
Abstract
Background:
The mental health (MH) treatment gap in India is particularly pronounced in underserved and rural areas. Community Health Officers (CHOs) play a crucial role in addressing this gap at the primary care level. A pan India digitally driven MH capacity-building program was designed to integrate MH care into primary care settings by training CHOs and supporting them through Collaborative Video Consultations (CVCs). We aimed to examine the profile of MH cases through CVCs by CHOs trained under a pan-India, digitally enabled MH capacity-building program, and to describe the diagnostic patterns and types of handholding provided across three Indian states.
Methods:
This cross-sectional study analyzed 591 CVC records from CHOs of Karnataka, Maharashtra and Bihar from November 15, 2022 to July 31, 2024, who underwent a six-session online training program on MH care, followed by real-time video consultations with MH professionals for case discussions and patient management. Descriptive statistics and crosstabulations were used for data analysis.
Results:
Most CVCs were from adult patients aged 19–60 years (79.69%), with women more frequently identified with common mental disorders (CMD) (25.42%) and men more commonly having severe mental disorders (SMD) (12.20%) and substance use disorders (SUD) (16.61%). Among states, Bihar had the highest number of CVCs (38.92%). CHOs provided handholding through referrals, counseling, and follow-ups.
Conclusions:
The program demonstrated the effectiveness of CVCs in empowering CHOs to identify and manage MH conditions. The consultation-based collaborative model facilitated accurate diagnoses and timely interventions, bridging the MH treatment gap in rural and underserved regions. Continued investment in CHO training, digital infrastructure, and follow-up care is essential for sustaining the program’s impact on primary MH care.
Keywords
A digitally enabled, pan-India training program successfully equipped Community Health Officers (CHOs) with skills to identify and manage mental health conditions at the primary care level. Collaborative Video Consultations (CVCs) served as an effective tool for real-time support, capacity building, and case management between CHOs and mental health professionals. The integration of digital tools and continuous mentorship through CVCs presents a promising, sustainable model for strengthening India’s mental health delivery at the primary level.Key Messages
Primary care plays a crucial role in identifying and addressing mental health (MH) conditions, particularly in underserved areas. 1 Poor MH can significantly affect quality of life (QOL) and contribute to caregiver burden, financial strain, and individual functionality. 2 Enhancing the primary care/community health workers can attain universal health coverage and strengthen basic healthcare. However, the sufficiency and competency of the health personnel are significant issues for low- and middle-income countries (LMICs). 3
CHOs in Addressing the MH Gap
To improve the primary health care (PHC) system’s ability to provide a broader range of services, the Indian government has launched the Ayushman Bharat Health Comprehensive PHC throughout the country (in collaboration with the State Governments), where in more than 150,000 current subcenters and primary health centers are converted into Ayushman Arogya Mandirs (AAM) and have introduced a new cadre of Community Health Officers (CHOs). 4 A CHO may be a dentist, a nursing officer, or a physician with training in AYUSH. CHOs are often the first point of contact in the community for many health-related problems. Their roles and responsibilities include wellness, preventative care, outreach services, curative care, rehabilitative and palliative care, communication, and management. As part of providing integrative care, the CHOs have close collaboration with rehabilitation staff, Multipurpose Health Workers (MPWs), Mental Health Care Providers (MHCPs), and Accredited Social Health Activists (ASHAs). 5 As regards mental healthcare, however, they are often undertrained, leading to difficulty in recognizing and treatment provision.
Integration of MH into Primary Care
Considering the pivotal role the newly emerged cadre CHO plays in health and wellness, a pan-India digitally driven MH capacity-building program was completed that contributed to integrating MH care into the broader framework of Comprehensive Primary Health Care (CPHC), as envisioned under the Government of India’s Ayushman Bharat Health and Wellness Centre (AB-HWC) initiative. The program also incorporated an instant, live, Collaborative Video Consultation (CVC) model to support CHOs in case discussions, treatment planning, and decision-making, addressing barriers such as digital literacy and infrastructure challenges.6,7 This study examines the profile of CVCs by the CHOs who underwent training under this program.
Methods
This study was based on the analysis of CVCs conducted for CHOs in the states of Karnataka, Maharashtra, and Bihar who underwent online training as part of the program. These CVCs cover the period from November 15, 2022, until July 31, 2024. Using a quantitative methodology, the cross-sectional study examines primary data from CVC records in these states (file review method). The training program employed a six-session Zoom training format, trained by MH specialists from a tertiary care National Institute of Mental Health and Neurosciences (NIMHANS). All CHOs underwent online sessions covering common mental disorders (CMDs), severe mental disorders (SMDs), substance use disorders (SUDs), disaster preparedness, MH introduction, and the use of MERIT, a screening tool to identify priority MH disorders in primary care settings. 8 Additionally, they received orientation on Tele-Consultation through CVCs. The program employed a robust training methodology tailored to different cadres of healthcare workers, with modules delivered in English or regional languages through online sessions, adapted to each state’s context. Each session, spanning 120 minutes, ensured active participation and comprehension. A dedicated WhatsApp group facilitated communication and provided continuous support, while pre- and post-training assessments evaluated knowledge, attitude, and practice. Following training, participants received supportive handholding through CVC to uphold service quality. Detailed training program’s specifics, procedures, and modules are explained elsewhere (Multistate digitally driven capacity building program to strengthen Indian primary mental healthcare: An Overview, Shah et al. 2025). 9
Collaborative Video Consultations
The CVC process followed a structured methodology. It began with CHOs identifying patients during routine health visits or through referrals. Soon after, CHOs prepare the case by gathering relevant information, including demographic details, psychosocial context, and medical history. CVC is sought by trainee CHOs from MH professionals, such as psychiatrists, psychologists, psychiatric social workers, or psychiatric nurses. The MH professionals were available to the CHOs during working hours and occasionally for emergency cases, for discussion/advice. CHOs choose to discuss selected patients where they have difficulty in identification/referral for MH issues (instantly, live).
Soon after the CVC, an MH professional enters all clinical data in a specially designed proforma containing demographic details, diagnosis, and learning points. CHOs discuss several cases ranging from children to the elderly. CHOs were also actively involved in providing follow-up care to psychiatric patients who were already on treatment, presenting to emergencies with psychiatric disorders, and who needed psychiatric care, including counseling patients.
A total of 591 CVCs from the states of Karnataka, Maharashtra, and Bihar were included in the study; 23 CVC data were excluded due to insufficient information. The details collected from CVC performance, such as age, gender, marital status, occupation, present complaints, diagnosis category (CMD, SMD, SUD, OTHERS) based on ICD, and advice type (referral, counseling, medication, follow-up, and others) are all included in this. Informed consent was obtained from all participants before data collection. The study was approved by the Institutional Ethics Committee (IEC) (Approval No. NIMHANS/ 43rd IEC (BEH.SC.DIV) 2023, dated December 8, 2023) and registered with the Clinical Trial Registry of India (Registration No. CTRI/2024/02/062906). Data analysis was conducted using Microsoft Excel and SPSS. Descriptive statistics, including frequencies and percentages, were used to summarize the data. Cross tabulations were performed to explore relationships between categorical variables. Results were presented in the form of basic tables and graphical representations, such as bar charts, to provide a clear and concise visualization of the findings. The study followed the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) cross-sectional reporting guidelines to ensure transparency and completeness in the reporting of the research methods and findings. 10
Results
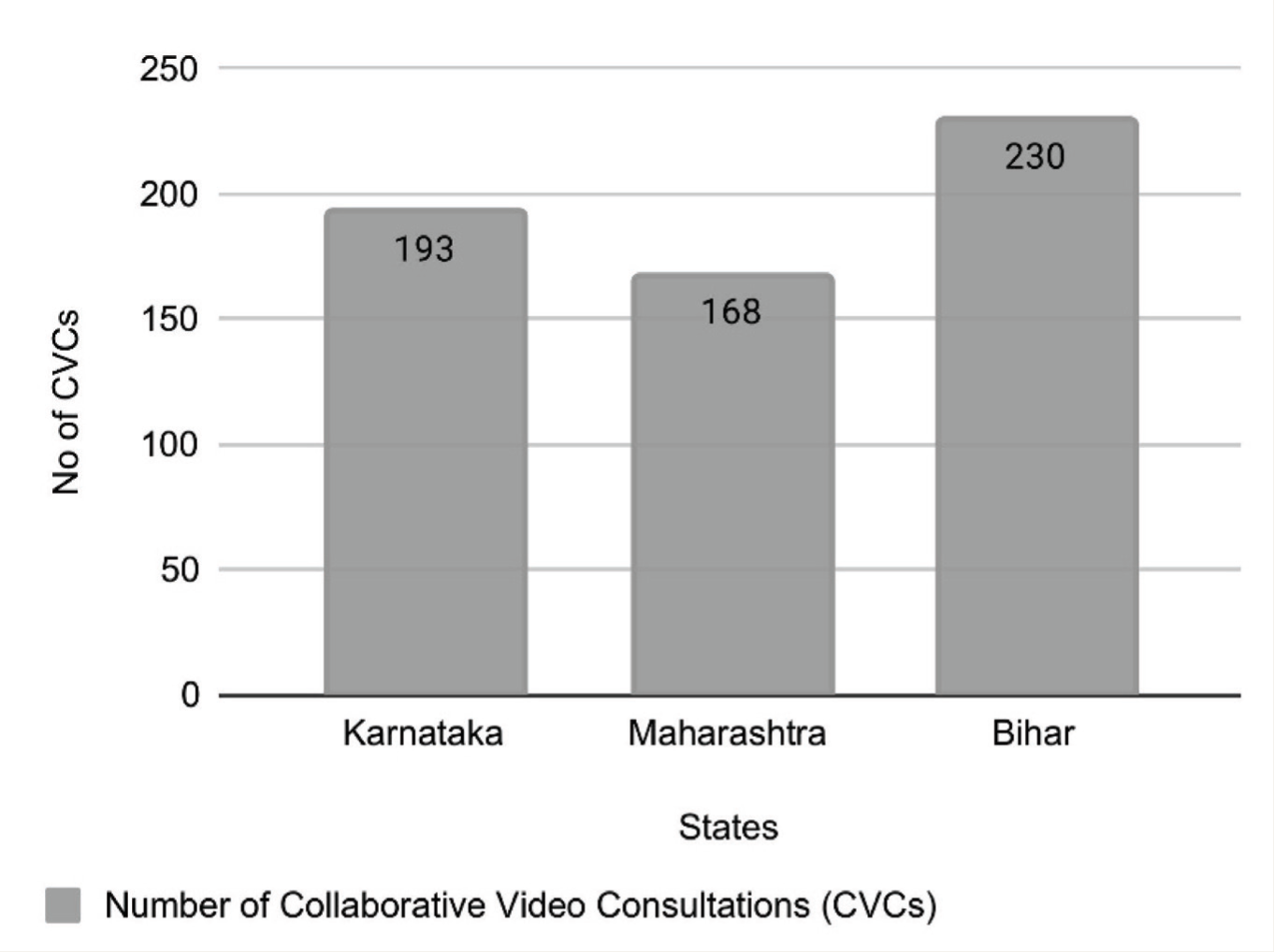
From the CVCs provided from November 15, 2022 to July 31, 2024, a total of 591 CVCs were included in the study. Bihar accounted for the largest percentage of the CVCs, with 230 consultations (38.92%), followed by Karnataka (193 cases, 32.66%), and Maharashtra (168 cases, 28.43%) (Figure 1). The age-wise distribution (Table 1) shows that the 19–39 age group is the highest, representing 44.50% (263 cases) of total cases, with Bihar leading at 49.57% (114 cases). The 40–60 age group follows, making up 35.19% (208 cases), particularly high in Karnataka (39.90%, 77 cases) and Maharashtra (39.88%, 67 cases). The above-60 age group constitutes 12.52% (74 cases). Overall, adults aged 19–60 represent most CVCs across all states. The gender distribution shows that males make up 54.82% (324 cases) of the total, with the highest in Bihar (62.17%). Females account for 45.18% (267 cases), with Karnataka having the highest female participation (52.33%).
State-wise Number of CVCs.
Age-wise Distribution of Collaborative Video Consultations (CVCs) by State.
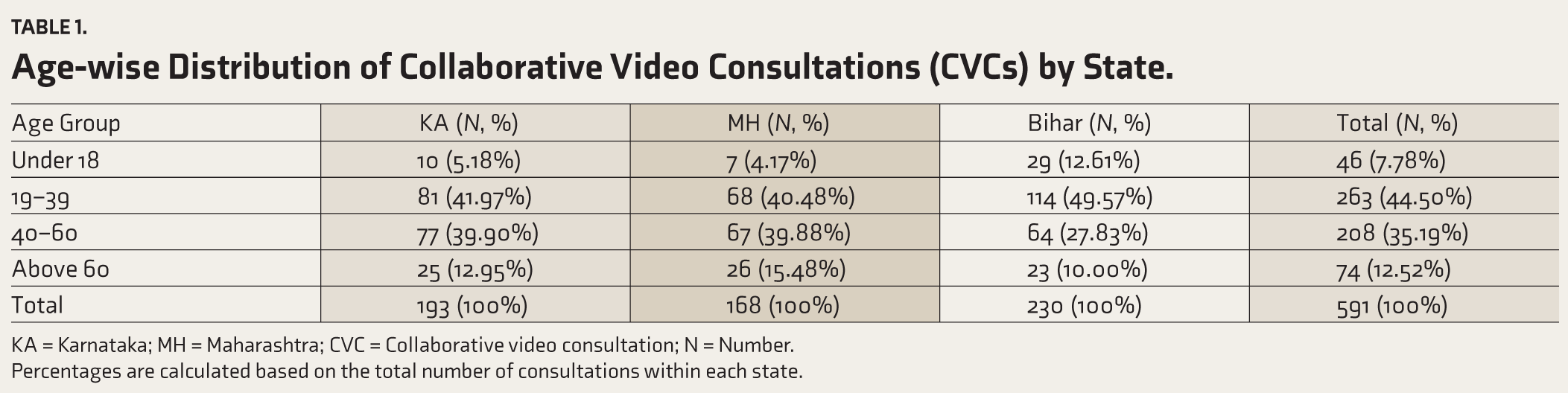
KA = Karnataka; MH = Maharashtra; CVC = Collaborative video consultation; N = Number.
Percentages are calculated based on the total number of consultations within each state.
There are significant differences in MH diagnoses based on gender and age, as shown in Table 2. The CMDs were more frequently diagnosed in women (25.42%), especially those aged 19–39. In comparison, men account for 15.76% of CMD cases, with a similar age distribution. Men are more likely than women to be diagnosed with SMD (12.20%), particularly in the 19–39 age group. SUDs are also more common in men (16.61%), especially those aged 40–60. These trends reveal that women are more often diagnosed with CMD, while men are more likely to be diagnosed with SMD and SUD, highlighting disparities linked to age and gender in MH.
Prevalence of Diagnosis Types Across Gender and Age Groups (n = 591).
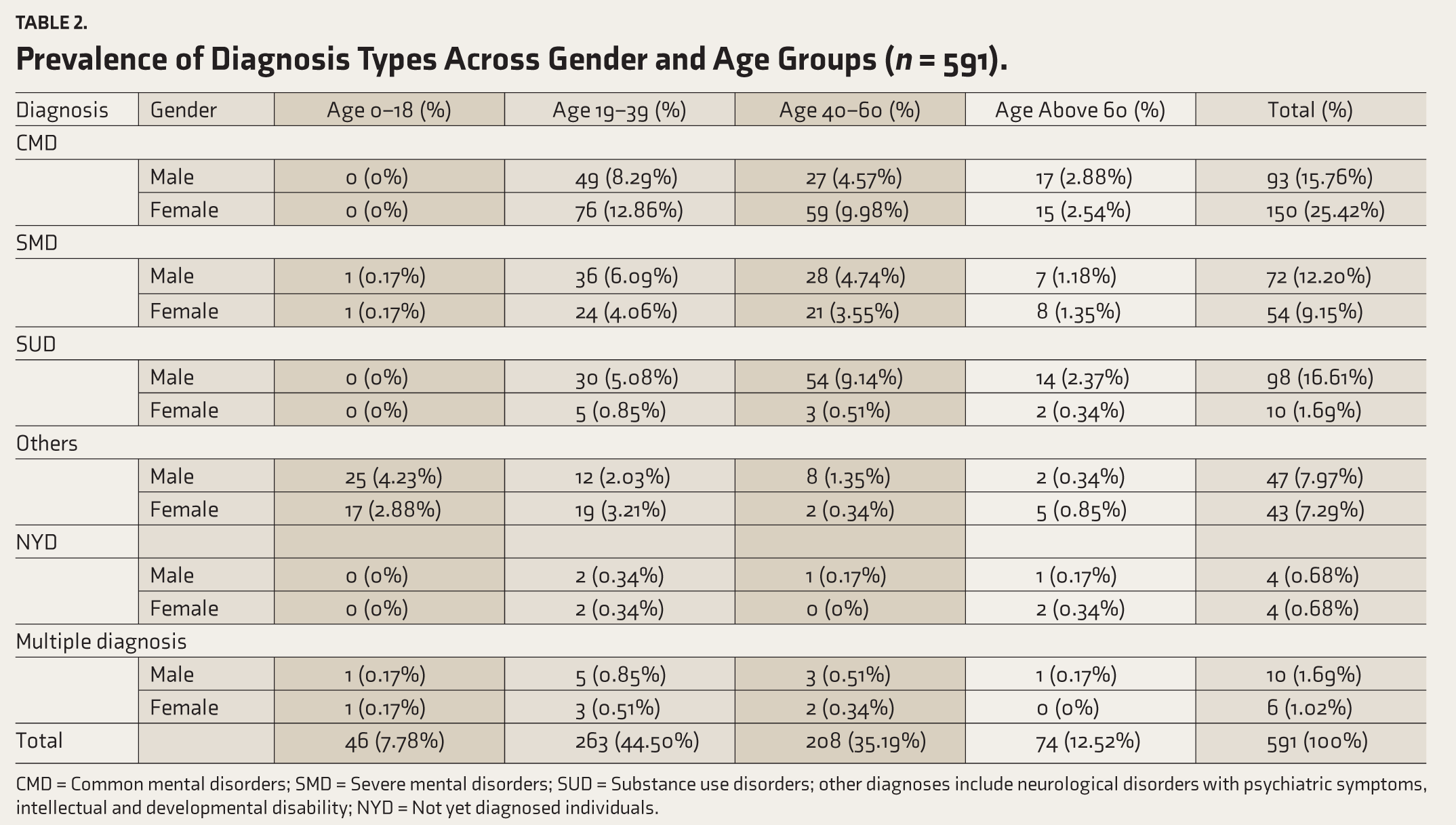
CMD = Common mental disorders; SMD = Severe mental disorders; SUD = Substance use disorders; other diagnoses include neurological disorders with psychiatric symptoms, intellectual and developmental disability; NYD = Not yet diagnosed individuals.
Important patterns in the CVCs are shown by the distribution of diagnostic categories in Karnataka, Maharashtra, and Bihar (see Figure 2). The CMDs were consulted by 41.62% of all. Among them, Karnataka had the most (50.26%), followed by Maharashtra (40.48%) and Bihar (35.22%). 21.32% have SMD, with Bihar having the highest percentage (22.61%). SUDs have 18.27%, with Maharashtra having the highest rate (28.57%). Bihar has the highest percentage of people in the other group (20.00%). SMD and SUD are also important, although CMD is the most common diagnosis overall.
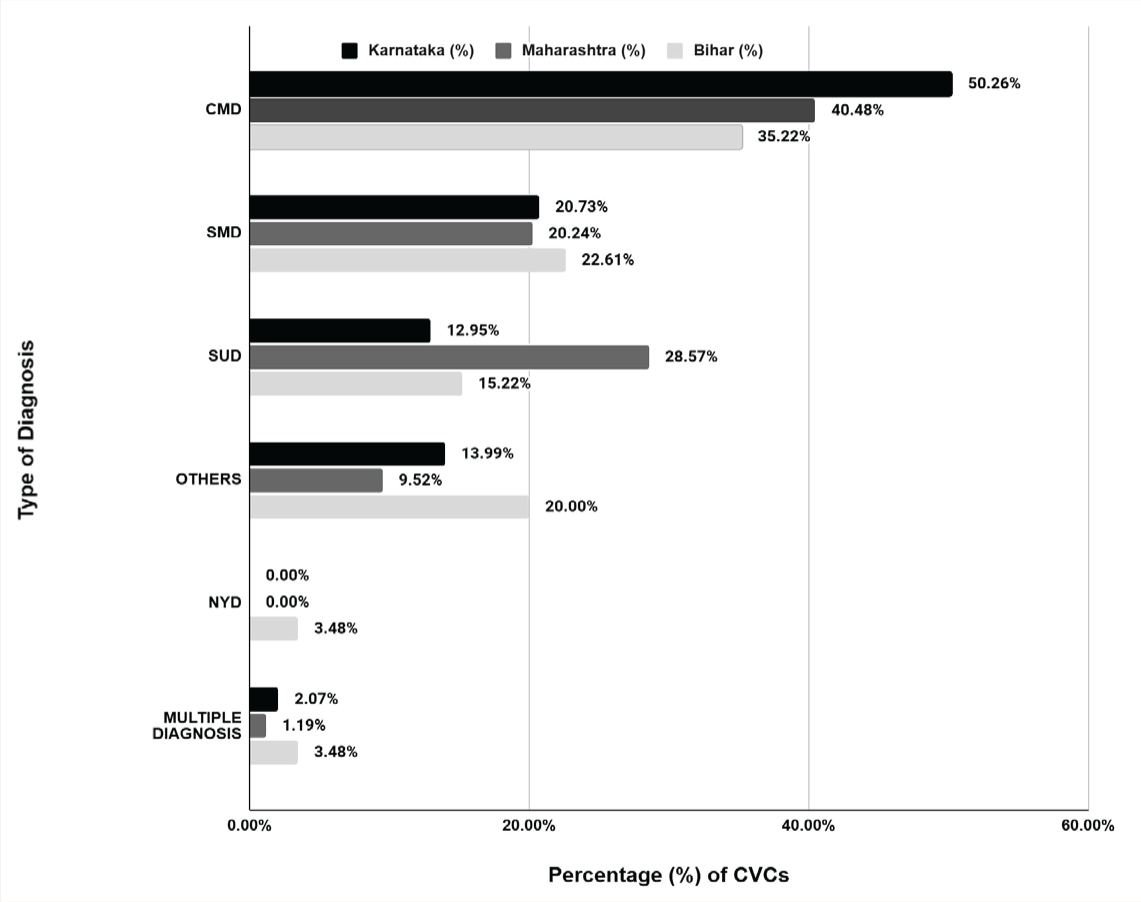
CMD = Common mental disorders; SMD = Severe mental disorders; SUD = Substance use disorders; NYD = Not yet diagnosed.
The results of handholding for CVCs in Karnataka showed that CMD had the highest referral rate at 50.60%, with significant attention also given to counseling (28.40%) and follow-ups (8.60%). In Maharashtra, follow-ups for SMD were the highest (58.60%) among all diagnoses. In Bihar, CMD had the highest follow-up percentage at 42.10%, while SMD had a significant counseling rate of 22.30%. The results indicate that CMD were the most frequently addressed condition across all three states, with significant emphasis on referrals, counseling, and follow-up care, particularly in Karnataka and Bihar. The overall trend highlights the need for more balanced care across MH conditions, with a particular focus on increasing referrals and follow-ups for SUD in all states (Table 3).
Distribution of Mental Health Diagnoses and Interventions Across States.
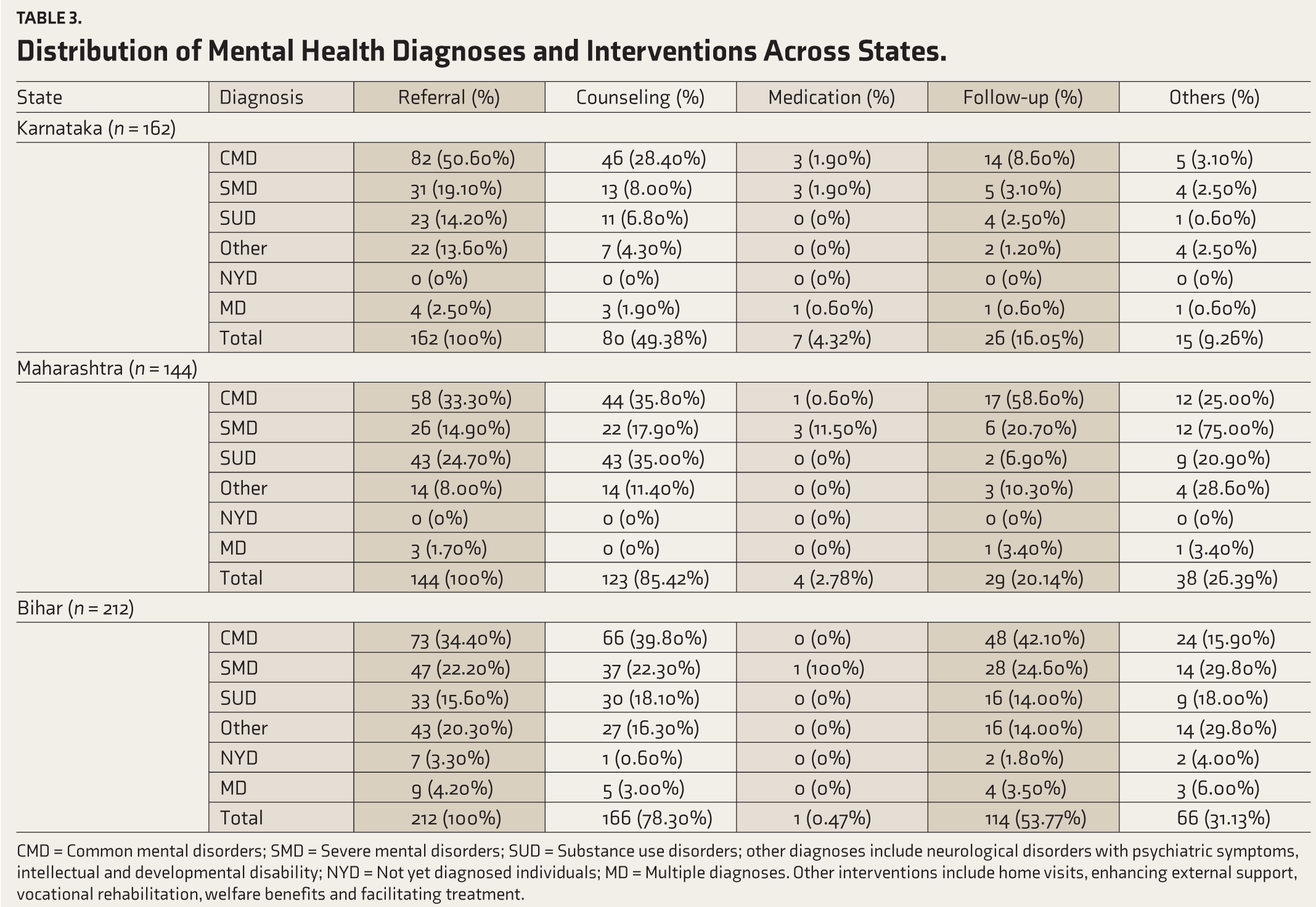
CMD = Common mental disorders; SMD = Severe mental disorders; SUD = Substance use disorders; other diagnoses include neurological disorders with psychiatric symptoms, intellectual and developmental disability; NYD = Not yet diagnosed individuals; MD = Multiple diagnoses. Other interventions include home visits, enhancing external support, vocational rehabilitation, welfare benefits and facilitating treatment.
Discussion
The findings of this study shed light on the role of CHOs in bridging the treatment gap for mental illness, particularly in rural and underserved areas, through the adoption of a digitally driven, instant CVC model. This program is a demonstration of the feasibility and efficacy of task-sharing types of approaches for MH care integration into primary care.
Significance of CVC in MH Delivery
The CVC model enables the collaboration between CHOs and MH professionals for the identification and timely management of commonly prevalent psychiatric disorders in primary care. This model is especially valuable in rural areas where there are limited MH specialists. The confidence of the CHOs increases as the CVC process includes preparing cases for discussion, real-time video consultations, and follow-ups, which in turn improves the accuracy of management of Psychiatric cases, including appropriate medication management, counselling, and follow-ups.11–13 This system can also facilitate early intervention, reducing the burden on the secondary and tertiary care system, and reducing the gap for MH care in the remote and rural areas.
Trends in Diagnosis and Interventions
The observation that CMDs accounted for most diagnoses, particularly among women aged 19–39 years (41.62%), aligns with previous research that highlights the vulnerability of women in this age group to CMDs, often due to stress, socio-cultural factors, and caregiving responsibilities. 1 Similar prevalence patterns have been reported in the National Mental Health Survey of India, 2015–2016, which found higher rates of CMDs such as depression and anxiety among women in the reproductive age group. 13 Studies conducted in low-resource settings have also demonstrated a disproportionate burden of CMDs among women.14,15 Conversely, SMDs and SUDs were more prevalent among men, especially in the 40–60 age group. This is supported by findings from the National Mental Health Survey (NMHS) and other epidemiological studies reporting higher prevalence of schizophrenia, bipolar disorder, and substance use, particularly alcohol and tobacco use, among middle-aged men.13,16 This gender and age-related disparity underscores the need for demographic-specific MH interventions and targeted programs for men in this age group. 17
The finding that CMDs are more frequently diagnosed in women, particularly those aged 19–39, is consistent with broader epidemiological data such as the NMHS, which reports higher CMD prevalence among women due to multifactorial stressors, such as domestic responsibilities, limited economic empowerment, and socio-cultural constraints. 17 Conversely, SMDs and SUDs were more common in men, mainly aged 40–60, aligning with established literature indicating gendered vulnerabilities: men are more prone to substance misuse and psychotic disorders due to socio-behavioral norms, stigma, and lower help-seeking behaviors.18,19
Cultural stigmatization of mental illness may inhibit women from expressing distress unless it manifests as somatic complaints, which CHOs trained in the Diploma in Primary Care Psychiatry or similar initiatives have learned to identify. 20 Men, conversely, may externalize stress via substance use, reflected in higher SUD cases, underscoring the need for gender-sensitive community-based interventions. Moreover, systemic barriers like limited access to specialized care in rural India further exacerbate diagnostic delays, reinforcing the value of CVCs.
The study also highlights the varied interventions provided through CVCs, including counseling, medication, referrals, and follow-ups. Analysis of referral, counseling, and follow-up rates revealed state and diagnosis-specific trends, offering insights into the real-world impact of CVC-enabled CHO interventions. Karnataka demonstrated high referral rates (50.6%) and counseling (28.4%) for CMDs, likely a reflection of its more extended engagement with collaborative MH models, as shown in previous capacity-building initiatives. 21 In Bihar, CHOs exhibited strong follow-up practices for CMDs (42.1%), highlighting a growing emphasis on continuity of care even in lower-resource settings.
Maharashtra, in contrast, showed the highest follow-up for SMDs (58.6%), pointing toward an evolving understanding of chronic psychiatric conditions and the need for persistent monitoring. This proactive stance aligns with findings from the Diploma in Primary Care Psychiatry, which emphasized continuing care protocols in its training modules.
Although CMDs formed the bulk of diagnoses, SUDs were consistently underserved in terms of referrals and follow-up across all three states. This suggests an ongoing stigma and diagnostic inertia around addiction, despite high prevalence in male patients, particularly aged 40–60. As reported by Sukumar et al., many CHOs still face difficulty initiating conversations around substance use, indicating a need for more targeted training and support. 18
CHOs’ Capacity Building and Training Impact
CHOs, despite their vital role, are frequently undertrained in MH care. 12 This limits their capacity to recognize and treat MH issues at the PHC level, 22 and the MH problems remain unnoticed or untreated. The CHOs, if provided with the proper training, may be able to play a more effective role in bridging the MH treatment gap.6,10
The study emphasizes the importance of structured training programs in equipping CHOs with the skills necessary to address MH issues effectively. CHOs trained through the program demonstrated the ability to provide holistic care, encompassing pharmacological and non-pharmacological interventions. The real-time feedback from CVCs further reinforced their learning and confidence, promoting skill refinement and improved clinical decision-making. 23 The training modules, including six-session Zoom-based training and teleconsultation orientation, played a crucial role in enhancing CHOs’ competencies. The integration of digital tools and collaborative approaches aligns with global trends in leveraging technology to expand the reach of MH services. 24
Challenges, Limitations, and Lessons Learned
Regardless of its success, the implementation of the digitally driven CVC model was not without its challenges. One of the major barriers encountered was limited digital literacy among CHOs, particularly those in remote or resource-constrained areas. While most CHOs were able to navigate online platforms post-training, some required additional handholding, including repeated orientation and asynchronous video demonstrations, an approach echoed in similar programs such as CHaMP in Chhattisgarh and TORENT.25–27
Intermittent internet connectivity, especially in Bihar and Maharashtra, frequently disrupted live consultations, reducing real-time interactivity between CHOs and specialists. This technical issue underscores the need for robust digital infrastructure as a precondition for scalable telepsychiatry interventions. As noted by Malathesh et al., tele-mentoring programs must embed infrastructure investment alongside training to ensure sustainability. 28
Moreover, resistance to adopting new practices was evident among a subset of CHOs, often driven by discomfort in interacting with MH professionals in real time. This hesitance diminished over time through structured mentorship, iterative engagement, and demonstration of clinical outcomes paralleling experiences from personalized mentorship programs described by Manjunatha et al. 30 Peer-to-peer encouragement within WhatsApp groups and the inclusion of reflective practice modules also helped mitigate early resistance, reinforcing the importance of psychosocial support structures for task-shifting programs.
Additionally, there is no follow-up data in this study, which limits the assessment of the long-term impact of this model on patient outcomes. It is crucial to address these issues to scale and sustain this model of care.
Implications for MH Care Delivery
The study shows the potential of the CVC model as a novel means of bridging the MH treatment gap in India. The model improves accessibility and improves quality of care by integrating MH into primary care and by giving the CHOs frontline delivery power. The approach ensures timely interventions to help strengthen the PHC system.
Future research must evaluate the cost-effectiveness of the CVC model, assess its scalability across various regions, and compare it with other training modalities in primary care psychiatry. Furthermore, the inclusion of follow-up data will be valuable in understanding the long-term benefits of such programs.
Conclusions
This program for primary MHcare demonstrates the effectiveness of digitally driven CVC models in enhancing the MH care capabilities of CHOs. The findings highlight the potential of such collaborative, technology-driven approaches to integrate psychiatric care into primary care, bridging the MH treatment gap, particularly in underserved regions.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
Same as the “Introduction ” article of this issue (Indian J Psychol Med. 2026;48(1 suppl)).
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Author Channaveerachari Naveen Kumar is the Principal Investigator of this project and supplemental issue. The author did not take part in the peer review or decision-making process for this submission and has no further conflicts to declare.
Declaration Regarding the Use of Generative AI
The authors used Chat GPT to paraphrase and formalize the text. After using this tool/service, the authors reviewed the translated and transcribed content and edited it as needed and take full responsibility for the content of the publication. The authors assume full responsibility for its entire content, including the parts generated by the AI tool.
Ethical Approval
The study was approved by the Institutional Ethics Committee (IEC) (Approval No. NIMHANS/ 43rd IEC (BEH.SC.DIV) 2023, dated December 8, 2023) and registered with the Clinical Trial Registry of India (Registration No. CTRI/2024/02/062906).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study’s data were derived from a project funded by the CSR initiative of a multinational company.
Informed Consent
Informed consent was sought from all participants, including the primary healthcare workers and patients.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.