
Abstract
Background:
Parental interventions are efficacious and robust in managing children’s behavioral problems. Yet, research addressing their role in parental stress and anxiety is sparse. Our first aim was to assess the extent of anxiety and stress among parents of children with autism spectrum disorder (ASD) and attention deficit hyperactivity disorder (ADHD). The second was to assess the effectiveness of a parent-to-parent support group for addressing the stress and anxiety among those parents.
Methods:
We selected a single group pretest posttest design. We recruited 24 parents from the two in-patient facilities of child and adolescent psychiatry. The intervention consisted of a parent-to-parent support group. We assessed parental stress and anxiety before and after the intervention.
Results:
The differences in anxiety and stress scores prior to and after the intervention were statistically significant (P < 0.001). Before the intervention, low level of parents’ education and lower family income had a statistically significant relationship with higher parental stress. Also, parents who were employed had lesser anxiety.
Conclusion:
The parent-to-parent support group effectively reduced stress and anxiety among parents of children with ASD and ADHD. These are preliminary findings. The lack of a control group is a major limitation.
Keywords
Parents of children with autism sectrum disorder (ASD) and attention deficit hyperactivity disorder (ADHD) face stress and anxiety. Parent-to-parent support group effectively reduced stress and anxiety in them. Nurses may play a significant role in reducing stress and anxiety among parents through a nurse-led parent-to-parent support group.Key Message:
According to the National mental health survey, 1.6% of children in India have autism spectrum disorder (ASD). 1 Recent studies on attention deficit hyperactivity disorder (ADHD) have shown the weighted prevalence of this disorder to be 8.8% in India. 2
Parenting stress arises when parents’ perception of parenting roles and responsibilities becomes overwhelming and surpasses their ability to cope with adverse circumstances. McCubbin and Figley (1983) stipulated that mental illness can be a catastrophic stressor for the family. Anxiety, on the other hand, is a feeling of uneasiness regarding unpredictable future events. 3 Green and Solnit (1964) revealed that parental anxiety about the child’s health could lead to maladaptive parent–child interactions. 4 Aspects of a child’s behavior related to ASD and ADHD have been found to cause stress and anxiety among parents. 5 Parents of children with these disorders have marital discords, financial constraints ascribable to treatment expenses, low self-esteem, and poor life satisfaction.6–8 Parents of a child with ASD have more stress and anxiety than parents of a typically normal child.9, 10 Parents’ response to accommodate the diagnosis of ASD varies according to the severity of symptoms in the child. Apart from the diagnosis, researchers have tried to study other factors responsible for high parental distress among parents of children with ASD. Parents of children with ASD blame themselves for their child’s illness, have significant negative parental self-view, and exhibit insufficient self-efficacy as a parent. 11 Additionally, inadequate social support is one major element described by these parents that causes parental stress and anxiety. 12
In the present study, a parent-to- parent support group (PPSG) was conceptualized and constructed using Roy’s adaptation model. 13 PPSG is a therapeutic group that aims to provide mutual support among parents, facilitate therapeutic communication, provide education about the illness by a mental health nurse, and inculcate coping strategies to deal with the stress and anxiety related to a child’s illness and brief stress management techniques. Parents who indulge in such groups have reported having better health status and family functioning.14–16 Despite the high frequency of parent peer support use among parents of children with ASD and ADHD, literature in this area is sparse.
The objectives of the study were to assess the level of anxiety and stress among parents of children with ASD and ADHD, plan and execute a nurse-led parent-to-parent support group, compare pretest and posttest levels of anxiety and stress, and find the association between severity of illness and parental stress and anxiety.
Methods
Sample
Parents of children diagnosed with ASD or ADHD admitted to the two in-patient facilities dedicated to children and adolescents at our center were invited to participate in the study. The study used a quasi-experimental, single-group prepost design. A pilot study was conducted with five parents (three of children with ADHD and two with ASD) who met the inclusion and exclusion criteria and were willing to participate. From the pilot study, the effect size was found to be 0.7, and the sample size for the main study was computed at a 5% level of significance and 90% power. Based on this, the minimum number of subjects required for the study was 24.
We used convenience sampling to recruit the parents. Twenty-four parents who met the inclusion and exclusion criteria participated. Fourteen were parents of children with ADHD and 10 with ASD. Inclusion criteria were: mother or father of children aged 4 to17 years diagnosed with ASD or ADHD admitted in child and adolescent psychiatric wards of National Institute of Mental Health and Neuro Sciences (NIMHANS), who can speak Hindi or English. Parents of children who had both ASD and ADHD and caregivers other than parents were excluded.
Procedures
Parent-to-Parent Support Group (PPSG)
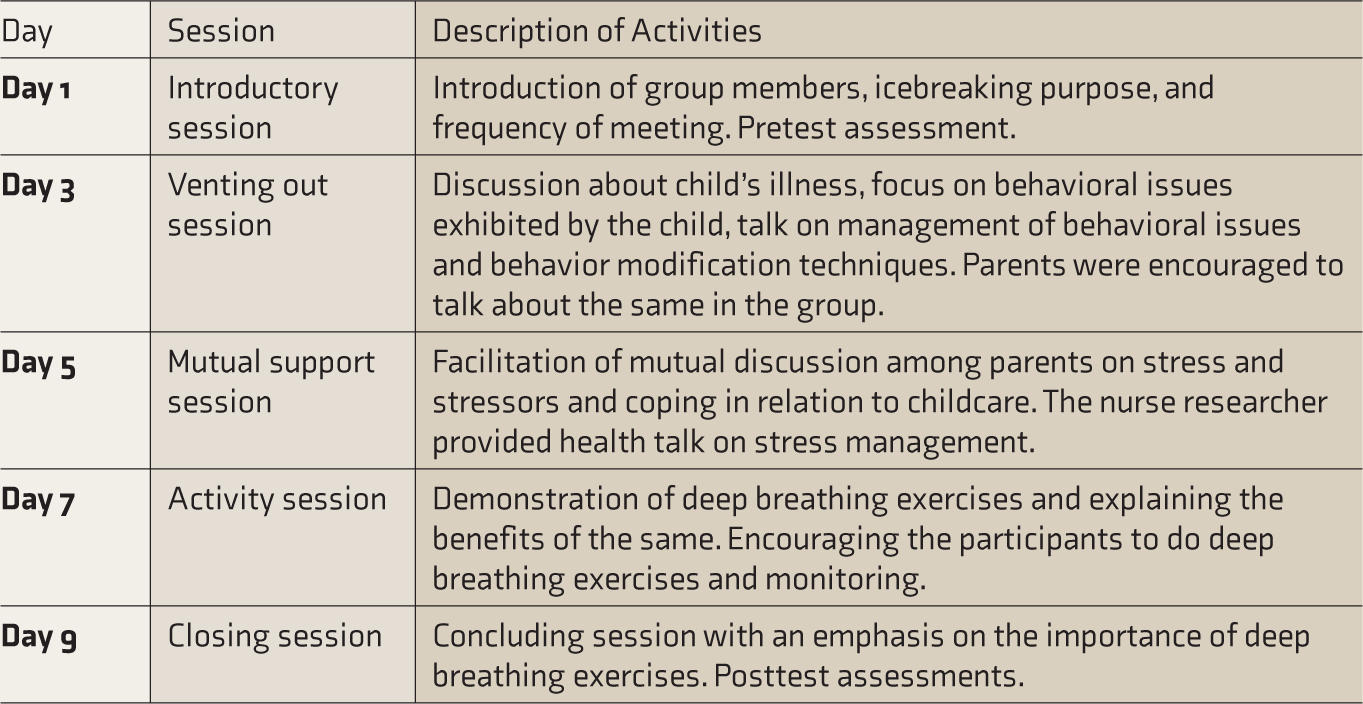
Participants were enrolled for five sessions; each session was conducted on an alternate day for one h. Therefore, the total time taken to conduct PPSG was nine days, including pretest and posttest assessments. The 24 participants were allocated into small groups of four to five members based on the diagnosis. Sessions were conducted and monitored by a mental health nurse. Assessment of sociodemographic profile and pretest assessment of stress and anxiety were done on the first session. A closing session focused on group termination and posttest of stress and anxiety. The intervention is described in Table 1. Data collection was done from September 2019 to October 2019.
Brief Description of Parent-to-Parent Support Group Interaction Session
Measures
Semistructured Proforma
It had two parts: sociodemographic data of parents and child’s clinical profile. Data related to the parent, gender, education, occupation, marital status, and annual family income were collected. The child’s clinical profile consisted of five items that included age, diagnosis, months of present illness, and the number of past hospitalizations.
Beck’s Anxiety Inventory (BAI)
It is a self-report instrument to measure anxiety. It consists of 21 anxiety symptoms, with respondents being asked to indicate the extent to which they were bothered by each item “during the past week, including today.” Responses are rated on a four-point Likert scale from 0 (not at all) to 3 (severely). The translated Hindi version of BAI was used in the study. Cronbach’s α for the translated Hindi version of BAI is 0.862. 26
Cohen’s Perceived Stress Scale (PSS)
The perceived stress scale (PSS) is a self-report instrument to quantify perceived stress. It assesses the degree to which one’s situations are perceived to be stressful. PSS-10 contains 10 items, and each item is rated on a 5-point Likert scale from 0 (never) to 4 (very often). Six out of the ten items have a positive stress factor; therefore, the remaining four items are scored reversely. 17 The translated scale has an acceptable level of internal consistency (Cronbach’s α = 0.731). 27 Hindi translated versions of both BAI and PSS are free-to-use tools, and we adopted them as is.
Data Analysis
We analyzed the effectiveness of the intervention with the Wilcoxon signed-rank test, using 0.05 as the level of significance. An exploratory analysis (Mann–Whitney test) was carried out to find the relationship between selected sociodemographic variables and preintervention stress and anxiety. Separate analyses for ASD and ADHD were also conducted as a secondary objective. The statistical analysis was performed using the statistical package for social sciences (SPSS) version 22. 18
Results
As the attrition rate was nil, the data collected from the total (24) sample were analyzed. Mean (SD) age of the participants was 39 (7.17) years (Table 2). The majority of the participants were females. 62.5% of the participants were graduates and above, while 8.3% had only primary education. Majority were married, employed, and lived in a nuclear family. Most (70.8%) had family income above INR 20,000 per month.
Key Sociodemographic and Clinical Variables (N = 24)
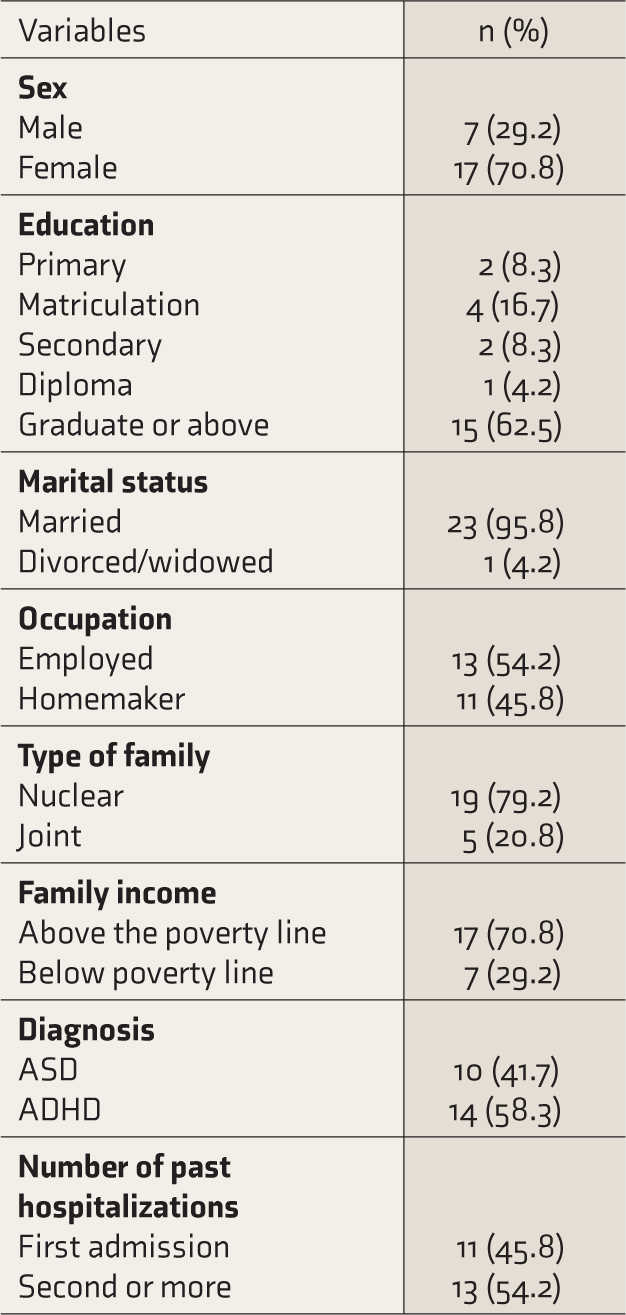
Mean age of the children was 12.5 (7.07) years. The duration of illness in most of the children was approximately 4 years. Most children had got admitted to the hospital more than once in the past. Fourteen children had ADHD, out of which three had co-morbid diagnoses of both Asperger’s syndrome and anxiety disorder. Ten had ASD; among them, two had oppositional defiant disorder and anxiety disorder, respectively. Table 3 shows the findings of stress and anxiety among parents based on the diagnosis of the child.
The median of the pretest scores and posttest levels of stress and anxiety for the combined group of parents are presented in Table 4. This shows a significant difference at a 0.05 level of significance for both stress and anxiety.
Stress and Anxiety Among Parents Based on the Diagnosis of the Child

ASD, autism spctrum disorder; ADHD, attention deficit hyperactivity disorder.
Pretest and Posttest Scores of Anxiety and Stress Among Parents of Children With ASD and ADHD

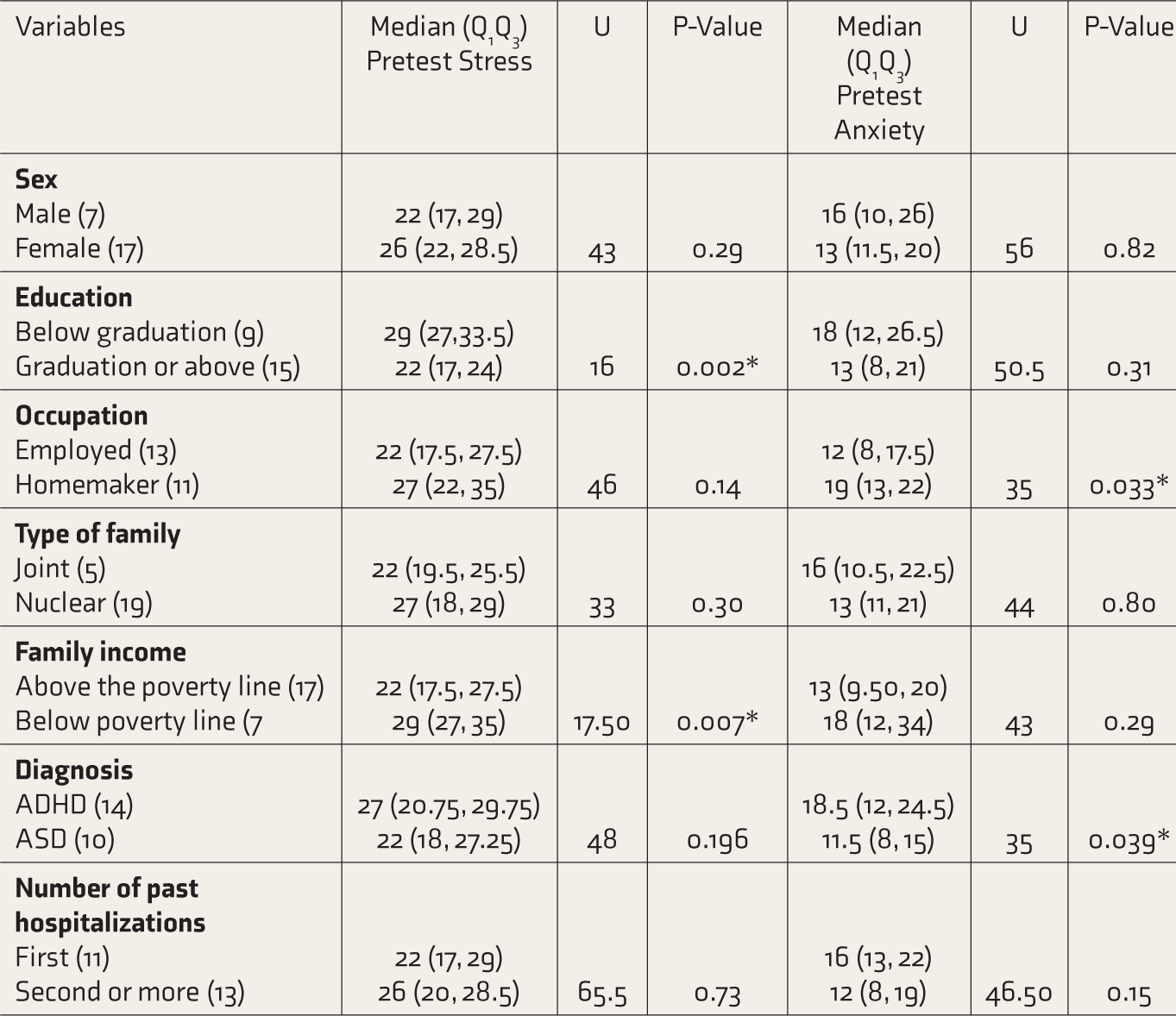
We also explored the relationship between selected sociodemographic variables and pretest anxiety and/or stress level among the parents (Table 5). Parents with low level of education or lower family income had a statistically significant higher stress before the intervention. Parents who are employed had less anxiety. Parents of children diagnosed with ASD had lesser anxiety compared to parents of children diagnosed with ADHD.
Relationship of Selected Sociodemographic Variables With Stress and Anxiety
Discussion
Stress and anxiety of the parents were high, as previously observed.19–21 This may suggest that raising a child with ASD or ADHD increases the risk for high stress and anxiety among the parents, but it is difficult to make such a conclusion as this was a cross-sectional study.
The PPSG was designed keeping in mind the key principles of psychoeducation, problem-solving, and social support provision. Results depict a statistically significant difference in stress and anxiety scores before and after the intervention. This suggests that PPSG can be utilized to address stress and anxiety among parents of children with ASD or ADHD. Our results are consistent with the findings of the randomized controlled trial (RCT) by Feinberg et al., in which they found positive effects of problem-solving education in reducing parenting stress and depressive symptoms during the critical postdiagnosis period. 22 RCT by Tonge et al. (2006) also showed the effectiveness on parental mental health of an education and skills training program for parents of 120 children with autism (2½–5 years old). Treatment sessions included education about autism; features of communication, social, play, and behavioral impairments, and principles of managing behavior and change. Mental health significantly improved over time in 54% of principal caregivers who had the highest levels of mental health problems. Prepost comparison and intervention, control group comparison both were significant. 15 Binbin Ji et al. 16 showed the efficacy of multidisciplinary parent education (MPE) for caregivers of children with ASD. The MPE program involved eight sessions of approximately 90 min each. The team included a special education teacher, a community nurse, a psychologist, and a psychiatrist. Results demonstrated better self-efficacy among parents following the intervention. The mean scores of positive coping styles significantly increased in the intervention group. 16
Majority of our participants were mothers. It is interesting to note that majority of the caregivers are mothers in the present study. A case-control study by Farsi et al. investigated stress, depression, and anxiety among parents of children with ASD. Results showed higher stress and depression among mothers than fathers. 21 However, no significant association was found between gender and stress or anxiety before the intervention in this study. Lianne van et al. assessed predictors of discrepancies between mothers and fathers of children with or without ADHD. Results revealed significantly more stress and depressive symptoms among the mothers. 23 The current study did not compare stress and anxiety among children with ADHD, because of an insufficient sample to draw any significant conclusion.
The majority of our participants were graduates and above. We also found higher level of stress among parents with lesser educational qualification. These findings are consistent with the previous studies. Sethi et al. investigated stress and related factors among parents of children with ADHD. Fifty mothers of children with ADHD and 50 mothers of healthy children constituted the sample. They found that higher education of the father is associated with less stress. Moreover, parents of children with ADHD had more anxiety than the parents of children with ASD. 24
Athari et al. found a significant relationship between maternal stress and family income among mothers of children with autism. 25 The results were analogous to the present study.
Limitations
The lack of a control group is the major limitation. The design used was quasi-experimental. Therefore, the effect of possible extraneous variables could not be controlled, such as possible reduction in anxiety and stress because of the treatment given to the children. The decline in the level of stress and anxiety could have been because of other ongoing activities in the treatment/in-patient facilities. RCTs with a larger sample can be conducted. Qualitative data can also be obtained to design interventions for the parents.
Conclusion
Our preliminary findings suggest that the PPSG effectively reduced stress and anxiety among parents of children with ASD and ADHD.
Footnotes
Acknowledgements
The authors express sincere gratitude to the biostatistics department for the data analysis.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.