
Abstract
Background:
Early identification and management are associated with better outcomes for individuals with autism. However, the limited awareness of autism among frontline healthcare workers has led to delays in referrals and diagnoses. This study aims to assess awareness and knowledge about autism among Accredited Social Health Activists (ASHA) workers.
Methods:
This cross-sectional study was conducted with 103 ASHA workers in Udupi district, Karnataka, India. A semi-structured assessment was used to collect socio-demographic information and assess basic awareness of autism. Knowledge of autism signs and symptoms was evaluated using items from the Indian Autism Screening Questionnaire (IASQ), which was modified for the study.
Results:
Among the participants, 70.5% categorized autism as a mental illness. Additionally, 58.8% identified the earliest age for autism diagnosis as 03 years. Furthermore, 68.2% knew that children with autism require medication alongside other treatment modalities, such as counseling, speech therapy, and occupational therapy. Compared with those without such experience, ASHA workers with prior experience attending lectures on developmental disorders had greater knowledge of identifying symptoms of autism, including social communication deficits and restricted, repetitive patterns of behavior and interest. Three percent of the participants reported no knowledge of autism symptoms.
Conclusion:
This study revealed that ASHA workers had limited awareness and knowledge regarding autism, including its symptoms, course, and management. These findings suggest the need for more specific awareness-building programs in addition to existing training programs available for ASHA workers, which might help with the early identification and referral of children with autism for early psychosocial intervention.
Keywords
Most ASHA workers recognized autism as a mental illness. ASHA workers with prior exposure to didactic programs for autism had better knowledge of autism symptoms.Key Messages:
Autism is a neurodevelopmental disorder characterized by persistent deficits in social communication and interaction across contexts and by restricted, repetitive patterns of behavior, interests, or activities. 1 The global prevalence of autism spectrum disorder is estimated at 65 per 10,000 children, 2 whereas in India, the prevalence is approximately 1% among children aged 2–6 years and 1.4% among those aged 6–9 years.1–4 In urban areas, the mean age of autism diagnosis is 4.62 years; in rural communities, it is 4.87 years, which is nearly 0.35 years later than in urban children. 5 This delay may be attributed to beliefs such as assuming that children will “outgrow” their difficulties, viewing poor eye contact as shyness or an endearing trait in young children, and seeing boys as “late-talkers.” Additionally, differing opinions among elderly family members regarding a child’s developmental challenges and rural families’ preferences for seeking help from traditional faith healers or untrained practitioners can impact early symptom identification and help-seeking behaviors. 5
Other contributing factors to the delay in autism recognition in rural areas include milder presentations of the disorder, limited access to specialized care services, long distances to care centers, financial constraints, lower educational levels, and limited awareness of neurodevelopmental disorders such as autism. 5 There is a strong consensus that early identification and intervention lead to better outcomes for children with autism spectrum disorders.5,6 The number of mental health professionals in India is currently inadequate, with fewer than 10,000 mental health professionals (approximately 0.75 psychiatrists per 100,000 population) and similarly low ratios of psychologists and psychiatric social workers.7,8 However, European regions have 40 times more mental health professionals (44.8 mental health professionals per lakh population) than do African regions (1.6 mental health professionals per lakh population), and in Southeast Asian countries, the number of mental health professionals per lakh population is 2.8. 9 This shortage highlights the importance of involving nonspecialists in the healthcare system and implementing task-shifting strategies at the community level.6,10
The Ministry of Health and Family Welfare, Government of India, introduced Accredited Social Health Activists (ASHA) under the National Health Mission in 2005. ASHA workers play a critical role in raising awareness of health programs, educating communities about maternal and infant health services to reduce maternal and infant mortality, and connecting rural populations with healthcare professionals. 11 In addition, they are part of the Rashtriya Bal Swastya Karyakram (RBSK) team, which works to identify and intervene early for children from birth to 18 years of age. Furthermore, it covers 30 selected health conditions for screening, early identification, and timely management. Among these 30 health conditions, developmental disorders such as autism, ADHD, and learning disorders are included. Hence, frontline healthcare workers need to be aware of common neurodevelopmental disorders in children. 12
Few studies have assessed the level of knowledge ASHA workers possess regarding autism spectrum disorder. 10 This study aims to evaluate ASHA workers’ awareness and knowledge of autism. Additionally, explored an association between previous experience attending a program on developmental disorders, work experience, educational qualifications, and knowledge about the signs and symptoms of autism.
Methods
Study Design
This cross-sectional, observational study was conducted from October 2023 to May 2024 in the Department of Psychiatry at (Kasturba Medical College, Manipal, MAHE), a tertiary care center in South India. The study received approval from the Institutional Ethics Committee of Kasturba Medical College and Kasturba Hospital (Approval No. IEC1: 286/2023 dated 09-08-2023), and the study protocol was registered in the Clinical Trial Registry of India (CTRI/2023/12/060632). Permission was obtained from the Directorate of Health and Family Welfare Services, Government of Karnataka, Arogya Soudha, Bangalore, and the District Health Office, Udupi. All study participants provided written informed consent.
Participants
ASHA workers were recruited from primary health care centers in Udupi district, one of the 30 districts in Karnataka, India. The Udupi district covers an area of 3,582 square kilometers, comprises seven taluks, and has a population of 11,77,361. 13 This study recruited participants from three taluks, Udupi, Brahmavara, and Kaup, using a convenient sampling method.
ASHAs are single or married women aged 25–45 years from the local community, with education up to a higher primary school level. One ASHA worker is appointed per 1,000 people. Their responsibilities include overseeing maternal and infant health, promoting institutional deliveries, conducting home visits during pregnancy, arranging access to complementary foods available through local government facilities, escorting pregnant women to hospitals for childbirth, and supervising newborns during the first month of life. They also assist families in attending immunization days and encourage the use of family planning methods. Additionally, ASHAs support other frontline workers, such as auxiliary nurse midwives (ANMs), during field visits and participate in various government health surveys within the community. ASHAs are also expected to be knowledgeable about the spread and referral pathways of diseases such as HIV/AIDS and tuberculosis.14,15 The Ministry of Health and Family Welfare of the Government of India introduced ASHA workers in 2005 under the National Health Mission. 15
Considering these various roles and functions of the ASHA workers, in the present study, participants were included in the study if they had minimum of one year of experience as an ASHA workers, as the initial year of work provides them exposure to children with various health problems (physical and psychological problems) during the community visit or that they might undergo multiple training programs from the government and private sector in the first years of their profession and those who did not consent to participate in the study were excluded.
Sample Size Estimation
The Udupi district has a total of 969 ASHA workers, according to the Udupi District Health Office. Assuming 50% of the population possesses the factor of interest, we estimated the required sample size with 10% absolute precision and a 95% confidence level, targeting a sample of 88 ASHA workers. The sample size was calculated using Statulator software, 16 with the formula: SS/[1 + {(SS −1)/Pop}].
Procedure
The researcher contacted the Udupi District Health Office (DHO) and collected the contact details of ASHA workers in charge and the posting details of ASHA workers at various primary and community health centers in Udupi district. Additionally, information on DHO program schedules for ASHA workers, including when the ASHA group participates as a whole, was collected.
The researcher contacted the ASHA workers in charge before visiting the DHOs and explained the present study and the purpose of the meeting. The in-charge person would provide information regarding any weekly meeting scheduled for a particular day in the respective Primary Health Centres (PHC) and used to inform their ASHA workers about the researcher’s visits to their PHCs. Through this method, the researcher approached each ASHA worker, provided information about the study, and invited them to participate. Additionally, the researcher met with the ASHA workers on their scheduled meeting days at the DHO office and recruited the entire group (those who provided consent and met the eligibility criteria), as it was difficult to refuse participants in the group setting. All the participants recruited in the study completed the assessment provided to them.
Overall, 103 ASHA workers were recruited from those present during the researcher’s visits to the DHO office in Udupi and fourteen primary health centers in the Udupi, Brahmavara, and Kaup taluks.
Assessment
The participants’ socio-demographic information (age, education, work experience, and nature of work), as well as details related to training in neurodevelopmental disorders (prior experience attending training programs on developmental disorders, duration of training, and methodology), basic awareness of autism, and knowledge regarding the course of autism (earliest age of diagnosis, treatment-related information), were collected through 10 questions with multiple-choice responses. Similarly, six semi-structured interview questions were included along with other multiple-choice response questions. For example, what are the common developmental disorders in children you know of? (details in Supplement Table 1).
Assessment of Knowledge About the Signs and Symptoms of Autism
Knowledge of autism signs and symptoms was assessed using items from the Indian Autism Screening Questionnaire (IASQ), 4 which was modified for the study. The IASQ contains 10 items: items 1, 2, 3, 4, and 7 assess difficulties in social communication and interaction across contexts, whereas items 5, 6, 8, 9, and 10 assess restricted, repetitive behaviors, interests, or activities. 4 Modifications to the IASQ included (a) translation of the original English version into the local language, Kannada; (b) changing response options from “yes” or “no” to “true,” “false,” and “Do not know”; (c) modifications to the IASQ individual items; and (d) adding the term “autism” to each item (details in Supplement Table 2).
The English version of the ISAQ was translated into Kannada with the original author’s permission. Two native Kannada speakers conducted the initial translation, and two independent Kannada language experts with formal education in English completed a back-translation. One of the authors (UT) reviewed the combined translation to finalize a single back-translated version. To ensure that the Kannada version was clear and understandable, four Kannada-speaking volunteers (nursing trainees and department interns) were asked to complete the questionnaire and provide feedback on the clarity of each question and any challenges they encountered in comprehension.
Following this process, a pilot test was conducted with 15 ASHA workers (who met the study criteria) to identify any practical difficulties in administering the Kannada version of the assessment and to obtain ASHA workers’ feedback. In this process, a few problems were identified in the assessment, such as ASHA workers not attempting some questions, being unsure of the answers, and having no “do not know” options. Additionally, the uniformity of the scale’s questions prevented participants from reading them thoroughly, as most were positive response statements. Hence, a few changes were incorporated into the assessment.
The response options in the IASQ were adjusted from “yes” or “no” to “true,” “false,” and “do not know.” To reduce response bias, negatively framed statements were rephrased in a positive frame. For example, “does not maintain peer relationships” was changed to “children with autism maintain close peer relationships.” Similarly, positive statements such as “engages in stereotyped and repetitive motor mechanisms” were revised to “children with autism do not engage in stereotyped and repetitive motor mechanisms.” Additionally, “children with autism” was prefixed with each item, as the objective was to assess knowledge about autism rather than screen for it (details in Supplement Table 2). The third author (AV), proficient in both Kannada and English, proofread the Kannada IASQ, resulting in the final IASQ-Kannada version used in this study. The second author (UT) discussed the final version of the assessment tool with the fourth author (SS) and the first author (STY) and sensitized them to address potential queries from study participants during its administration. In addition, to avoid response bias, the fourth author (SS), proficient in Kannada, read each item individually to help participants understand the questions and respond. Additionally, the participants were asked to sit at a distance from one another so they would not be able to see each other’s responses. The researcher instructed them not to refer to external sources (such as mobile devices or others) when answering the questions. The assessment was completed within a timeframe of twenty to thirty minutes. The English version of the assessment tool is available as supplementary material (see Supplement Table 1 for details).
Statistical Analysis
The data were analyzed via SPSS version 16.0 for Windows. Descriptive statistics (frequency and percentages) were used to summarize the data. Demographic variables, including education, work experience, prior experience attending training programs on developmental disorders, training program duration, training methods, awareness of autism, knowledge of autism signs and symptoms, and understanding of the course of autism, were described using frequency distributions. The ASHA workers were grouped based on prior experience attending training programs on developmental disorders, and their knowledge of identifying persistent deficits in social communication and interaction, as well as restricted, repetitive patterns of behavior, interests, or activities in children with autism, was compared using Pearson’s chi-square test. Statistical significance was set at p < .05 (2-tailed). Those responses, derived from the semi-structured interview questions, were manually coded to organize participants’ responses. They were later entered into the SPSS master sheet with appropriate codes, and descriptive statistics (frequency and percentages) were used to summarize the data.
Results
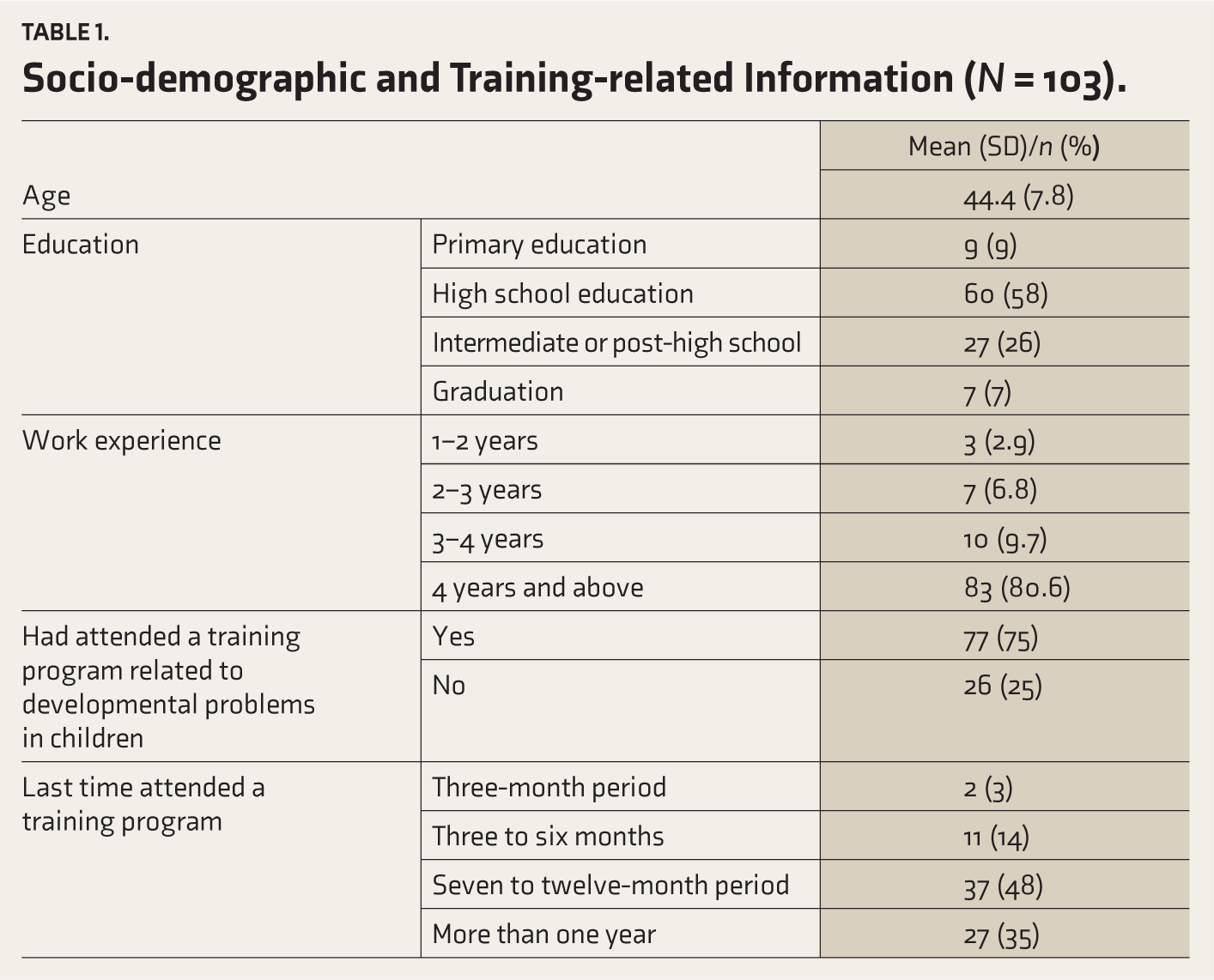
A total of 103 ASHA workers were recruited for the present study. Socio-demographic information and details regarding previous training are presented in Table 1. Among the participants, 80.6% had more than 4 years of work experience, and 74.8% had attended lecture programs on neurodevelopmental issues in children. Of those, 68% had participated in a one-day lecture program.
Socio-demographic and Training-related Information (N = 103).
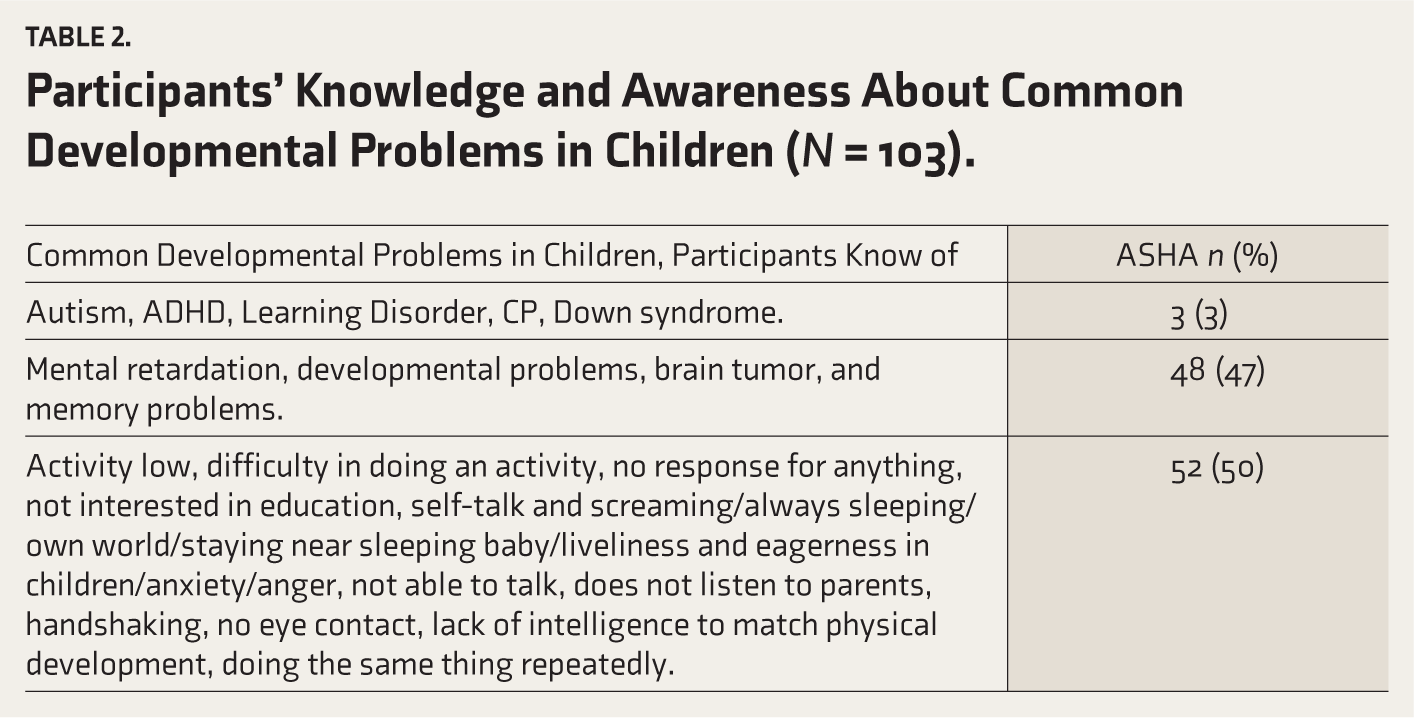
Responses to the open-ended question, “What are the common developmental problems in children you know of?,” were tabulated, and the corresponding frequencies are reported in Table 2. In this study, 94.2% of the participants reported having heard of autism, with 70.5% identifying autism as a mental illness.
Participants’ Knowledge and Awareness About Common Developmental Problems in Children (N = 103).
ASHA Workers’ Knowledge About the Signs and Symptoms of Autism
In identifying persistent deficits in social communication and interaction across multiple contexts, 94.8% of participants recognized that children with autism exhibit poor eye contact, and 91.8% noted a lack of social smiles. Other reported behaviors included being aloof (85.6%) and being unable to initiate or sustain conversations with others (94.8%). However, 64.9% of the participants reported that children with autism easily reach out to others.
In identifying restricted, repetitive patterns of behavior, interest, or activity, 85.6% of participants recognized that children with autism engage in solitary, repetitive play. Additionally, 56.7% reported that children with autism do not maintain close peer relationships, 75.3% identified attachment to inanimate objects, and 72.2% reported that children with autism respond to objects unusually, by smelling, touching, or tasting them. Additionally, 55.7% of the ASHA workers reported that children with autism do not engage in stereotyped and repetitive motor behaviors. Between 11% and 38% of ASHA workers reported that children with autism do not engage in solitary and repetitive play activities or maintain close peer relationships. Additionally, 20% reported that children with autism do not attach to inanimate objects or respond to objects unusually by smelling, touching, or tasting. Three percent of the participants reported that they did not know any symptoms of autism.
ASHA Workers’ Knowledge About the Course of Autism and Treatment
With respect to the earliest age at which autism was diagnosed, 58.8% of the participants reported that autism can be diagnosed between 0 and 3 years of age, 35.1% reported between 3 and 6 years, and 3% reported between 6 and 10 years. One participant noted that the earliest age for diagnosis was over 18 years, and 2% of participants stated that they did not know the earliest age for diagnosing autism.
With respect to the management of autism, 68.2% of ASHA workers reported that children with autism require medication and other treatment modalities, such as counseling for children and parents, parent training, speech therapy, and occupational therapy; 19.7% of the participants reported counseling, parent training, speech therapy, and occupational therapy only; and another 12% mentioned specific individual treatment modalities, such as counseling for children/parents, parent training, or speech therapy.
In identifying and referring children with autism, 91.8% of ASHA workers reported that they had not identified or referred children with autism for treatment. However, 8% of the ASHA workers reported referring children to nearby primary health centers (n = 4), NGOs (n = 1), or tertiary care centers (n = 3).
Association Between the Previous Experience of Attending a Program on Developmental Disorders and ASHA Workers’ Knowledge About Signs and Symptoms of Autism
A chi-square test comparing two groups of ASHA workers based on their previous experience attending programs on developmental disorders revealed significant differences between the groups in identifying persistent deficits in social communication and social interaction across multiple contexts, as well as in identifying restricted, repetitive patterns of behavior, interest, or activities (Table 3). No significant difference was found between those who had attended the training program within the last six months and those who had participated more than six months prior.
Group Differences Among ASHA Workers Based on Their Previous Experience with Attending Programs for Developmental Disorders.
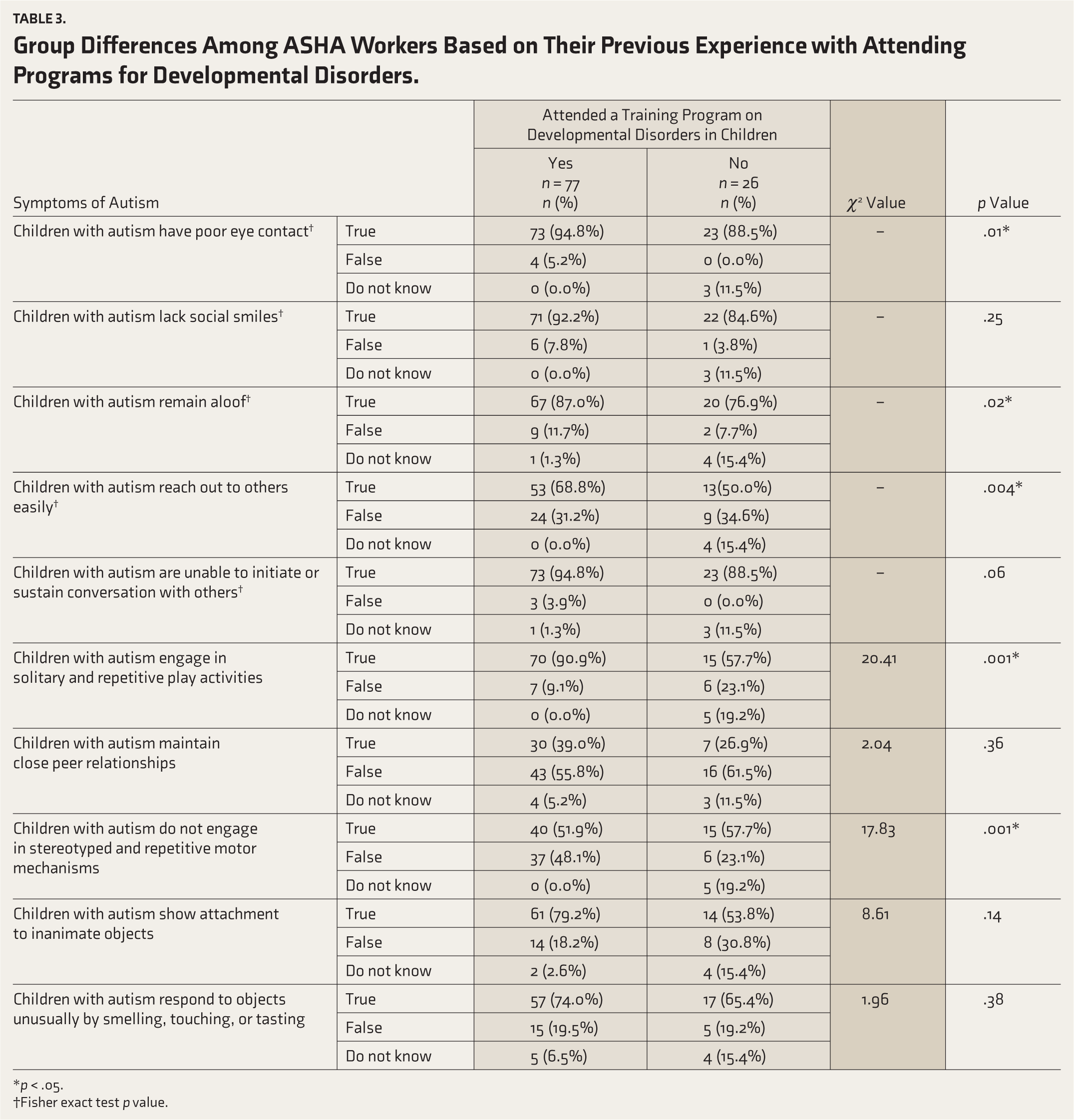
*p < .05.
†Fisher exact test p value.
Associations Among ASHA Workers’ Work Experience, Education Qualifications, and Knowledge About the Signs and Symptoms of Autism
No significant relationships were found between ASHA workers’ work experience and identifying persistent deficits in social communication and social interaction across multiple contexts, or between ASHA workers’ work experience and identifying restricted, repetitive patterns of behavior, interests, or activities (details in Supplement Tables 3 and 4). Similarly, there was no significant relationship between educational qualifications and identifying restricted, repetitive patterns of behavior, interest, or activities, or identifying the majority of the symptoms of persistent deficits in social communication and social interaction across multiple contexts. However, a significant group difference was found between ASHA workers’ educational qualifications and identifying a single symptom (children with autism have difficulty in initiating or sustaining conversations with others [χ2 = 22.13, p < .01]), among other symptom lists for identifying persistent deficits in social communication and social interaction across multiple contexts (details in Supplement Tables 5 and 6).
Discussion
This is one of the few studies to examine the awareness and knowledge of autism among ASHA workers. Our findings revealed that the majority of ASHA workers reported autism as a mental illness, and only a few participants were able to identify autism, attention-deficit hyperactivity disorder (ADHD), and learning disorders as neurodevelopmental disorders. In this study, 68% of participants attended a one-day didactic program on neurodevelopmental disorders that was not specific to autism. This may explain why many participants recognized autism as a mental illness, grouped head injury and memory problems under neurodevelopmental disorders, or were unable to identify autism or ADHD specifically. Rather than naming the disorders, participants tended to report discordant symptom clusters as a disorder. A previous study reported that ASHA workers’ knowledge of child health was positively associated with the number of days they attended training programs. 17
In the present study, 12.4% of the participants reported obtaining information about autism through a mental health training program, whereas 74.2% reported acquiring information through lectures on neurodevelopmental disorders during their initial training or through social media. This may explain why many participants had heard of the disorder called autism. However, participants reported different age ranges (0–3 years, 3–6 years, 6–10 years, and>18 years) as the earliest age at which autism can be diagnosed. Children with autism typically show symptoms in their first years of life and can be diagnosed before the age of three 18 ; however, many are not diagnosed until after the age of four, according to the CDC in 2014. 19 In India, the mean age of diagnosis is 4.62 years in urban areas and 4.87 years in rural communities. 5 Early diagnosis of autism is crucial for accessing professional services, as delays can deny children pivotal treatment opportunities and increase their risk for poor long-term functional outcomes. 5
In the present study, participants showed mixed responses in identifying persistent deficits in social communication and interaction, as well as restricted, repetitive patterns of behavior, interests, or activities in children with autism. Some participants reported being aware that children with autism have poor eye contact, lack social smiles, remain aloof, are unable to initiate or sustain conversations, engage in solitary and repetitive play activities, do not maintain close peer relationships, show attachment to inanimate objects, and respond to objects unusually by smelling, touching, or tasting. However, other participants held opposing views, such as believing that children with autism easily reach out to others, do not engage in stereotyped and repetitive motor behaviors, are not aloof, do not engage in solitary play, maintain close peer relationships, do not show attachment to inanimate objects, and do not respond to objects in unusual ways. A few participants reported that they did not know about the restricted, repetitive patterns of behavior, interests, or activities in children with autism. These mixed responses suggest that while some participants were aware of specific autism symptoms, their overall knowledge about the signs and symptoms of autism and the earliest age for diagnosing autism was inadequate. This lack of comprehensive understanding could explain why only a few study participants referred children to nearby healthcare centers. Similarly, a previous study had reported that causal explanations for autism (such as supernatural causes, vaccinations, cultural beliefs, such as boys speaking later than girls, or speech delay being a good sign of intelligence) may influence help-seeking behavior. 20 which might further influence referral pathways of these children to health care services.
Additionally, participants who attended a didactic program on neurodevelopmental disorders in children were better able to identify persistent deficits in social communication and social interaction, as well as restricted, repetitive patterns of behavior, interests, or activities, in children with autism than those who did not attend such programs. However, this group had difficulty understanding that children with autism have difficulty reaching out to others easily, maintaining close relationships, showing attachment to inanimate objects, and responding to objects in unusual ways, such as smelling, touching, or tasting. This may be due to the nature of the didactics they received, which did not focus specifically on autism. Furthermore, autism is one such neurodevelopmental disorder that includes persistent deficits in social communication and social interaction and has restricted, repetitive patterns of behavior, interest, or activities. Hence, understanding disorders like autism may require special training to recognize the qualitative differences in communication patterns exhibited by children with autism, which can be difficult to comprehend unless specific examples and illustrations are provided, unlike categorical yes-or-no responses for other developmental disorders. A study on public health midwives found that participants who attended a particular program of training on autism had greater knowledge of autism than those who did not receive such targeted training. 21
Interestingly, the duration of work experience was not associated with participants’ knowledge of autism symptoms. Additionally, participants’ knowledge of the symptoms of autism was not influenced by whether they had attended a didactic program in the past six months or more than six months. This suggests that attending an educational program has a substantial impact on improving frontline health workers’ knowledge about autism. Those who participated in a didactic program on neurodevelopmental disorders were more knowledgeable in recognizing the symptoms of autism than those who did not 21 Considering the inadequate knowledge about autism among health professionals, studies have suggested the need to improve the knowledge level of autism through training programs, and many health professionals have expressed a strong interest in attending such programs on autism.22–26 Furthermore, there was no group difference among participants with different educational backgrounds in identifying the majority of autism symptoms, except for isolated symptoms in the social communication and social interaction categories. This might require further exploration in future studies. Overall, the abovementioned findings from the present study indicate the need for a specific awareness-building program on autism for frontline health workers, such as ASHA workers.
There were mixed opinions among ASHA workers regarding the treatment process in the present study. Some participants reported treatment modalities such as counseling, parent training, speech therapy, and occupational therapy, but did not include medication as part of autism treatment. However, others believe that children with autism require medicine in addition to nonpharmacological treatments such as counseling for children and parents, parent training, speech therapy, and occupational therapy. A few participants mentioned only one form of nonpharmacological intervention, such as counseling for children/parents, parent training, or speech therapy. Interestingly, none of the participants mentioned alternative treatment modalities such as Ayurveda, Yoga, Naturopathy, Unani, Siddha, or Homeopathy. This could be due to the limitations of the assessment used in the present study, as it provided a place to write down any other treatment modalities at the end of the assessment; however, the participants did not write anything there, and they just opted for the options provided in the assessment tool where none of these treatment modalities (Ayurveda, Yoga, Naturopathy, Unani, Siddha, or Homeopathy) were mentioned in the treatment list.
This study adapted items from the IASQ and modified them to assess participants’ knowledge of autism symptoms. We reframed some item statements from negative to positive and vice versa to reduce response bias. However, the validity and reliability of the Kannada version of the IASQ were not analyzed in the present study. Also, regarding “knowledge on the course of the illness,” we did not explore it extensively in the present study. Given these limitations in the assessment, future research could reframe all 10 items of the IASQ to better capture ASHA workers’ knowledge of autism symptoms and assess the validity and reliability of the Kannada version of the IASQ.
We acknowledge that the study employed convenience sampling rather than a stratified random sampling design, which may have introduced selection bias. Hence, the generalizability of these findings should be explored in future studies that include participants from different regions across India. Since most participants in the current study were high school educated and from a single district in Karnataka, it is essential to assess the awareness and knowledge of ASHA workers from other parts of the country, as this may inform the development of various community-level awareness-building programs by mental health professionals. Furthermore, at a policy level, developing a specific awareness-building program in addition to existing training programs for ASHA workers may help improve knowledge and awareness about neurodevelopmental disorders, such as autism, which could further aid in decreasing the delay in referring these children to early intervention centers.
Conclusions
In conclusion, the majority of ASHA workers reported autism as a mental illness and had difficulty identifying problems in social interaction and restricted, repetitive patterns of behavior in children with autism. The various ages, ranging from late childhood to adolescence, were reported as the earliest age for the diagnosis of autism. Participants who had previously attended awareness programs on autism demonstrated better knowledge levels in identifying autism symptoms. No significant group differences were found between participants’ years of work experience and educational background in identifying symptoms of autism.
Supplemental Material
Supplemental material for this article available online.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Data Availability Statement
Data will be available on request from the authors.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
AI was not used in manuscript preparation.
Ethics Approval and Informed Consent Statements
This study was approved by the Institutional Ethics Committee of Kasturba Medical College and Kasturba Hospital (Approval No. IEC Number: 286/2023 Date: 08-08-2023) and registered in the Clinical Trials Registry-India (CTRI/2023/12/060632). All the study participants provided informed consent, which the Institutional Ethics Committee approved.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Prior Presentations
The authors declare that the present study findings were not presented at any national or international conference.
Simultaneous Submission to Another Journal or Resource
The authors declare that the present study manuscript has not been submitted to any other journal or resource. We are submitting it to the Indian Journal of Psychological Medicine first time.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.