues (e.g., guilt, fear of conflict) and external pressures (e.g., direct requests, parental persuasion). Challenging V’s belief that accommodation equated to care increased his insight and readiness for change. Cognitive flexibility was facilitated through reflection on the unintended reinforcing effects of accommodation.
Session 4–5: Modifying Caregiving Beliefs
The agenda was to shift V’s focus from relieving W’s distress to helping her tolerate it, thereby reframing his caregiving goals. Through Socratic questioning, assumptions like “If I don’t help, she’ll break down” and “She needs me to function” were identified and gently challenged. Additional columns were added to his behavioral log to help record alternative, value-consistent, non-accommodative responses. The following week, V returned feeling discouraged. He expressed doubts about the efficacy of the intervention. His initial attempts led to increased conflict (with W and their parents), reinforcing earlier fears of not accommodating. These reactions were normalized as expected responses during behavior change, which might delay but not prevent progress. Graded exposure to low-risk non-accommodation was initiated (e.g., delaying reassurance, allowing W to manage rituals independently), reinforcing V’s agency and commitment to change.
Session 6: Promoting Behavioral Change
V attended the sixth session and reported a sense of accomplishment. He reported increased efficacy in using assertive communication strategies and greater emotional regulation following refusal to accommodate. To rehearse boundary-setting while maintaining empathy, role-plays were conducted to simulate common scenarios involving W and to practice new responses. During the discussion of the home situation, the therapist observed emerging patterns. While W sometimes tolerated his refusal, she often redirected requests to other family members, especially their mother. With consent, V was asked to initiate a discussion with his parents about FA to align family responses. A conjoint meeting was proposed to address systemic accommodative patterns.
Session 7: Systemic Family Engagement
Although W declined participation, their parents joined V for a conjoint session. The therapist facilitated a discussion on how caregiving had become disproportionately focused on W’s needs, often at the expense of the family’s well-being. Psychoeducation was provided on the cyclic interaction between obsessions, compulsions, and accommodation. The mother shared that her accommodative behaviors stemmed from a fear of escalation and a wish to maintain household harmony, reflecting both emotional concern and apprehension about conflict. Her ambivalence toward change was acknowledged and validated. The therapist reframed accommodation as an understandable but unhelpful attempt to manage distress, and collaboratively explored alternative caregiving strategies. An alternative view of care (based on emotional presence, encouragement, and shared activities) was introduced. Gradual behavioral commitments were identified, such as delaying immediate reassurance, allowing W to manage her cleaning routines independently, and planning short shared family activities to reintroduce positive interactions. A shared understanding of consistent boundary-setting across caregivers was emphasized to support W’s autonomy while protecting family well-being. Self-stigma related to W’s condition was addressed. The family was encouraged to re-engage with personal and shared activities to model functional coping and re-establish balance in family roles. The session concluded with the parents expressing readiness to implement small, sustainable changes.
Session 8: Consolidation and Relapse Prevention
The concluding session involved a comprehensive review of the therapeutic progress. V reported increased self-awareness, improved boundary-setting, and reduced distress linked to accommodation. He noted that W’s demands had become less frequent and urgent, likely due to more consistent family responses. This insight was used to focus on sustaining gains through values-based, long-term goals. Potential triggers for renewed accommodation were identified, and learned skills and alternative responses were reviewed and practiced. Continued family coordination was also encouraged.
An additional follow-up session was conducted one month after the conclusion of the primary intervention phase to assess progress.
Challenges in Intervention
One of the earliest and most persistent challenges in the intervention was building a conceptual distinction between caregiving and accommodation. V’s strong sense of responsibility and concern for W’s distress led to feelings of guilt when setting boundaries, particularly during initial attempts at behavioral change. Psychoeducation and Socratic dialogue were used to foster dissonance between well-intentioned help and symptom-reinforcing accommodation. This shift was essential in developing V’s readiness for change. Similar conversations were required with the parents, especially the mother, who continued to equate accommodation with emotional support and caregiving. The lack of consistency in boundaries across caregivers periodically undermined V’s efforts, necessitating focused work on family alignment and encouraging unified responses to W’s compulsive demands. Addressing the entrenched relational patterns and self-stigma motivated the family to resist reverting to their long-standing roles and to question the validity of their beliefs.
Another key barrier was W’s poor insight and active resistance to change. Despite not being part of the intervention, her distress escalated when V reduced his accommodating behaviors. These responses led to intermittent relapses in accommodation, driven more by conflict avoidance than conviction. Additionally, V’s motivation dipped when his efforts did not yield visible changes in W’s functioning and instead contributed to interpersonal strain. These moments were addressed through validation, empathic listening, and by reinforcing the long-term goals of the intervention. It was highlighted that although W’s functioning did not improve despite V’s refusal to accommodate (an erroneous expectation), it also did not deteriorate, which had been V’s initial fear and the primary reason for the previous accommodation. Structured problem-solving strategies, communication skills training, and graded boundary-setting were instrumental in rebuilding V’s confidence in navigating setbacks. Setbacks were also normalized as part of the process of achieving sustainable behavioral change. Across the sessions, V gradually reported increased confidence in managing his responses and a shift from reactive to proactive caregiving.
Therapist and Relational Factors
Several relational considerations shaped the therapeutic process in this case. Building trust with V required balancing the validation of his caregiving efforts with the gentle challenge of maladaptive patterns. The therapist maintained an empathic-neutral stance, acknowledging cultural values regarding family responsibility while encouraging boundary -setting as an act of care rather than as a form of withdrawal. Consistency, transparency regarding therapeutic goals, and paced introduction of behavioral changes helped manage V’s initial ambivalence. Rapport was also extended to V’s parents during conjoint sessions, emphasizing collaboration rather than directive instruction.
Treatment Outcome
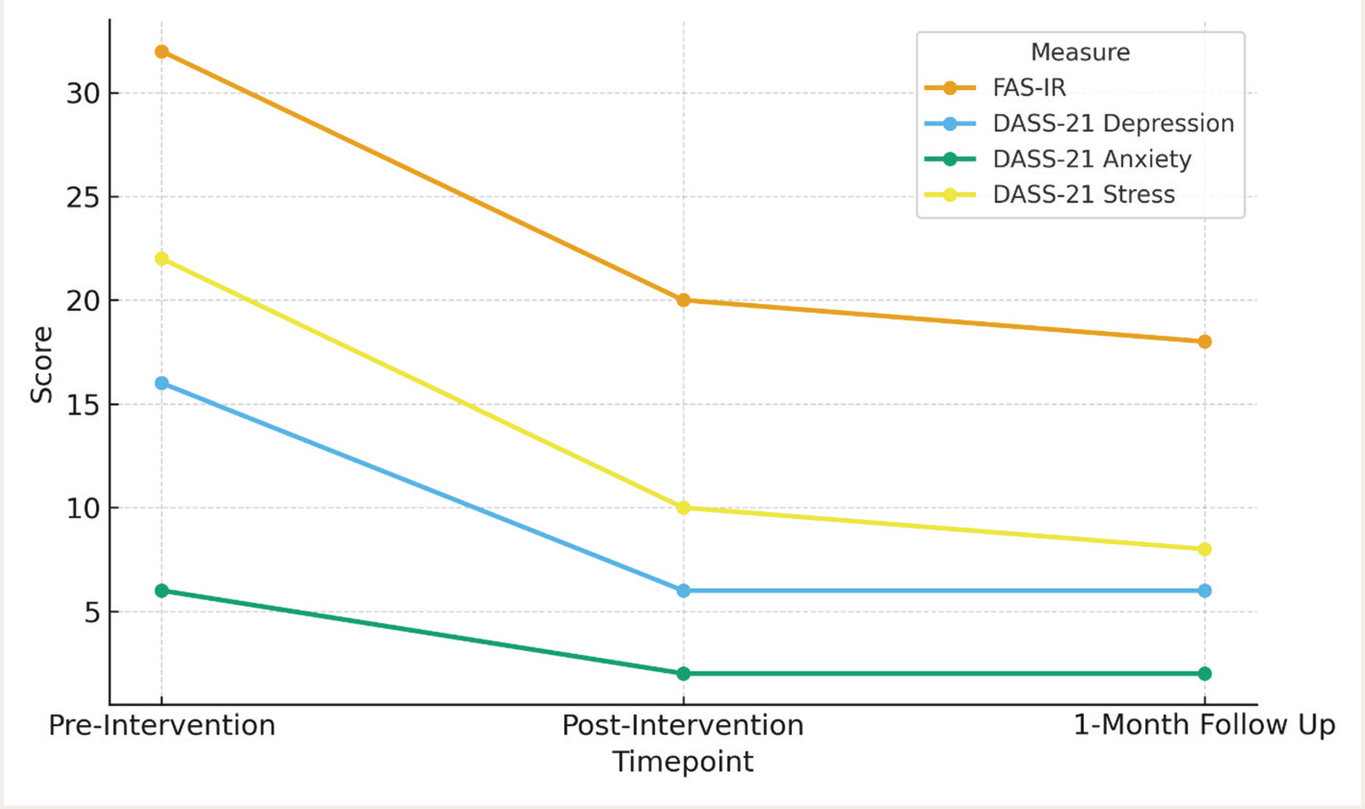
At the end of the 8-session intervention, V was reassessed using the FAS-IR and the DASS-21. His scores on both scales decreased from baseline, suggesting significant behavioral change and improved emotional well-being. These gains were maintained at the 1-month follow-up session. V reported reduced time spent performing proxy compulsions, less frequent reassurance giving, and a shift toward boundaried engagement with W. The outcome measures are represented in Table 1 and Figure 1.
Scores on Family Accommodation and Emotional Functioning Across Timepoints.
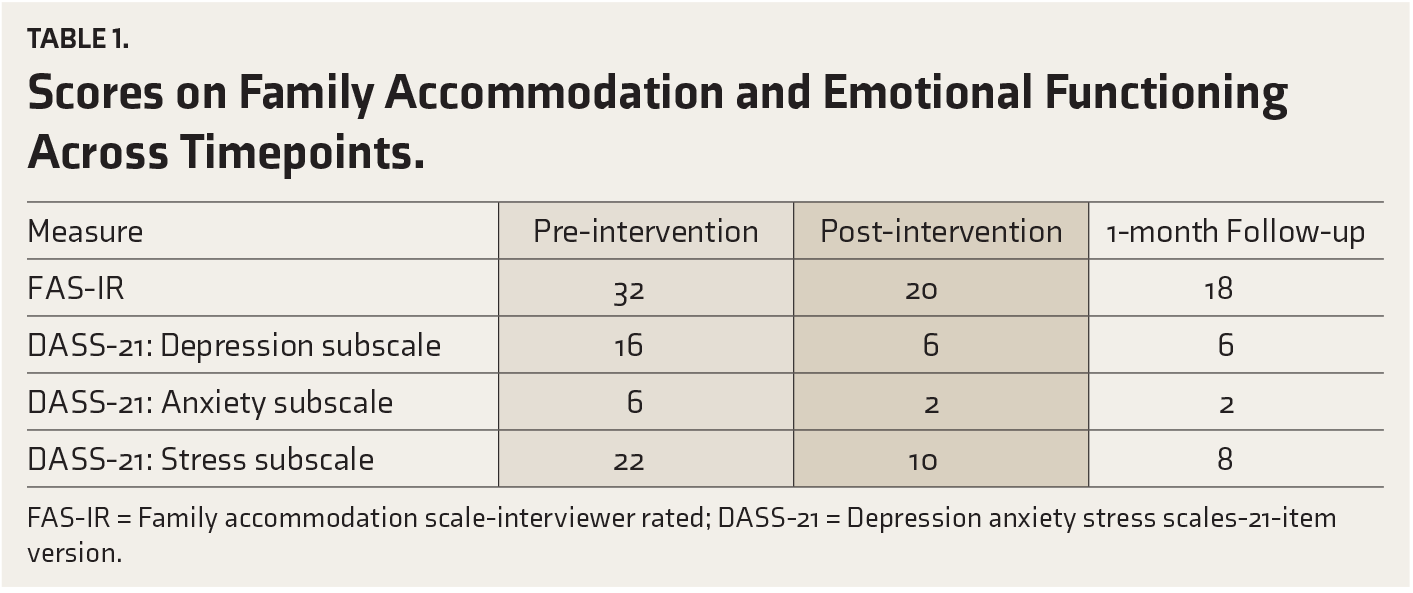
FAS-IR = Family accommodation scale-interviewer rated; DASS-21 = Depression anxiety stress scales-21-item version.
FAS-IR = Family accommodation scale-interviewer rated; DASS-21 = Depression anxiety stress scales-21-item version.
Subjectively, V described a greater sense of personal autonomy, improved focus during his remote work hours, and resumption of previously abandoned leisure activities, including regular exercise and social contact with peers. He also noted improved emotional regulation when faced with W’s distress and was better able to tolerate temporary conflict without reverting to accommodation.
No objective post-treatment Y-BOCS data for W were available; therefore, patient-level changes are reported as collateral observations only. Although W’s OCD symptoms persisted, V observed a slight increase in her independent functioning, including initiating certain hygiene rituals without external support and tolerating minor disruptions in routine.
Discussion and Limitations
This case demonstrates the clinical utility of caregiver-focused interventions in OCD, even when the patient remains uncooperative. While the central features of OCD remained untreated directly, the intervention led to improved caregiver functioning, as seen in trials demonstrating the efficacy of FA-focused family modules.3,15 Despite W’s consistent refusal to engage in treatment, V reported reduced emotional distress and decreased participation in symptom-reinforcing behaviors. His functional gains in work, social interactions, and self-directed caregiving underscore the potential for systemic improvement when environmental contingencies are modified, irrespective of the patient’s direct involvement.
Several contextual factors likely facilitated the relatively rapid gains in this case. V’s strong motivation for help-seeking, a flexible remote work schedule that enabled consistent session attendance, and a commitment to homework contributed to steady progress. The family’s willingness to participate in a conjoint session further enhanced alignment between the caregivers and reinforced therapeutic change. These factors underscore the role of individual readiness and contextual support in optimizing outcomes in caregiver-focused interventions.
The intervention is particularly relevant in the Indian sociocultural context, where caregiving is often deeply tied to emotional interdependence and stigma surrounding mental illness.6,11 Within this context, the sibling’s role is rarely addressed in clinical practice or literature. V’s struggle to set boundaries was initially compounded by guilt and familial pressure to maintain harmony. However, with psychoeducation and structured therapeutic input, he began to shift from reactive accommodation to intentional, values-consistent caregiving. This reorientation was crucial not only for V’s emotional health but also in laying the groundwork for shifts in caregiver behaviors and family routines.
This case adds to emerging evidence that working with family members alone can yield meaningful outcomes, especially when OCD symptoms are severe, and insight is limited.5,16 Reductions in accommodation may catalyze the patient to confront distress independently and potentially become more open to treatment in the future. In V’s case, small changes in his behavior appeared to introduce friction into the symptom-maintaining cycle, an uncomfortable but necessary precursor to longer-term change. Importantly, these shifts were not aimed at reducing symptoms in W, but rather at empowering V to reclaim his own life and, in doing so, modify environmental contingencies related to the disorder.
While outcomes were encouraging, several barriers, such as inconsistent caregiver implementation, early dips in motivation, and patient hostility, underscore the need for paced implementation and family-wide engagement. The case illustrates that caregiver distress deserves clinical attention in its own right. Helping oneself is often the first step toward helping others effectively. Future directions may include readiness-focused approaches with the patient and the expansion of caregiver-focused modules to more actively engage the wider family system.
Limitations
The caregiver-focused intervention was tailored to V’s specific context, making it challenging to assume similar outcomes in different family dynamics or cultural settings. Given the single-case study design, the findings are inherently limited in their generalizability. Additionally, without W’s active participation, objective measures of her symptom change (such as post-intervention and follow-up Y-BOCS scores) were unavailable. This limits the ability to quantify indirect effects on the patient, relying instead on caregiver reports that may be subject to subjective bias. The focus on relational and systemic factors, while clinically valuable, also restricts causal inferences regarding the intervention’s efficacy. Also, the absence of a formal assessment of caregiver quality of life, which is often impaired,12,17 limits a more comprehensive view of change in well-being, role functioning, and relational balance. Future case reports may consider incorporating it to strengthen outcome evaluation.
Implications and Recommendations
Implications for Clinical Practice and Theory
This article is an essential addition to the emerging discourse on caregiver-focused interventions for OCD, especially in contexts marked by treatment refusal and with entrenched FA. By focusing on the often-overlooked role of a primary caregiver, the intervention demonstrated that meaningful change is possible even without direct patient involvement. Within the Indian familial context, where caregiving often emerges from close emotional interdependence and limited formal support systems, structured interventions for caregivers can help address systemic gaps in mental health service delivery. By equipping family members with skills to manage distress and set functional boundaries, such approaches can foster healthier relational patterns and create conditions conducive to eventual patient engagement.
Implications for Research
Future research should systematically evaluate the efficacy of caregiver-only interventions across diverse sociocultural contexts using larger sample sizes and controlled designs. Specifically, studies could examine whether reductions in FA resulting from caregiver interventions indirectly affect changes in patient symptom severity, insight, or treatment engagement.
Reporting Guideline (uploaded as
Conclusions
A structured intervention focusing on caregivers and aiming to reduce family accommodation can decrease caregiver distress and harmful accommodation behaviors, even if the person with OCD does not want treatment. Supporting caregivers, including siblings, may also help break cycles that maintain symptoms and enhance the family's overall functioning, especially in cultures with strong family ties.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
The authors assume full responsibility for the content of the manuscript and wish to clarify that, although no part of the manuscript was written using AI, Grammarly and its generative AI features were used during editing.
Ethical Approval
The study has received ethical clearance from the NIMHANS Institutional Ethics Committee (IEC)- No.NIMH/DO/BEH.Sc.Div./2023-24.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study is part of the ongoing PhD thesis of the first author, who receives a fellowship from the University Grants Commission (UGC-JRF, NTA Reference No.-190510217317).
Informed Consent
The caregiver (V) provided informed consent for his participation in treatment and for publication. The patient (W) declined involvement in treatment; she did not undergo therapeutic assessments. However, she consented to the publication of anonymized, de-identified clinical details.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.