
Abstract
Background:
Undergraduate (UG) medical students are one of the stakeholders and ultimate beneficiaries of the competency-based medical education (CBME) curriculum introduced in 2019 by the National Medical Commission (NMC). There is a dearth of literature on student perspectives on CBME Psychiatry clinical posting in India.
Methods:
Second professional students who attended the psychiatry clinical posting were invited to participate in the qualitative study. They were asked to give perspectives about the training during clinical posting based on a semi-structured questionnaire.
Results:
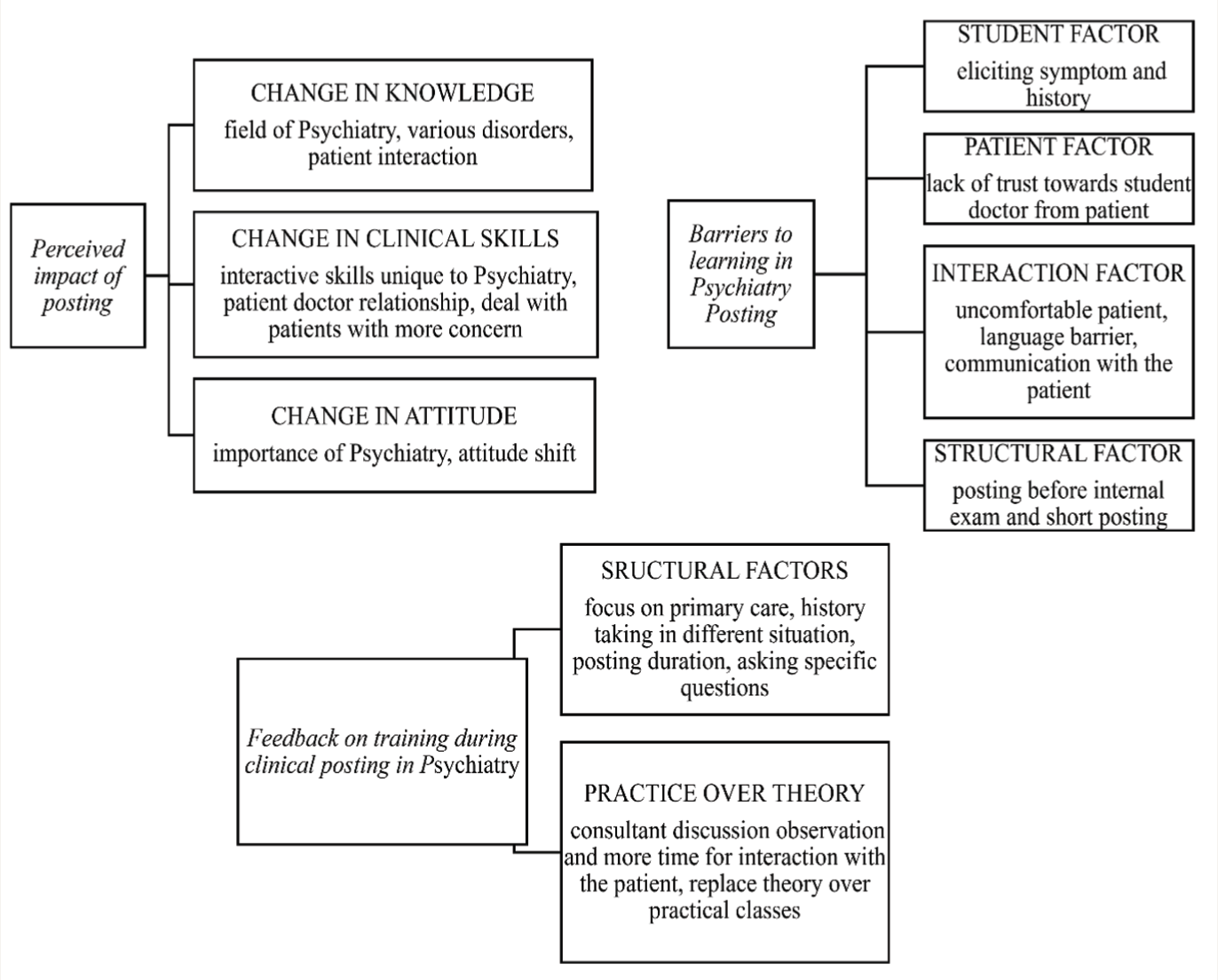
Written feedback forms were obtained from 44 students. Data were analyzed using thematic analysis. Results showed the perceived impact of posting (change in knowledge, skills, and attitude), barriers to learning (student factors, patient factors, interaction factors, structural factors), and feedback on training during clinical posting (structural factors, practice over theory).
Conclusion:
UG students perceived improvement in their knowledge, attitude, and clinical skills during their posting in Psychiatry. They reported several barriers to learning at variouslevels. Their feedback to improve the posting focused on demonstrating skills using patients rather than theory classes.
Keywords
Students perceive improvement in their knowledge, skills, and attitude during their posting in Psychiatry. Lack of trust toward students from patients, eliciting history especially from uncooperative patients, language barriers, and posting during their internal exam are perceived barriers to learning. Students’ feedback to improve the posting includes consultant-guided observation of discussion with patients, more focus on specific questions in history taking, and replacing theory with practical classes.Key Messages:
The National Mental Health Survey, 2016 showed that the prevalence of common mental disorders was 5%. 1 The treatment gap for common mental disorders in India is 80%. 2 There are only seven psychiatrists for every 10-lakh population. 3 With this severe shortage of human resources, doctors, especially in primary health care, need to be trained well in managing psychiatric patients. This requires definitive undergraduate (UG) psychiatry training to achieve basic skills in treating psychiatric disorders. 4
Competency-based medical education (CBME) was launched by the National Medical Commission (NMC) in 2019 to address gaps in UG training and make it structured and uniform across the country.5,6 The treatment gap in mental health care is given due recognition in CBME by including psychiatry as a subject of study and focusing on skill training rather than knowledge-based training.7,8,9,10 This is especially pertinent for managing patients with psychiatric symptoms in primary care. 11
Unique features of CBME include competencies, specific learning objectives (SLO), teaching-learning methods (T-L), elective domains, and a foundation course.5,12 Competencies are based on Bloom’s taxonomy of classification encompassing cognitive, psychomotor, and affective domains. 6 The cognitive domain refers to knowledge, comprehension, and application of information. Psychomotor skills mainly relate to planning and performing activities during learning. The affective domain refers to physician interaction with patients, such as receiving, responding, valuing, and showing empathy to patients. CBME mainly focuses on skill development through competencies and assessment of learning outcomes. 13 “Knows and knows how” are products of knowledge attributes where the student can describe and analyze the given clinical situation respectively. “Shows and shows how” are skill attributes where the student demonstrates steps and procedures involving knowledge, attitude, and behavior. 5 Responses to CBME from stakeholders are mixed. Faculty have reported inadequate training to impart the CBME curriculum and perceived it as difficult to implement.14,15
Some have argued that focusing on more than just skill-based training can be counterproductive. 13
There have been studies from India that have evaluated the attitudes of medical students toward psychiatry and mental illness.16,17 Students exposed to psychiatry clinical training, for example, fifth termers as opposed to earlier, 18 medical students more than interns, 19 and female students more than their male counterparts 20 seemed to have positive attitudes toward psychiatry training. All of these studies are focused on curriculum structure and implementation. Most of them are quantitative studies. A recent qualitative paper on UG Psychiatry training in the non-CBME curriculum explicated the needs and barriers of training as perceived by students during their clinical posting. 21 Findings from that study offered pointers to enhance teaching and training for UG medical students in psychiatry, making it more acceptable and beneficial for them. This article builds on the previous study by examining students’ perspectives of UG Psychiatry training in the CBME curriculum during their clinical posting. This study uniquely focuses on student perspectives on the CBME curriculum as the main contextual factor. The structure and implementation of the psychiatry curriculum have been discussed in detail. This study is unique in offering a qualitative perspective of medical students about a structured CBME curriculum. This has the potential to tailor the teaching curriculum and methods according to real-life practical clinical scenarios and the felt needs of the students based on their feedback.
Aims of the Study
To evaluate students’ perspectives of UG CBME Psychiatry clinical posting in the following domains: (a) Change in knowledge, skill, and attitude toward psychiatry, (b) barriers to learning psychiatry, and (c) feedback on training during the clinical posting in psychiatry.
Materials and Methods
Study Design and Setting
This qualitative study was conducted in the Department of Psychiatry in a tertiary care teaching hospital in South India. The hospital has 1300 beds, including 60 inpatient Psychiatry beds. It caters to the urban underprivileged population. When the study was conducted, the Department of Psychiatry had 13 psychiatrists, three clinical psychologists, and three psychiatric social work consultants. Ethical clearance was obtained from the Institutional Ethics Committee (IEC number 147/2021).
Research Team
All authors in this study worked as teaching faculty from the same setting with MD Psychiatry or DNB Psychiatry or PhD in Clinical Psychology. All of them were female except author 4, a male Psychiatrist. All the authors were part of the department’s Undergraduate Committee. They were involved in implementing the UG CBME Psychiatry Curriculum in the medical college from 2021. The corresponding author was part of the “Indian Psychiatric Society UG education Subcommittee” for drafting guidelines for the CBME manual for UG Psychiatry training. 22 The authors were interested in the perspectives of stakeholders of CBME, that is, students. Before the study started, the authors assumed that students would have more exposure to clinics and hands-on training in clinical postings in psychiatry with the CBME curriculum. All the authors have taken UG classes for the current second professional batch during the clinical posting. All the authors are well-versed in conducting qualitative studies.
Participant Recruitment
There is an annual intake of 150 medical students. The UG medical students of the second professional year were divided into eight batches comprising 18–20 students, each in a schedule predetermined by the Department of Medical Education. According to the National Medical Council-Competency-Based Undergraduate Curriculum document, these batches of students attended the first clinical posting in Psychiatry. 5
Inclusion criteria: UG medical students in their second professional year attending their first clinical posting in Psychiatry from July 2021 to November 2021.
Exclusion criteria: Students with <50% attendance in the clinical posting. Eighty-three students attended the clinical posting in psychiatry during the study period. On their first day of posting, students were informed that they were the main beneficiaries of CBME, and hence, the authors wanted to know their perspectives on the CBME curriculum.
We recruited students after written informed consent. Sixty-seven consented to participate, and one refused to participate. Fifteen students were absent on the first day of the posting and, therefore, needed to be enrolled. Consecutive sampling was used. We mentioned that end-of-posting marks will not be affected if they choose not to be part of the study. We assigned an alphanumeric code to each participant. The data were anonymized by removing all identifiers. The study was conducted according to Helsinki’s declaration.
Methods
The teaching program was based on the Draft Practical Guidelines for CBME, which were framed by the UG education subcommittee of the Indian Psychiatric Society. 22 Appendix 1 illustrates the time schedule for the clinical demonstration class in the medical college where the study was conducted. Table 1 depicts a sample schedule for alcohol use disorder.
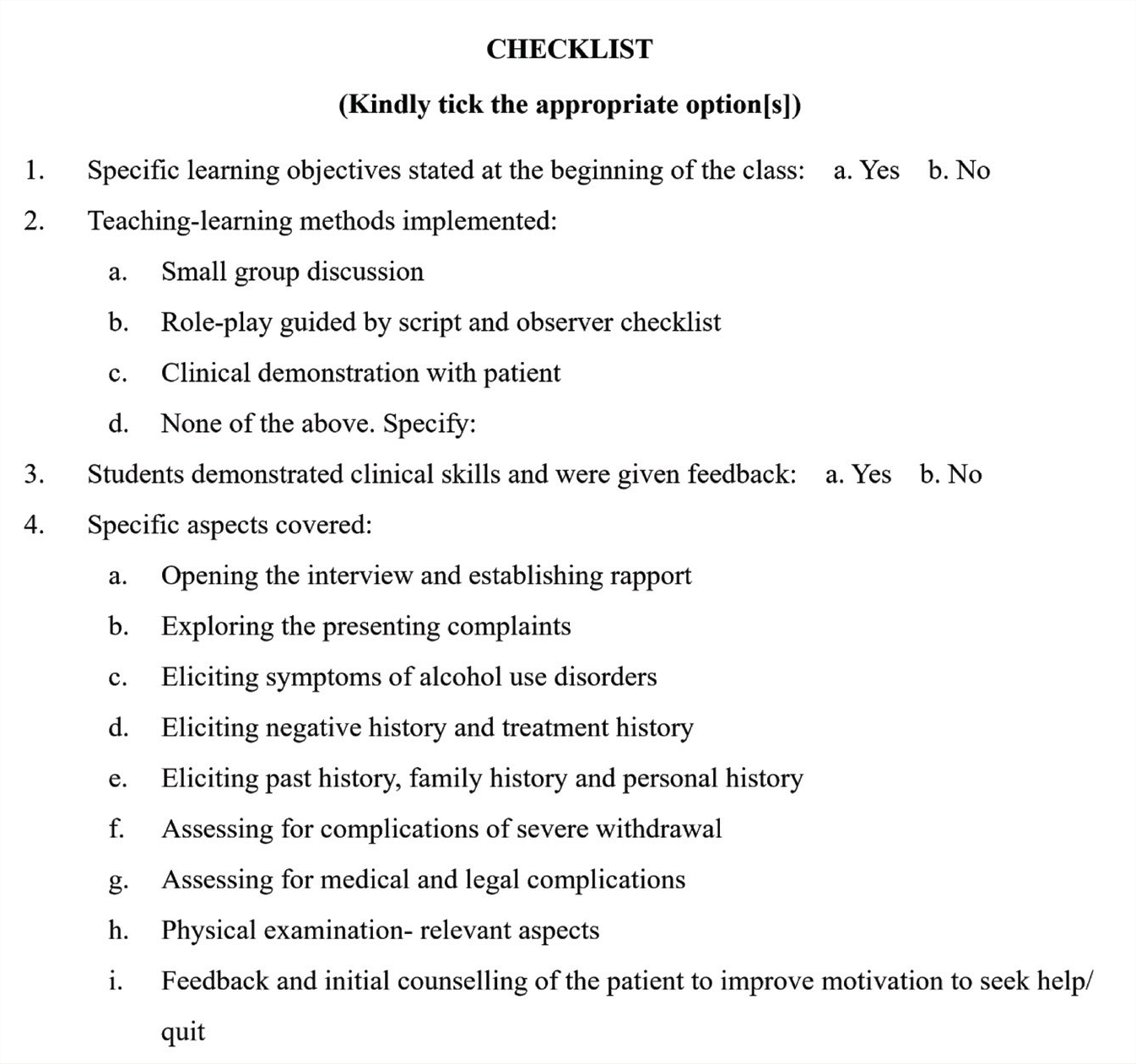
Teachers were given a written guideline for each clinical demonstration class: a checklist comprising competencies, SLOs, suggested T-L methods, and a lesson plan for a particular topic, as illustrated in Figure 1 for alcohol use disorder.
Sample Schedule of Clinical Demonstration Class for Alcohol Use Disorder.
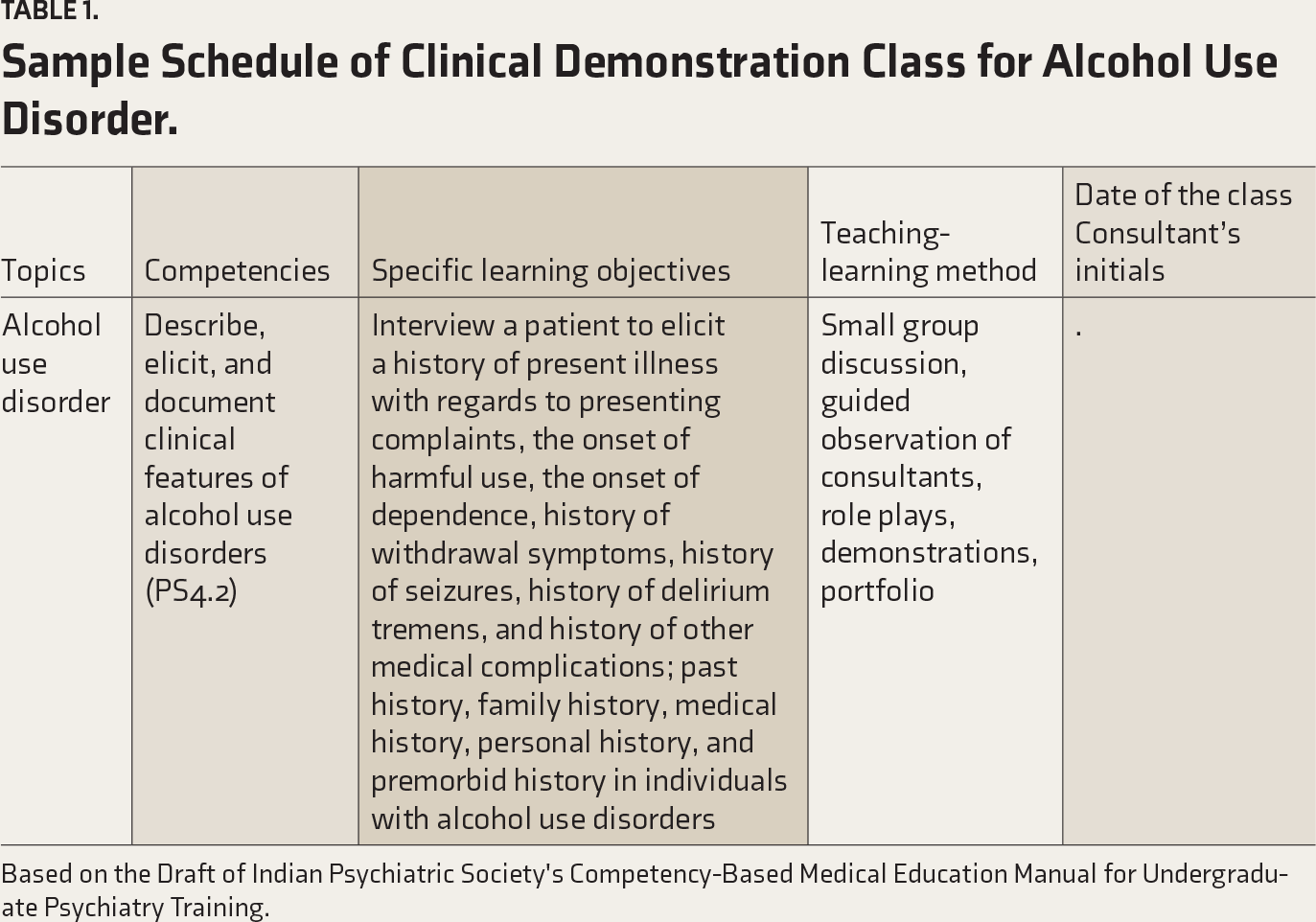
Based on the Draft of Indian Psychiatric Society's Competency-Based Medical Education Manual for Undergraduate Psychiatry Training.
Checklist/lesson plan for alcohol use disorder clinical demonstration class for second professional undergraduate students.
Topics were covered in separate sessions, each lasting around an hour. After classes, students were assigned a teacher in groups of 2–3. Students used learning portfolios with SLOs to guide their interactions with patients. Learning portfolios are tools to stimulate learning from experience. Appendix 2 shows a sample portfolio the students used in the medical college where the study was conducted. 23 The students and portfolios completed 23 clinical evaluations of the patient. Students were asked to document their reflective experience of fulfilling the SLOs in the portfolio sheets and their challenges during the clinical interview. Students would then discuss this with their allotted teacher for individual input from the teacher. The end of the posting was evaluated on the last day of the posting. It consisted of objective structured clinical examination (OSCE) and multiple-choice questions (MCQ). During this formative assessment, students’ extent of learning and skills developed were rated based on a structured marks scheme (checklist) by the examiners from the Department of Psychiatry. Individual feedback was given to students based on their performance in the assessment.
After the end-of-posting assessment, the authors with MD Psychiatry as a postgraduate degree (teaching faculty from the Department of Psychiatry) invited the students to give written feedback about the Psychiatry posting. This was organized in the psychiatry ward after the end of the posting assessment, based on a semi-structured questionnaire, as shown in Box 1. The authors and students were present alone while conducting and collecting the feedback forms. Approximately 10 minutes were given to each student to fill out the feedback forms. Feedback forms were retained by the authors for analysis. Written feedback from students was analyzed using deductive thematic analysis. 24
A Semi-structured Questionnaire for Feedback from Students Posted in the Department of Psychiatry.
Has this posting changed your knowledge, clinical skills, and attitudes toward Psychiatry? How?
Did you face any difficulties during the posting?
How can we improve the training during the posting?
Data Analysis
Thematic analysis was used to analyze the data according to the method described by Braun and Clark. 24 The data corpus, consisting of written responses to the semi-structured questionnaire, were analyzed manually in its entirety, forming the data set. A deductive approach consisted of predefined themes of the perceived impact of UG posting on knowledge, skills, and attitude, barriers to learning, and suggestions to improve the posting. This was in line with Braun and Clarke’s suggestions. 24 The first and second authors coded the data separately. Then, the first and second authors independently searched for subthemes, reviewed them, and defined and named the subthemes. All the authors jointly produced the report after discussion. Differences in structure and nomenclature of the subthemes were resolved by reaching a consensus through discussion among all the authors. Artificial Intelligence tools were not used in the data collection or analysis.
Results
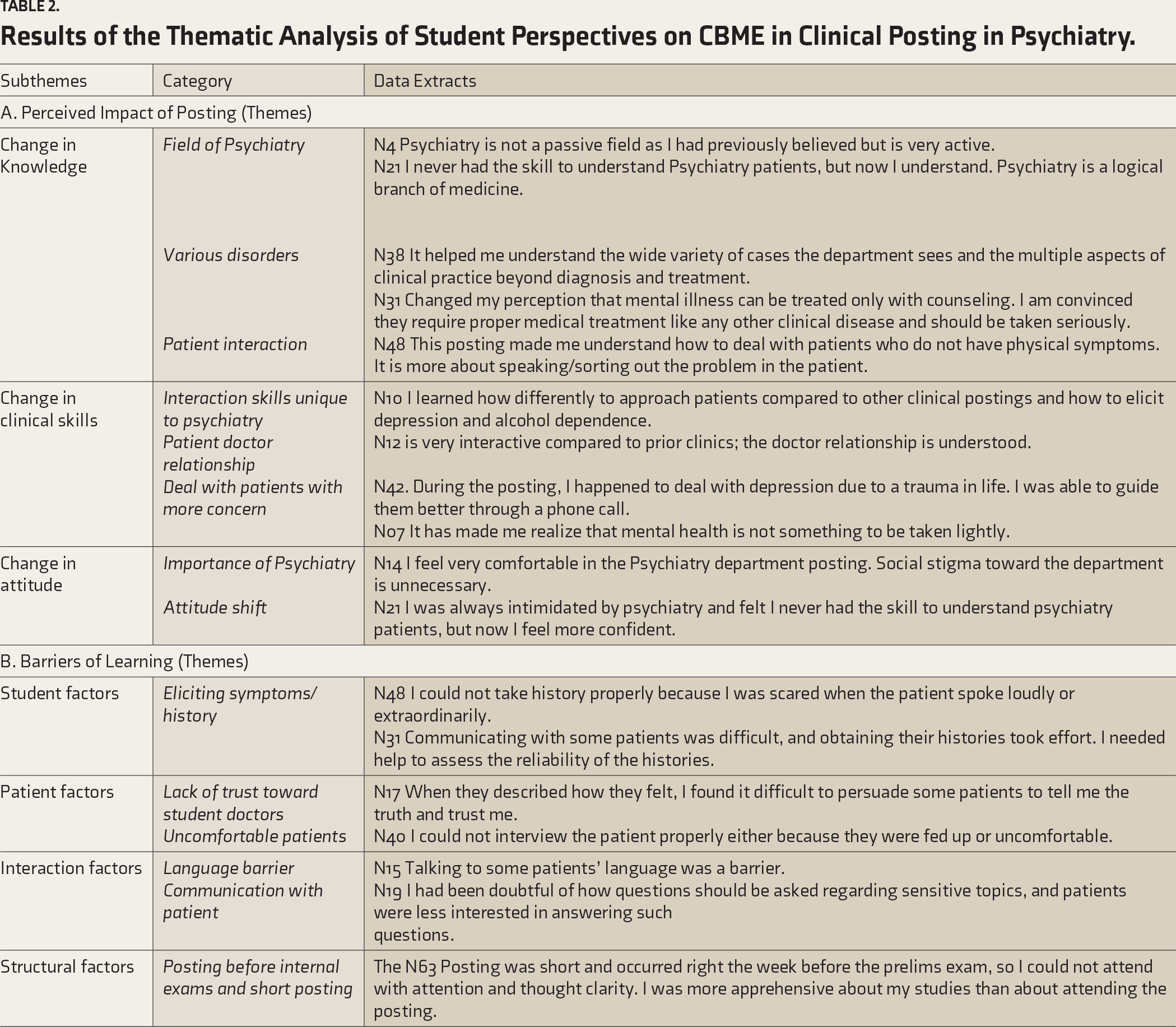
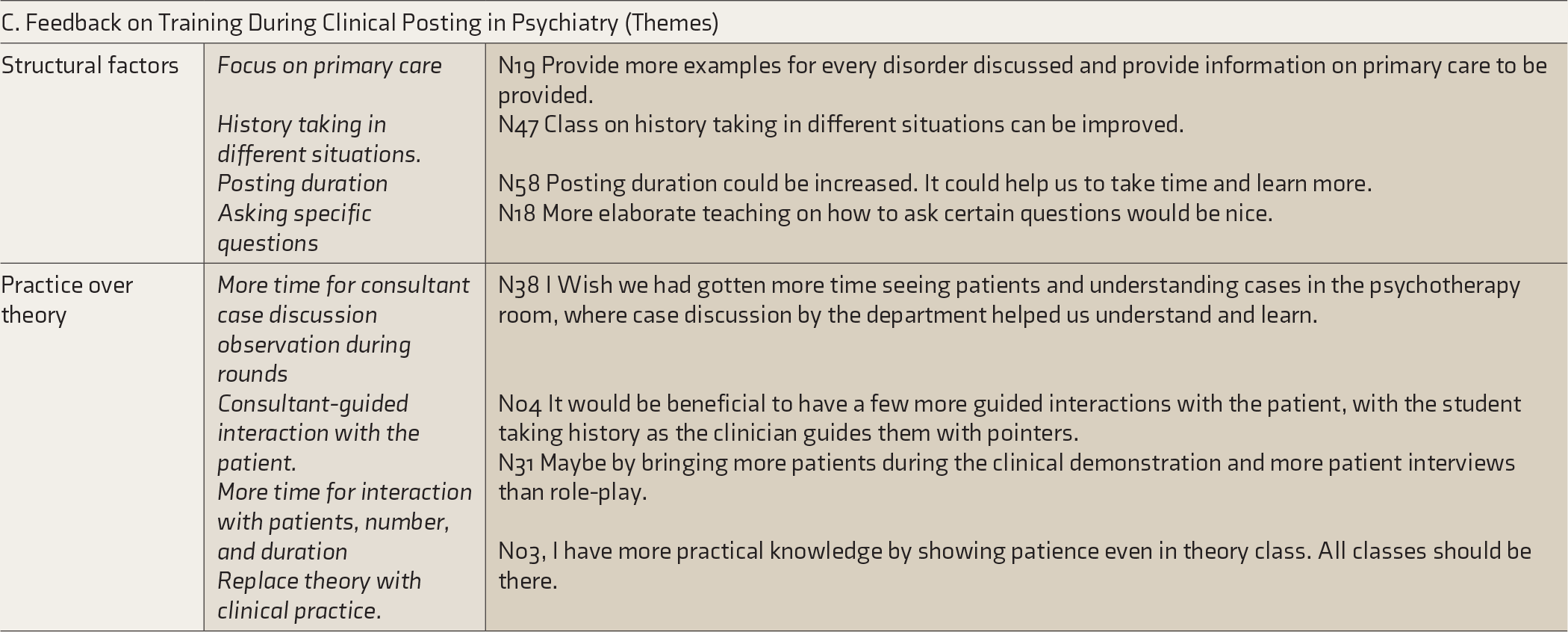
Of the 67 students enrolled in the study at the beginning of their posting, 44 students (11 males and 33 females with a mean age of 21.63±2.23 years) completed the feedback forms on the last day of their posting, which were included in the analysis. The rest did not attend the end of the posting assessment and hence dropped out of the study. The reasons for these 23 students not attending the end of the posting or completing the feedback forms were not captured as part of this study. The entire data set was analyzed.24,25 Table 2 shows the results of the thematic analysis. Themes and subthemes are illustrated in Figure 2. There was consistency between the students’ perspectives (data excerpts) and the results.
Results of the Thematic Analysis of Student Perspectives on CBME in Clinical Posting in Psychiatry.
The Framework of Student Perspectives on CBME Psychiatry Posting (Themes and Subthemes).
Discussion
Implementation of the CBME curriculum during psychiatry posting aims to improve students’ skills in dealing with patients with psychiatric disorders. Our findings shed light on students’ experiences on the first psychiatry clinical posting per CBME. We discuss the derived themes and their impact on knowledge, skill, and attitude. We also attempt to understand barriers to learning and how to improve the posting. This student feedback provides a valuable perspective in the context of students being essential stakeholders in the CBME implementation process. The discussion follows this article’s three important threads: the perceived impact of the posting, barriers to learning, and feedback on training.
Perceived Impact of the Posting
Students expressed a sense of increased knowledge in treating patients presenting with distress and unexplained physical symptoms. This is a welcome change in light of past research showing suboptimal skills in primary care physicians dealing with similar patients. 26 Students opined that Psychiatry was a “logical branch” and an active field of medicine. This could be due to students witnessing various techniques used by the consultants to elicit various signs of mental status examination (MSE). This contrasts with other studies from India where students perceived psychiatry as not precise and unscientific.19,27 Students in our study reported learning clinical aspects beyond diagnosis and treatment. The Department of Psychiatry at All India Institute of Medical Sciences, Rishikesh, has developed a model for UG Psychiatry training comprising neurobiology, lumping and splitting of disorders, formulation of short-term plans, clinical interpretation of lab reports, and is thus not limited to diagnosis and treatment. 28 This model was developed on the premise of the NMC document, which aimed to make the Indian Medical Graduate (IMG) a physician, scientist, administrator, and policy maker. 28 Our students understood that mental illness needs medical treatment like any other medical condition. Others have shown similar results. For example, the curriculum of Monash University provides as much importance to training students about psychiatric illnesses as other medical disorders. 29
Students in our study felt that stigma toward psychiatry was unnecessary. Correspondingly, fear of psychiatry was reduced among students, and confidence increased in dealing with psychiatry patients. Students reported to have understood the importance of mental health. We infer that students in this study had favorable attitudes toward psychiatry. Other studies have shown mixed results. A study on the impact of psychiatry training done on first and second-year students showed negative attitudes toward psychiatry and psychiatric illnesses. 30 However, a qualitative study noted that the type of UG Psychiatry teaching, exposure to Psychiatry during clinics, and charismatic teachers as role models were some of the reasons for choosing psychiatry for post-graduation. 31
This was supported by another study that suggested clinical exposure during psychiatry postings could change students’ perspectives on patient care and clinical practice and minimize stigma toward psychiatry and psychiatric patients. 16 These discrepant findings could be related to differences in settings, the level of available resources, and training received by teachers of Psychiatry. Manohari et al. recommend that teachers actively inculcate interest and remove stigma toward psychiatry. 32 Concerning students, attitude changes could occur in association with the use of strategies like elective postings, mentorship programs, and direct clinical assessment of patients by students.33,34
Study participants expressed that the clinical posting helped them learn interaction/communication skills, particularly in psychiatry. This is in keeping with the agenda of CBME to produce IMG with good communication skills. 11 Students also report “improved skills in the doctor-patient relationship.” IMG needs skills in developing doctor-patient relationships. 27 This helps in dealing with difficult or uncooperative patients in any branch of medicine. 4 Our students realized the importance of dealing with patients with empathy, which follows Attitude, Ethics, and Communication (AETCOM) principles. 35
Barriers to Learning During Posting
Students in our study expressed many barriers. Difficulties in assessing uncooperative patients and “loud” patients have been reported. The recommended strategies to overcome the barriers include simulation techniques and videos of agitated and uncooperative patients in the clinical classes. 33 Students reported a need for more trust by patients in students’ doctors. This is concerning as CBME has introduced the student doctor method of learning. It is thus important to address this. It should also be considered that traditional T-L methods are tough to employ in subjects like psychiatry. 33 This could be due to a need for more trust in student doctors, patient’s perspective of their therapeutic alliance with students, and patients’ discomfort with their presence in therapy sessions. Some strategies to address this could be the distribution of students across the teaching faculty, consultant-guided demonstration during patient interaction, and reduction in several student doctors in the therapist room.
Students in this study report barriers due to their inadequate expertise in asking sensitive questions; this has been shown even in postgraduate Psychiatry residents. 36 This perceived barrier could be overcome by consultants demonstrating how they handle sensitive issues of patients during outpatient clinics in the presence of a limited number of students. Students also reported challenges from external factors, like difficulty in assessing the reliability of history from informants. The posting timing and the patient’s language match the student’s language, which can be managed with prior planning. Barriers to learning, such as logistic issues and lack of interest in didactic teaching, were reported by the non-CBME batch. 21 Students have reported that the need for more effort in history taking is a deterrent to learning. Teachers could reflect that effort in history taking by students is expected to be a “process” of skillset development rather than an outcome. This may address the barrier reported by students.
Feedback on Training to Improve the Clinical Posting in Psychiatry
Students’ feedback was to emphasize clinical practice over theory. A study from South India examining first-year MBBS students’ perspectives highlighted the need for clinical exposure early in their careers. 37 Students emphasized that small group teaching should be implemented among the TL methods. 38 In a study about innovative teaching methods as discussed by students, patient-based clinical teaching and guided demonstration with patients have been perceived as useful by students. 39 So, case-based teaching is a suggested strategy to enhance learning in Psychiatry. 40 UG students will benefit from close professional relationships with consultants and senior residents for a positive teaching experience and attitude shift.33,41
Students in our study sought an increase in the duration of Psychiatry posting. Current CBME focuses on stipulated time for completion of specific skill sets. 11 The Original context of CBME was to give students time flexibility so they can complete skills at their own pace. 42 Another suggestion from students was for classes to focus on primary care. This is in keeping with the need for primary care physicians to identify and treat common mental health issues. 4 These reflect the cornerstone of CBME, which emphasizes skill-based learning over knowledge. 5 Students have suggested a specific focus on teaching history, taking in “different situations” and “asking specific questions” according to different situations. This reflects that students have been exposed to real-world case scenarios in the Psychiatry ward. Demonstration classes can include co-operative and non-cooperative patient assessment and special populations like elderly and young mothers and patients with medical co-morbidities. Skill-building sessions can be focused on eliciting effect and thought and asking sensitive/specific questions.
Strengths of the study
Students are the stakeholders, and this study discusses student perspectives on the CBME curriculum. This is one of the few qualitative studies on students’ perspectives on the CBME curriculum in UG Psychiatry clinical posting in India. Qualitative studies provide depth of information about students’ perspectives. The availability of students’ perspectives on CBME and non-CBME curricula may help in the future to compare the benefits of both curriculums.
Limitations
The findings are not generalizable to government colleges or resource-limited settings. However, similar questions in settings with resource constraints can be beneficial in ascertaining the associated themes that emerge. A formal quantitative assessment of change in stigma toward Psychiatric disorders was not measured. This is the qualitative reporting of students. We have yet to receive feedback from faculty or patients whom students interviewed.
Conclusions
UG students perceived improvement in their knowledge, attitude, and skills in the context of CBME Psychiatry posting. They perceived numerous barriers in real-world scenarios. Their suggestions focus on the structural level and emphasize clinical exposure over theory teaching. Program evaluation models of CBME UG posting are needed in the future, which will guide the refinement of the CBME curriculum implementation.
Supplemental Material
Supplemental material for this article is available online.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
The authors state that the current article has not been published or been accepted for publication elsewhere. The manuscript has been read and approved by all the authors. We believe the requirements for authorship have been met. The authors believe that the manuscript represents honest work. Authors state that the manuscript does not infringe upon any copyright of any third party to the best of their knowledge.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
All participants provided written informed consent.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.