
Abstract
Background:
Mental health disorders are a common cause of disability worldwide. Disparities exist between the mental health frameworks of high-income countries (HICs), upper middle-income countries (UMICs), and low- and middle-income countries (LMICs). LMICs have shortages in infrastructure, financial resources, laws, and workforce, resulting in significant gaps in treatment. This study compares mental health system indicators across 10 nations to examine how economic and policy-level factors influence service access and population-level burden.
Methods:
A cross-sectional comparative analysis was conducted using publicly available secondary data. Sources included the WHO Mental Health Atlas, World Bank Open Data, Global Burden of Disease (GBD), and national mental health policies. Five HICs (United States, United Kingdom, Germany, Australia, Japan) and five UMICs plus LMICs (Brazil, South Africa, India, Kenya, Nigeria) were selected. Mental health budget allocation, treatment gap, psychiatrist density, psychiatric bed availability, primary care integration, and disability-adjusted life years (DALYs) were assessed. Descriptive statistics and Pearson correlations were applied.
Results:
HICs allocated 6.1%–11.3% of health budgets to mental health, had lower treatment gaps (19%–32%) and higher psychiatrist densities (11.8–14.6/100,000). On the contrary, LMICs had a budget share below 1%, treatment gaps >75%, and psychiatrist densities <1. A strong positive correlation was observed between GDP per capita and the prevalence of psychiatrists (r = 0.77, p < .001), and a strong negative correlation was observed between the gap in treatment and the share of the budget (r = -0.82, p < .001).
Conclusions:
Economic capacity and political commitment have a substantial impact on mental health systems. Strengthening the workforce, integrating services, and reforming legislation are essential to closing the gaps in treatment and achieving equity.
High-income countries invest significantly more in mental health systems, resulting in better workforce capacity and lower treatment gaps compared to low- and middle-income countries. Economic resources and political commitment are strongly correlated with improved access to mental health care and a reduction in disparities. Strengthening the workforce, financing, and service integration is essential for closing treatment gaps and achieving equity in global mental health.Key Messages
Mental health disorders are a substantial and growing component of the Global Burden of Disease (GBD). As per GBD-2021, mental and behavioral disorders (including substance use disorder) account for approximately 7%–8% of all disability-adjusted life years (DALYs) and about one-fifth of years lived with disability (YLDs) worldwide. 1 This significant disease burden contrasts with the historically limited attention and resources devoted to mental health in many countries. The WHO’s Mental Health Action Plan 2013–2030 and the inclusion of mental health targets in the Sustainable Development Goals (SDGs) are examples. 2 Yet, implementation of comprehensive strategies for mental health systems is uneven.
High-income countries (HICs) have made significant advancements in the development of integrated and rights-based mental health systems. These systems have robust legislation, better funding, and more specialists. 3 In contrast, many low- and middle-income countries (LMICs) struggle with outdated or fragmented policies, chronic workforce shortages, underfunding, and weak infrastructure.4,5
One of the most important indicators of this disparity is the availability of trained mental health professionals per population. According to the WHO Mental Health Atlas 2020, in contrast to more than 10 psychiatrists per 100,000 population in HICs, most LMICs have even fewer than one psychiatrist per 100,000. 6 The shortage of psychiatric nurses, psychologists, and social workers also affects service delivery.7–9 Low financial support in many LMICs is another critical gap. HICs allocate more than 5% of the health budget to mental health, LMICs <1%. This often leads to higher out-of-pocket payments for mental health in poorer countries. 10 The HICs generally have strong mental health legislation, often in line with the United Nations Convention on the Rights of Persons with Disabilities (UNCRPD) and well-integrated services. The LMICs either do not have or have recently adopted legislation on mental health, but it is not implemented well.11,12 The Indian Mental Health Act of 2017 is a progressive example of initiative by the LMICs. However, implementation is uneven due to funding issues and training deficiencies.13,14 In many LMICs, mental health services are not appropriately integrated into primary health care (PHC), which leads to accessibility problems and a lack of continuity of care. 15
COVID-19 revealed system deficiencies in the LMICs, where increased needs were outstripping the availability of infrastructure. 16 These options are less available in low-resource countries. Untreated mental health disorders impair productivity, and due to less state support, high out-of-pocket costs reinforce cycles of poverty for many families. 17
Few studies have compared mental health systems across income groups using standardized metrics. Comparative research to concurrently examine workforce, policy, financing, service integration, and health outcomes is urgently needed to inform global health policy and resource prioritization. By identifying gaps and drawing empirical links between economic indicators and the system’s performance, stakeholders can develop targeted strategies to address mental health inequalities. In this study, we conducted a cross-sectional comparative analysis of mental health systems in 10 countries representing a wide range of income brackets. The objective is to guide reforms and make mental health a central component of universal health coverage.
Methods
Study Design
This study used secondary data from high-quality, publicly available global datasets in a cross-sectional, comparative research design. We evaluated system metrics across 10 nations of varied income levels. We focused on evaluating population-level impacts and the connection between the capacity of national mental health systems and structural and economic indicators. Data extraction and cross-verification across different sources, as well as final compilation, were completed between December 2024 and March 2025.
Ethical Considerations
This study utilized only publicly available, de-identified, and aggregated secondary data and, therefore, did not involve any direct interaction with human subjects. As such, it was exempt from institutional ethics review under the Declaration of Helsinki (paragraph 23), and no informed consent was required. 18 The study followed the STROBE (Strengthening the Reporting of Observational Epidemiological Studies) guidelines for cross-sectional studies. 19 The completed STROBE checklist is provided as a supplementary file E with this article. We have introduced three safeguards: (a) cross-checking all data with government reports, prioritizing official statistics; (b) the contextualization of the LMIC findings to avoid stigmatization; and (c) the full documentation in the A-D supplementary files for transparency. The study also adheres to Committee on Publication Ethics (COPE) guidelines and WHO reporting standards. An institutional waiver letter was also obtained, exempting the requirement for consent or ethics permission.
Country Selection
We included 10 countries, five HICs (Germany, the United Kingdom (UK), the United States (US), Australia, and Japan), and two upper middle-income countries (UMICs, Brazil and South Africa), plus three LMICs (India, Kenya, and Nigeria). The countries were selected using a purposive sampling method based on five systematic criteria. This sampling technique was chosen over random sampling because it was more suitable for ensuring representation across various income levels, which is crucial for our comparative analysis. The following selection criteria were used to ensure meaningful comparison across economic strata: (a) representation of distinct World Bank income categories (HICs vs. LMICs/UMICs) 20 ; (b) geographical diversity across continents to enhance global applicability; (c) the availability of recent (with most metrics reported for 2019 or the latest available year) national-level data for significant mental health indicators; (d) the presence of a national mental health policy or legislation, and; and (e) population exceeding 20 million to ensure sufficient healthcare system scale for analysis. Countries with incomplete data or active conflict were excluded.
The purposive sampling technique was theoretically supported as it aligned closely with our research hypothesis concerning economic inequalities in mental health systems. A random sample would not be able to deliver the income-based stratification required for our comparative analysis. We deliberately selected 10 countries to ensure balanced representation across different income levels and geographical areas within our resource limitations, even though many other countries also met our inclusion criteria. This method placed more emphasis on analytical nuance and thoughtful comparison than on thorough coverage.21,22 Although this method restricts generalizability to all nations within each income bracket, the fact that our chosen nations comprise a variety of geographic areas and account for roughly 45% of the world’s population supports our findings for the development of global mental health policies.
Data Sources and Rationale
We used four widely cited international data sources:
The WHO Mental Health Atlas 2020 provides the most recent globally harmonized system-level standardized data on infrastructure, service integration, workforce density, and mental health policies. The globally harmonized system-level indicators are the standardized metrics that cover policy and legislation, leadership and governance, financing, human resources, service availability and coverage, integration, and promotion. The GBD Study: GBD 2021 provided DALY estimates for mental and substance use disorders to ensure consistency across most indicators. World Bank Open Data (2020–2022): Offered health system and economic indicators such as health expenditure per capita, health budget as a percentage of GDP, and out-of-pocket spending (OOP). National Policy Portals and WHO MindBank: Provided legislative documentation and information about the status and implementation of national mental health laws and policies.
The study also used secondary data from international databases that define and classify mental and behavioral disorders based on standardized diagnostic frameworks, such as the ICD-10, ICD-11, and DSM-5. These diagnostic classifications were used by the original data collection organizations, not by the authors of this study. When 2021 data for a particular indicator, such as DALYs, were unavailable for the study country, we used the following most recent data available.
Indicator Framework and Rationale
We analyzed 12 core indicators across six domains assessing system capacity and burden:
Policy and Legislation (To track the legal commitments and enforcement capacity of each country): The presence of a national law or policy regarding mental health; coherence with the UNCRPD; and the categorization of implementation status. Mental Health Workforce (Proven correlate of service capacity and access): The number of psychiatrists for every 100,000 individuals in the population. Secondary indicators included the availability of psychologists, psychiatric nurses, and social workers, where available. Infrastructure (Provides information on in-patient care availability): Number of psychiatric beds per 100,000 population, as a proxy for in-patient capacity. Financial Investment (Indicates the importance placed on mental health and responsibility in distributing resources): The proportion of government spending on mental health relative to the overall health budget, along with OOP expenses as a percentage of total expenditures. Service Integration (Crucial for guaranteeing accessibility from the initial interaction and ongoing care): The extent to which mental health services were incorporated into PHC (classified as fully, partially, or not integrated) and the presence of community-based service delivery initiatives. Burden of Disease (Measures the true and demographically adjusted impact of psychiatric disorders on population health): Mental health outcomes were measured using both age-standardized and raw DALYs per 100,000 people. International comparisons of relative burden are facilitated by age-standardized DALYs, which account for variations in age distribution. Raw DALY rates, on the other hand, offer a more accurate assessment of the total burden of mental and substance use disorders within the actual demographic profile of each nation. Using both measures enabled us to assess system strain and compare cross-national equity. Where available, suicide mortality rates were also extracted and included as complementary indicators of untreated mental illness.
We also collected contextual information, such as anti-stigma programs, national surveys, and rights-monitoring mechanisms, primarily to supplement the interpretation, although these were not included in the formal scoring.
Data Collection and Quality Assurance
Indicators were standardized per 100,000 population or percentage of national totals. To maintain quality, all extracted data were independently cross-verified by two reviewers. Discrepancies were resolved by checking source documents (e.g., Ministry of Health reports, WHO databases). Missing data were flagged, and in limited cases, imputation was performed using income group averages (e.g., for LMICs in sub-Saharan Africa).
Supplementary Files A, B, C, and D include data profiles and outputs for transparency and reproducibility.
Statistical Analysis
We used descriptive statistics to compile key metrics of mental health systems in various nations according to income brackets. During this process, means, medians, and ranges were computed for continuous variables, including the percentage of treatment gaps, the number of psychiatric beds per capita, the density of psychiatrists, and the allocation of funds for mental health.
Before conducting Pearson correlation analyses, the distribution of each continuous variable (e.g., psychiatrist density, psychiatric beds per 100,000, budget share, raw and age-standardized DALYs) was assessed for normality. We performed the Shapiro–Wilk test for each indicator (α = 0.05). All variables met the assumption of normality (Shapiro–Wilk p > .10), supporting the use of Pearson correlation. Pearson correlations assessed links between economic and system indicators: GDP per capita compared to psychiatrist density, the share of the mental health budget against the treatment gap, and the integration of PHC (rated as binary) with both the treatment gap and OOP expenses. The following five criteria were used to select the variables for Pearson correlation: (a) theoretical relevance linking system inputs (e.g., GDP per capita) to outputs (e.g., psychiatrist density); (b) inclusion in our 12-indicator framework with 80% country coverage (2010–2022); (c) sufficient cross-country variance to support analysis with n = 10; (d) fulfillment of normality assumptions (Shapiro–Wilk p > .10); and (e) direct policy actionability, linking economic and structural levers to access and burden outcomes. All statistical analyses were performed using IBM SPSS statistics version 26.0 23 and Microsoft Excel 2019, with a significance threshold of 0.05.
Results
This study analyzed mental health system indicators across 10 countries—five HICs and five UMICs plus LMICs—to examine disparities in workforce, infrastructure, financing, legislation, implementation, integration, and treatment gaps.
Mental Health Workforce and Infrastructure
Infrastructure capacity reflected the imbalance between HICs and LMICs. HICs had an average of more than 10 psychiatrists per 100,000 population, with the US having 14.60 and Australia at 13.50. Nigeria and Kenya had only 0.1 and 0.2 psychiatrists per 100,000 (Table 1 and Figure 1), highlighting a severe shortage. Apart from the fact that fewer professionals are trained in LMICs, the problem is exacerbated by the tendency of trained professionals to leave the country frequently.24,25 Many countries lack psychiatric training and incentives to move to rural areas. 26
Country-wise Key Mental Health System Indicators.
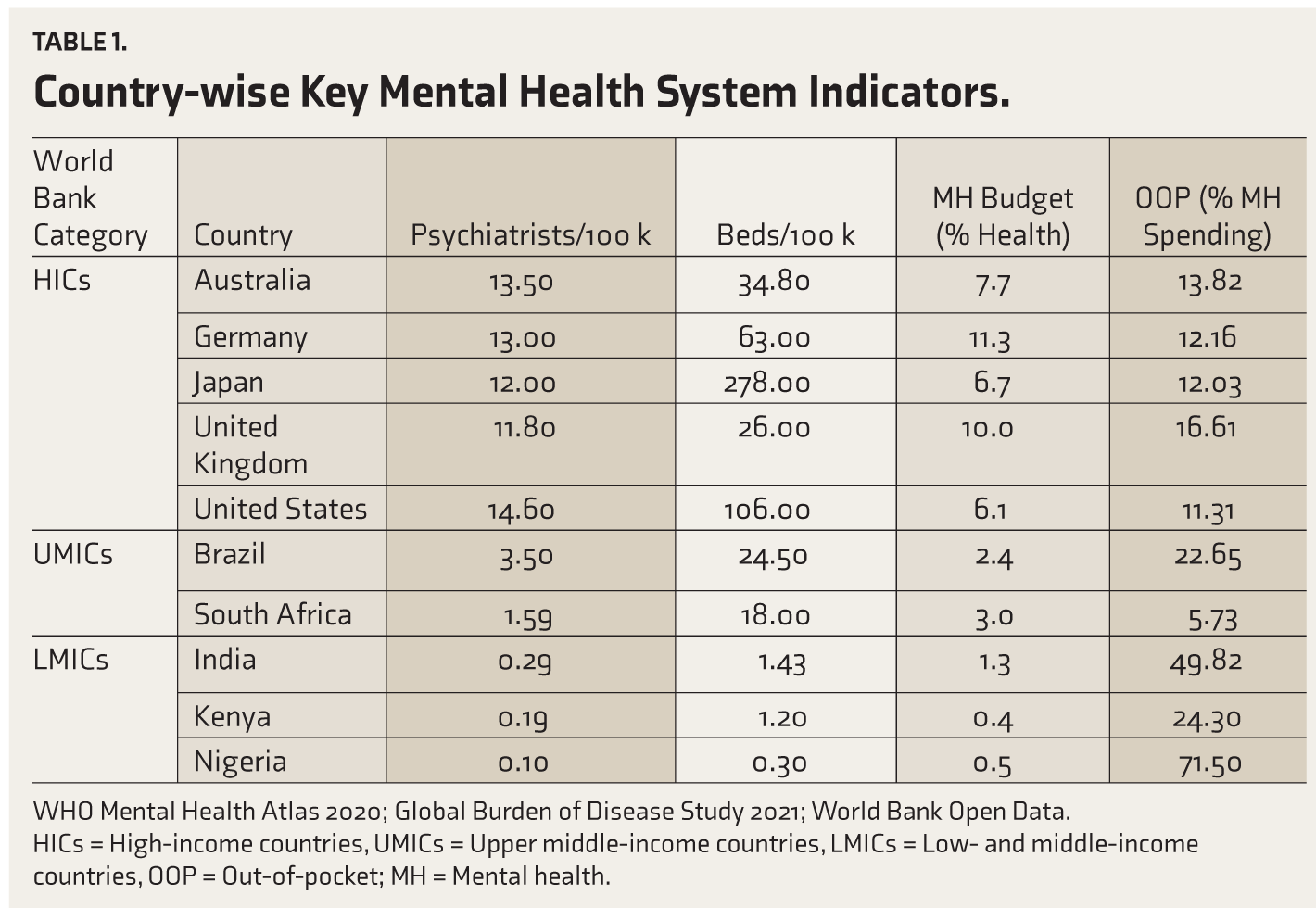
WHO Mental Health Atlas 2020; Global Burden of Disease Study 2021; World Bank Open Data.
HICs = High-income countries, UMICs = Upper middle-income countries, LMICs = Low- and middle-income countries, OOP = Out-of-pocket; MH = Mental health.
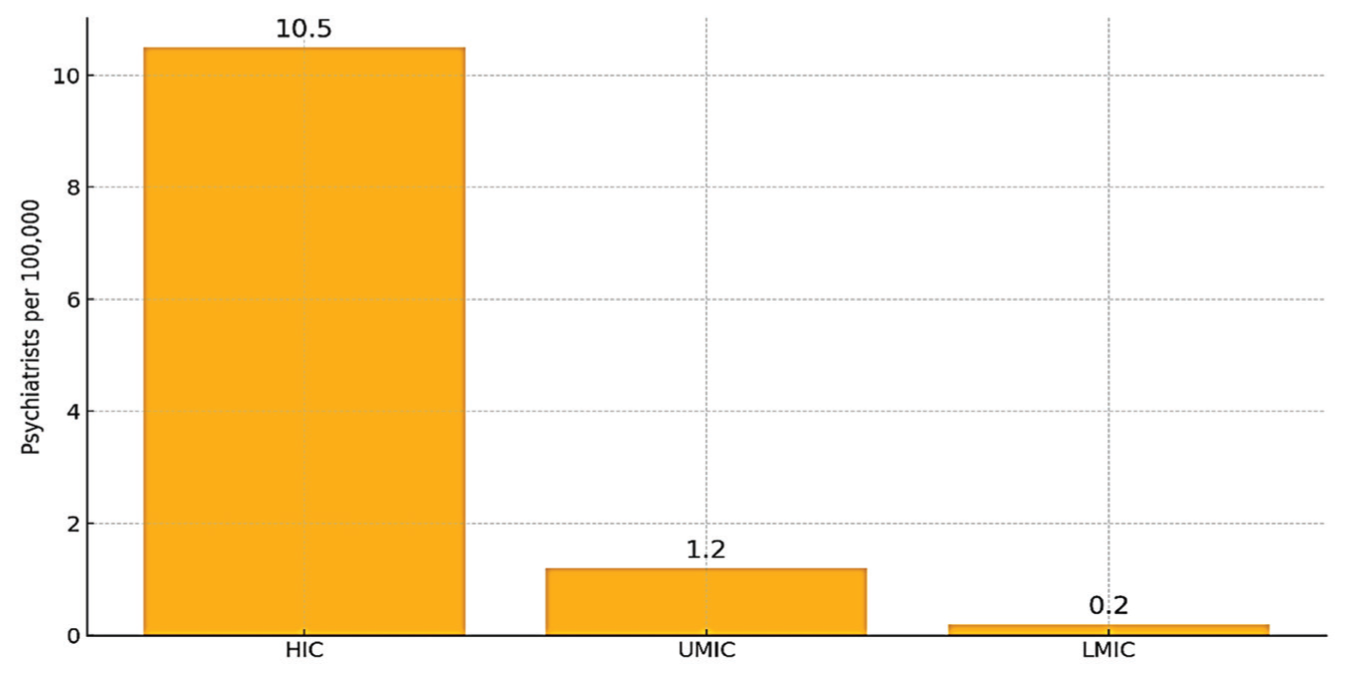
Comparing psychiatrists per 100,000 population across HICs, UMICs and LMICs. Income groups classified using World Bank criteria. Data from the WHO Mental Health Atlas 2020.
In addition, HICs had, on average, more than 30 psychiatric beds per 100,000 inhabitants, offering both short-term and long-term in-patient treatment. Japan reported a rate of more than 278 beds per 100,000 people, which reflects a well-established institutional strategy. However, in Kenya and Nigeria, the number of psychiatric beds was less than five per 100,000, and these were mostly in urban hospitals, which made access difficult for rural populations. LMICs lack community care and rehabilitation infrastructure. Facilities for psychosocial rehabilitation, day hospitals, and community care centers were among the essential infrastructures lacking in LMICs.
Financing and OOP Spending
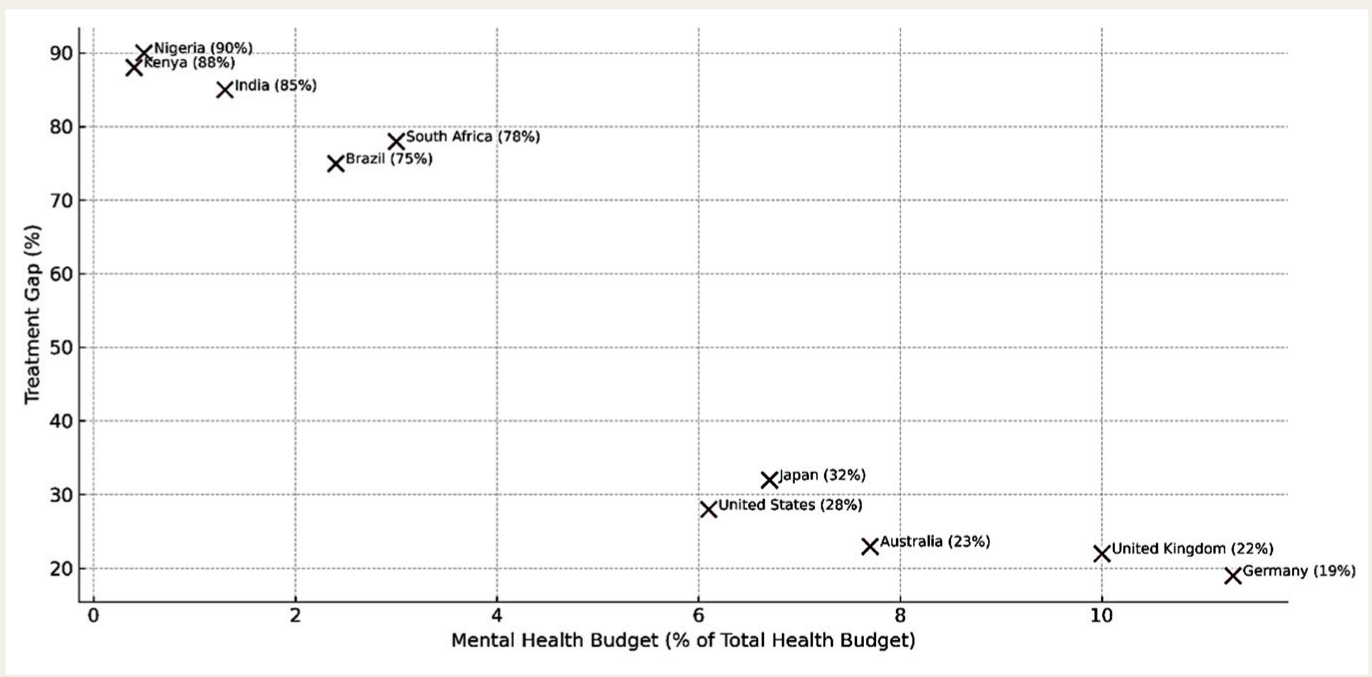
Public financing of mental health services showed consistent disparities between income groups. The percentage of total health budgets that HICs allotted to mental health services ranged from 6% to 11.5%. This percentage was drastically lower in LMICs, with Nigeria and Kenya allocating less than 0.5% of their health budgets to mental health, and India allocating just 1.3% (Table 1 and Figure 2). Furthermore, the lack of dedicated budgets weakens accountability in LMICs. The OOP costs in these LMICs are disproportionately high. In Nigeria, more than 71% of mental health costs were borne directly by individuals.
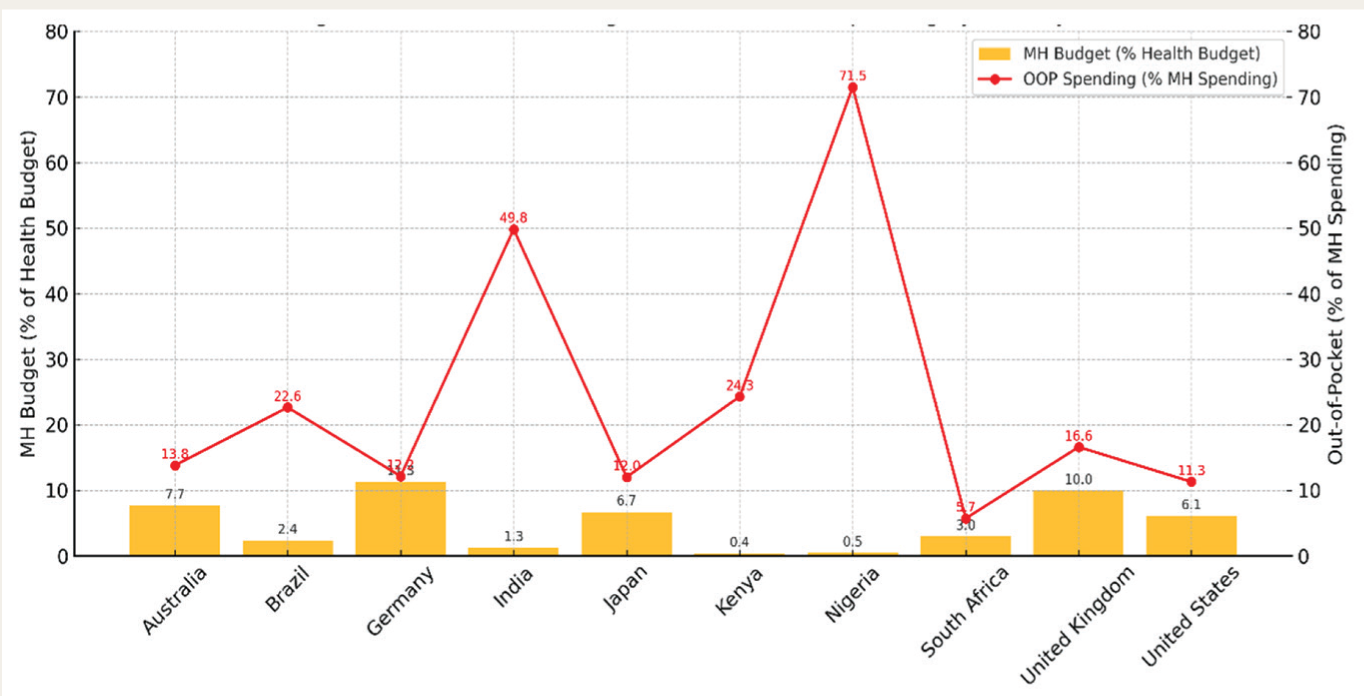
Percentage of health budget allocated to mental health and out-of-pocket spending on mental health services by country. All values reflect 2021 data unless otherwise noted. OOP and expenditure indicators sourced from the World Bank and WHO datasets.
In contrast, Germany and the UK cover mental health via public insurance. High OOP costs limit care, especially where stigma persists. These financing inequalities, when mapped alongside workforce and infrastructure indicators, clearly show how financial commitment correlates with system capacity and access.
Policy, Legislation, and Integration
All 10 countries reported having a national mental health law or policy in place (Table 2). For clarity, we used the following standard terms to categorize implementation status: (a) Comprehensive: All significant provisions of the national mental health law or policy, including governance structures, financing mechanisms, service delivery guidelines, workforce training, and monitoring systems, are fully operational and routinely assessed at the national and subnational levels; (b) State-led variation: Although the policy provisions are present nationwide, they are implemented differently by each state or province. Some regions exhibit complete implementation, while others lag because of resource or local governance disparities; (c) Expanding (in progress): Initial implementation steps (e.g., A formal plans to scale up, pilot programs, and regional roll-outs) are underway; key components are operational but not yet widespread; (d) Ongoing (phased implementation): A planned, multi-phase roll-out is underway, with policy components (such as funding, training, and legislation) being implemented one after the other over predetermined time periods; (e) Moderate: Although laws or policies have been passed, there are gaps in enforcement, data collection, and service guidelines; (f) Early implementation: Although the policy has been formally adopted, only the initial stages, such as stakeholder consultations, have been completed; (g) Limited (resource constraints): Although the policy framework is in place on paper, the lack of adequate financial, human, and infrastructure resources prevents its meaningful implementation beyond small-scale projects; (h) Fragmented (uneven by state): Multiple, non-harmonized policy instruments or programs operate in various regions without central coordination, resulting in significant inter-state disparities in scope and quality of implementation. (i) Weak: Recent paper policy change, but there is a severe financial, human, or infrastructure-related dearth that makes almost no implementation. For HICs, policies have been closely aligned with the UNCRPD, including the establishment of enforcement mechanisms and regular assessments. Although most UMICs and LMICs have their policies aligned with the UNCRPD, the implementation and financing of these policies remain weak. For example, Nigeria and South Africa have national strategies but lack regional compliance mechanisms and a coordinated implementation framework.
One of the important features that distinguishes the HICs from others is the integration of mental health services. The UK and Australia, two HICs, reported full integration, including the establishment of referral channels and training for General Practitioners (GPs). Brazil, a UMIC, has also shown strong PHC involvement through its Psychosocial Care Centers (CAPS) model. Nigeria and Kenya lacked integration, with services limited to tertiary centers.
Treatment Gap and System Performance
The percentage of people with a diagnosable mental illness who do not receive treatment, or the treatment gap, was noticeably higher in LMICs. All five examined LMICs had treatment gaps exceeding 75%. Nigeria’s treatment gap exceeded 90%, ranking among the highest globally. While LMICs showed treatment gaps of over 75%, HICs, such as the UK and Germany, reported gaps of between 20% and 25% (Table 2 and Figure 3). Inadequate infrastructure, stigma, financial barriers, and a lack of human resources all contribute to this disparity. Treatment gap values from the literature, based on regional studies, were used in areas where official estimates were unavailable.
Policy, Mental Health Legislation, Policy Implementation, Integration, Treatment Gap, and DALY Rates by Country.
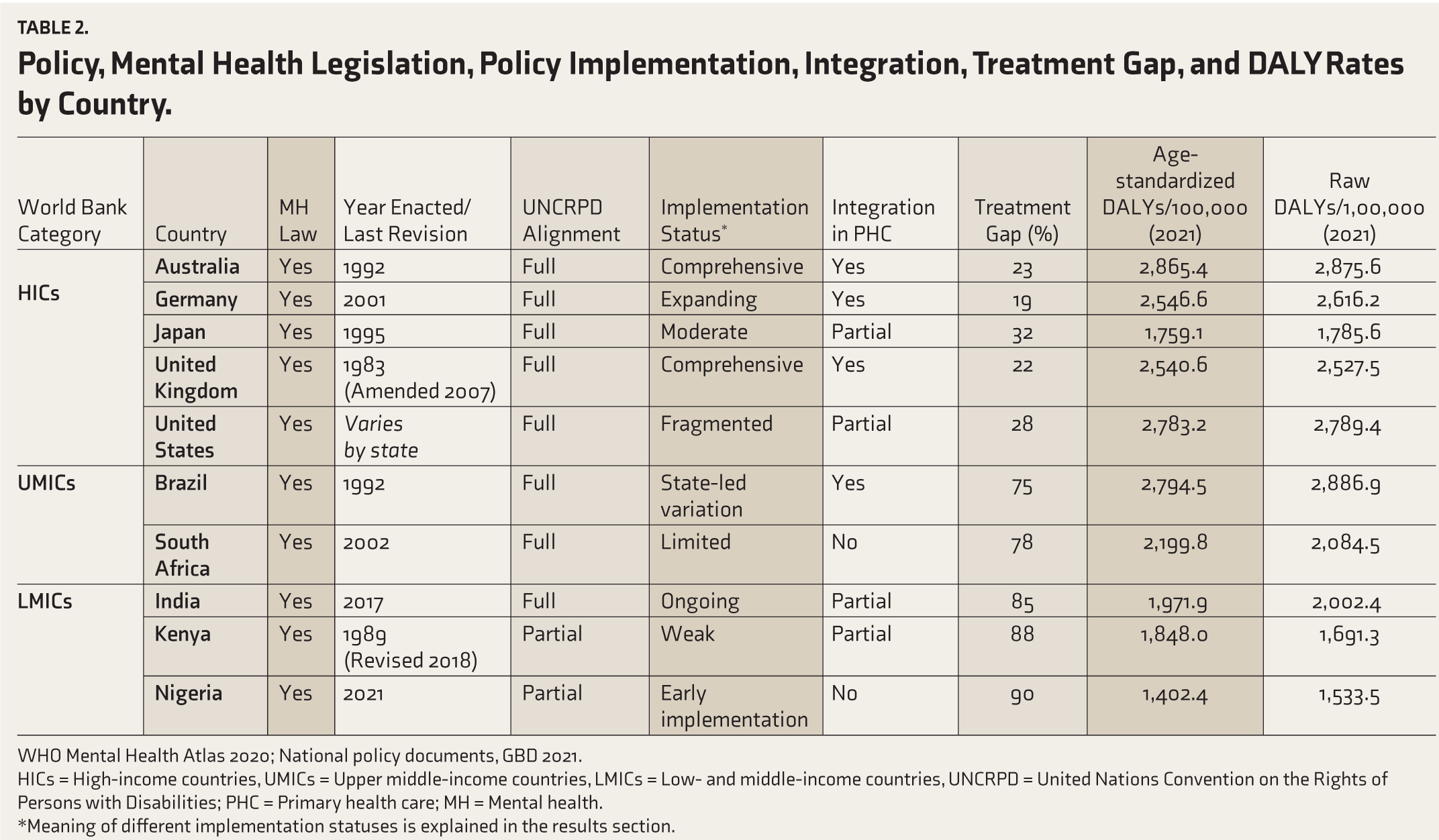
WHO Mental Health Atlas 2020; National policy documents, GBD 2021.
HICs = High-income countries, UMICs = Upper middle-income countries, LMICs = Low- and middle-income countries, UNCRPD = United Nations Convention on the Rights of Persons with Disabilities; PHC = Primary health care; MH = Mental health.
*Meaning of different implementation statuses is explained in the results section.
WHO Mental Health Atlas 2020; National reports on treatment gap.
Service Integration and Access
The presence or absence of mental health service integration into PHC proved to be a critical system-level variable. Countries with integrated PHC systems (e.g., UK, Brazil) had lower treatment gaps and more equitable access, especially in rural and underserved regions. Conversely, LMICs without integration models (e.g., Nigeria and Kenya) reported significant differences in access to care between urban and rural areas.
There are innovations at the partial integration level in countries like India and South Africa. These models have shown potential but need scaling and financing. Despite progress, the District Mental Health Program (DMHP) in India continues to struggle with significant inadequate professional workforce supply and urban-rural maldistribution, lack of infrastructure, medicines, financing, data flows, sparse integration with primary care, and strong cultural stigma against service use. 27
Burden of Disease: DALYs and Suicide
As shown in Table 2, both HICs and LMICs have high raw rates of DALY per 100,000 people because of mental health problems. The high raw DALY rates in Nigeria, Kenya, and India reflect the unmet needs of the LMICs.
Conversely, the age-standardized DALY rates revealed a different trend. HICs, such as the US (2,783.2), Australia (2,865.4), and Germany (2,546.6), had a higher age-standardized DALY rate than most other LMICs, primarily due to their older populations and more intensive monitoring. Conversely, countries with lower age-standardized DALYs included Nigeria (1,402.4), Kenya (1,848.0), and India (1,971.9). This discrepancy highlights a key paradox in global mental health metrics. Although LMICs are under considerable systemic pressure, their epidemiological burden may be underestimated due to insufficient reporting and a young population structure. Suicide-related mortality, for which data were available, followed a similar trend-often higher in under-resourced countries, reflecting deeper treatment gaps and delayed interventions.
Summary of correlation analysis results revealed several significant relationships (Table 3). As shown by the positive correlation between GDP per capita and the prevalence of psychiatrists (r = 0.77, p < .001), the share of mental health budgets in the OOP is strongly correlated to the gap in treatment (r = -0.82, p < .001), suggesting that financial prioritization improves access.
Pearson Correlations Between Key System-level Mental Health Indicators.
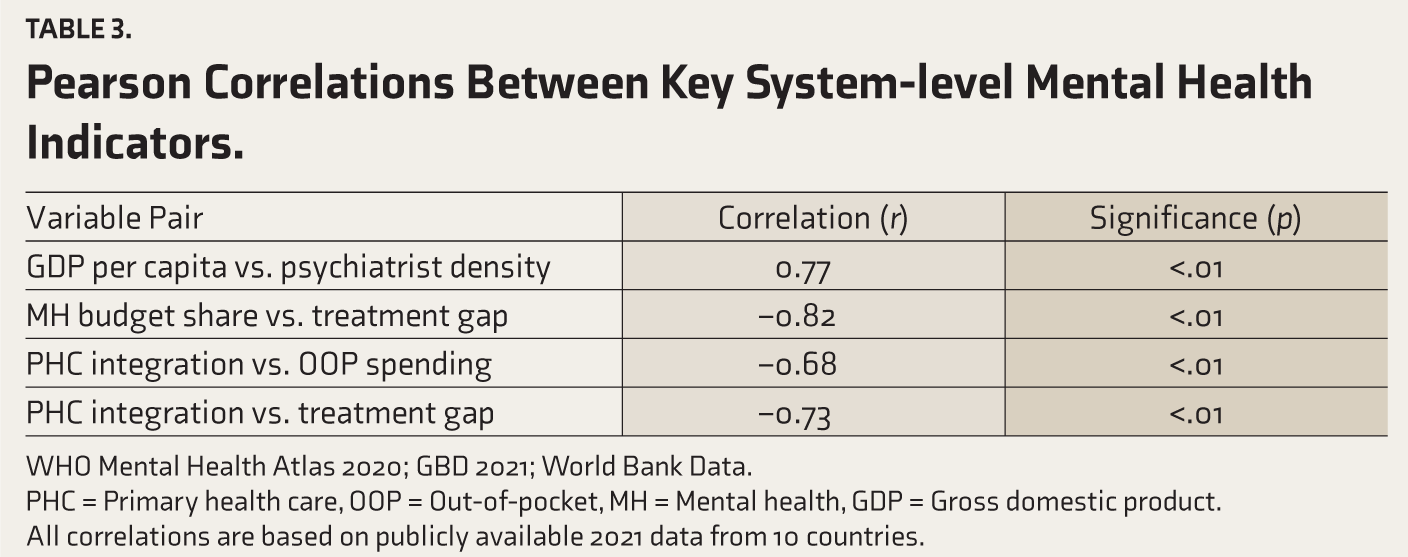
WHO Mental Health Atlas 2020; GBD 2021; World Bank Data.
PHC = Primary health care, OOP = Out-of-pocket, MH = Mental health, GDP = Gross domestic product. All correlations are based on publicly available 2021 data from 10 countries.
Discussion
This study underscores the persistent global disparities in mental health system capacity and effectiveness, as LMICs face persistent barriers to mental health care. While HICs continuously improve and broaden their integrated mental health systems, LMICs often suffer from chronic underfunding, shortages of healthcare workers, and inconsistent policy implementation. These findings echo concerns expressed by the World Health Organization and the Lancet Commission, both of which have called for urgent reforms to address the shortcomings in mental health care worldwide.28,29
Workforce Shortages
The WHO recommends having at least one psychiatrist for every 100,000 individuals; yet, over half of the countries analyzed have not met even this fundamental benchmark. Psychologists, psychiatric nurses, and social workers are also scarce in rural areas. 28 For example, in contrast to many HICs, which have more than 20 mental health professionals per 100,000, India has less than 0.30. 30
Infrastructure and Service Models
In countries like Nigeria and Kenya, there are few options for community-based or outpatient care. They rely on centralized mental health facilities as a primary source of care. Institutional care raises risks of abuse, delays, and poor reintegration. 31 Interestingly, Brazilian CAPS have demonstrated a more efficient and patient-centered approach since they are incorporated into regional health systems. 32 The lack of infrastructure and human resources ultimately leads to significant differences in the mental health outcomes of different populations.
Our results demonstrate that contextualizing DALY data is indispensable. Age-standardized DALY rates are commonly used to compare the performance of health systems; however, since the LMIC population is typically younger, they often fail to capture the actual burden accurately. Interestingly, the study showed that the raw DALY associated with mental illness was significantly higher in LMICs such as India (2,002.4 per 100,000), Kenya (1,691.3), and Nigeria (1,533.5) compared to many HICs. This reflects a well-known paradox in the interpretation of global health data. In LMICs, where the population is typically younger, these figures may underestimate the actual burden. Additionally, underdeveloped mental health monitoring systems in LMICs often lead to dependencies on modeled data rather than real evidence, underreporting, and a lack of diagnostic coverage. Thus, raw DALYs may mask severe systemic issues. LMICs already face systemic pressure because of a lack of proper psychiatric staff, low government investment, and poor integration with primary care. In countries like Nigeria and Kenya, even modest raw DALY figures can place an excessive burden on already fragile systems that are ill-equipped to handle them. 33
Financing and Access
Resilient health systems depend on sustained financial support. However, mental health receives less than 1% of the national health budget in the LMICs. Low funding impedes the expansion of services, workforce, and infrastructure. Unused appropriations reduce the visibility of the divestiture portfolio. Budget tracking mechanisms, such as the System Dynamics (SD) models introduced in Australia, the Mental Health Investment Standards (MHIS), and the Socio-technical Resource Allocation (STAR) model, could be adapted for the LMIC setting to ensure ring-fenced funding and systematic growth.34–36 Certain LMICs in this study had OOP costs for mental health care that were more than 70%. This suggests ineffective risk-pooling and universal health coverage (UHC). Weak UHC frameworks force patients into high OOP mental health costs. Nigeria’s situation is emblematic: despite increasing public health insurance penetration, mental health remains largely excluded from coverage, contributing to catastrophic health expenditures and worsening health inequities. 37
Policy Implementation
While every country in our sample has a mental health policy or law on paper, implementation remains a key weakness. For instance, India’s Mental Healthcare Act (2017) ensures that mental health services are accessible to everyone and removes the criminalization of suicide. However, according to a recent WHO review, fewer than 20% of Indian states have fully implemented the law due to weak infrastructure, staffing, and funding. 38 In HICs, execution is typically more effective and frequently linked to measurable results. The Japanese legal framework requires regular assessments of the quality of services and protection of patients’ rights, and the UK requires annual reports on funding and outcomes in the mental health sector.39,40 LMICs can adopt similar approaches by setting up national mental health commissions, publishing annual accounts, and engaging with civil society.
The PHC Integration and Community Innovations
Integrating mental health into PHC represents one of the most underutilized opportunities to broaden access. WHO’s endorsement of this strategy is based on evidence that the most common mental disorders can be diagnosed and managed at the primary level, provided staff are trained and referral systems exist. 41 Yet, in many LMICs, primary care providers lack both the training and confidence to screen for or treat mental illness. India’s DMHP provides insights into both the advantages and challenges of integration. When properly implemented, the DMHP increased mental health access in rural regions and incorporated services into PHC clinics. Nevertheless, in many states, the program operates only on a superficial level, characterized by inadequate staffing, inconsistent drug supplies, and a lack of proper monitoring. Training, oversight, and extensive system modifications are required for national-level scaling of integration. 27
The HICs provide excellent integration examples. Evidence-based treatments are readily accessible in the UK due to the IAPT (Improving Access to Psychological Therapies) program, which integrates psychological services into GP clinics. Evaluations of the IAPT program have demonstrated lower costs, enhanced patient satisfaction, and reduced unemployment and absenteeism rates. 42 Brazil’s CAPS system, which has multidisciplinary teams and strong ties to PHC, provides an LMIC-appropriate model. 32 Kenya and Nigeria have begun pilot integration projects within PHC, but these efforts will not be viable or able to grow nationally without donor support and political will. 43
Community mental health programs have proven that adequate care is achievable even in resource-constrained environments. The Friendship Bench in Zimbabwe trains lay health workers to provide problem-solving therapy in public areas, and it has been rigorously assessed and expanded nationally. 44 Similarly, the MANAS trial, in which non-specialist health workers coordinated collaborative stepped care intervention for depression and anxiety in primary care, showed encouraging results in specific randomized controlled trials. 45 Despite their potential, these projects usually face sustainability-related obstacles, as most of them rely on donations or non-governmental organizations for assistance. For effective scaling, governments must establish policy structures that incorporate task-sharing into workforce strategies, outline supervisory frameworks, and allocate specific funding sources. The WHO’s Mental Health Gap Action Program (mhGAP) guides implementation; however, the fidelity of these models varies and is contingent upon local engagement. 46
Youth Mental Health
Depression has emerged as the leading cause of disability among adolescents globally, and suicide is the fourth leading cause of death for individuals aged 15–19, with most of these deaths occurring in LMICs. Nevertheless, only a few nations have formulated dedicated policies or services for youth mental health.47,48 Australia has established youth-focused services, such as headspace centers, which offer combined mental, physical, and career support. 49 None of the LMICs included in the study had a national initiative of a similar nature.
Because untreated youth mental illness has long-term effects, such as school dropout, substance abuse, and intergenerational poverty, this neglect is particularly detrimental. 50 The LMICs must establish programs for early detection, digital harm reduction, gender-based violence prevention, and initiatives aimed at improving mental health literacy in schools.
Equity and Rights
Discrimination, stigma, and criminalization make LGBTQ+ individuals, refugees, and ethnic minorities vulnerable. 51 Despite constitutional protections, Black and colored communities in South Africa report substantial unmet mental health needs due to socioeconomic disadvantages and long-standing mistrust of the healthcare system. 52 Comprehensive and culturally relevant rights-based frameworks need to be established, linked with anti-discrimination laws and strategies aimed at achieving health equity.
Strategic Recommendations for System Strengthening
National mental health financing plans: Implement investment criteria for mental health that link the allocation of funds to service expansion, staff development, and infrastructure development.
Decentralized service models: To improve access, establish primary and community health services that encourage local participation, cooperation between the public and private sectors, and peer-led initiatives.
Workforce planning and support: Provide incentives for rural placements, enhance mental health training for various positions, and formally recognize task-sharing in healthcare systems.
Integrated data systems: Health management information systems should incorporate mental health surveillance to monitor equity metrics, service utilization, and prevalence.
Policies focused on youth: Develop national policies addressing the mental health needs of young people. Those regulations should integrate aspects of technology, education, employment, and child welfare.
Empowering communities: Include mental health support organizations, peer support programs, and the views of people who have experienced the system firsthand in its design and evaluation.
Strengths and Limitations
The strengths of this study include its in-depth cross-country comparison of mental health systems across income brackets, which is ensured by using standardized data sets from the World Bank, the GBD, and the WHO. A multifaceted assessment of workforce, financial, political, and service integration provides a comprehensive understanding of systemic differences. The inclusion of geographically diverse LMICs and HICs increases the universality of the findings for global mental health reform, and the strong empirical correlation between economic capacity and mental health outcomes provides policy-relevant insights.
Although we used the latest available data (mostly from 2019 and GBD 2021), the quality of reporting varies from country to country, particularly among the LMICs, which may have had an impact on the accuracy of our estimates. Second, the cross-sectional design of the study, together with the purposive sampling employed, restricts to some extent the study’s ability to establish cause-and-effect relationships. The sampling approach is rational; however, given that countries were not chosen randomly and not all countries that met the criteria were included, it may result in selection bias. This, in turn, impacts the ability of the findings to be generalized to all countries within each income category. We attempted to mitigate this limitation by rigorously applying selection criteria and including countries from diverse geographic regions. Third, some indicators—in particular, the breakdown of mental health expenditure and the suicide rate—were either missing or not reported in an orderly manner. The complexity of the sociopolitical environment in individual countries shapes the development of mental health policies.
Conclusions
This research offers an in-depth cross-sectional analysis of mental health systems in 10 diverse countries. It highlights how various factors, including income levels, policy formulation, system cohesion, and financial investment, impact population-level health outcomes. The HICs have made notable progress, while many LMICs find themselves at a crucial juncture. Without targeted reforms, the disparities in treatment will persist.
Nevertheless, this research is also encouraging. Brazil and Zimbabwe have shown that there are scalable, local solutions. With the proper financial support, better political will, and community involvement, countries can restore their mental health systems.
The LMICs should be supported by academic institutions, development partners, and international organizations such as the WHO. They can provide opportunities for exchanges of expertise, knowledge, and sustainable financing techniques. Dignity, productivity, and prosperity depend on mental health. It is not only morally imperative, but also legally imperative to ensure that everyone has access to high-quality mental health services, regardless of their identity, geographical location, or financial situation.
Supplemental Material
Supplemental material for this article is available online.
Supplemental Material
Supplemental material for this article is available online.
Supplemental Material
Supplemental material for this article is available online.
Supplemental Material
Supplemental material for this article is available online.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
The authors express their sincere gratitude to the World Health Organization (WHO), the Global Burden of Disease (GBD) research team, and national health authorities for making publicly accessible datasets available, which made this comparative analysis possible. The authors also thank all contributors involved in curating the WHO MiNDbank and Mental Health Atlas resources, which provided invaluable information for this cross-national study.
Copyright
All the images and tables, both in the main article and in supplementary material, are original, and no copyright material is used. Data taken from secondary sources is all publicly available by different global and national bodies for public use. The authors take full responsibility for all the material used.
Data Sharing Statements
We used data widely available from the government or other well-known sources. Extracted data is available in supplementary files A, B and C; extra statistical analysis due to limitation of scope is provided in Supplementary file D, and the data source directory with links from where data has been taken is also provided in table format within supplementary file A (
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Disclaimers
The views expressed in this manuscript are solely those of the authors and do not necessarily represent the views of their affiliated institutions.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
As study include only secondary data and no direct participants involved, no consent was required.
Prior Presentations
Not done.
Simultaneous Submission to Another Journal or Resource
None.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.