
Abstract

India faces a substantial treatment gap in mental health care, estimated between 70% and 92% across major disorders. 1 This gap stems from limited mental health resources, workforce shortages, and pervasive stigma, particularly in rural and underserved regions. 2 The pandemic further widened this divide, heightening psychological distress and disrupting already strained service delivery systems. 3
A critical but less-examined dimension of this divide is the psychosocial care gap, the mismatch between mental health needs and the availability of psychosocial interventions. 4 Psychosocial care, which integrates psychological therapies, family support, and community-based approaches, is vital for recovery and social functioning. 5 However, access remains highly unequal, with stigma, low awareness, and inadequate integration into primary care limiting its reach. 6 Addressing this gap requires scalable, context-sensitive, and sustainable solutions that can strengthen the continuum of mental health support.
Technological innovations, particularly telepsychiatry and collaborative video consultations (CVCs), have emerged as promising models to bridge this divide. 7 Evidence suggests that digitally enabled capacity building initiatives enhance the competence of frontline health workers, extend specialist supervision, and facilitate continuity of psychosocial support. 8 Such technology-supported interventions align with India’s efforts to integrate mental health into primary care under the National Mental Health Program. 9
In response to these challenges, the National Institute of Mental Health and Neurosciences (NIMHANS) collaborated with a Corporate Social Responsibility (CSR) funded capacity building program named “A Pan India Digitally Driven Capacity Building Program to strengthen Primary Mental Healthcare.” The program addressed frontline workers’ training needs while integrating evidence-based practices to boost mental health literacy, improve crisis response, and reduce stigma. Through telemedicine, it reached regions like Karnataka, training over 10,000 professionals, including medical and community health officers (CHOs).
The program employed a robust training methodology tailored to various cadres of healthcare workers. Modules in English and Kannada were delivered online, with each 120-minute session ensuring engagement and understanding. To address digital literacy gaps, a hybrid approach was used with a WhatsApp group for communication and support. Post-training, case discussions, and CVCs ensured continued guidance and service quality. Informed consent was obtained from all participants before data collection. The study was approved by the Institutional Ethics Committee (IEC) (Approval No. NIMHANS/43rd IEC (BEH.SC.DIV) 2023, dated December 8, 2023) and registered with the Clinical Trial Registry of India (Registration No. CTRI/2024/02/062906). Detailed specifics, procedures, and modules of the training program are explained elsewhere. 10
This article examines how technology-enabled collaborative models can effectively bridge the psychosocial care gap in India’s primary mental healthcare system. Drawing on case examples from Karnataka, this article highlights the feasibility, benefits, and policy implications of CVC-based digital supervision to enhance access, quality, and equity in psychosocial care.
Case Series
This case series illustrates the effectiveness of collaborative, technology-enabled psychosocial interventions delivered by CHOs across diverse mental health conditions. Each case demonstrates how structured tele-assistance and CVC mechanisms facilitated continuity of care, family engagement, and community reintegration. A detailed summary of psychosocial gaps, interventions, and outcomes is presented in Table 1.
Addressing Psychosocial Care Gaps Through Collaborative Care Interventions.
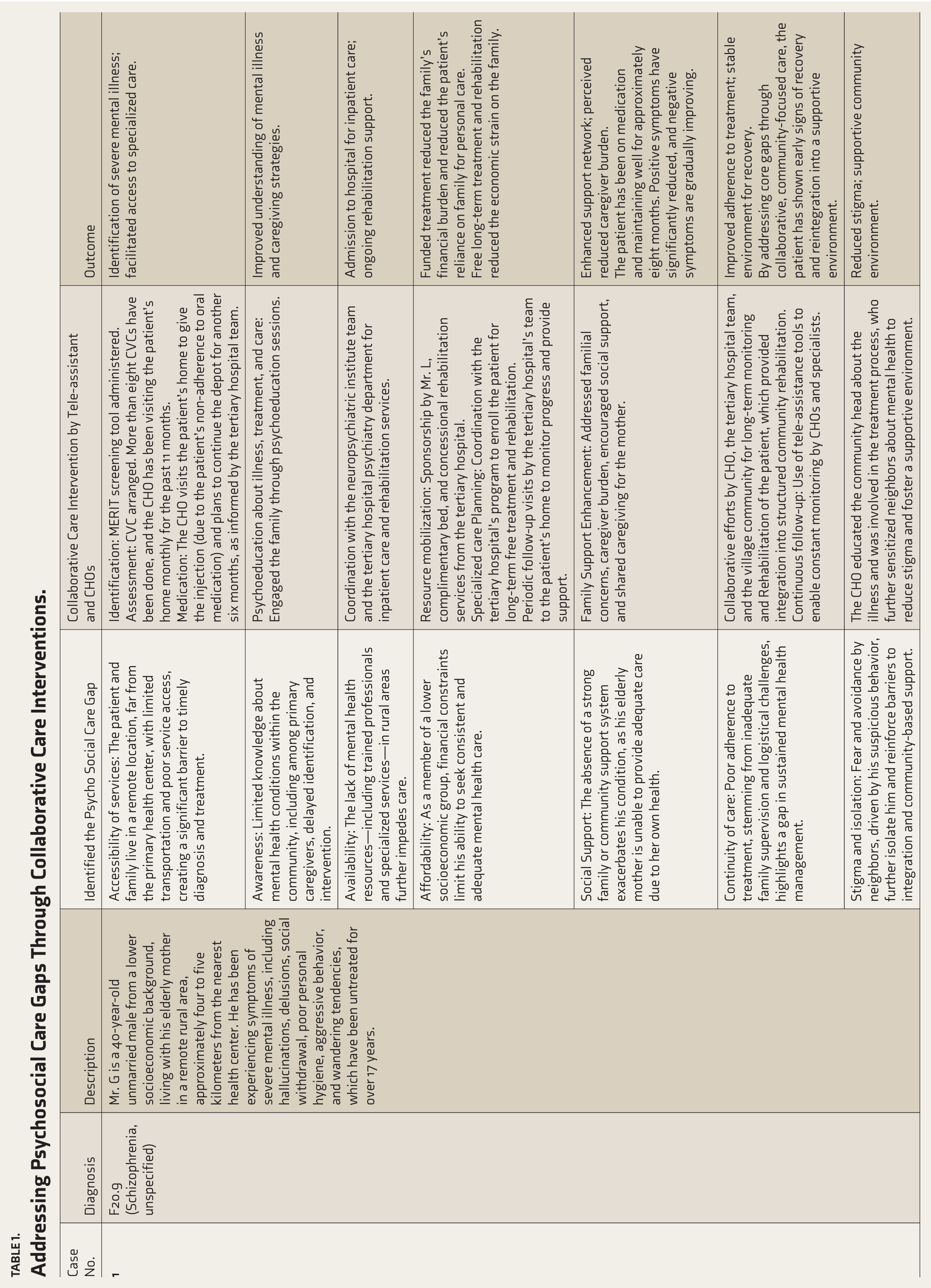
CVC: Collaborative video consultation; CHO: Community health officer.
Case 1: Schizophrenia with Long-term Untreated Illness
Mr. G, a 40-year-old unmarried male from a lower socioeconomic background, resided with his elderly mother in a remote rural village nearly five kilometers from the nearest health center. He had a 17-year history of untreated psychotic symptoms, including auditory hallucinations, delusional beliefs, social withdrawal, poor self-care, and occasional aggression. Before identification by the CHO, he had never received a formal psychiatric evaluation.
Mental Health Screening and Coun-selling Tool (MERIT) screening facilitated early detection of severe mental illness. Subsequently, more than eight CVCs were held with a neuropsychiatric institute over 11 months. Given poor adherence to oral medication, the care team initiated depot antipsychotic therapy administered monthly by the CHO during home visits. The intervention also included family psychoeducation, linkage to subsidized rehabilitation services, and mobilization of local resources. With support from a tertiary hospital program, the patient received free inpatient care followed by community-based rehabilitation.
After approximately eight months of treatment, positive psychotic symptoms markedly reduced, while self-care and social interaction gradually improved. The family reported reduced caregiving burden and improved understanding of illness. Community awareness sessions conducted by the CHO and village leaders contributed to reduced stigma and enhanced social inclusion.
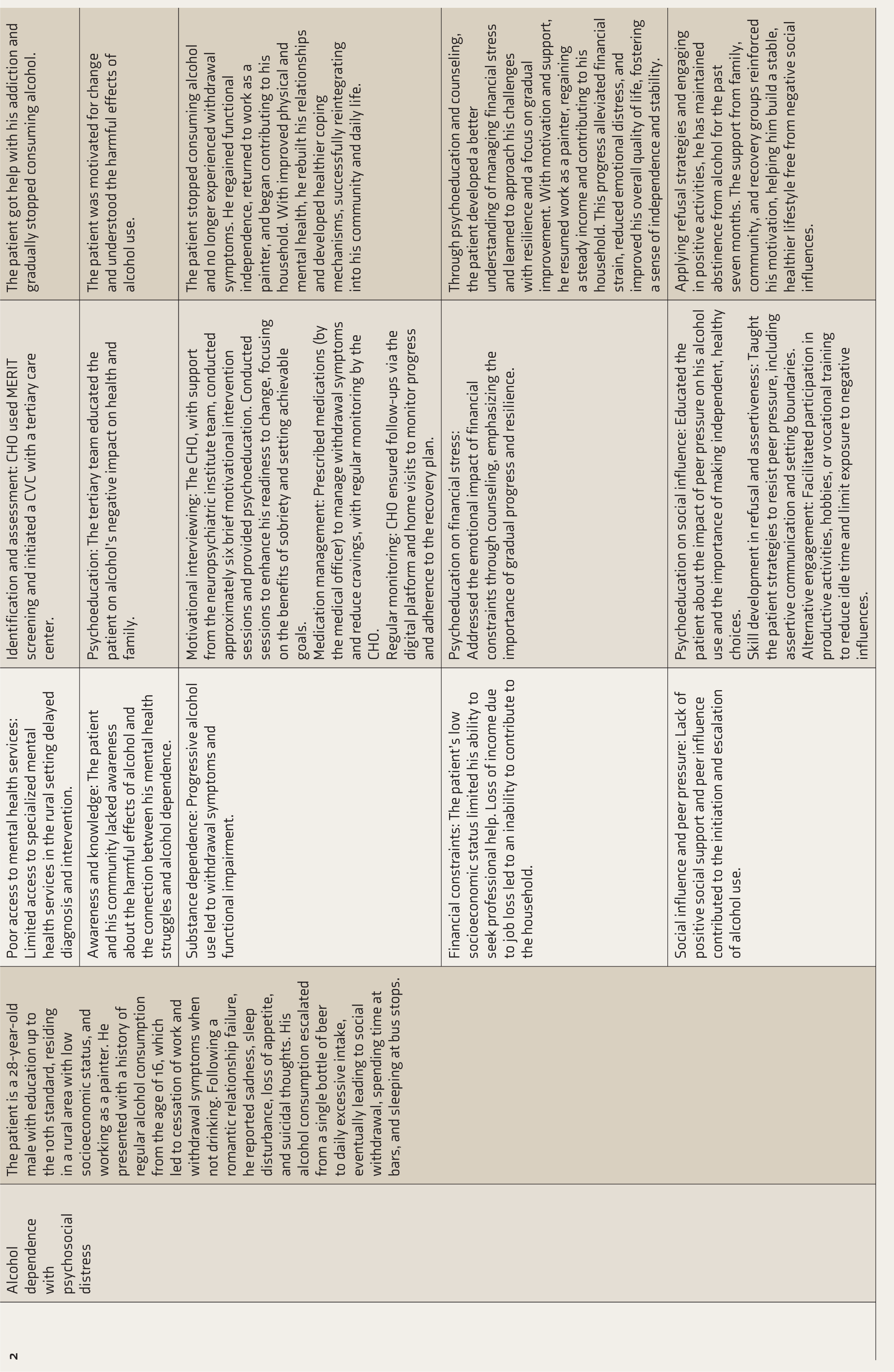
Case 2: Alcohol Dependence Syndrome with Psychosocial Distress
The second case involved a 28-year-old male painter from a rural, low-income background with a 10-year history of escalating alcohol use beginning in adolescence. Following a romantic relationship failure, he developed depressive symptoms, insomnia, and suicidal ideation. He had no prior exposure to mental health services and initially sought help for physical withdrawal symptoms.
The CHO conducted MERIT screening and arranged tele-consultations with a tertiary care psychiatrist. A combination of motivational interviewing, psychoeducation, and withdrawal management was implemented, alongside medication prescribed by the primary medical officer. The CHO conducted six brief counseling sessions over two months and weekly follow-ups through tele-assistance. Interventions addressed emotional distress, financial strain, and social reintegration.
After seven months, the patient achieved sustained abstinence, resumed work, and regained stable family relationships. He reported improved self-esteem and coping, and family members observed increased participation in household responsibilities.
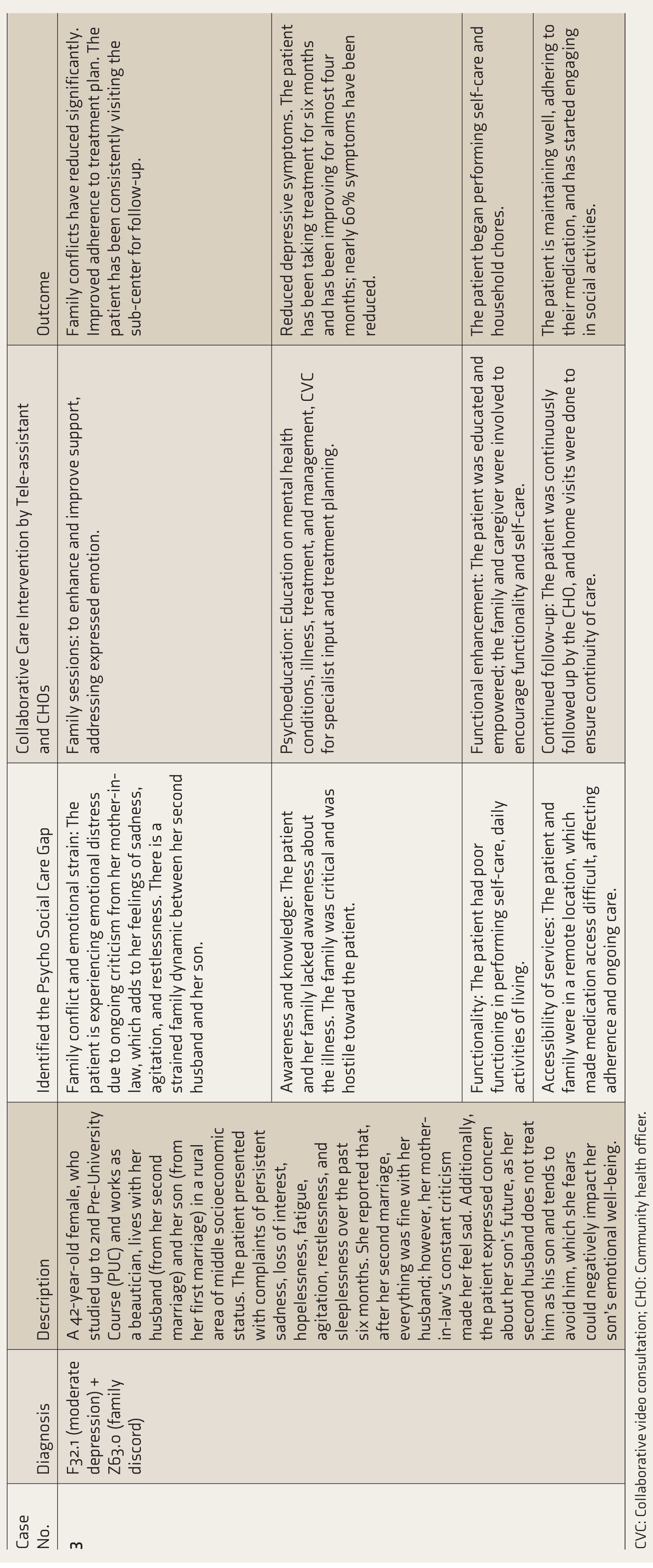
Case 3: Moderate Depressive Episode with Family Discord
Ms. S, a 42-year-old beautician from a semi-rural area, presented with six months of persistent sadness, anhedonia, restlessness, and sleep disturbances. She lived with her second husband and adolescent son from her previous marriage. Family dynamics were strained due to her mother-in-law’s persistent criticism and her husband’s emotional distance from her son, contributing to her psychological distress.
Following CHO screening and a CVC session, she was diagnosed with moderate depression with family discord. Interventions included pharmacotherapy, individual counseling, and family psychoeducation sessions focusing on communication and expressed emotion. The CHO maintained fortnightly follow-ups via home visits and tele-consultations.
After four months, the patient reported approximately a 60% reduction in depressive symptoms, improved self-care, and increased family harmony. By six months, she maintained regular follow-up and resumed work at her salon, reporting greater social engagement and stability.
Across all cases, the collaborative care model integrating telepsychiatric guidance, CHO-led follow-ups, and community-based interventions addressed key psychosocial barriers to care. These cases demonstrate how structured coordination between primary and tertiary care can promote early identification, reduce stigma, enhance treatment adherence, and enable holistic recovery in low-resource settings.
Discussion
This case series highlights how technology-enabled collaborative care can effectively bridge psychosocial care gaps in low-resource contexts by linking community health workers with mental health specialists through tele-assistance and CVCs. Rather than simply demonstrating feasibility, these cases underscore how digitally supported, task-shared interventions can address accessibility, adherence, and stigma, as well as affordability, utilization, and functional outcomes, simultaneously critical dimensions of India’s persistent treatment gap.
A key contribution of this series is to illustrate how trained CHOs, when supported by real-time specialist input, can deliver contextually appropriate psychosocial care. Across conditions as diverse as schizophrenia, alcohol dependence, and depression, telemedicine functioned not merely as a conduit for expert advice but as a mechanism to strengthen continuity of care, mobilize local resources, and enhance family engagement. 11 These interventions demonstrate the holistic integration of clinical, family, and community support, addressing multidimensional psychosocial needs and fostering sustainable recovery. This integration of clinical, social, and community dimensions represents a scalable model for decentralized mental health delivery.
Our findings complement and extend existing evidence on tele-mental health in India. While national programs such as Tele-MANAS (Tele Mental Health assistance and networking across states)and e-Sanjeevani have demonstrated feasibility at scale, 12 the present cases offer micro-level insights into how such platforms can be operationalized within primary care through CHO-led implementation. Comparatively, similar models in other low- and middle-income countries, such as the Friendship Bench initiative in Zimbabwe, 13 Mental Health Gap Action Programme (mhGAP)-based tele-consultations in Nigeria, 14 and the SmartCare e-mental health network in Sri Lanka, 15 have achieved parallel success in integrating community-level task-sharing with digital supervision. Collectively, these examples highlight how culturally responsive digital infrastructure, combined with workforce capacity building and task-shifting, can sustainably extend mental health care to underserved populations.
From a policy perspective, this case series reinforces the importance of embedding digital mentorship and structured supervision into India’s primary mental health system. CHOs represent a pivotal resource for last-mile delivery; their empowerment through telemedicine platforms can operationalize the goals of the National Mental Health Policy, 16 by improving access, continuity, and community engagement. Moreover, integrating psychosocial care into ongoing digital initiatives can ensure that telemedicine serves not just diagnostic or pharmacological needs but the broader psychosocial and rehabilitative spectrum of care. 17 Embedding digital training and ongoing mentorship strengthens the capacity of frontline health workers, enabling them to deliver contextually appropriate interventions and maintain care quality across diverse settings.
This collaborative model emphasized training community health workers to act as the first line of contact for mental health cases, providing continuous support from specialists (Figure 1). The approach also highlights the scalability and sustainability of telemedicine-supported, community-based care, offering a replicable blueprint for other low-resource regions. In summary, beyond reaffirming the utility of telemedicine, these cases provide evidence that digitally networked, community-based mental health care can simultaneously bridge structural and psychosocial barriers. The lessons from this series support a multi-dimensional, technology-enabled, and scalable collaborative model that aligns with both national priorities and global strategies for equitable mental health service delivery.
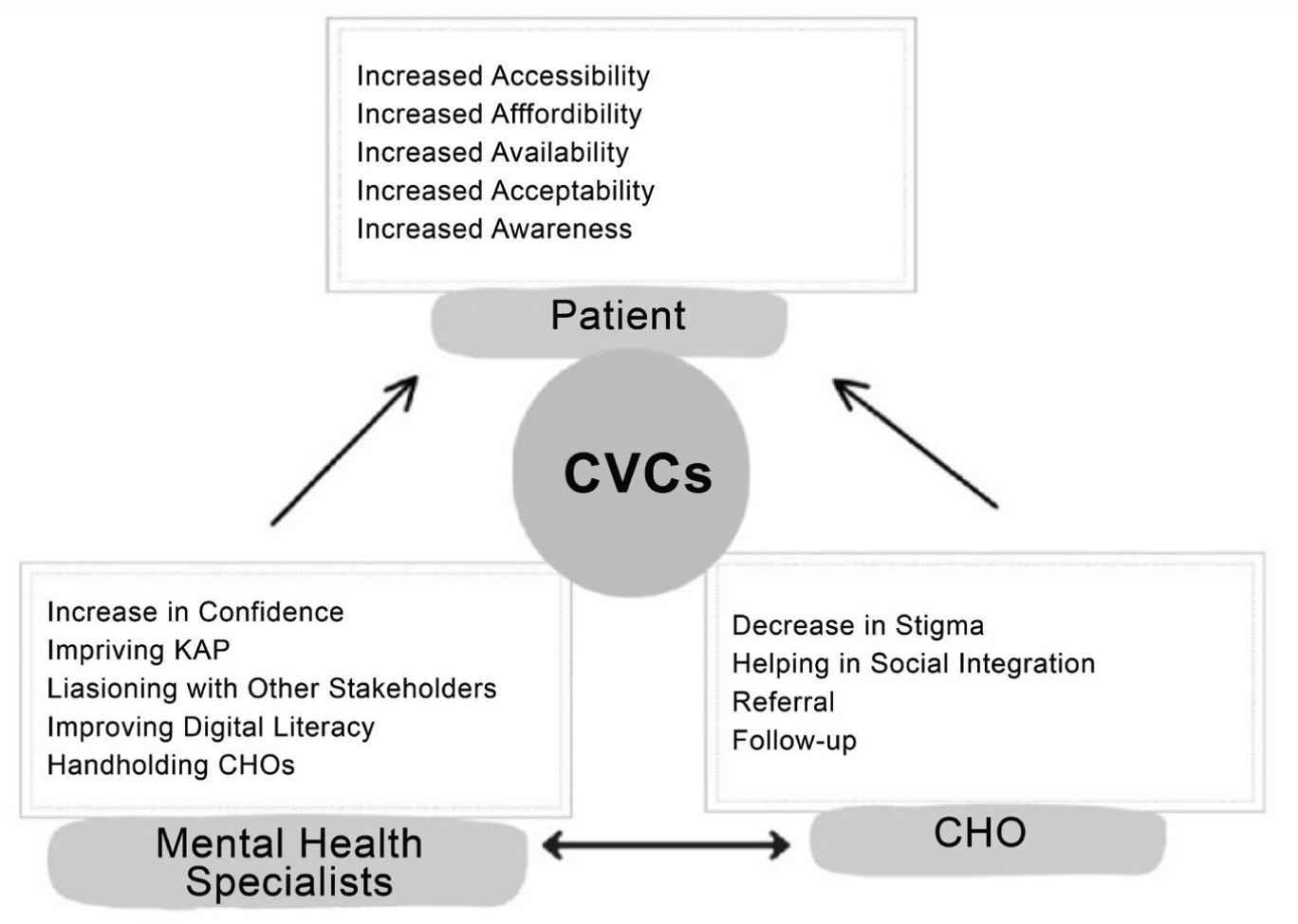
CBC: Collaborative video consultations, CHS: Community health officer.
Limitations and Future Directions
While the results are promising, several limitations must be acknowledged. The study was confined to a specific geographical region (Karnataka) and may not fully represent the broader diversity of mental health challenges across India. While the case series shows promising results, broader studies are needed to generalize the findings. Additionally, challenges such as digital literacy and internet access, particularly in rural and low-income areas, may limit the widespread applicability of these interventions. 18
Future research should explore scaling these interventions across regions, assess long-term outcomes, and evaluate integration into national health systems. Studying cost-effectiveness could also reveal their potential as a sustainable solution to the psychosocial care gap.
Conclusion
This case series illustrates that leveraging technology, particularly telemedicine and CVC, can significantly bridge the psycho social care gap in mental health, particularly in underserved and rural areas. By improving accessibility, reducing financial burdens, and fostering community involvement, these interventions provide a comprehensive, scalable model for mental health care. As mental health challenges continue to rise globally, especially post-pandemic, integrating technology into mental health care delivery will be crucial for ensuring equitable access to quality psycho social support.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
Same as the “Introduction ” article of this issue (Indian J Psychol Med. 2026;48(1 suppl)).
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Author Channaveerachari Naveen Kumar is the Principal Investigator of this project and supplemental issue. The author did not take part in the peer review or decision-making process for this submission and has no further conflicts to declare.
Declaration Regarding the Use of Generative AI
The authors used ChatGPT to paraphrase and formalize the text. After using this tool/service, the authors reviewed the translated and transcribed content and edited it as needed, and took full responsibility for the content of the publication.
During the preparation of this work, the authors used ChatGPT to paraphrase and formalize the text. After using this tool/service, the authors reviewed the translated and transcribed content and edited it as needed, and took full responsibility for the content of the publication.
Ethical Approval
The study was approved by the IEC (Approval No. NIMHANS/ 43rd IEC [BEH.SC.DIV] 2023, dated December 8, 2023) and registered with the Clinical Trial Registry of India (Registration No. CTRI/2024/02/062906).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study’s data were derived from a project, “A Pan India Digitally Driven Capacity Building Program to strengthen Primary Mental Healthcare,” funded by the CSR initiative of a multinational company.
Informed Consent
Informed consent was sought from all participants, including the primary healthcare workers and patients.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.