
Abstract
Nonprobability sampling, especially the consecutive and snowball methods, is common in Indian mental health research due to their practical utility. Yet, their unchecked use shapes whose experiences are heard and whose are excluded. This article critiques their ethical costs and proposes realistic reforms for inclusive, responsible data collection.
The sampling method a researcher chooses is not a passive decision; it determines whose voices shape evidence, whose realities are rendered legitimate, and whose struggles remain unseen. 1
In Indian mental health research, systemic constraints around funding, institutional inertia, and access barriers favor the frequent use of nonprobability techniques, particularly consecutive and snowball sampling. 2 These approaches persist largely unquestioned and, in some cases, institutionally embedded. 3 While methodological handbooks highlight the statistical limitations of these approaches, far less attention is paid to their ethical implications. 4 This manuscript critically examines how these techniques silently exclude certain populations, reinforcing inequities in whose mental health needs are documented.
Its novelty lies in shifting the conversation from methodological convenience to ethical responsibility, drawing from lived experiences of over a decade in Indian mental health spaces as a field researcher, clinician, ethics reviewer, and academic supervisor. 5
While Berksonian bias in consecutive sampling and selection bias in snowball sampling are well described in methodological texts, 6 our contribution lies in reframing these not simply as statistical concerns but as ethical ones. Methodological handbooks often treat bias as a technical limitation, yet rarely ask how such exclusions affect whose realities are legitimized in evidence. 7 The novelty of this manuscript, therefore, is twofold: first, in shifting the frame from methodological feasibility to ethical responsibility, and second, in illustrating through lived experiences across research, clinical practice, and ethics review how unchecked use of nonprobability sampling consolidates inequities in whose mental health needs are rendered visible. In this sense, the article does not introduce bias as a new concept, but extends the discussion into the moral domain, showing how statistical shortcuts translate into epistemic injustice.
Discussion
Consecutive sampling is widely used in psychiatric outpatient clinics and hospital-based studies across India. It operates on a seemingly neutral logic: all patients who meet predefined inclusion criteria during the study period are recruited until the desired sample size is reached. Yet this approach assumes that those who access services are representative of the population of interest, an assumption that fails under scrutiny.
For example, a study on school-based anxiety compared private and government school students but still represented only adolescents enrolled in formal education. Such designs unintentionally exclude out-of-school youth—often those experiencing higher psychosocial adversity—yet the findings are commonly interpreted as representing ‘adolescent anxiety’ in general. 8 This gap between the sample and the scope constitutes an ethical failure, not merely a methodological one, raising serious concerns about the research’s findings.
It is essential to recognize why researchers often rely on consecutive and snowball sampling. Consecutive sampling is logistically feasible in clinical settings, enabling studies to enroll all eligible participants within a defined period. Snowball sampling can be invaluable for reaching hidden or stigmatized populations, where trust and peer referrals are crucial for recruitment. These approaches, despite statistical limitations, can generate practical insights and help document experiences that might otherwise remain inaccessible. 9
At the same time, even idealized random sampling from an enumerated population faces practical constraints, such as refusals, illness, or time limitations, which can introduce heterogeneity and bias. Thus, all sampling strategies involve trade-offs, and awareness of both strengths and limitations is essential for responsible research design. 10
Moreover, in a country where mental health stigma prevents many from seeking care, consecutive sampling in hospitals and clinics systematically filters out those most vulnerable individuals in rural areas, women from conservative households, transgender individuals denied services, or survivors of violence, who are reluctant to disclose trauma. In each case, the technique does not just miss data, it misses lived experiences that matter most.
Gaining Access Losing Diversity
Snowball sampling is often considered for reaching “hard-to-access” populations such as survivors of gender-based violence, substance users, or Lesbian, Gay, Bisexual, Transgender, Queer/Questioning, Intersex, and Asexual (LGBTQIA) communities. It relies on peer referrals within networks to identify additional participants. While it can be a powerful tool for building trust and ensuring safety, it carries the risk of severe homogeneity. 11 The initial seed participants are often connected by caste, class, religion, or geography. As referrals multiply, the diversity tends to narrow rather than expand. 12
For example, a field study on widows in Odisha used snowball sampling initiated through a self-help group. While it achieved recruitment targets, the resulting sample included only those already participating in support networks. Completely isolated widows —arguably those in greatest need of research and intervention —were excluded. Yet the findings were generalized to “rural widowhood in India.” 13 Such methodological slippage transforms convenience into epistemic violence.
Even in progressive studies, snowball sampling among queer youth or migrant laborers can become an echo chamber. One urban queer activist refers another within their circle, but Dalit or transgender voices outside that network remain absent. Yet, findings are generalized across broad categories such as “queer youth” or “migrant experience.” When marginalized groups are represented solely through the most visible or networked members, data reflect only a fraction of lived realities while claiming to be comprehensive. 14
Structural Exclusion in Research
When specific populations are systematically underrepresented or entirely excluded from our samples, research becomes a tool of erasure. Mental health studies, especially those that inform policy or clinical protocols, are not merely academic exercises; they shape how services are delivered, to whom, and under what conditions.
Consider a study on substance use among men in an urban Indian context. Researchers used respondent-driven approaches beginning with clients in a rehabilitation center. 15 Unsurprisingly, all participants had sought treatment voluntarily. The resulting conclusion emphasized the role of motivation and family support in recovery. However, this completely ignored the experiences of those who use substances but never access formal help due to poverty, stigma, or lack of services. The final dataset thus privileges the recoverable, the supported, the visible. The structurally silenced remain both missing and unmissed.
Similarly, consecutive sampling in hospital-based studies of post-traumatic stress disorder (PTSD) in survivors of domestic violence has shown similar distortions. 16 Many survivors never seek institutional care due to fear, shame, or control by perpetrators. Those who do may already be in late-stage crisis, which skews data toward high-severity cases. As a result, our understanding of trauma becomes primarily associated with clinical thresholds rather than with community-based or silent suffering.
The danger lies not only in data gaps but also in epistemic distortions. When flawed samples construct categories like “depression among working women” or “stress in adolescent boys,” we create reductive, often inaccurate, knowledge that informs diagnostic trends, therapeutic approaches, and funding priorities. These distortions ripple outward into clinics, classrooms, and communities, reinforcing a narrow version of reality.
Ethical Shortcuts and the Illusion of Sufficiency
In over 20 mental health studies reviewed from Indian journals and postgraduate theses, using either consecutive or snowball sampling, only a handful provided any justification for their method choice. 17 Fewer still acknowledged limitations around generalizability, inclusion bias, or ethical implications. This suggests that convenience sampling has become normalized to the point that its use no longer demands critical reflection.
Ethics committees, pressed for time and overwhelmed by volume, often accept these sampling strategies without challenge, mainly if ‘informed consent’ and ‘anonymity’ are addressed. But what about epistemic justice? If research systematically excludes specific populations, are we not complicit in sustaining that exclusion?
A recent thesis on resilience among women in urban slums used snowball sampling starting from a daycare center run by a non-governmental organization. The participants were mostly employed mothers who were already engaged in supportive programs. Yet the thesis concluded that resilience was a “character trait” among low-income women, without discussing how access to services or social capital shaped that resilience.
Such examples illustrate how method can become an ideology, obscuring critical contextual factors. The illusion that a sample is inherently valid simply because it meets size criteria must be resisted. Sampling is not merely procedural; it is a moral act.
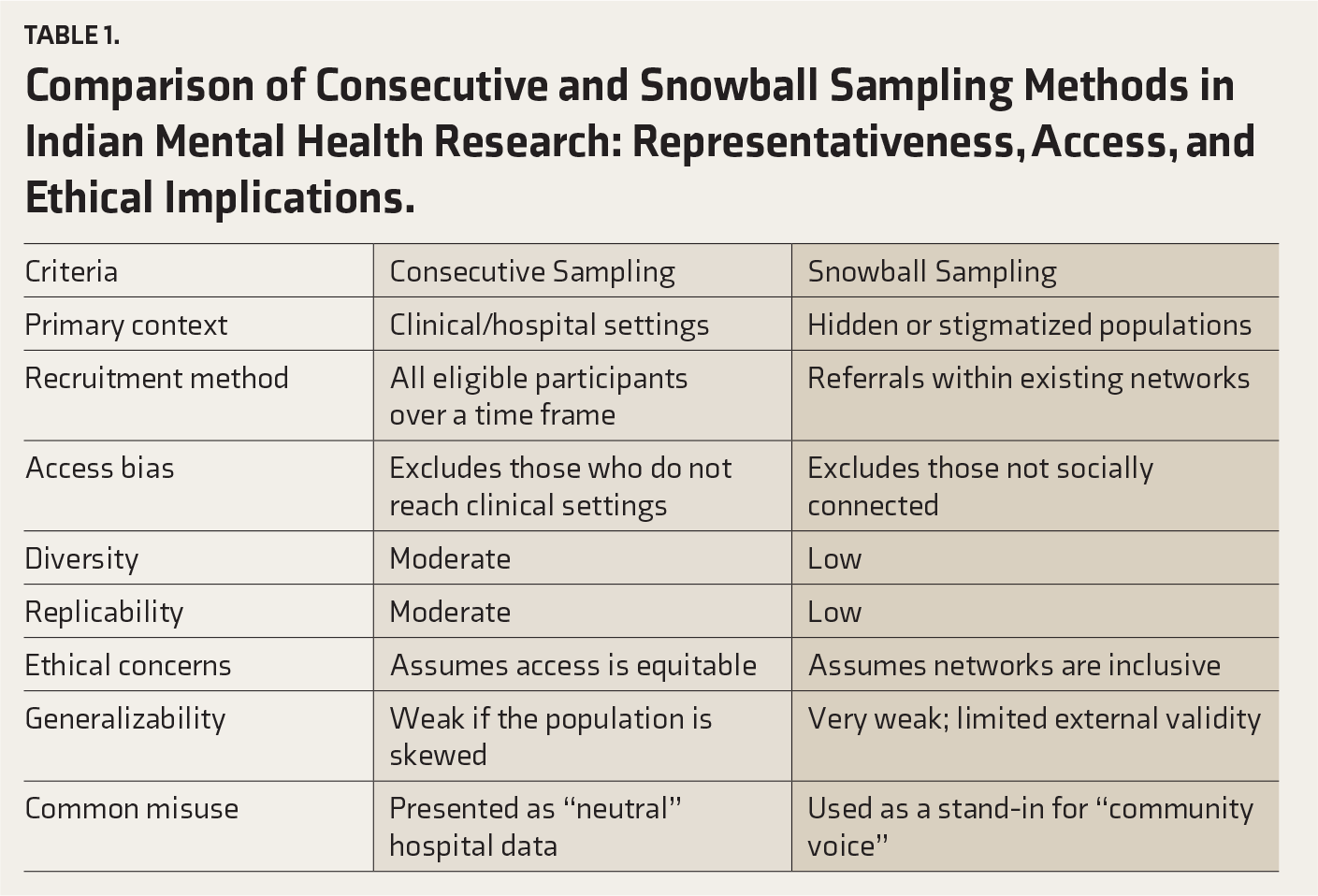
As summarized in Table 1, consecutive and snowball sampling differ in terms of representativeness and access. This table highlights the systemic nature of these biases and the ethical shortcuts embedded in routine sampling decisions. Neither method is inherently unethical, but both demand greater transparency and intentionality than they currently receive.
Comparison of Consecutive and Snowball Sampling Methods in Indian Mental Health Research: Representativeness, Access, and Ethical Implications.
If we accept that sampling shapes what becomes valid knowledge, then reforming how we sample is not optional; it is urgent. Below are five key proposals for reshaping sampling culture in Indian mental health research:
Reforming sampling practices in Indian mental health research begins with transparency and deliberate choice. Every study, especially those using nonprobability methods, should clearly explain why a particular approach was selected, what other options were considered, and why techniques like snowball or consecutive sampling were ultimately used. Equally important is acknowledging who may have been left out of the research. A brief description of likely exclusions not only enhances transparency but also prompts researchers to reflect on whether their sample truly represents the population they aim to study.
18
Inclusion can be strengthened even in resource-constrained settings by blending methods, for example, using purposive recruitment followed by snowball referrals, or starting with consecutive sampling and then extending outreach into the community to reduce bias and widen diversity.
19
Ethics committees and peer reviewers also have a crucial role. Instead of limiting their evaluation to procedural compliance, they should actively ask questions such as, “Who is excluded?” and “What assumptions does this sampling approach reinforce?” When such questions reveal significant exclusion risks, committees should not automatically reject the study. Still, they should require explicit justification from researchers, including identification of likely exclusions, limits of generalizability, and mitigation strategies such as blended or supplementary recruitment. If these concerns remain unaddressed, committees should formally flag them and request revision before approving.
20
Ultimately, the mindset within academic institutions, funding agencies, and research departments must evolve. This does not mean that studies using nonprobability methods should be denied funding, but that such studies should be expected to justify their sampling rationale, articulate anticipated exclusions, and, where feasible, propose corrective strategies. Funders can encourage good practice by making these elements explicit criteria in grant evaluation. Academic training programs, similarly, should emphasize that sampling is not a logistical hurdle but a value-driven choice, equipping future researchers to approach it with inclusion and ethics at the forefront.
These reforms are not costly or complex. They require a willingness to confront the structural habits we’ve normalized in the name of feasibility.
Strengths
This viewpoint integrates practical field experience with ethical critique, focusing squarely on the impact of common sampling practices on equity and justice in Indian mental health research. It moves beyond abstract methodological discussions to highlight the real consequences of exclusionary research practices for marginalized populations.
Limitations
The discussion centers on the two most prevalent nonprobability sampling approaches and does not empirically quantify exclusion across all Indian contexts. Recommendations stem from experiential insight rather than systematic meta-analysis, which is a valuable direction for future research.
Conclusions
Sampling is not technically a methodological footnote; it is a deliberate value-laden choice that predicts which lives are seen as legible and which remain invisible. In other words, decisions about who to include or exclude inherently privilege specific populations while systematically omitting others, shaping the evidence base, and determining whose experiences are recognized in research. The inclination toward consecutive and snowball sampling in Indian mental health research has produced data that are much easier to gather but are narrow in perspective, masking heterogeneity and producing knowledge that is efficient yet ethically impoverished. This gives rise to both epistemological and moral problems when sampling is treated as neutral. Correcting sampling requires reorientation of practice and incentives. This must be framed and reviewed as ethical acts; protocols should justify inclusion and exclusion, quantify biases, and articulate plans to counter exclusions. Methodologically, researchers should combine probability-informed designs, purposive oversampling of marginalized groups, community-engaged recruitment, and mixed methods to surface complexity rather than flatten it. Institutionally, funders, ethics committees, and journals must demand rigorous sampling rationales, bias assessments, and capacity building so that representativeness and justice are not optional extras but core metrics of quality.
If we treat sampling as an architecture of inclusion rather than a technical implementation, Indian mental health research can produce findings that are scientifically valid, socially responsive, and capable of informing policies and interventions that reflect the diversity and complexity of lived experiences.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.