
Abstract
Purpose of the Review:
Attitudes toward mental illness and psychiatry (ATMIP) have been widely studied, and various instruments have been developed to assess them. However, the characteristics and psychometric properties of these instruments have not been comprehensively reviewed, leaving researchers uncertain about which scale to use in specific contexts. This review aims to synthesize the features of these scales, including their psychometric properties.
Collection and Analysis of Data:
Following Arksey and O’Malley’s scoping review framework, a comprehensive search was conducted across Scopus, PubMed, Cochrane, and Google Scholar. Studies reporting scales designed to assess ATMIP among medical students and healthcare professionals (HCPs) were included. Data were extracted on scale characteristics, domains, psychometric evaluation, and cultural adaptations. Twenty-two scales were eligible for inclusion. Most originated in Western contexts and were primarily developed for medical students and HCPs. The majority used Likert-type items or vignette-based assessments, and 19 scales (86.3%) reported psychometric evaluation. While most scales were initially developed in English and global south setting and later adapted to non-Western settings, contextual sensitivity and cultural validity varied. Overall, despite frequent reporting of psychometric properties, the applicability of these instruments across diverse cultural and educational contexts remains uncertain.
Conclusions:
This review provides researchers and educators with a consolidated understanding of existing scales, guiding informed use, adaptation, and potential development of culturally relevant instruments for ATMIP assessment. Careful selection and adaptation to local needs are essential to accurately assess attitudes toward psychiatry globally.
Keywords
The attitudes of medical students (students, henceforth) and Healthcare Professionals (HCPs) toward mental illness and psychiatry play a critical role in psychiatry teaching, students’ motivation to learn psychiatry, and pursuing it as a career.1,2 Poor knowledge about mental illness and associated stigma often create barriers to the identification of mental health conditions and the care delivery, emphasizing the need to explore attitudes of students and HCPs within healthcare settings. 3 Studies suggest that students and HCPs face several barriers to seeking mental health support, with mental health-related stigma being a significant factor.4,5 Even among senior students, worries about social judgment and stigma are widely prevalent, showing how negative attitudes toward mental illness can reduce help-seeking and affect engagement with psychiatry. 4 Concerns about confidentiality, uncertainty about where to get help, financial issues, and fear of negative academic or professional consequences often prevent students from seeking care. 5
Regular assessment of these attitudes among students and HCPs and their changes following an educational/antistigma intervention is crucial in terms of reducing mental health or psychiatry-related stigma. Furthermore, understanding the nuances of the students’ or HCPs’ knowledge, attitude, and practice toward mental illness and psychiatry in general can help gauge the problem and effectively address it.
Stigmatization is a complex social process that operates on multiple levels and often involves labelling, stereotyping, separation, loss of social status, and discrimination, usually within situations of unequal power. 6 It can be categorized into four main types: self-stigma, which occurs when individuals with mental health conditions internalize society’s negative beliefs about them; stigma by association, which affects family members or mental health professionals through the attribution of negative stereotypes; public and interpersonal stigma, which includes societal knowledge, negative attitudes, and discriminatory behaviors directed toward people with mental health conditions; and structural stigma, which is embedded in policies or institutional practices that disadvantage stigmatized groups. 6
Public stigma related to mental illness and psychiatry can be understood through three related elements: knowledge, attitudes, and behaviors. Limited or inaccurate knowledge contributes to misconceptions about mental health; attitudes mainly reflect negative emotional responses or prejudiced feelings toward individuals with mental health conditions; and discriminatory behaviors lead to social exclusion or other harms. 6 Literature on the medical students’ knowledge and attitude assessment toward mental illness or psychiatry, including scales developed to measure the same, often explores the issue in terms of stigma or negative attitude toward mental illness or psychiatry.
For assessment of stigma or negative attitudes (henceforth, attitude) toward mental illness and psychiatry (ATMIP), and subsequent intervention, reliable and validated tools are the cornerstone. 7 Various instruments or scales (henceforth, scales) have been developed to assess these attitudes, each with its unique methodologies, theoretical foundations, structure, targeted domains, and populations. 8 While some scales have been designed specifically for the students of health professions and HCPs, others have adapted tools initially designed for the general population. 9 Hence, evaluating the development, theoretical framework, characteristics, and psychometric properties of these scales is vital to use them in the proper context, thereby ensuring their utility in healthcare and medical institutional settings and for generating reliable and valid results.
Despite the significance of scales in studying ATMIP, with vast array of tools available to assess the same, a comprehensive review the same is lacking. More so, the ones primarily focusing on medical students and HCPs. The primary objective of this scoping review is to review and document characteristics of original scales developed to measure the medical students’ and healthcare professionals’ ATMIP.
The secondary objectives of this review are twofold: (a) to highlight the development process and psychometric properties (reliability and validity) of these scales, and (b) to explore the domains of these scales, including their relevance to assess attitudes and perceptions of medical students and HCPs towards mental illness and psychiatry.
Methods
In this review, we followed Arksey and O’Malley’s framework for scoping reviews, 10 which comprises five steps: (a) identifying the objectives, (b) identifying relevant studies, (c) study selection, (d) data charting, and (e) summarizing and reporting the results. This review was further guided by the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews) Checklist. 11 The completed checklist is uploaded as Supplementary Online Material.
Eligibility Criteria
We included original studies (quantita tive/qualitative/mixed-method), involving medical students (undergraduate or postgraduate trainees), and HCPs as the study population; based on instruments being developed/used to measure ATMIP; available in English, with full-text available. We did not apply any restriction on the publication period. Further, systematic reviews summarizing the development of such scales were also included. However, studies that used preexisting scales without reporting their development process or addressing unrelated psychiatric topics were excluded.
Information Sources
We conducted comprehensive literature searches using PubMed, Scopus, and Cochrane Library; Google Scholar search and bibliographic search were also performed to identify additional eligible studies, including gray literature.
Search Strategy
A systematic search strategy was employed using search terms such as “scale,” “tool,” “questionnaire” (for the instrument); “attitude,” “perception” (for attitude); and “mental illness,” “psychiatry”; and “medical students,” Healthcare Professionals (for medical students and HCPs). We also adapted these terms to the specific indexing systems of each database. (refer to Supplementary File A). Two investigators (first author and second author) independently searched each database to ensure reliable and accurate retrieval of relevant studies.
Selection Process
The selection process for potentially eligible studies was conducted in two stages. First, all search results were imported into reference management software, Rayyan, for organization and de-duplication. At this stage, two independent reviewers (first author and second author) screened the identified records based on the eligibility criteria. At the second stage, full-text reviews were conducted for shortlisted studies (initially by the first author, subsequently verified by the second author).
Data Charting
Data extraction was performed using a predefined charting form; variables were co-designed by the investigators to capture the details of each study. Extracted information included general information (e.g., scale's name, country of origin, year of publication), scale-specific details (e.g., number of items, domains, scoring system, availability in different languages), target population characteristics, strengths and limitations (as highlighted by the scale developer), and remarks by the current investigators (Refer to Table 1).
Summary of Key Findings from Included Studies on Instruments Assessing Attitudes Toward Mental Illness and Psychiatry (ATMIP).
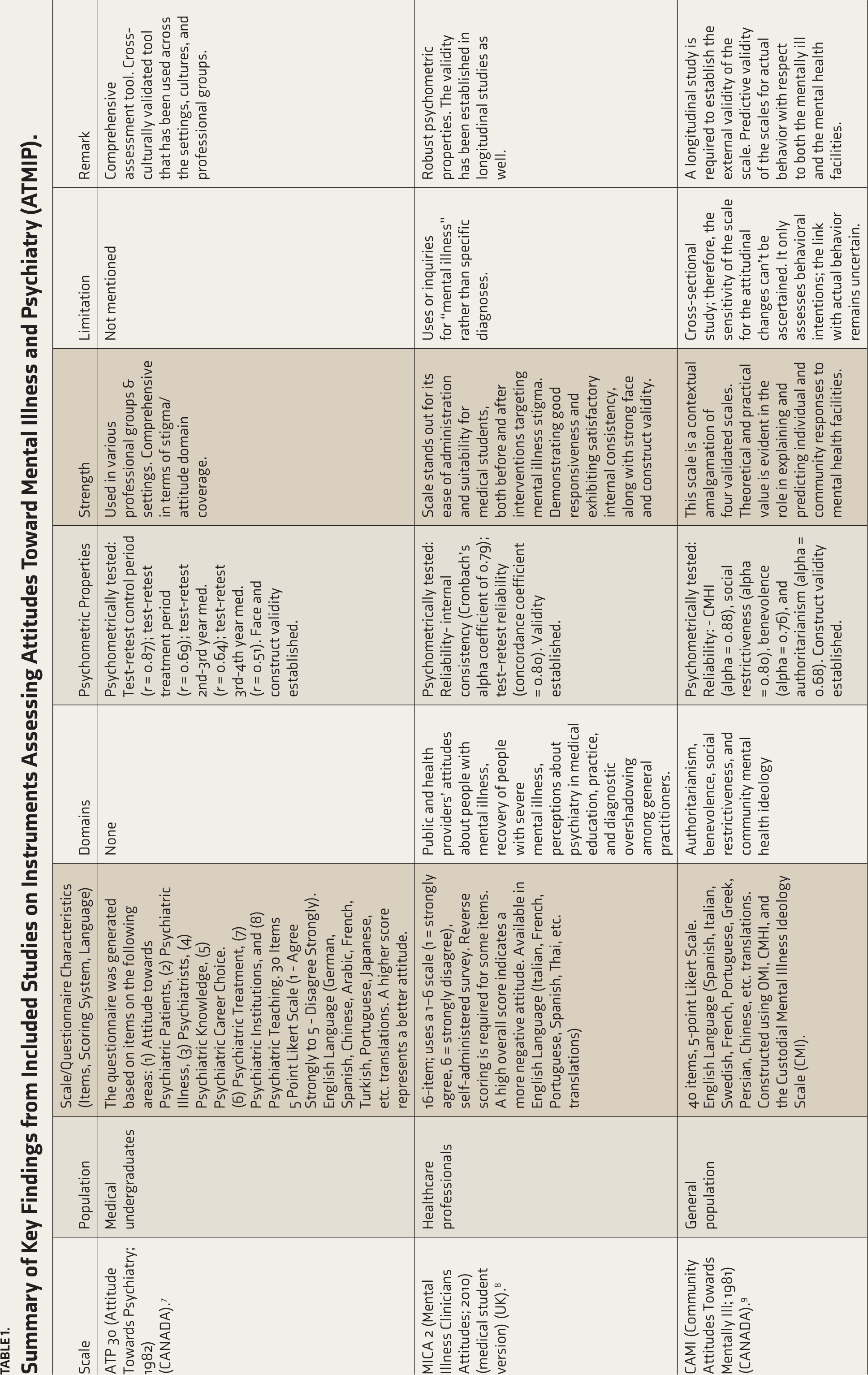
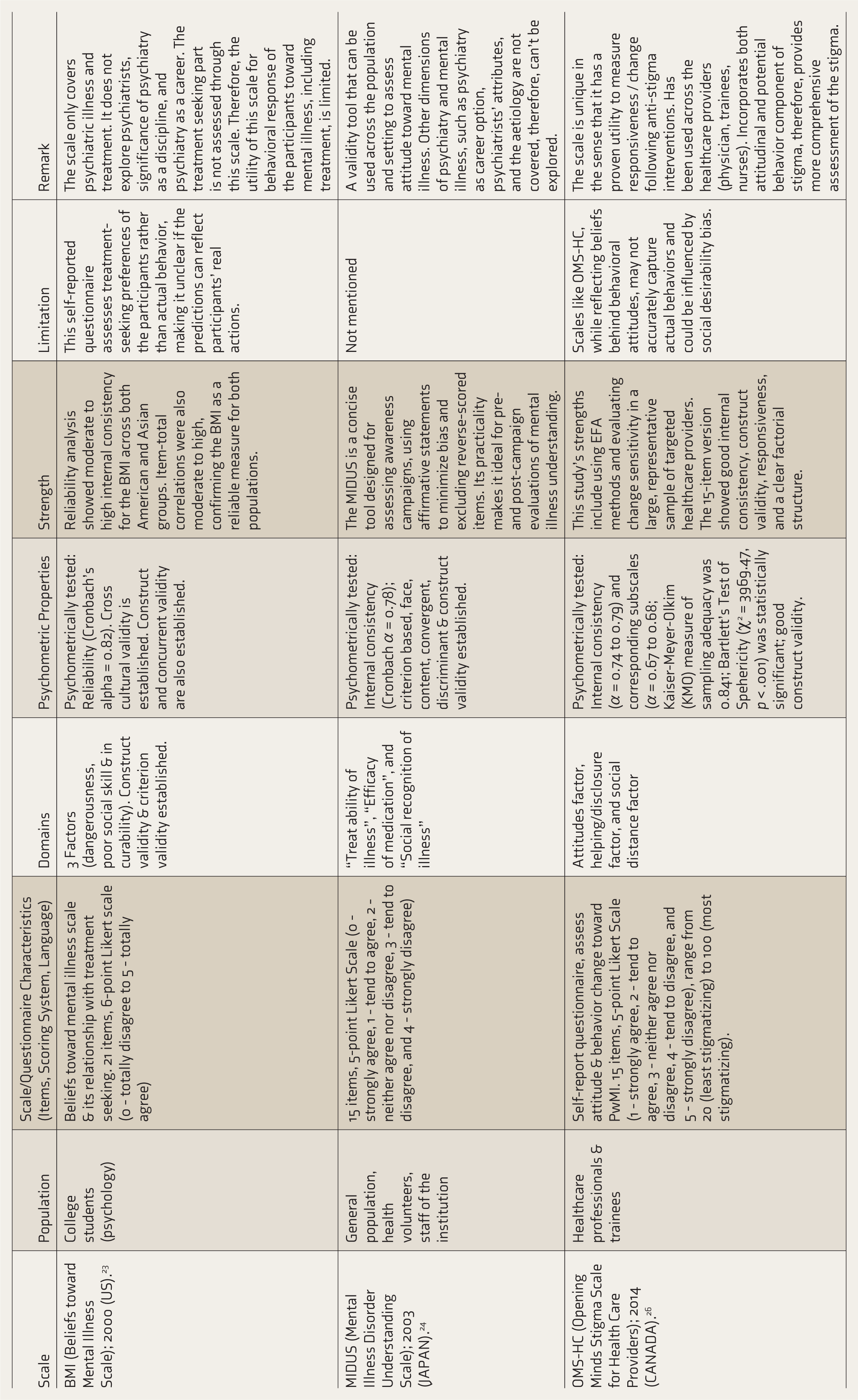
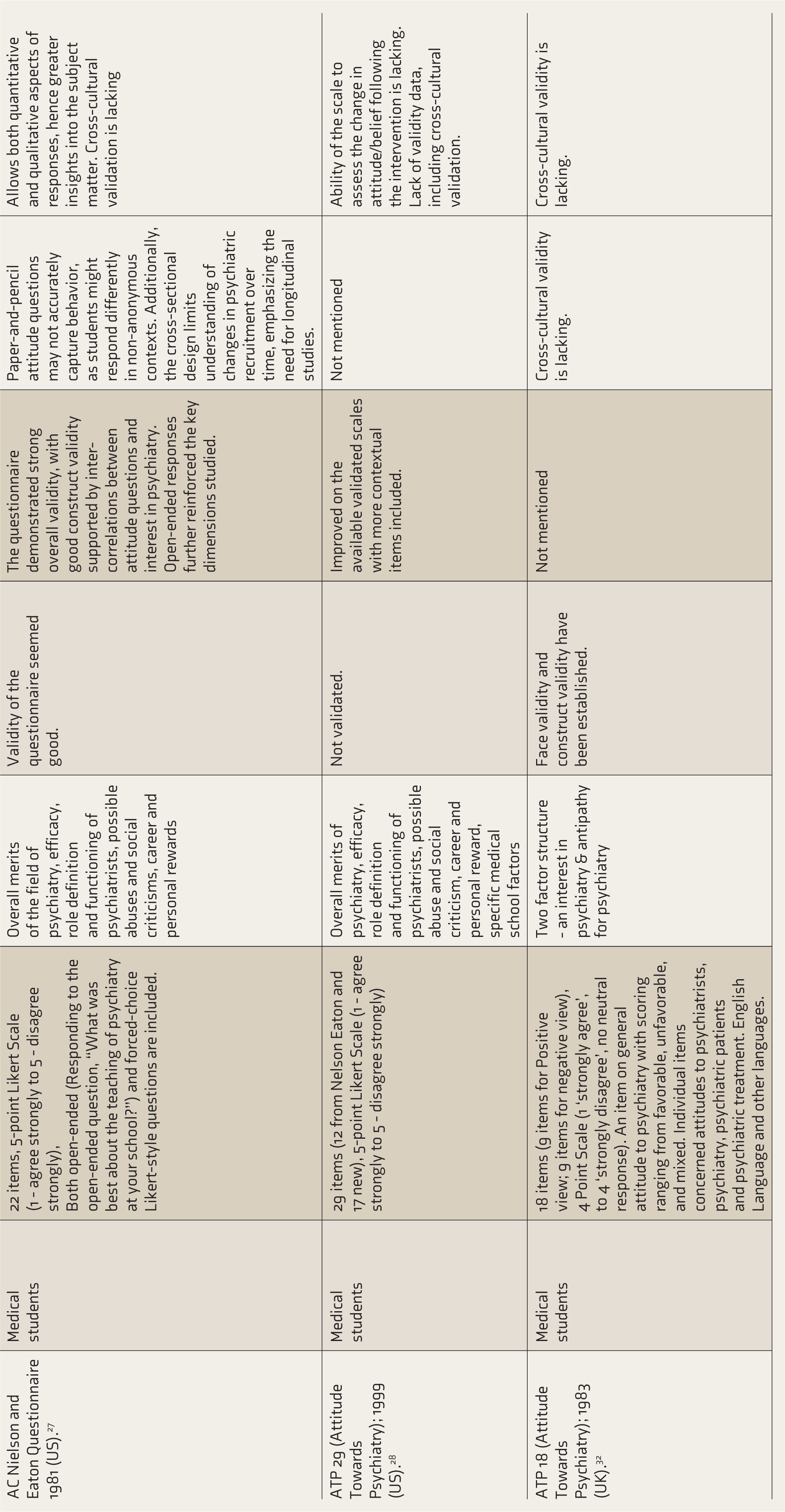
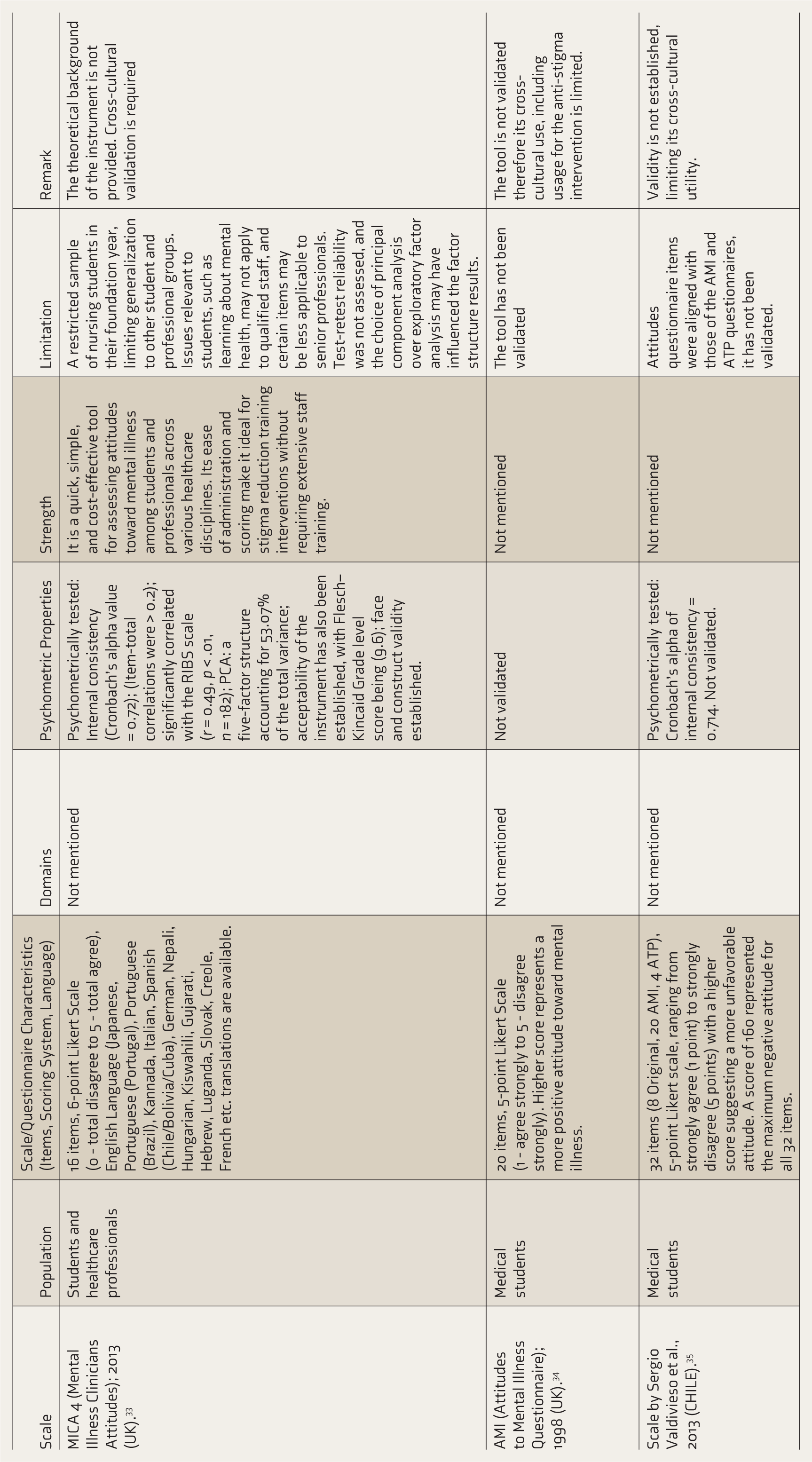
Furthermore, attention was given to the scale’s development process (theories, domains, etc.) and its psychometric properties (reliability and validity). The charting form was piloted on five studies under the supervision of a senior researcher involved in medical education and tool development (corresponding author) to ensure consistency and accuracy in data extraction and handling missing information. In case of any discrepancies among the reviewers, the issues were sorted through mutual discussion.
Synthesis and Presentation
We provided a detailed overview of the original scales developed to measure ATMIP. Also, scales’ critical aspects, including their development process, psychometric properties, domains, and intended applications, were synthesized and systematically evaluated. Subsequently, we provided our remarks on the individual scale (Refer to Table 1). For scales whose psychometric properties were not reported and where the original authors did not explicitly state that these indices were not assessed, we contacted the authors directly to request the missing information. Any details received were incorporated into our review to ensure completeness and accuracy of the data.
Results
Study Selection
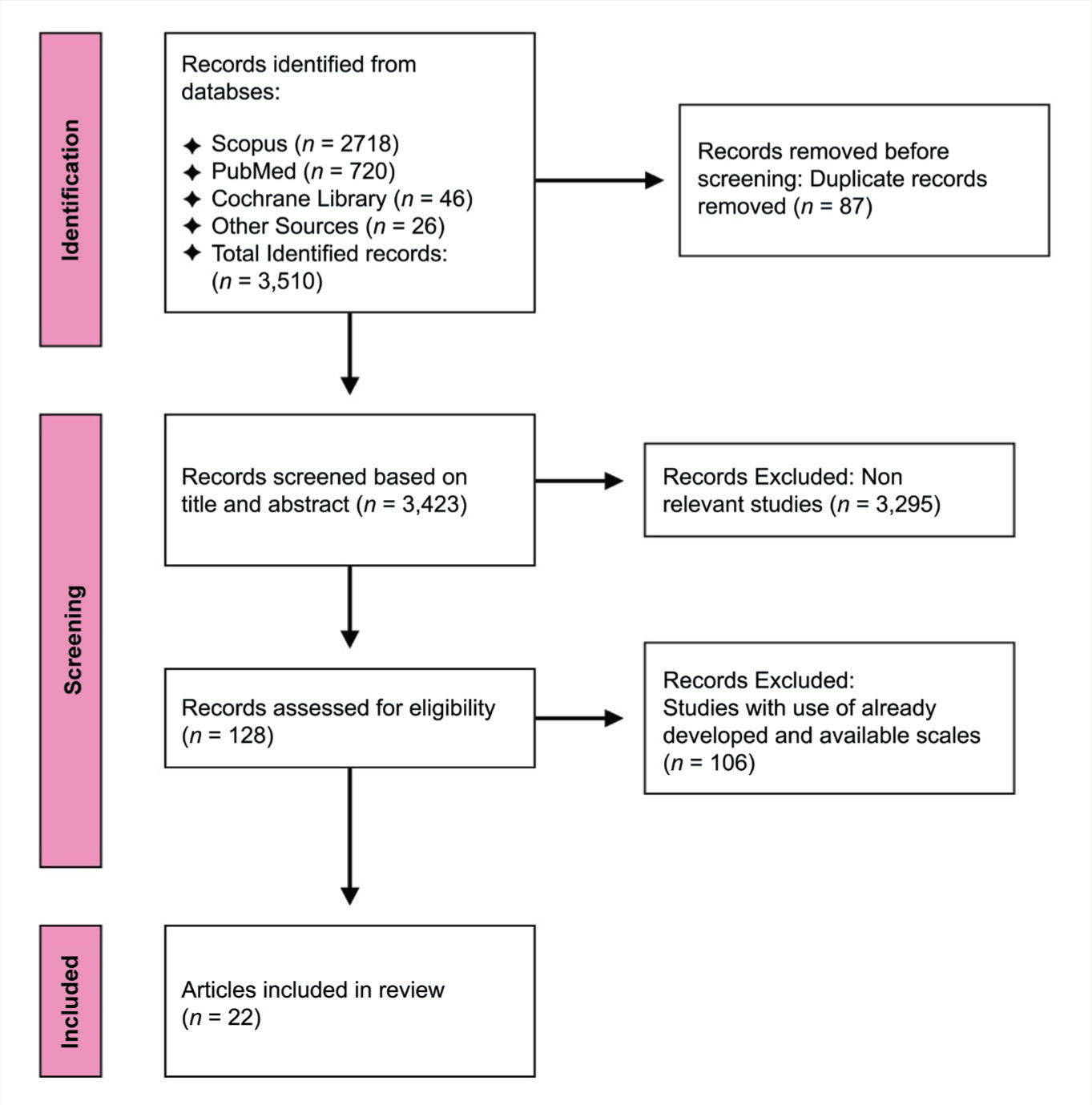
A literature search yielded 3,510 articles. After removing duplicates, title and abstract screening, followed by a full-text screening and a bibliographic search, a total of 22 original papers were identified. We followed PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines for the screening process (Refer to Figure 1). 11
PRISMA Flow Diagram.
Temporal and Geographical Distribution
Scale development was concentrated in the United Kingdom (n = 9) and North America (United States, n = 8; Canada, n = 3). However, we found one scale each from Japan and Chile, underscoring a global trend to evaluate ATMIP among HCPs and medical students.
Target Population and Adaptation for Other Populations
Out of the 22 scales, 16 (73%) were originally designed for medical students and HCPs. The remaining scales were initially developed for the general population and were subsequently adapted for medical students and HCPs.
Scale Characteristics
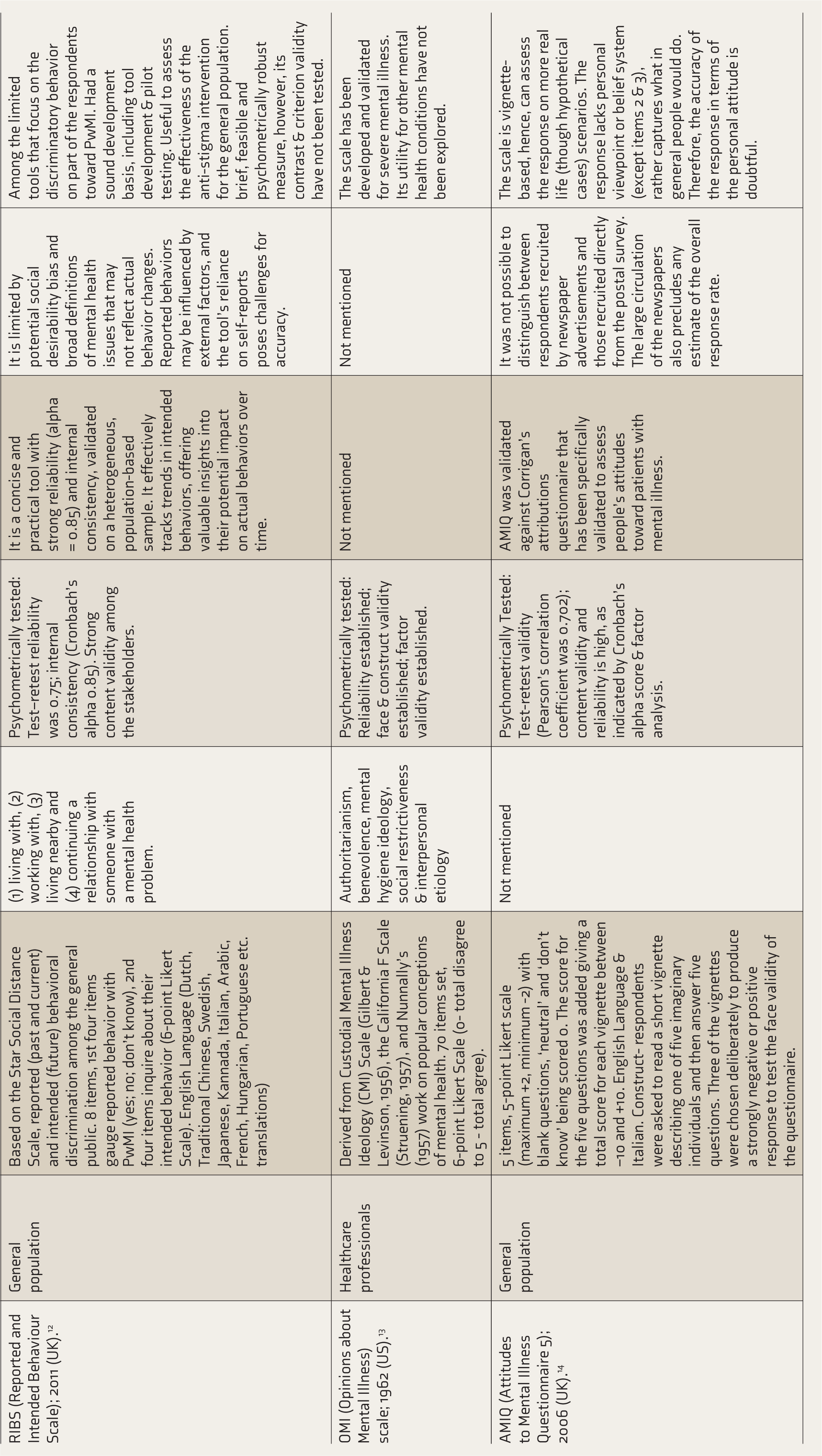
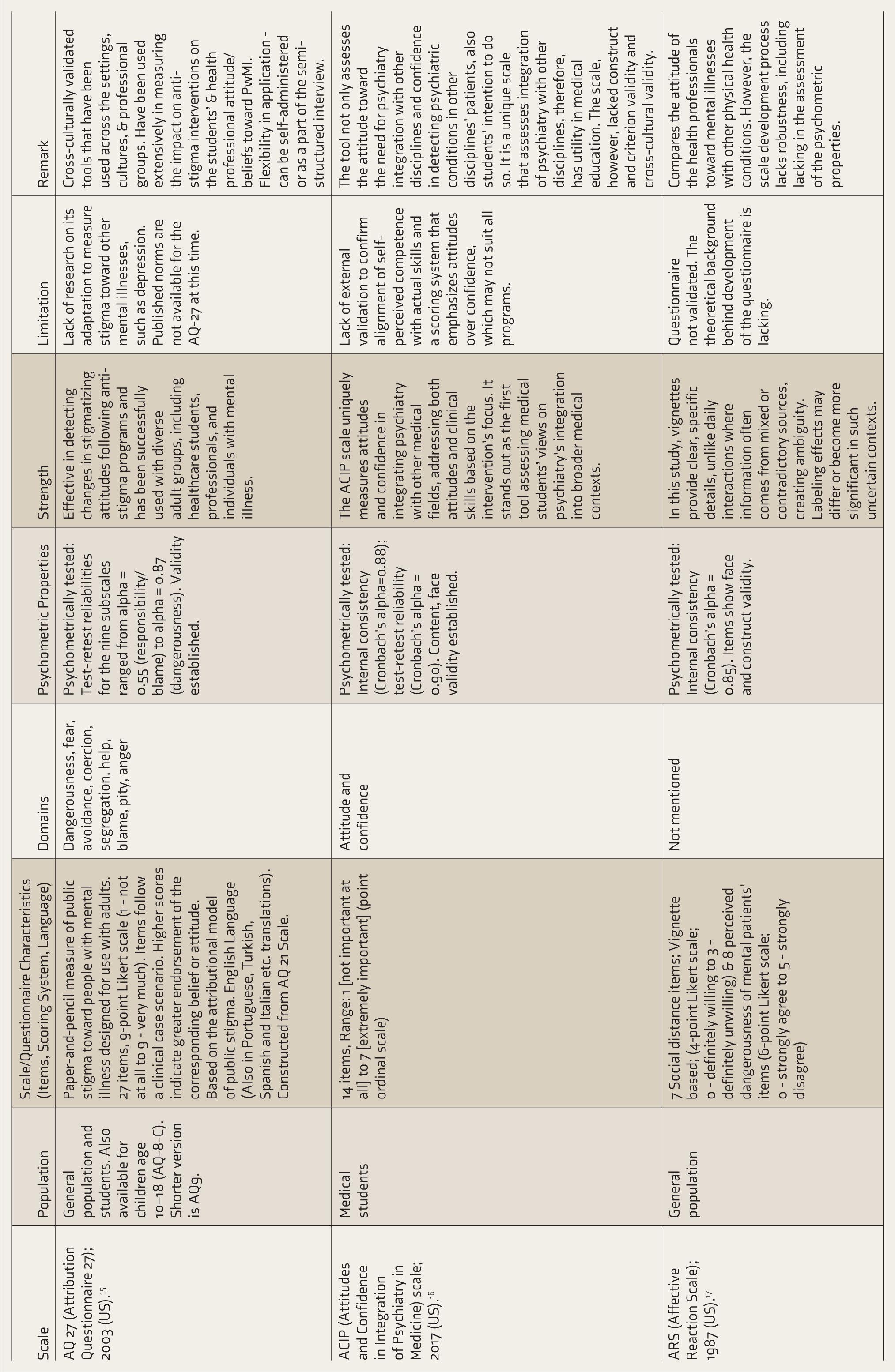
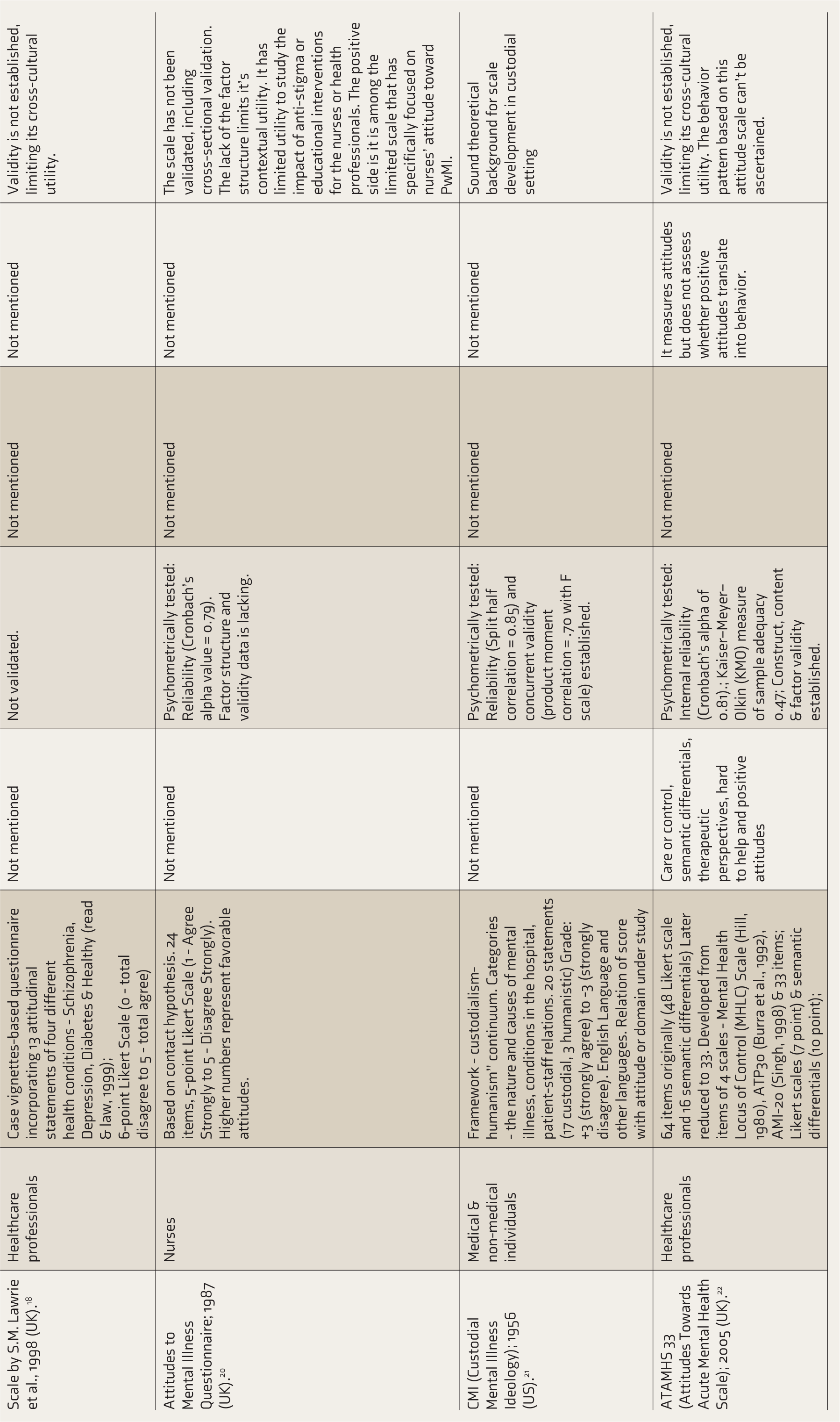
The scales varied widely in their structure and content. All were initially designed for pen-and-paper use except the Reported and Intended Behavior Scale (RIBS) (Online). 12 The item numbers ranged from 70 (Opinions about Mental Illness (OMI) scale) 13 to as few as five (Attitudes to Mental Illness Questionnaire (AMIQ)). 14 Some scales were derived from earlier tools, for example, Community Attitudes Toward the Mentally Ill (CAMI), 9 which was constructed using the OMI and Community Mental Health Ideology Scale (CMHI); similarly, Attribution Questionnaire 27 (AQ-27) 15 evolved from the Attribution Questionnaire 21 (AQ-21).
All scales used a Likert scoring pattern, with the number of points differing across instruments. Ten (45.45%) of these scales specifically employed a standard 5-point Likert scale, allowing for a balanced range of responses. Notably, Attitudes and Confidence in the Integration of Psychiatry (ACIP) 16 used a 7-point ordinal scale.
It is emphasized that tool developers have frequently used reverse scoring to test participants’ negative reaction or unfavorable ATMIP (e.g., Attitude Towards Psychiatry (ATP 30) and Mental Illness Clinicians’ Attitudes (MICA 2)), ensuring accuracy and minimization of response bias.
The Affective Reaction Scale (ARS) also employed a vignette-based approach. Additionally, it incorporated information such as income, grooming, and work behavior, along with general aspirations such as the desire to meet young women and secure a better-paying job. This approach is particularly valuable, adding validity to the assessment, given that some researchers have argued that labelling effects are most pronounced when minimal information is available for evaluation. 17
Another vignette-based questionnaire, the AMIQ, 14 further explores qualitative responses. Respondents are presented with a short vignette describing one of five imaginary individuals (for example, diabetes, depression, schizophrenia, substance abuse, etc.) and then asked to answer five follow-up questions. Authors observed that vignettes describing highly stigmatized individuals (e.g., a convicted criminal) consistently produced negative scores. In contrast, vignettes depicting non-stigmatized individuals (e.g., a Christian or a diabetic) resulted in positive scores, further supporting face validity.
The General Practitioners’ Attitudes to Psychiatric and Medical Illness Scale, developed by SM Lawrie et al., also followed a similar approach (Table 1). 18
Theoretical Basis of the Scales
Many studies described the underlying theoretical background for the tool domains. For instance, the ARS scale 17 is based on Scheff’s Labeling Theory, which suggests that individuals with history of psychiatric illness face stigmatization and rejection when reintegrating into society. 19 Following a vignette-based approach, it examines the interaction between labeling, perceptions of dangerousness, and social rejection, offering insights into mental health stigma.
The CAMI Scale (Community Attitudes Toward the Mentally Ill) is grounded on the theoretical framework proposed by Dear and Taylor, which suggests that ATMIP are shaped by personal characteristics (socioeconomic status, life stage, beliefs, and values) of the community members. 9 Moreover, their attitudes toward Persons with mental illness (PwMI) strongly influence their reactions to mental health facilities. The CAMI Scale comprises the public’s attitudes across four key domains related to PwMI and mental health facilities: Authoritarianism (viewing individuals with mental illness as inferior and in need of strict control), Benevolence (reflects a sympathetic and compassionate perspective, emphasizing care and support), Social Restrictiveness (captures fear and discomfort with PwMI, advocating for limited integration of individuals with mental illness into society), and Community Mental Health Ideology (supports community-based treatment and social inclusion of PwMI).
Likewise, the Weller and Grunei Attitudes to Mental Illness Questionnaire is based on the Contact Hypothesis, which suggests that group interaction can reduce prejudice under certain conditions. It assumes that mutual acquaintance fosters understanding, making it applicable not only to racial and ethnic relations but also to attitudes toward PwMI. Here, the authors have studied HCP-patient interactions in influencing stigma within mental healthcare settings. 20
Furthermore, the Custodial Mental Illness (CMI) Scale is based on the distinction between custodial and humanistic orientations in mental healthcare. 21 This framework aligns with theories of authoritarian and equalitarian personality structures.
Domains Assessed by Scales
Among the studies reviewed, only a subset has provided details on the domains assessed and their theoretical underpinnings. For instance, ATP 30 contains domains such as attitudes toward psychiatric patients, psychiatric illness, psychiatrists, psychiatric knowledge, psychiatric career choice, psychiatric treatment, psychiatric institutions, and psychiatric teaching (however, no such clusters emerged during the factor analysis). 7
The CAMI includes authoritarianism, benevolence, social restrictiveness, and community mental health ideology. 9 AQ27 covers dangerousness, fear, avoidance, coercion, segregation, help, blame, pity, and anger. 15 OMI includes authoritarianism, benevolence, mental hygiene ideology, social restrictiveness, and interpersonal etiology. 13 Attitudes Towards Acute Mental Health Scale (ATAHMS) assesses care or control, semantic differentials, therapeutic perspectives, hard-to-help, and positive attitudes. 22 The Beliefs Toward Mental Illness Scale (BMI) includes dangerousness, poor social skills, and incurability. 23 (See Table 1 for more details).
These domains reflect a broad spectrum of attitudes and beliefs, offering insights into various mental illnesses and psychiatric facets. For instance, AQ27 addresses the theory of public stigma (stereotypes, prejudice, and discrimination). It highlights the psychosocial consequences of public stigma, such as social rejection and restricted access to employment and housing. The scale emphasizes the importance of accurate assessments of public stigma to evaluate the effectiveness of anti-stigma programs. 15
Involving Qualitative Components in Tool Development
Although most scales followed quantitative measures to assess medical students’ and HCPs’ knowledge and ATMIP, two scales also incorporated qualitative aspects.12,24 Qualitative interviews can help in the development of quantitative measures by identifying key themes for rating scales, uncovering essential aspects of a topic that might otherwise be overlooked, or supplementing the quantitative measures for a comprehensive assessment of a phenomenon or a well-grounded theory. 25 Moreover, it helps content validate existing tools through cognitive interviews.
For instance, the Opening Minds Stigma Scale for Health Care Providers (OMS-HC) is part of the anti-stigma program by the Mental Health Commission of Canada, embedded in a larger national initiative aimed at reducing stigma. 26 The scale was developed by involving various stakeholders (sociologists, psychiatrists, and an anti-stigma campaign manager) to generate initial item pools, which were subsequently validated through cognitive interviews and by involving HCP, medical trainees, and persons with lived experience.
Similarly, RIBS underwent a rigorous development process. The initial items were selected based on expert review. This was followed by pre-pilot testing through cognitive interviews involving laypersons. Subsequent testing and validation followed a three-stage empirical testing process: Stage 1 involved face-to-face interviews with the participants representing the general population, Stage 2 included surveys involving participants of Stage 1, and Stage 3 refined the scale based on feedback from earlier stages, with online surveys used to test the final version. 12
Psychometric Validation and Language
A total of 19 scales (86%) were psychometrically tested in their original studies. Reliability assessment included test-retest reliability and internal consistency (commonly calculated as Cronbach’s alpha). Scales such as MICA-4 and MIDUS underwent rigorous tool development processes, for example, factor analysis (principal component analysis), reliability (internal consistency), validity (convergent validity, face validity) assessment, and acceptability, thereby establishing their broad utility for the concerned research.
All 22 scales were available in English, with several scales, such as Attitude Towards Psychiatry (ATP 30), MICA 2, MICA 4, RIBS, etc., also available in regional languages (e.g., Dutch, Chinese, Swedish, Japanese, Italian, Arabic, French, Hungarian, Portuguese) (Table 1). Many of these translated versions have also undergone validation (content validity and construct validity) and reliability testing to ensure their cross-cultural utility.
We also found that most of the scales used to measure ATMIP lack longitudinal reliability or validity, limiting their ability to measure change over time, including following anti-stigma interventions and exposure to psychiatry as a subject.
Importantly, scales such as ATP30, RIBS, MICA-2, and OMS-HC have undergone longitudinal psychometric assessment, underscoring their utility in this regard. The OMS-HC scale is unique in the sense that it has been widely used among HCPs (physicians, trainees, and nurses). It incorporates both attitudinal and behavioral aspects of stigma, allowing it to capture not just implicit biases but also potential discriminatory behaviors.
Similarly, the development process of the ATP30 scale involving medical students showed positive ATMIP following a direct and sustained exposure to psychiatric patients. 7
Qualitative Responses
In addition to quantitative assessment, one scale (AC Nielsen and Eaton et al.) 27 incorporates qualitative responses (open-ended questions, e.g., “what was best about the teaching of psychiatry at your school?”) with a Likert scale-based (forced-choice questions), allowing for qualitatively emerged themes to validate the forced-choice questions and to explore students’ opinions in greater detail.
Discussion
In this scoping review, we reviewed and documented the characteristics of the original scales and their development processes, including psychometric properties. Importantly, we explored the scale’s domains and factor structures, particularly in relevance to medical students’ and HCPs’ ATMIP. The latter has a crucial role in determining students’ or HCPs’ knowledge, attitude, and behavior concerning mental illness, PwMI, psychiatry, and considering it as a career.
We analyzed 22 original studies that developed scales to assess ATMIP. Most of these studies were conducted in developed nations, highlighting the need for further research in other geographical regions, particularly in developing countries, to capture diverse perspectives. Future research can focus on developing new scales tailored to the specific cultural and societal context of these regions or adapting and translating existing scales to ensure their cross-cultural validity.
Among the identified scales, 72.7% (n = 16) were specifically designed for medical students and HCPs. At the same time, the remaining six were initially developed for the general population but have since been adapted for use in medical education and healthcare settings. A key finding of our review is that 19 (86.3%) of the scales underwent psychometric assessment. However, ATP 29, AMI, and the scale by SM Lawrie et al. lacked formal psychometric testing despite their extensive use in research, thereby limiting their findings’ robustness and overall utility.18,28
While all scales were initially developed in English, many scales, for example, ATP 30, MICA 2, MICA 4, and RIBS, have been translated and validated in multiple languages, making them more versatile for cross-cultural research. It must be highlighted here that before developing a scale for cross-cultural settings, it is essential to understand whether the targeted construct reflects a culturally independent phenomenon and can be reliably assessed.29,30 Studies show that this can be achieved through techniques, such as conducting a literature review and engaging in qualitative research with the target population across different contexts. 29 In some cases, specific constructs, measures, or items may not hold universal relevance but are highly significant in specific settings. In such instances, the scale may be adapted to suit the context. Additionally, original scales often need to be translated into the relevant target languages to ensure accessibility and accuracy. 29
In terms of format, most scales use Likert-type responses, allowing for quantitative measurement of attitudes. However, scales like the one by Lawrie et al. employ qualitative assessment methods. Qualitative data-based scales provide deeper insights into individual perspectives on mental illness and psychiatry, complementing traditional quantitative methods. Research should incorporate qualitative nuances to assess students’ or HCPs’ ATMIP. 30
We found that only two-thirds of studies explicitly defined the constructs/domains (the idea, characteristic, or underlying behavior that a study aims to explore) of their scales. It is essential to clearly define and establish this domain before developing any scale. A well-defined domain helps create a clear understanding of the topic, sets its boundaries, and makes the process of designing relevant questions and content validation much smoother. 30
Our study also explored the theoretical basis underlying many of these instruments. Understanding the conceptual framework behind each scale is crucial for researchers selecting the most appropriate tool for their specific research and study population. 31
The strength of this review lies in its findings grounded in a comprehensive literature review using multiple databases, ensuring the incorporation of a wide range of available scales. A key strength of our study is the systematic review of the identified scales by two independent reviewers (first and second author), under the supervision of a senior reviewer (corresponding author). We adhered to established guidelines for scoping reviews to ensure that the data were presented in a structured, objective, and unbiased manner. We conducted an extensive and transparent search, making the process reproducible.
We opted for a scoping review rather than a systematic review, as our objective was to identify and compile all potential tools available for assessing medical students’ and HCPs’ ATMIP, thereby informing researchers to take up a more systematic approach to review this topic and identify the most suitable scale for their intended research. Additionally, we examined the theoretical framework, domains, and applicability of individual scales, allowing for a nuanced understanding of their strengths and limitations. It also provides valuable insights into the constructs measured by each scale, which can assist readers in interpreting the scales’ findings, including their psychometric properties.
Our work lays a strong foundation for the evolution of better-validated, cross-culturally applicable, and longitudinally tested instruments in the field of ATMIP. Finally, we not only summarized the strengths and limitations of each scale but also provided critical insights about it. This will be particularly useful for future researchers looking to select the most suitable instrument, identify research gaps in the existing scales, and develop new, more robust scales on ATMIP among medical students/professionals that are longitudinally validated and incorporate cultural contexts.
Limitations
We only included scales originally developed in English; they may have been translated into regional languages later. Although this approach ensured a standardized approach to review the topic, it may have led to the omission of some relevant scales developed in non-English-speaking regions. Additionally, our review focused only on the original and initial research in which each scale was developed; we did not include (or analyze) papers on its subsequent adaptations, modifications, or validations of these scales in later research. This means that scales' limitations identified in the original studies might have been addressed in later versions, but these revisions were not captured in our review. As a result, our findings may not fully reflect the most updated form of the scale and its applicability in contemporary research and practice.
Conclusions
Our review reveals that most scales used to measure medical students’ or HCPs’ ATMIP greatly vary in their characteristics, theoretical underpinnings, psychometric robustness, and importantly, societal and cultural context. Therefore, their applicability across diverse cultural and educational settings needs to be contextualized. Careful scale selection and adaptation to local needs are essential for accurate assessment of attitudes toward psychiatry globally.
This work can inform researchers and educationists to utilize the available scales on ATMIP more methodically, adapt the existing scales, and develop new scales to address the research question.
Supplemental Material
Supplemental material for this article available online.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Appropriate Permissions from the Concerned Authorities
Not applicable.
Data Sharing Statements
This is a review article and does not contain any studies with human or animal participants.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethics Committee Details
As this was a synthesis of data available in the literature, no patient consent or ethics committee approval was sought.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent/Assent
This article does not contain any studies with human or animal participants.
Prior Presentations
Not presented.
PROSPERO/CTRI Details
Not registered.
Registration
Not applicable for a scoping review.
Simultaneous Submission to Another Journal or Resource
Not submitted to any other journal or resource.
Status of Your Study (for Study Protocol)
Not applicable.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.