
Abstract
Background:
Psychiatric disorders contribute significantly to the global burden of disease, especially in rural areas with limited healthcare resources. Psychiatric medications are essential for managing these conditions, but their availability and appropriate use remain inadequate at Primary Health Centers (PHCs) in India.
Methods:
This is a secondary analysis conducted within a larger cluster randomized controlled trial (RCT) evaluating the add-on Online Mental Health Training (OMHT) for primary care doctors (PCDs) compared with training as usual (TAU). The primary outcomes of the RCT were patient-level diagnostic and treatment concordance with psychiatrist assessments, reported separately. In this article, we focus on psychiatric medication requisition patterns as a proxy for clinical practice improvement among PHCs in Tumkur District, Karnataka, India. Psychiatric medications procurement data were extracted from a centralized drug procurement portal across three phases: Pre-training, training and assessment, and post-training.
Results:
Within-group analysis over time showed a statistically significant increase in the proportion of PHCs procuring amitriptyline in both the OMHT arm (p = .01) and the TAU arm (p = .03). Additionally, in the OMHT arm, there was a significant increase over time in the proportion of PHCs procuring alprazolam (p = .03) and clonazepam (p = .02).
In the between-group comparison of total quantities procured during the combined training and post-training phases, the OMHT arm demonstrated significantly higher procurement of escitalopram (p < .01) and risperidone (p < .01) compared to the TAU arm, indicating greater confidence in prescribing practices of key psychiatric medications among trained PCDs.
Trial Registration:
Clinical Trials Registry of India (CTRI/2024/02/062906).
The add-on OMHT program demonstrated the potential of digitally driven mental health training to improve psychiatric medications procurement trends at PHCs. This suggests a scalable strategy for enhancing access to evidence-based mental health care in resource-limited settings. Future studies should link procurement trends to clinical and patient outcomes to better understand the long-term impact of such interventions.Key Messages:
Mental health is a critical component of overall health, with a rising burden of psychiatric disorders globally. 1 In India, they contribute significantly to morbidity and disability, particularly in rural areas where healthcare resources are limited.2,3 Despite growing awareness, mental health care accessibility remains a substantial challenge in India, especially at the level of Primary Health Centers (PHCs), which serve as the first point of contact for healthcare in rural and semi-urban regions. 4
PHCs play a vital role in managing and treating common mental health conditions due to their accessibility to a broad segment of the population; however, these centers often face barriers such as a shortage of trained mental health professionals, limited resources, and stigma surrounding mental health issues. 5 Primary care doctors (PCDs) at PHCs typically lack formal training in mental health care, making it challenging for them to independently identify, manage, and prescribe psychiatric medications for patients with mental health disorders. 6
Psychiatric medications, including antidepressants, antipsychotics, anxiolytics, and mood stabilizers, are essential tools for treating common psychiatric disorders and can significantly improve the quality of life for persons with mental health conditions. 7 When used appropriately, these medications reduce distress and enable patients to participate more fully in daily life. For PHCs, having an adequate supply and proper requisition of these medications is crucial for effective mental health service delivery. However, the lack of training in psychiatric medication management often leads to under-prescription or inappropriate use, which affects patient outcomes and can exacerbate the stigma associated with mental health. 8 Therefore, ensuring an adequate supply and proper requisition of psychiatric medications is crucial for effective mental health service delivery at PHCs.
Several programs have aimed to equip PHC doctors with the skills and knowledge needed to integrate mental health services into primary care.9,10 These initiatives have highlighted the need for scalable, structured approaches to address the persistent gaps in mental health care delivery. The current study is part of a multi-state, digitally driven capacity-building program designed to strengthen primary mental healthcare by training primary care providers in mental health practices. As part of this program, a cluster randomized controlled trial (RCT) was conducted in the Tumkur district, Karnataka, to evaluate the effectiveness of an online mental health training (OMHT) program. The cluster RCT assessed whether the training improved diagnostic and treatment concordance and facilitated the integration of mental health services into general healthcare.
This study, derived from the cluster RCT, examines whether a structured additional OMHT program (add-on OMHT) improves knowledge and confidence among PCDs at PHCs to appropriately procure psychiatric medications compared to training as usual (TAU). By using psychiatric medication requisition data as an objective measure of practice change, rather than relying on subjective assessments such as Knowledge, Attitudes, and Practices surveys, cross-sectional evaluations, or self-reports.9,11,12 This study provides concrete evidence of clinical behavior shifts and enables ongoing monitoring through electronic systems, aiming to enhance mental health care access in rural and underserved areas. The increased requisition of psychiatric medications from warehouses may serve as indirect evidence of improved identification and management of psychiatric conditions by trained PHC doctors. It hypothesizes that PCDs who received add-on OMHT will demonstrate a statistically significant increase in the requisition of essential psychiatric medications compared to those in the TAU arm.
Methods
This study is part of a comprehensive evaluation of an add-on OMHT program, which aims to enhance mental health care capacity across healthcare cadres, including PCDs, auxiliary nurse midwives, and accredited social health activists (ASHAs). The add-on OMHT program comprises six remote training sessions over six weeks, followed by six months of continued mentoring through Collaborative Video Consultations (CVC). CVC involves real-time consultation between a specialist and the primary care doctor, who would review the patient in person, with input from the specialist. 13 Participants from over nine Indian states were involved in this multi-state, digitally driven capacity-building program initiative.
For the outcome evaluation, Tumkur district in Karnataka, India, was selected as the study site. Within this district, PCDs routinely participate in ongoing mental health training programs, such as those provided by the District Mental Health Program (DMHP). A cluster randomized approach was used to divide the taluks into two arms. Taluks randomized to the add-on OMHT arm received supplementary training comprising six remote sessions over six weeks, conducted by psychiatrists, followed by six months of tele-mentorship through CVCs, facilitated by psychiatrists. Taluks in the TAU arm continued with only the ongoing mental health training provided through programs such as DMHP. Cluster randomization was carried out by the principal investigator, ensuring that each taluk was assigned to either the add-on OMHT or TAU arm. Outcome assessors were blinded to allocation.
The present article reports a secondary analysis focusing on one year of psychotropic medication procurement patterns as a proxy indicator of clinical practice change. Sample-size estimation and power assumptions were determined for the parent trial’s primary patient-level outcomes and are reported in detail elsewhere. 14 , 15 Procurement outcomes were not powered a priori. Procurement outcomes were not powered a priori, as this analysis focuses on service-level indicators rather than patient-level outcomes.
In the present article, we focused on patterns and trends in psychiatric medication requests at the PHCs assessed for a cluster RCT. Data on psychiatric medications procurement were obtained from the e-Aushada portal (
Study Period
The study was conducted over 12 months, from October 2023 to September 2024, and was divided into three distinct phases:
Pre-training Period (October 2023–January 2024; Four Months)
During this phase, no interaction occurred with the PCDs of either the add-on OMHT arm or the TAU arm regarding the OMHT. This period was primarily dedicated to logistical and administrative preparations for the training program.
Training and Assessment Period (February 2024– May 2024; Four Months)
During this phase, training sessions were conducted for PCDs from the PHCs in the add-on OMHT arm. Assessments for both the add-on OMHT and TAU arms were carried out in person by qualified psychiatrists at the PHCs during this period.
Post-training Period (June 2024–September 2024; Four Months)
This phase focused on the sustainability of the interventions following the training. No onsite assessments were conducted with the PCDs during this period to evaluate outcomes.
Study Design
The analysis in this study was conducted as part of a larger cluster RCT evaluating OMHT for PCDs. While the main trial focused on diagnostic and treatment concordance, this article reports a secondary analysis of psychiatric medication procurement patterns over one year at PHCs.
A total of 26 PHCs from the Tumkur district were randomized into two groups:
Intervention Group/Add-on Online Mental Health Training (OMHT)
The PCDs from 13 PHCs received OMHT from psychiatrists affiliated with the Mental Health Program. During the four-month training phase, PCDs in the intervention group engaged in virtual sessions focused on psychiatric medication management, with active guidance from qualified psychiatrists. In addition to this structured add-on OMHT, the intervention group also participated in the ongoing mental health training provided through the DMHP, which was available to both groups.
Control Group (Training as Usual)
The PCDs from 13 PHCs in the control group participated in the ongoing mental health training typically provided through programs such as the DMHP. These programs, organized by the state government, are conducted as full-day sessions at the district headquarters and typically last up to five days. The DMHP-run program provides foundational training for managing mental health conditions and was open to both the intervention and control groups. This “TAU” arm serves as the baseline for evaluating the additional impact of the add-on OMHT intervention.
Timing and Structure
While the control group continued with the routine DMHP training programs (which had last occurred in February 2024), the intervention group received additional OMHT sessions conducted over four months, starting in February 2024 through May 2024.
Data Collection
Detailed requisition records were obtained from the e-Aushada portal for psychiatric medications requested from the Tumkur District warehouse and distributed to each PHC during the study period. This included data on the number of boxes of each psychiatric medication sent to each PHC, enabling a precise analysis of requisition trends. This study included oral psychiatric medications available in tablet and capsule forms, namely alprazolam, amitriptyline, clonazepam, diazepam, escitalopram, fluoxetine, haloperidol, lorazepam, olanzapine, risperidone, and sodium valproate.
Data Analysis
The Kolmogorov–Smirnov test was used to test normality. Continuous variables were reported with mean and standard deviation or median and interquartile range (IQR) as appropriate. Comparison between pre-, during-, and post-training PHC was performed using the Cochran’s Q test. The Mann–Whitney U test was used to determine whether there was a significant difference between offline and online PHC training scores. Given the small number of clusters, advanced models (e.g., generalized estimating equations and mixed-effects regression) were not feasible; therefore, nonparametric tests at the PHC level were used. Analysis included PHCs with procurement data available across all three study periods in both groups. IBM Statistical Package for the Social Sciences (SPSS) Statistics 29.0 was used for statistical analysis. A p value < .05 is considered statistically significant.
Results
Socio-demographic Characteristics of Primary Care Doctors (PCDs) and the Patients Screened
Each arm comprised 13 PCDs. In the add-on OMHT arm, the mean age of PCDs was 38.77 (±9.58) years, while in the TAU arm, it was slightly higher at 41.85 (±9.31) years. PCDs in the add-on OMHT arm had an average of 15.23 (±8.50) years since completing university and 12 (IQR: 7–19) years of work experience, compared to 18.08 (±9.02) years since completing university and 15 (IQR: 7–21) years of work experience in the TAU arm. Both groups had comparable exposure to psychiatric training during their MBBS and internships. Moreover, recent psychiatric training within the last year was similar between the TAU arm (n = 8, 61.5%) and the add-on OMHT arm (n = 7, 53.8%). A higher proportion of PCDs in the TAU arm (n = 11, 84.6%) attended DMHP training, a common program for both arms, compared to 69.2% (n = 9) in the add-on OMHT arm. There was no significant difference between the two groups in the socio-demographic characteristics studied.
The socio-demographic characteristics of the patients were captured cross-sectionally during the training and assessment period, when assessors visited PHCs for diagnostic and treatment concordance. Of the 289 patients screened in each arm, 118 were identified as having a psychiatric diagnosis and included for further analysis. The following socio-demographic findings refer to these 118 patients in each arm. The mean age of patients in the add-on OMHT arm was 55.19 (±15.23) years, while in the TAU arm it was 51.86 (±15.03) years. In the add-on OMHT arm, males comprised 48.3% and females 51.7%; in the TAU arm, males comprised 51.3% and females 48.7%. Most patients in both groups were from rural areas (OMHT: 91.5%; TAU: 94.9%) and came from families below the poverty line (OMHT: 94.1%; TAU: 96.6%). A small proportion of patients had a history of prior mental health treatment (OMHT: 7.6%, TAU: 5.1%), predominantly pharmacological.
There was no significant difference between the two groups in the socio-demographic characteristics studied. For more detailed information on the socio-demographic profiles of both the PCDs and the screened patients, please refer to the related manuscript. 15
Proportions of Primary Health Centers (PHCs) Procuring Psychiatric Medications
Analysis included PHCs with procurement data available across all three study periods in both groups.
Training as Usual (TAU) Arm
In the TAU arm, procurement of psychiatric medications during the pre-training period was limited. Diazepam was procured by 38.5% (n = 5) of PHCs, followed by risperidone at 15.4% (n = 2), while fluoxetine, clonazepam, and valproate were procured by only one PHC (7.7%, n = 1). No PHCs procured alprazolam, amitriptyline, haloperidol, lorazepam, olanzapine, or escitalopram. During the training and assessment period, the proportion of PHCs procuring amitriptyline increased substantially to 46.2% (n = 6). Alprazolam was procured by 23.1% (n = 3). There was a 15.4% reduction in the procurement of clonazepam, diazepam, escitalopram, fluoxetine, and valproate by 15.4% of PHCs (n = 2). In the post-training period, clonazepam procurement rose further to 38.5% (n = 5), and olanzapine to 23.1% (n = 3). The proportion of PHCs procuring amitriptyline and alprazolam declined to 30.8% (n = 4) and 23.1% (n = 3), respectively, although these remained higher than pre-training levels.
Among all medications, only the change in amitriptyline procurement by the PHCs across the three periods was statistically significant (p = .030).
Add-on Online Mental Health Training (OMHT) Arm
In the OMHT arm, diazepam was the most commonly procured drug during the pre-training period (23.1%, n = 3), followed by risperidone (15.4%, n = 2), and fluoxetine and valproate (7.7%, n = 1 each). No other medications were obtained by any PHC during this phase. In the training and assessment period, the number of PHCs procuring psychiatric medications increased substantially. Amitriptyline was procured by 53.8% (n = 7), clonazepam by 38.5% (n = 5), and alprazolam by 46.2% (n = 6). Risperidone procurement also rose to 46.2% (n = 6), and fluoxetine to 30.8% (n = 4). New additions included escitalopram (15.4%, n = 2) and olanzapine (15.4%, n = 2). In the post-training period, procurement of amitriptyline and clonazepam was sustained at 46.2% (n = 6) each, while alprazolam declined to 15.4% (n = 2). Escitalopram showed a further increase to 30.8% (n = 4). Diazepam, fluoxetine, valproate, olanzapine, and risperidone remained stable at 15.4%–23.1% (n = 2–3).
In the OMHT arm, statistically significant increases over time were observed in the proportion of PHCs procuring amitriptyline (p = .014), clonazepam (p = .021), and alprazolam (p = .030), unlike in the TAU arm, where only amitriptyline showed a significant change. However, although not statistically significant, a higher proportion of PHCs in the OMHT arm began procuring escitalopram and risperidone, with a more sustained increase observed for the former in the post-training period as well. For olanzapine and fluoxetine, the proportions fluctuated over time but followed a broadly similar pattern across both arms, without statistically significant change. Details are provided in Table 1.
Comparison of Proportions of Primary Health Centers (PHCs) Procuring Psychotropics Across Study Periods in Training as Usual (TAU) and Add-on Online Mental Health Training (OMHT) Arms.
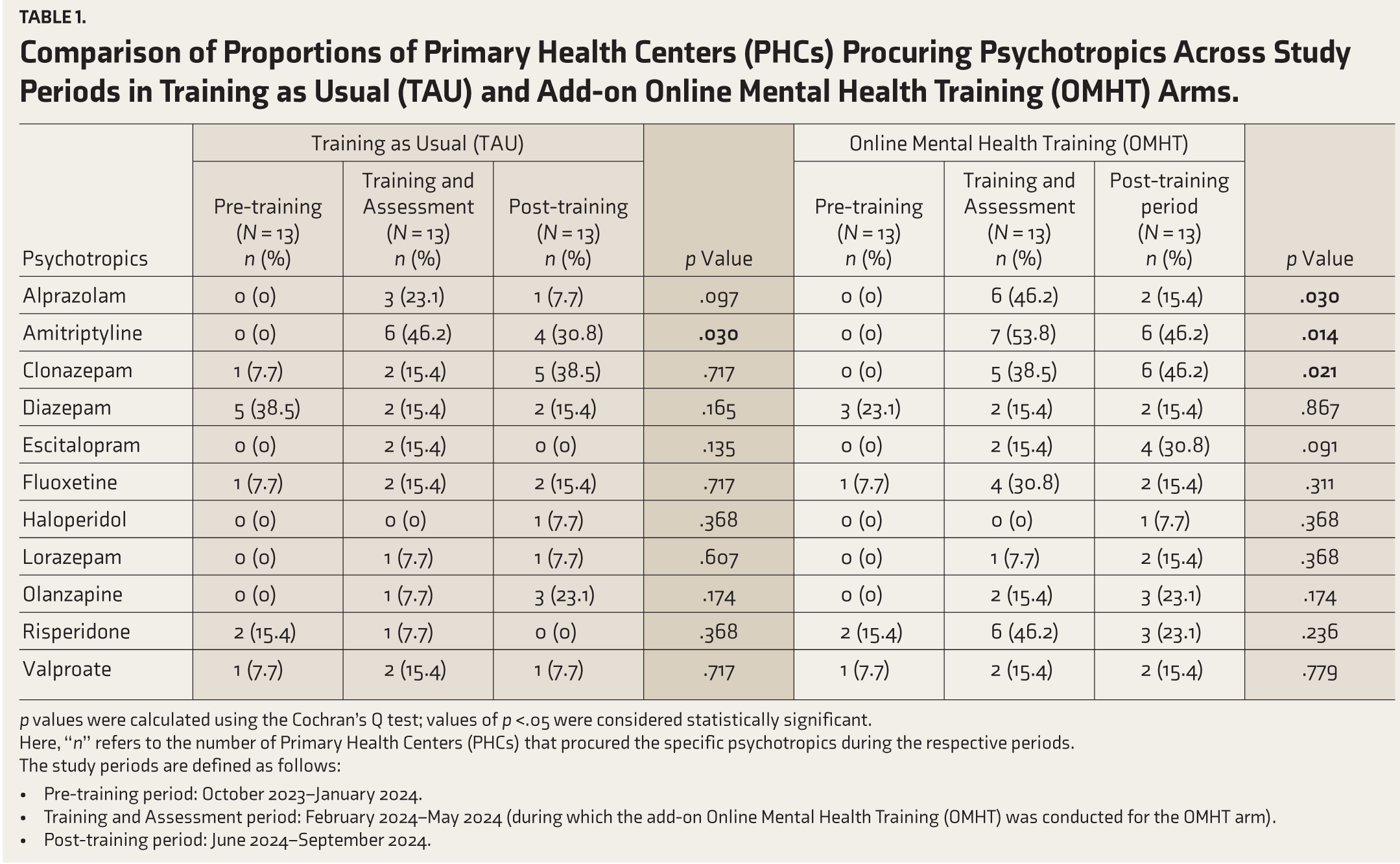
p values were calculated using the Cochran’s Q test; values of p <.05 were considered statistically significant.
Here, “n” refers to the number of Primary Health Centers (PHCs) that procured the specific psychotropics during the respective periods.
The study periods are defined as follows:
Pre-training period: October 2023–January 2024. Training and Assessment period: February 2024–May 2024 (during which the add-on Online Mental Health Training (OMHT) was conducted for the OMHT arm). Post-training period: June 2024–September 2024.
Comparison of Psychiatric Medications Procurement Between TAU and Add-on OMHT Across Study Periods
For this analysis, a “unit” refers to a box containing 10 × 10 tablets or capsules of a given psychiatric medication. For analysis, the training and post-training periods were combined, as several medications had sparse counts when examined separately, which limited meaningful between-group comparisons. Complete procurement data were available for all PHCs in both the OMHT and TAU groups across the pre-training and combined training–post-training periods.
Pre-training Period
During the pre-training period, the procurement of psychiatric medications was comparable between the TAU and add-on OMHT arms. None of the drugs, including alprazolam, amitriptyline, clonazepam, and haloperidol, were procured in either arm, with risperidone and diazepam showing similar low median values (six units and 42 units in TAU compared to 11 units and 13 units in add-on OMHT). As shown in Table 2, all baseline comparisons were non-significant (p > .05), confirming equivalence between the two arms at the start of the study.
Comparison of Psychotropics Procurement Quantities Between Training as Usual (TAU) and Add-on Online Mental Health Training (OMHT).
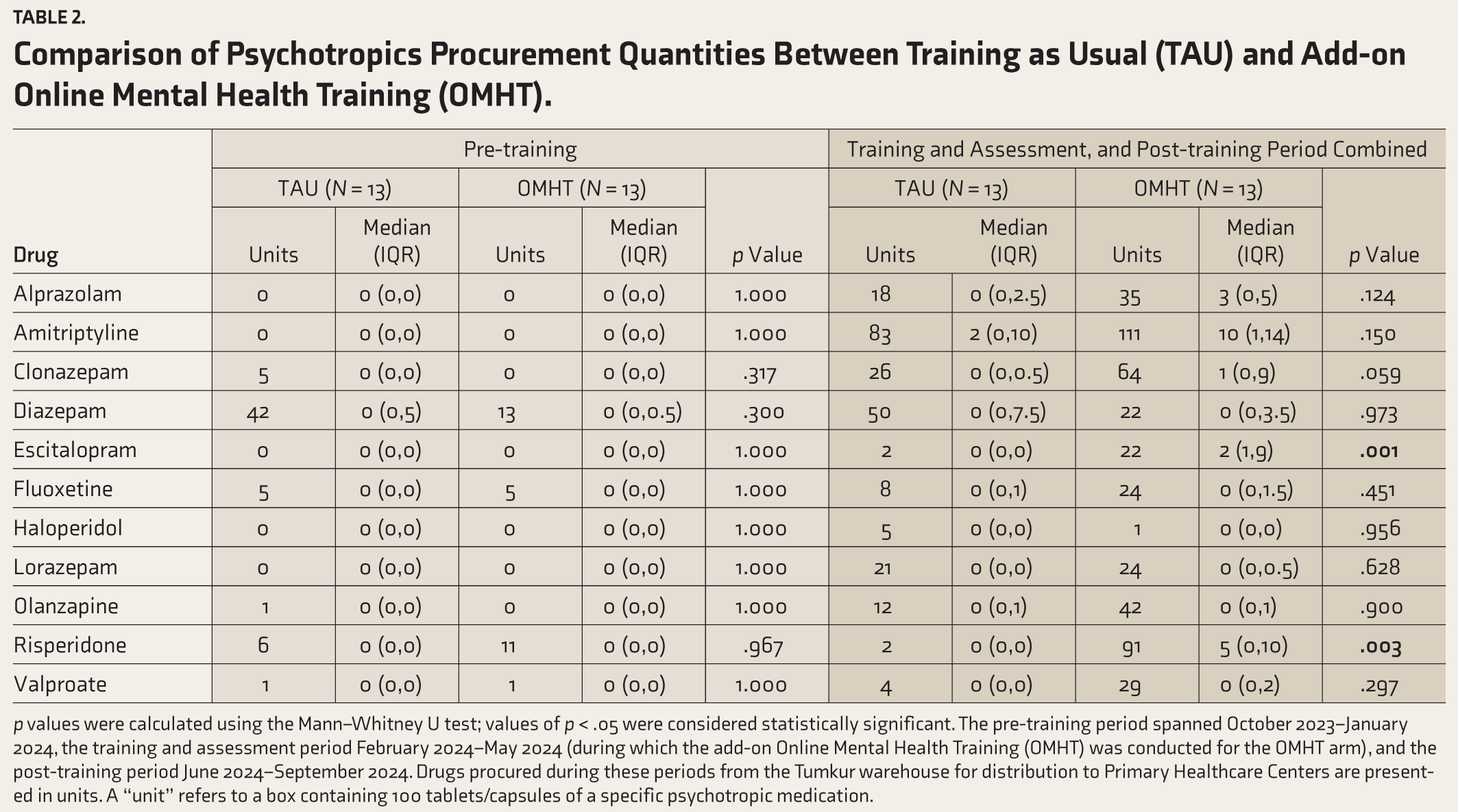
p values were calculated using the Mann–Whitney U test; values of p < .05 were considered statistically significant. The pre-training period spanned October 2023–January 2024, the training and assessment period February 2024–May 2024 (during which the add-on Online Mental Health Training (OMHT) was conducted for the OMHT arm), and the post-training period June 2024–September 2024. Drugs procured during these periods from the Tumkur warehouse for distribution to Primary Healthcare Centers are presented in units. A “unit” refers to a box containing 100 tablets/capsules of a specific psychotropic medication.
Training and Post-training Period Combined
Significant differences emerged between the arms during the combined training and post-training period. The add-on OMHT arm showed markedly higher procurement for escitalopram (median: 22 units in OMHT, two units in TAU; p = .001 and risperidone (median: 91 units in OMHT, two units in TAU; p = .003). While differences in clonazepam, alprazolam, amitriptyline, and diazepam were evident, they did not reach statistical significance (p > .05). The procurement of haloperidol and valproate remained minimal and consistent across both arms, with no significant differences observed.
Monthly Trends by Psychiatric Medication Class
Monthly trends in psychiatric medication procurement revealed distinct patterns between the TAU and add-on OMHT arms, as illustrated in Figures 1–4. Figure 1 highlights antidepressant procurement, showing a steady rise in escitalopram and amitriptyline in the add-on OMHT arm during and after the training period, while procurement in the TAU arm remained minimal across all months. Figure 2 focuses on antipsychotics, where the add-on OMHT arm demonstrated a significant monthly increase in risperidone, compared to limited changes in the TAU arm.
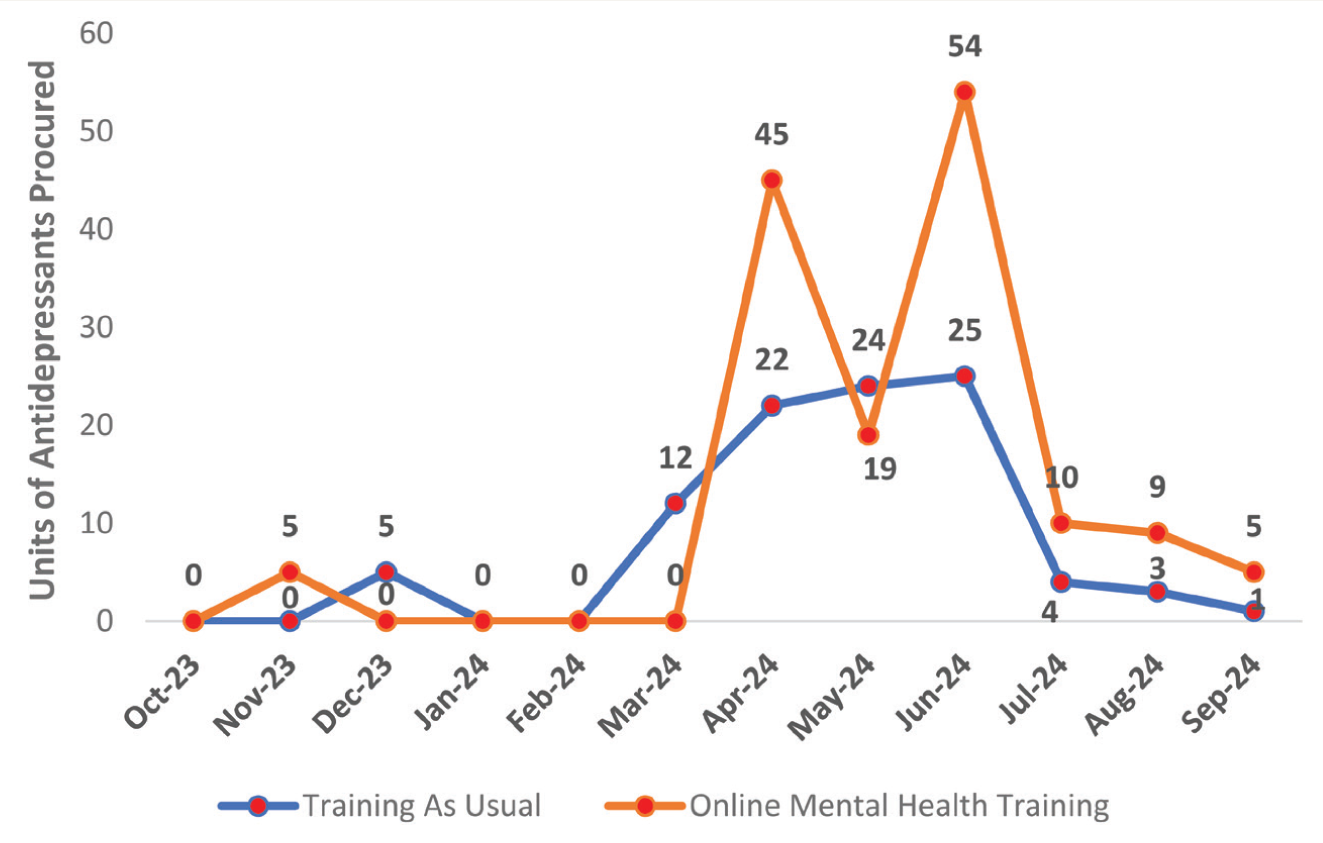
Antidepressants included were Tab. Escitalopram (10 mg), Cap. Fluoxetine (20 mg/60 mg) and Tab. Amitriptyline (25 mg). Training refers to the mental health training provided to Medical Officers (MOs) associated with Primary Healthcare Centers (PHCs). The pre-training period spanned from October 2023 to January 2024, the training period occurred from February 2024 to May 2024 (during which the add-on Online Mental Health Training [OMHT] was conducted for the OMHT arm), and the post-training period extended from June 2024 to September 2024. Drug procurement data during this period, sourced from the Tumkur warehouse for distribution to PHCs, are presented in units or boxes, with each box containing 100 tablets.
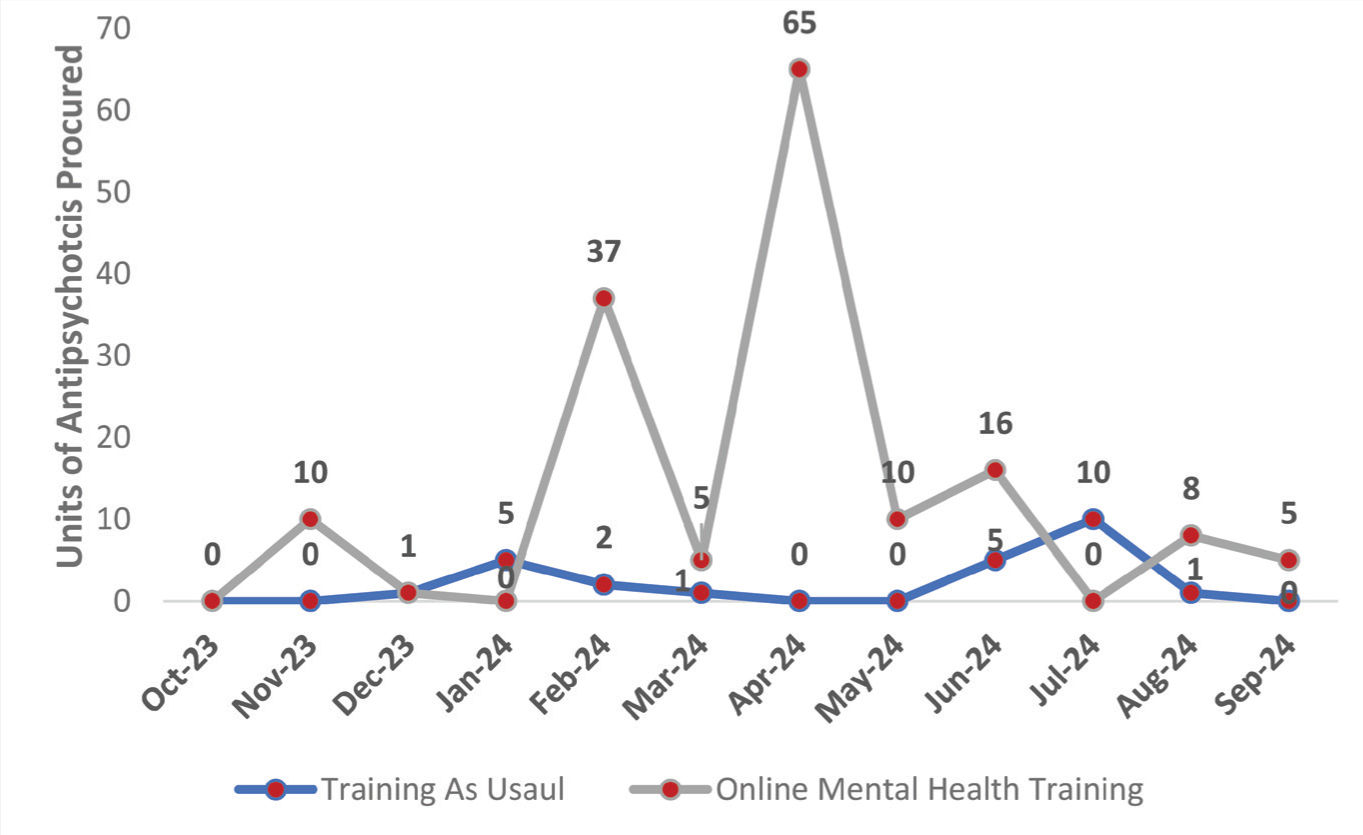
Antipsychotics included were Tab. Risperidone (2 mg/4 mg), Tab. Haloperidol (5 mg), and Tab. Olanzapine (5 mg/10 mg).
Figure 3 presents monthly trends for benzodiazepines, indicating a consistent rise in clonazepam and alprazolam procurement in the add-on OMHT arm, whereas the TAU arm showed stable or negligible changes. Figure 4 displays mood stabilizer procurement, with the add-on OMHT arm showing a gradual increase in valproate over time, though differences between arms were not statistically significant.
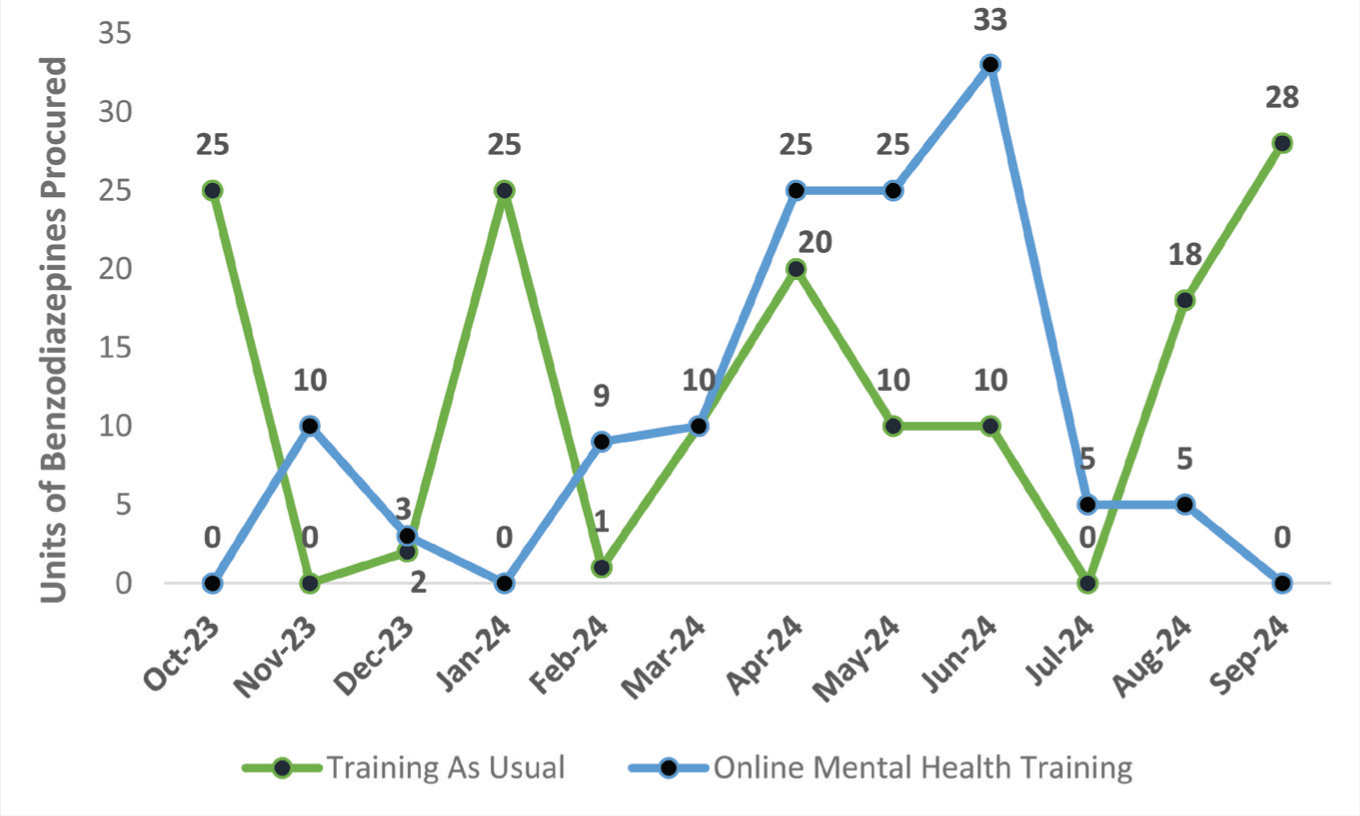
Benzodiazepines included were Tab. Alprazolam 0.25 mg, Tab Clonazepam 0.5 mg, and Tab Diazepam 5 mg.
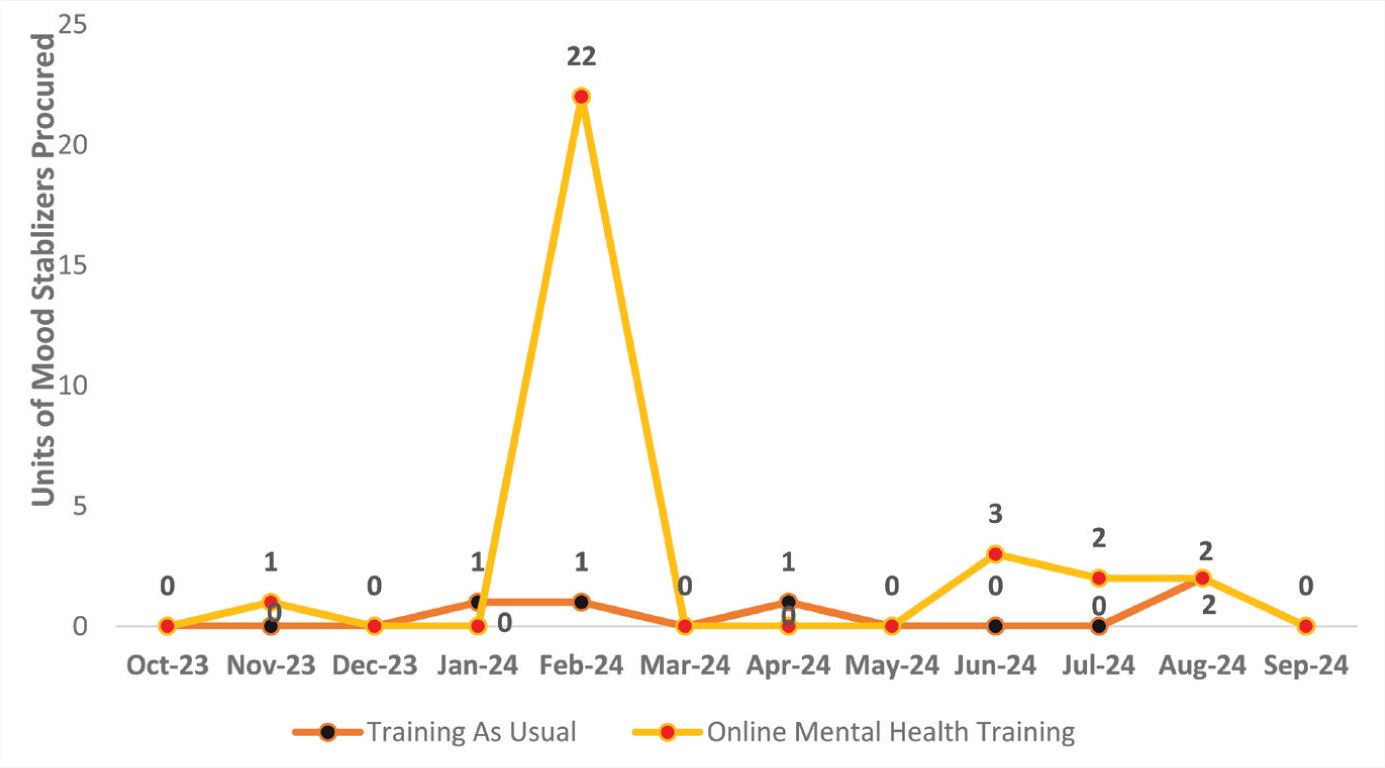
Mood stabilizer included is Tab Sodium Valproate and Valproic Acid CR 500 mg.
Discussion
This study, an extension of a cluster RCT evaluating the add-on OMHT program, examined psychiatric medication procurement as a proxy for translating clinical skills into practice. Data from the State Drug Procurement Portal were analyzed across three phases: Pre-training, training and assessment, and post-training (each spanning four months). During the training and assessment phase, the add-on-OMHT arm received TAU training supplemented with six online mental health sessions and six months of tele-mentoring via collaborative video consultation. Assessors visited PHCs in both arms. The study observed an increase in the number of PHCs procuring psychiatric medications during the training and assessment period, with a more pronounced rise in the add-on OMHT arm. Cumulative requisitions of risperidone and escitalopram were significantly higher in the add-on OMHT arm, reflecting enhanced prescribing practices among trained PCDs. This design enabled a direct comparison of the impact of add-on OMHTs beyond TAU, contributing to evidence on upskilling through additional OMHT.
The mean age of the PCDs in our study was comparable to that reported in previous studies conducted in similar settings. 11 Baseline “TAU” was consistent, with approximately two-thirds of participants receiving brief mental health training, typically lasting less than a week. The DMHP training, conducted biannually for batches of 30 PCDs, usually spans two days. 16 While effective in raising awareness about psychiatric illnesses, it has been criticized for not building sufficient confidence to treat psychiatric conditions. 17 Leveraging technology for capacity-building has gained traction, with online specialist-led training showing promise. However, the outcomes of such interventions are often limited to knowledge and attitude assessments or self-reported measures.9,13 By leveraging existing state-level mechanisms for drug procurement, our study offers a more practical, real-world evaluation of the translation of these training programs’ clinical outcomes.
Impact of Training on Procurement Practices
Baseline procurement of psychiatric medications was notably poor in both arms, with many essential medications never procured by several PHCs. The procurement rate for fluoxetine and risperidone remained below 20%. This aligns with findings from earlier studies in India,18,19 where limited demand and availability for psychiatric treatments from both doctors and patients were observed at the PHCs. Diazepam, often the only psychiatric medication available, was primarily used for temporary management and to stabilize patients before transferring them to higher healthcare centers, 19 a pattern that remains consistent with our observations.
Drug procurement increased in both intervention and control arms, despite the absence of an add-on structured intervention in the latter. This may reflect systemic and behavioral dynamics. The presence of psychiatrists during assessments could have influenced practices through observation effects 20 or passive learning, where behaviors are adopted via informal modeling.21,22 Informal communication among PCDs across PHCs may also have facilitated the spread of practices from the intervention arm to the control arm. 23 Additionally, external scrutiny from visits might have prompted pre-emptive efforts to address gaps in drug availability.
Differences in PHC Level Adoption of Psychotropic Procurement with Training
Beyond the factors contributing to increased procurement during the assessment period, it is essential to highlight the broader improvements observed during the training and post-training phases. These phases marked a clear departure from baseline patterns, with at least some PHCs procuring every listed psychiatric medication—a notable contrast to baseline, where several drugs saw no procurement at all. Within-group analyses revealed a significant increase over time in the proportion of PHCs procuring amitriptyline in both arms, suggesting its widespread perceived utility. However, only the OMHT arm demonstrated additional significant increases in the procurement of alprazolam and clonazepam, indicating that the structured digital training may have enabled a broader and more confident use of psychotropics.
Amitriptyline’s broad clinical utility likely contributed to its consistent uptake, given its effectiveness in psychiatric conditions such as depression and somatization disorder, and non-psychiatric indications such as diabetic neuropathic pain, 24 chronic low back ache, 25 and migraine prophylaxis. 26
This difference between arms in using benzodiazepines, specifically clonazepam, may reflect the impact of ongoing clinical mentoring and structured knowledge reinforcement in the OMHT group, which could have addressed diagnostic uncertainty or hesitation in prescribing. Clonazepam’s long half-life makes it particularly useful for managing anxiety disorders and seizure conditions in low-resource settings where follow-up may be limited. 27 In contrast, the relatively smaller increase in the number of PHCs initiating procurement of other psychotropics may reflect prescriber caution due to narrower indications, perceived side-effect profiles, or uncertainty about appropriate use—barriers that the OMHT program may have partially mitigated through continuous mentoring and case-based discussions.
While combined analyses suggested sustained improvements beyond baseline, monthly trends showed variability once active mentoring ended. Procurement of several drugs declined in the post-training phase, which may reflect reduced confidence without ongoing support, procurement cycle fluctuations, or, in the case of benzodiazepines, more rational tapering after short-term use. In contrast, TAU showed later increases in benzodiazepines, possibly reflecting less structured guidance. The isolated spike in valproate procurement was likely due to bulk requisition or case-specific needs rather than a sustained trend. These nuances highlight the need for ongoing support to consolidate practice changes and sustain rational prescribing.
While the differences were not statistically significant, a notable trend was observed in the add-on OMHT arm, where 23% of PHCs continued to procure risperidone and 30% procured escitalopram, compared to no procurement in the TAU arm during the post-training period. These patterns suggest that targeted training may support continued translation of learning into clinical practice, even beyond the active training period. Broader literature supports this interpretation. A systematic review of task-sharing approaches highlighted how training interventions in low-resource settings can enhance provider competence and improve access to essential mental health services. 28 Similarly, health system strengthening frameworks emphasize that equipping healthcare providers with practical knowledge fosters adherence to evidence-based practices and contributes to improved clinical outcomes.29,30 Although further investigation is warranted, these findings suggest that structured training programs such as the add-on OMHT can promote sustainable improvements in psychotropic prescribing practices. Scaling up such initiatives across PHCs may help bridge existing treatment gaps and empower PCDs to deliver more consistent, evidence-informed mental healthcare. Future research should explore long-term patient outcomes alongside system-level improvements to better guide policy and implementation.
Variations in Quantities Procured Following Training Implementation
An important observation in the add-on OMHT group is the significant increase in the quantity of key psychiatric medications such as risperidone and escitalopram procured by PHCs, even though the proportion of PHCs procuring these medications did not differ significantly from the TAU group. This indicates a potential shift in confidence among PHCs in prescribing and stocking these medications, particularly among PCDs who actively engaged during the training and subsequently started prescribing psychiatric medications, likely influenced by the targeted training provided in the add-on OMHT. Risperidone and escitalopram stood out as medications with statistically significant increases in procurement. Risperidone, an atypical antipsychotic, is widely recognized for its efficacy in managing schizophrenia and other psychotic disorders, with a lower risk of extrapyramidal side effects compared to first-generation antipsychotics such as haloperidol. Its increased procurement in the add-on OMHT arm suggests a more evidence-based approach to managing severe mental illnesses in trained medical officers (MOs) at primary care, potentially replacing the older reliance on haloperidol, which showed no similar increase in procurement, consistent with the training module’s recommendations.
Escitalopram, a selective serotonin reuptake inhibitor, is considered a first-line treatment for depression and anxiety disorders due to its superior efficacy and tolerability compared to other antidepressants. The significant increase in its procurement may reflect heightened awareness among trained MOs of the benefits of using Selective Serotonin Reuptake Inhibitor (SSRI) in the primary care context, driven by the clinical emphasis of the add-on OMHT training. In contrast, the TAU group did not exhibit a comparable pattern of increased procurement for these medications, except for benzodiazepines and amitriptyline, which remained consistent across both arms.
These findings highlight the importance of digitally driven tele-mentoring programs in promoting evidence-based psychiatric medication prescribing. By equipping healthcare providers with the knowledge to prioritize clinically recommended treatments, add-on OMHT demonstrates its potential to bridge gaps in mental health care delivery, particularly in resource-limited settings. Similar trends have been observed in studies highlighting the impact of training programs on improving medication use patterns and adherence to evidence-based guidelines in low-resource settings.9,31
Risks of Irrational Use
While the procurement of amitriptyline and benzodiazepines highlights their utility in primary care, their potential for irrational use warrants caution. Amitriptyline, though effective for depression and neuropathic pain, poses risks of anticholinergic side effects, cognitive impairment, and overdose toxicity. Benzodiazepines, similarly, carry risks of dependence, withdrawal, and psychomotor impairment. 32 These concerns are particularly relevant given the study population’s average age of 45–55 years, a demographic more vulnerable to these adverse effects. Importantly, procurement increases alone cannot confirm clinically appropriate prescribing. The significant rise in benzodiazepines must therefore be interpreted with caution, and future research should link procurement data with patient-level outcomes to determine whether these trends reflect rational treatment or potential overuse.
The consistent procurement of these medications across both arms suggests the emergence of a prescribing trend, potentially reflecting a new practice adopted by healthcare providers. While this may indicate increased familiarity and confidence in using these drugs, it underscores the need for mindfulness in their rational application. Future research should explore the drivers of this trend, assess its clinical appropriateness, and develop strategies to mitigate risks associated with overuse or misuse in resource-limited primary care settings.
Strengths and Limitations of the Study
Strengths of this study include its cluster RCT design, which enabled robust comparisons between the add-on OMHT and TAU arms, and the use of real-world procurement data from a centralized online portal, minimizing bias. The six-month follow-up allowed us to capture sustained effects beyond the immediate training period, and reliance on objective procurement data reduced the influence of social desirability bias.
However, several limitations must be noted. As an offshoot of a larger cluster RCT, the study’s focus on procurement data introduces certain constraints. In person attendance by assessors may have inadvertently influenced participant behaviors. Potential contamination between intervention and control arms also warrants consideration, as informal professional interactions among PCDs and the presence of psychiatrists during assessments may have led to spill-over effects. To minimize this, PCDs in the OMHT arm were instructed not to discuss training materials with colleagues in the TAU arm. Because psychiatrists were present in both arms, any influence arising from their involvement would have been equally distributed, reducing systematic bias. While such communication could have reduced observed differences between arms, it also reflects real-world implementation contexts where cross-learning and external oversight are common.
Procurement data, while objective, do not directly reflect clinical appropriateness or patient outcomes. Patient-level outcomes from the same cluster RCT, including diagnostic and treatment concordance, are reported separately. 15 A further limitation is that patient-level data were collected only cross-sectionally during the training and assessment period, whereas procurement data were longitudinal across all phases. Therefore, we could not directly correlate patient load with procurement trends. Procurement may also have been influenced by existing stock levels and warehouse supply cycles, explaining sudden dips in some months. While procurement serves as a practical proxy for prescribing, actual utilization data would have been a more precise indicator of treatment practices.
From a statistical perspective, the small number of clusters precluded the use of more complex modeling approaches such as Generalized Estimating Equations (GEE) or mixed-effects regression. Instead, nonparametric tests were applied at the PHC level, limiting the ability to adjust for clustering effects. No formal adjustment for multiple comparisons was made, and findings should therefore be interpreted with caution.
Finally, the relatively short follow-up period restricts inference about the sustainability of effects. Increases in procurement cannot by themselves distinguish between appropriate and inappropriate prescribing, and their clinical significance can only be established when linked to patient-level outcomes in future studies.
This study also demonstrates the utility of real-world data in assessing trends in medication procurement. It provides a strong foundation for future research to evaluate drug usage patterns and optimize rational medication use in primary care.
Conclusions
The add-on OMHT program was associated with a significant improvement in psychiatric medication procurement at PHCs, reflecting better prescribing practices among trained PCDs. Compared with the TAU arm, the OMHT arm demonstrated significantly higher levels of risperidone and escitalopram, along with within-group increases in amitriptyline, alprazolam, and clonazepam. While procurement trends serve as a valuable proxy for practice change, they cannot, by themselves, confirm clinical appropriateness; future research linking procurement data with patient-level outcomes will be essential. These findings highlight the potential of digitally delivered mental health training programs to enhance rational prescribing at the primary care level, while also underscoring the need for ongoing mentoring and system-level support to sustain gains over time.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
Same as the “Introduction” article of this issue (Indian J Psychol Med. 2026;48(1 suppl)).
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Author Channaveerachari Naveen Kumar is the Principal Investigator of this project and supplemental issue. The author did not take part in the peer review or decision-making process for this submission and has no further conflicts to declare.
Declaration Regarding the Use of Generative AI
The authors used OpenAI’s ChatGPT to assist with structuring the content and refining the manuscript’s language and readability. After using this tool/service, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
Ethical Approval
The study was approved by the Institutional Ethics Committee (IEC) (Approval No. NIMHANS/43rd IEC (BEH.SC.DIV) 2023, dated 8th December 2023) NIMHANS/EC(BH.SC.DIV.) MEETING/2024 dated 25th October 2024 and No. NIMHANS/EC(BEH.SC.DIV.) MEETING/2025 dated 1st July 2025) and registered with the Clinical Trial Registry of India (Registration No. CTRI/2024/02/062906).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: CSR Grants of a multinational company–project name: Multistate Digitally Driven Capacity-Building Program for Primary Mental Healthcare.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.