
Abstract
Background:
India has made significant strides in digital mental health capacity building over the past decade. This pan-India initiative was implemented through National Institute of Mental Health and Neurosciences (NIMHANS) to enhance the delivery of primary mental healthcare by digitally training medical officers (MOs), community health officers (CHOs), and field-level workers (FLWs) of India.
Methods:
Between October 2022 and June 2024, the program engaged MOs, CHOs, and FLWs of Karnataka, Maharashtra, Telangana, Uttarakhand, Bihar, Goa, Kerala, and West Bengal in a standardized six-week-district-wise digital training module curated to identify and manage commonly prevalent psychiatric disorders in primary care settings. Onsite training was conducted for participants in Tripura and Telangana. Participant engagement and changes in knowledge, attitude, and practice (KAP) scores were analyzed for each cadre along with ongoing support through real-time collaborative video consultations (CVCs).
Results:
The program engaged 42,192 participants (7248 MOs, 18,993 CHOs, and 15,951 FLWs) across nine Indian states. Overall, participants attending ≥50% of training revealed higher engagement in CHOs of Bihar (80.51%), followed by MOs of Goa (69.7%), followed by FLWs of West Bengal (64.57%). Paired t-test analysis of KAP scores showed post-training statistically significant (p < .05) improvement for MOs of Karnataka, Maharashtra, Telangana (onsite), and Goa; CHOs of Karnataka, Maharashtra, Telangana (onsite), Tripura (onsite) and Bihar; and FLWs of Karnataka, West Bengal, and Kerala. A total of 1,320 CVCs were conducted, assisting the management of psychiatric disorders in the community.
Conclusion:
Digital capacity building is a viable, scalable, and practical approach for mental health training of frontline workers to improve their clinical KAP.
Keywords
Digital capacity-building in mental health can deliver real, measurable benefits at scale, potentially enhancing provider knowledge, reducing stigma, and improving community mental health outcomes. Success hinges on strong governance, thoughtful incentivization, and coordinated implementation.Key Messages:
Mental health disorders are the second leading cause of disease burden in terms of years lived with disability (YLDs) and the sixth leading cause of disability-adjusted life years (DALYs) globally. Coupled with a 70–90% treatment gap in India, this situation presents a significant challenge for the country’s healthcare system.1,2 There is a scarcity of mental health professionals, compounded by stigma, which results in inadequate community outreach. Moreover, existing literature highlights the concept of the “functional treatment gap,” which lies in Indian primary care environments owing to the lack of knowledge for recognizing and treating prevalent mental health disorders in the community. 3 This can be addressed, in part, by fortifying the existing primary healthcare system to enhance early recognition and treatment, that is, capacity building. Hence, central and state governments have actively collaborated on various mental health capacity-building initiatives in the last decade, such as the integration of mental health in primary care by district mental health program, the “Atmiyata” program in Maharashtra, “Amma Manasu” (Mother’s mind) in Kerala, and “Manochaitanya” program by Karnataka state government.4–7 Some limitations of onsite training of primary healthcare workers are lack of scalable outreach, high costs, and inadequate human resources.
In this digital age, leveraging digital methods for capacity building appears feasible and advantageous due to their accessibility, cost-effectiveness, reduced need for human resources, and inherent flexibility. Several digital training initiatives are focusing on mental health capacity building in India, such as the National Institute of Mental Health and Neurosciences (NIMHANS) digital academy online courses, The Karnataka Telemedicine Mentoring and Monitoring Program (KTM), NIMHANS ECHO model, Project ESSENCE in Madhya Pradesh, Project EMPOWER in Gujarat and MINDS community mental health worker program.8–10 These digital training initiatives have substantially improved frontline workers’ knowledge, attitudes, and practices, helping to reduce stigma and the treatment gap.
Public–private partnerships (PPPs) are vital in transforming mental healthcare systems, particularly in addressing gaps in service delivery, access, and resources. In the mental health sector of developing countries, PPPs can drive innovation and improve outcomes by combining the strengths of both public and private sectors. Governments provide the policy framework, public health infrastructure, and outreach capacity, while private organizations contribute expertise, technology, funding, and efficiency. 21 This article examines the implementation and performance of a pioneering pan-India, digitally driven capacity-building program for primary mental healthcare conducted by National Institute of Mental Health and Neurosciences (NIMHANS) through funding from a multinational agency. As the first initiative in India, this program addresses the critical treatment gap in mental health through an innovative PPP model. This program aimed to empower primary care doctors/medical officers (MO), community health officers (CHO), and field-level workers (FLW) in nine Indian states. By training all three cadres within the community simultaneously, the program sought to enhance the early identification of psychiatric disorders and facilitate prompt treatment initiation by strengthening the hierarchical referral network in the community.
Methods
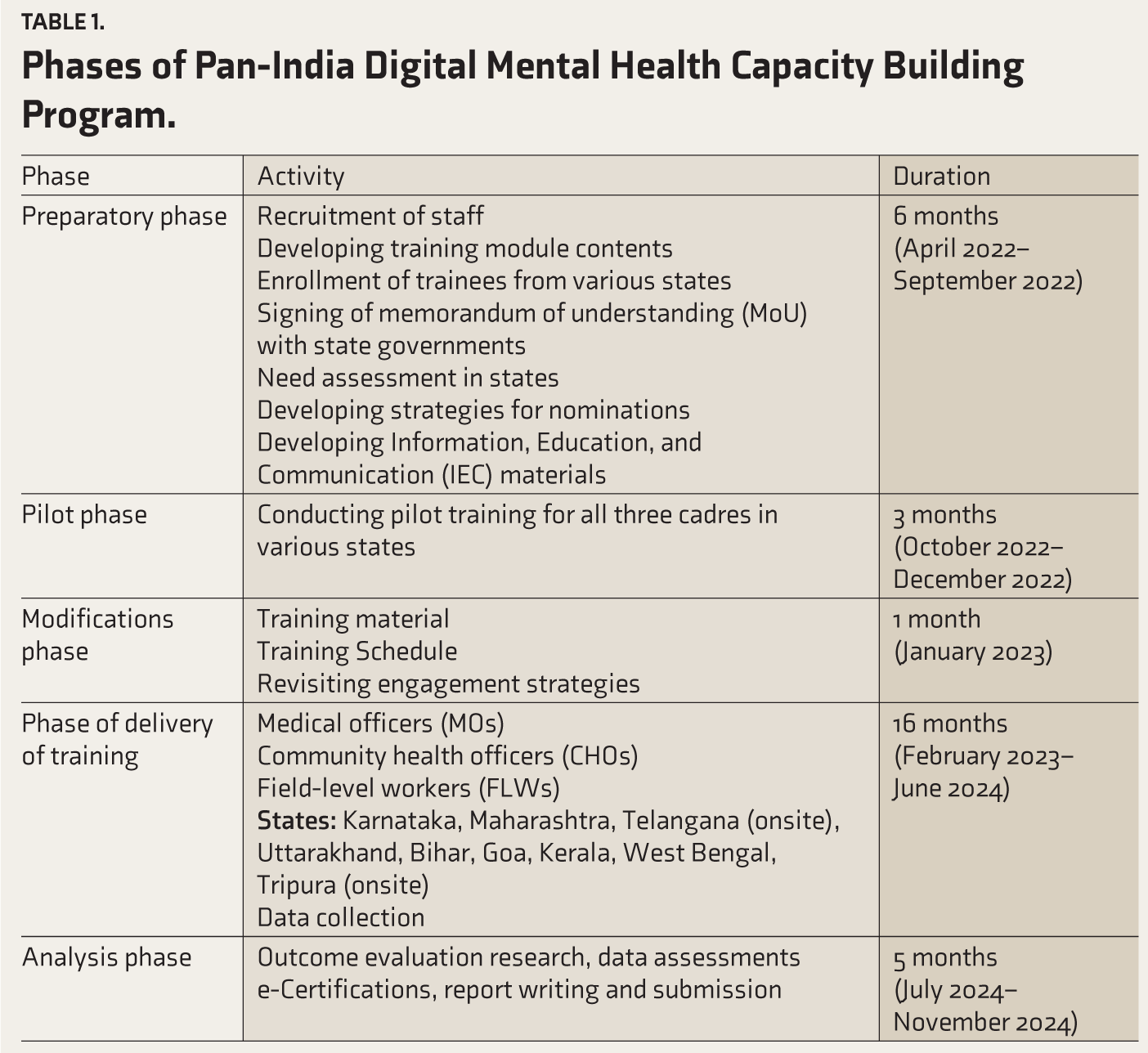
The program was initially conceived during the coronavirus disease 2019 (COVID-19) pandemic to equip frontline workers with the skills to address the emerging mental health morbidities in the general population. A memorandum of understanding (MoU) was signed between NIMHANS and the multinational funding agency for the program in March 2022. The program progressed as per the phases shown in Table 1. This digital training program was implemented by NIMHANS over the period from April 2022 to November 2024, encompassing various phases, as shown in Table 1. As the program progressed, this initiative engaged nine states across India in a time-bound manner (Table 1).
Phases of Pan-India Digital Mental Health Capacity Building Program.
Trainers
The trainers’ team consisted of nine psychiatrists, three clinical psychologists, three psychologists, two psychiatric social workers, two psychiatric nursing officers, and three medical social workers who were collectively involved in the development of training materials, information, education, and communication materials, conducting the training sessions, and providing follow-up support. Two IT professionals and seven project coordinators facilitated online training sessions and managed the data registry.
Training Module, Materials, and Schedule
Curated training modules were specifically developed for this project for the three cadres: MOs, CHOs, and FLWs. Training for CHOs and FLWs was conducted in local languages to enhance comprehension and participation, with materials developed in English and translated into Kannada, Marathi, Hindi, Malayalam, and Telugu. The MO training was conducted in English, which was observed to be a comfortable and appropriate medium. The online classroom teaching training included standardized PowerPoint presentations on introduction to mental health disorders, common mental health disorders (CMD), severe mental health disorders (SMD), substance use disorders (SUD), pandemic preparedness, and Tele-MANAS overview. The MOs’ training utilized Clinical Schedules for Primary Care Psychiatry: Version 2.4 (CSP 2.4), which is a point-of-care manual specifically designed for MOs by NIMHANS containing guidelines for screening, early diagnosis, referral, first-line prescription templates, and routine follow-ups of adult patients with psychiatric disorders at outpatient settings of primary health centers. 11 Mental Health Screening and Counselling Tool (MERIT) developed by NIMHANS containing categorical questions for effective mental health disorder screening was integrated into CHOs and FLWs’ modules. 12 The training schedule for MOs and CHOs comprised 120 minutes of weekly online sessions for six weeks, whereas for FLWs, it was for four weeks. Table 2 demonstrates the outline of a model session.
Receiving Nominations and Engagement Strategies
After signing MoU/equivalent written agreements with the respective state government health departments/agencies in the states of Karnataka, Maharashtra, Uttarakhand, Kerala, West Bengal, Goa, and Bihar, the district health administrators were approached by the team to obtain nominations of the consenting participants in all three cadres to schedule the online training (Figure 1). Communication and training materials distribution were handled via dedicated district-wise groups through a popular online messaging platform for seamless information sharing and continuous engagement. Additionally, Telangana MOs, CHOs, and Tripura CHOs were trained on-site at the request of the respective state governments. Participants were given access to specialists at NIMHANS for expert guidance in the screening and management process through instant collaborative video consultations (CVCs), available during working hours on all days, and audio consultations, accessible 24/7 for continuous support as needed. Through CVCs, trainees can seek instant video consultations with the tele-psychiatrist/clinical psychologist for real-time second opinions on patient diagnosis and treatment, also providing follow-up consultations for up to three months.13,14
Outlines of a Model Online Session of This Digital Program.
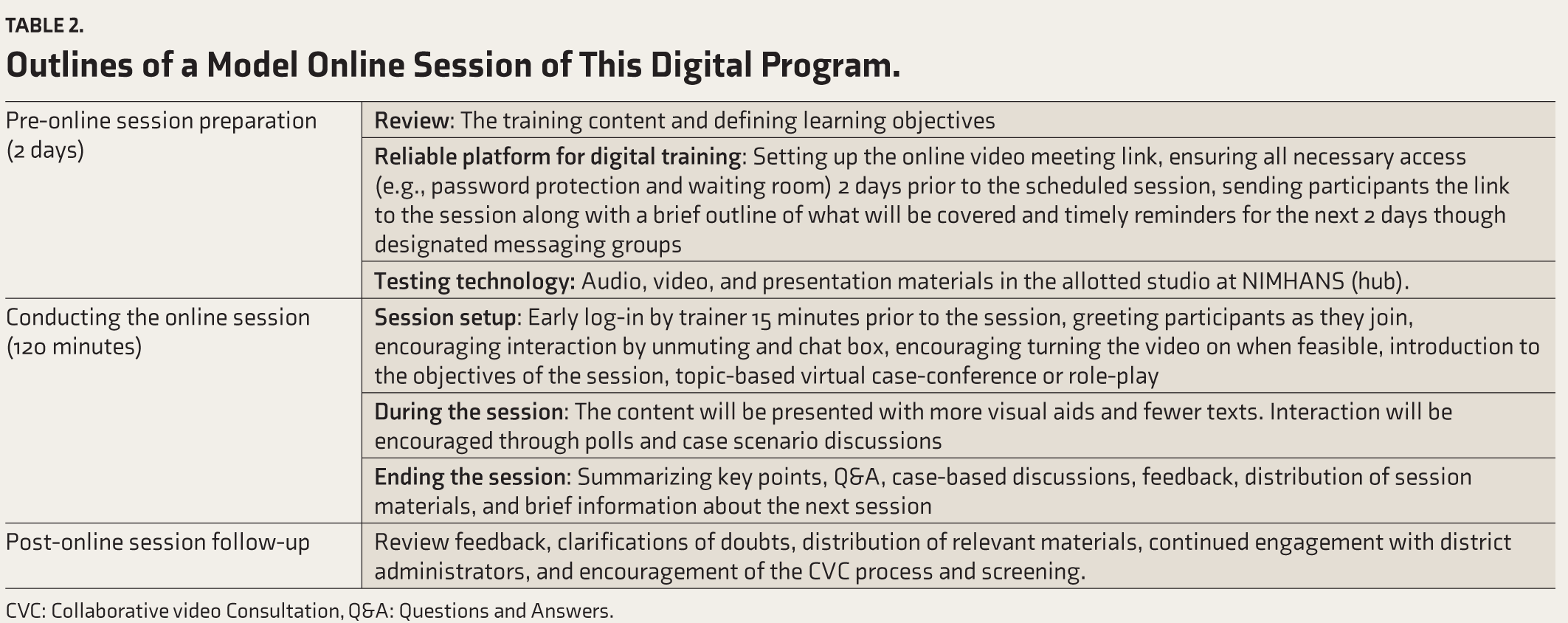
CVC: Collaborative video Consultation, Q&A: Questions and Answers.
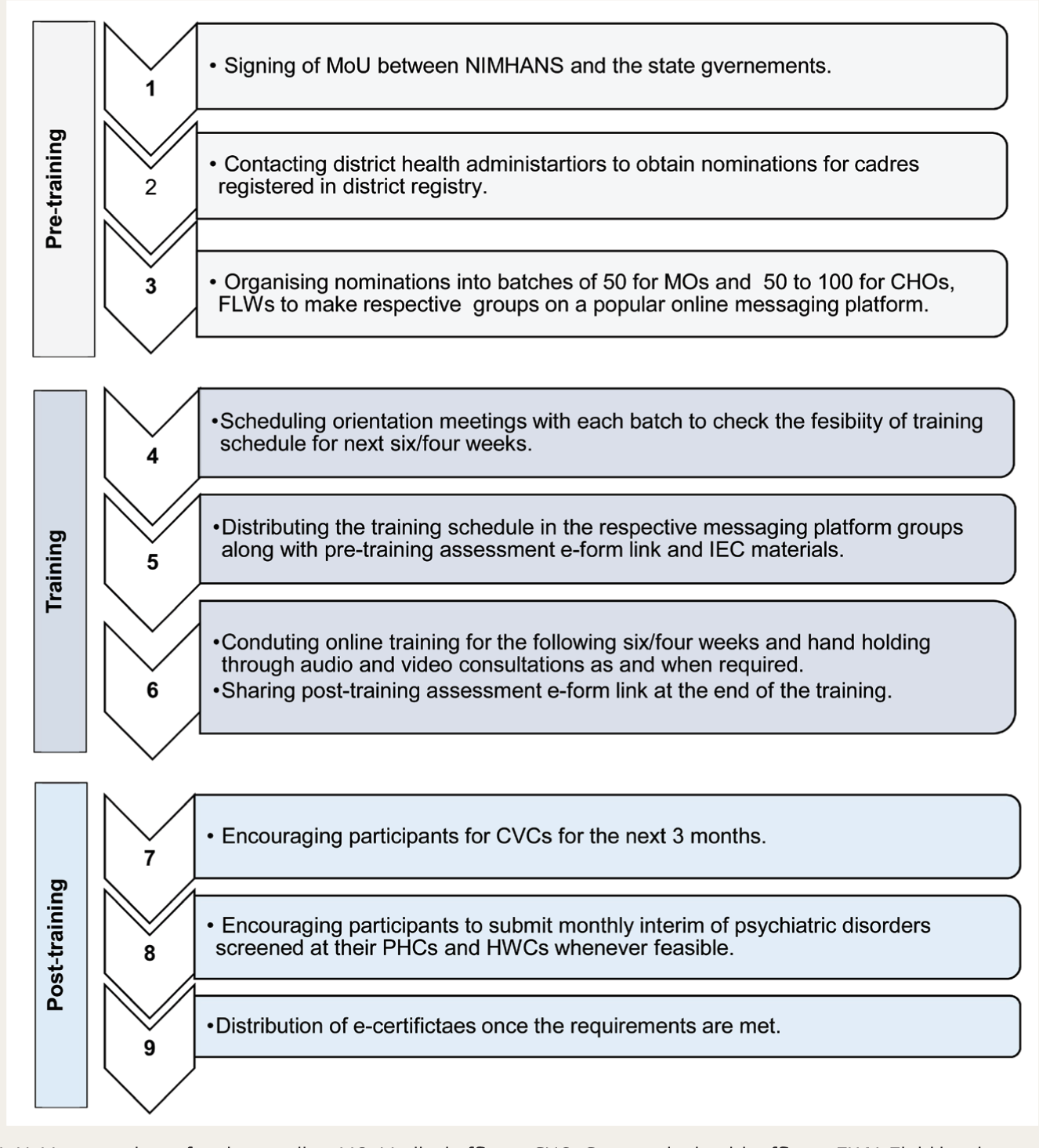
MoU: Memorandum of understanding, MO: Medical officers, CHO: Community health officers, FLW: Field level workers, CVC: Collaborative video consultations, PHC: Primary health center, HWC: Health and wellness center, IEC: Information, Education and Communication, NIMHANS: National Institute of Mental Health and Neurosciences.
Data Collection and Certification
Data was collected after obtaining informed verbal consent from all participants involved in digital training, assessment forms, and CVCs. Curated online forms (e-forms) were utilized for pre-training and post-training assessments of Knowledge, Attitude, and Practice (KAP) out of a total score of 28. Monthly, interim, and annual reports (of cases managed) were also utilized to track progress whenever feasible. Focused group discussions were conducted for different cadres in different states to understand the impact and challenges of the training. Training completion e-certificates were distributed after successful completion of training, that is, attendance in more than 80% of online sessions, completion of pre-and post-training assessments, and 1 CVC. Participation e-certificates were distributed to the remainder of the participants who failed to fulfill the earlier criteria. Descriptive impact stories and testimonials from a few district participants were collected post-training. A paired samples T-test was employed to assess the KAP scores before and after the training using licensed SPSS version 29. Only the participants’ scores who completed the pre- and post-KAP forms were analyzed. Institutional Ethics Committee approval was obtained for the same.
Outcome Evaluation
To study the impact and outcome of the program scientifically in MOs, a hybrid cluster randomized control trial was conducted after Institutional Ethics committee approval in the district of Tumkur, Karnataka.15–17
Results
This digitally driven mental healthcare capacity development program engaged a total of 42,192 participants across all three cadres in the states of Karnataka, Maharashtra, Telangana, Uttarakhand, Bihar, Goa, Kerala, West Bengal, and Tripura in 20 months (Figures 2 and 3).
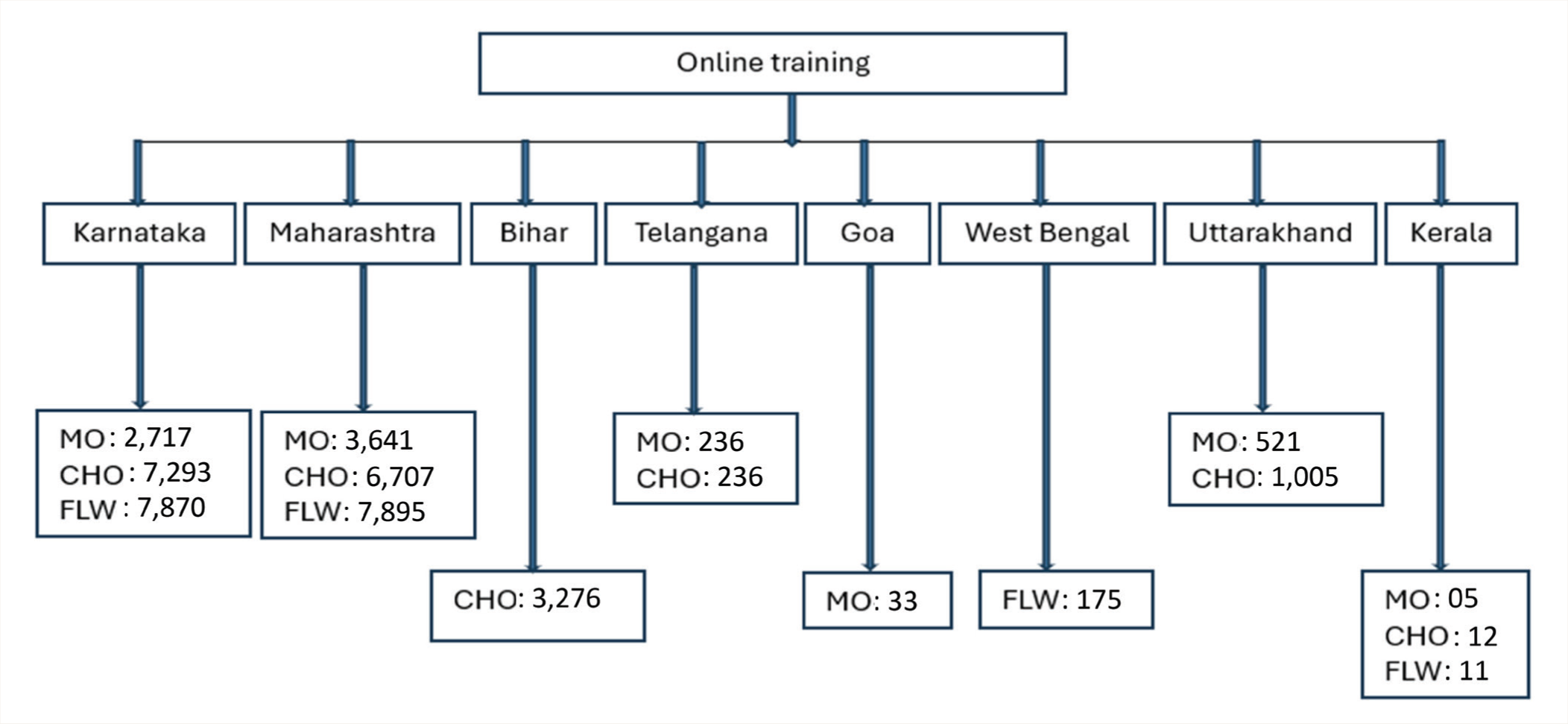
MO: Medical Officers, CHO: Community health officers, FLW: Field-level workers.
MO: Medical officers, CHO: Community health officers, FLW: Field-level workers.
Analysis of attendance during online and onsite training revealed the best and most consistent engagement during onsite training compared to online training, as predicted (Table 3). However, in digital training, Bihar CHOs (80.51%), Goa MOs (69.7%), and West Bengal FLWs (64.57%) showed better participant engagement compared to other states (Table 3).
Quantitative analysis was conducted on pre- and post-training KAP scores using paired samples t-tests for all three trained cadres in each state (Tables 4–6) with p <.05 was considered significant. Statistically significant improvements were observed in KAP assessment scores following online training for MOs in Karnataka, Maharashtra, Telangana(onsite) and Goa (Table 4); for CHOs in Karnataka, Maharashtra, Bihar, Telangana(onsite) and Tripura(onsite) (Table 5); for FLWs in Karnataka, West Bengal, and Kerala (Table 6).
The CVCs were integrated as a form of extended handholding during and three months post-training for all the cadres. One thousand one hundred seventy total CVC cases were discussed during the program. Table 7 summarizes CVCs received during the program from all three cadres identifying and managing psychiatric cases in primary care environments. The “Others” category includes non-CSP psychiatric diagnoses, cases that were not yet diagnosed, and non-psychiatry diagnoses. More details on CVCs can be found in separate articles in this supplement.18,19
Discussion
This digital capacity-building initiative effectively empowered 42,192 participants over nearly 20 months, significantly advancing mental healthcare delivery within India’s primary healthcare systems. The program’s implementation plan and evolving engagement strategies were instrumental in driving notable improvements in performance outcomes. Despite the challenges inherent in such a large-scale initiative, developing thoughtful and strategic solutions ensured the program’s objectives were successfully achieved amidst real-world implementation complexities.
Maintaining participants’ consistent engagement throughout the online training was the program’s most significant challenge. Various strategies were employed to improve attendance, contributing to sustained participation in several districts. These included pre-training orientation sessions to assess schedule feasibility and familiarize participants with the digital platform; repeated engagement with district administrators to promote attendance; timely reminders via online messaging groups; regular dissemination of IEC materials; continuous encouragement to attend training and complete CVCs; and interactive activities like virtual case conferences and role-plays at the start of training sessions. However, the effectiveness of these strategies fell short in districts where there was little to no engagement from the outset of the training.
The variations in attendance (Table 3) clearly emphasize that engagement is better ensured onsite than online training. The active monitoring support from the state government and district administration influenced participant engagement, which has been reflected in district-wise attendance variations within and across the states. Several factors contributing to the lower attendance in online training were identified, including limited administrative support, lack of incentivization or reinforcement, digital illiteracy, particularly among the FLW cadre, low participant motivation, poor internet connectivity, training during busy work hours, and overlapping online training sessions, especially within the MO cadre. These factors were highlighted in the focused group discussions with these cadres, as discussed in the articles by Shah et al. 20 and Pearala et al., 21 which also aligns with existing literature. 22 As per a systematic review of 19 qualitative studies on digital health interventions done by O’Connor et al., participant motivation remains one of the most significant factors influencing engagement. 23
It is noteworthy that attendance rates are comparatively higher for Bihar CHOs (80.51%) (Table 3) and Goa MOs (≈ 70%) in digital training, which emphasizes the role of strong administrative support. In several districts, such support contributed to high participant engagement. This included prompt responses from administrators, assistance with training schedules, brief yet impactful participation in orientation sessions, and continuous encouragement to meet certification criteria. Another reason for better engagement in Bihar CHOs in online training and Tripura CHOs in onsite training was the involvement of implementation partners working closely with state administrations. These partners facilitated IEC distribution, enhanced engagement, and ensured the smooth execution of training. 24 his underscores the critical role of local implementation partners in large-scale capacity-building programs. Another key finding from the program was that CHOs demonstrated higher engagement and significantly better post-assessment scores in online training compared to MOs and FLWs, indicating the CHO cadre’s greater feasibility and adaptability to digital formats.
State-wise Distribution of Participants in All Three Cadres with Attendance of ≥3 Online Sessions (≥ 50%) During the Training.
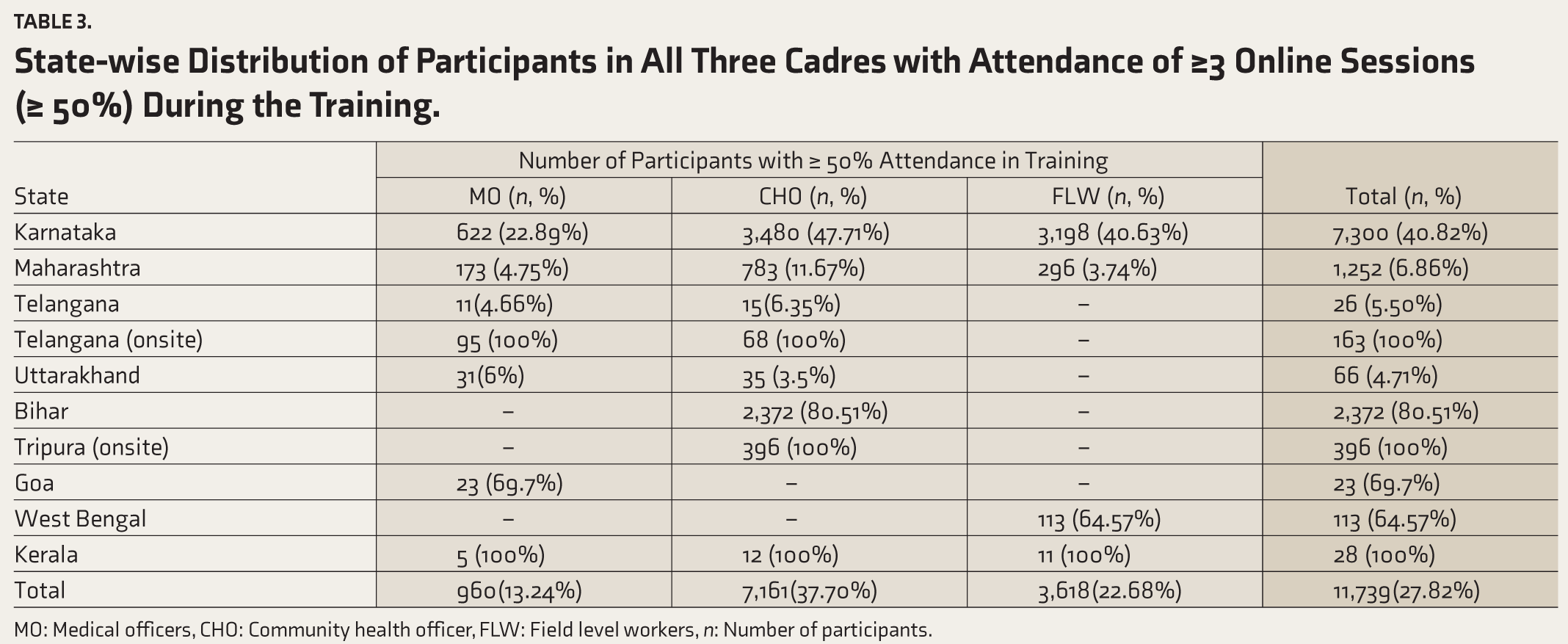
MO: Medical officers, CHO: Community health officer, FLW: Field level workers, n: Number of participants.
In our program, participants’ KAP scores demonstrated statistically significant improvement across all cadres following both online and onsite training in most states (Tables 4–6). Considering the large sample size, these findings will likely apply on a broader scale. This also replicates the existing evidence on the impact of digital training on frontline workers in mental health. 25 Despite consistent efforts to ensure uniform implementation of the training across all states, a few cadres in certain states did not show significant improvement in post-training KAP scores. Insights from focus group discussions with district-level cadres pointed to several contributing factors: poor network connectivity, limited digital literacy, and competing workload during training hours may have affected participants’ ability to engage with the content and retain information fully. Furthermore, irregular attendance and varying levels of personal interest may have influenced participants’ motivation to complete training assessments. The lack of substantial improvement in KAP scores for Kerala, Uttarakhand, and Telangana may be attributed to evidently lower engagement during the training (Table 3) and a limited number of participants (n < 20) submitting assessment forms from those states (Tables 4–6). Given that the training was conducted in the respective local language of each state, language was unlikely to have been a barrier or to have affected training outcomes.
Pre-and Post-training Analysis of KAP Score of MO Cadre.
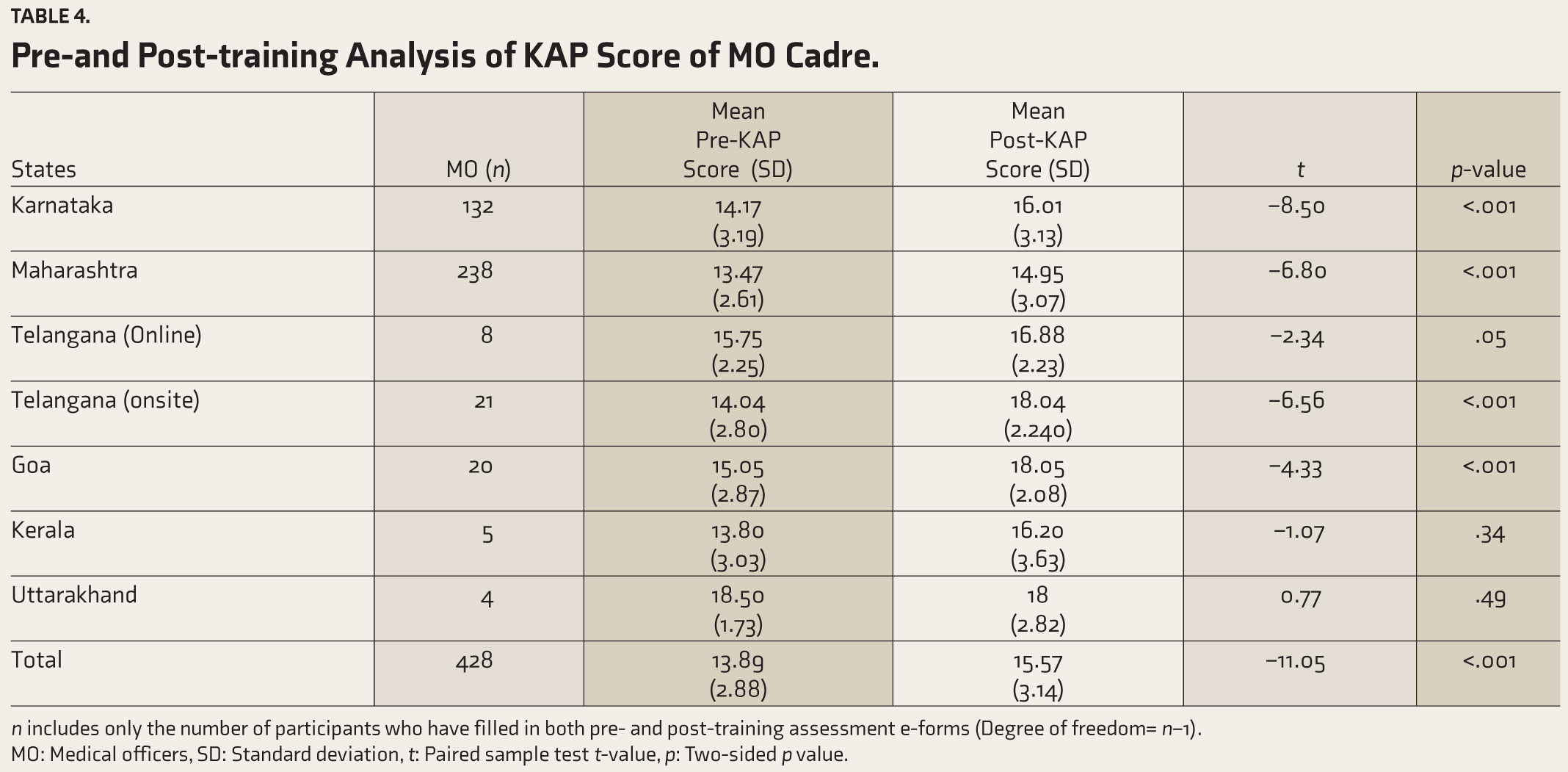
n- Includes only the number of participants who have filled in both pre and post training assessment e-forms, (Degree of freedom= n-1); MO- medical officers, SD- Standard deviation, t- paired sample test t-value, p- two-sided p value.
Pre-and post-training analysis of KAP scores for the CHOs cadre
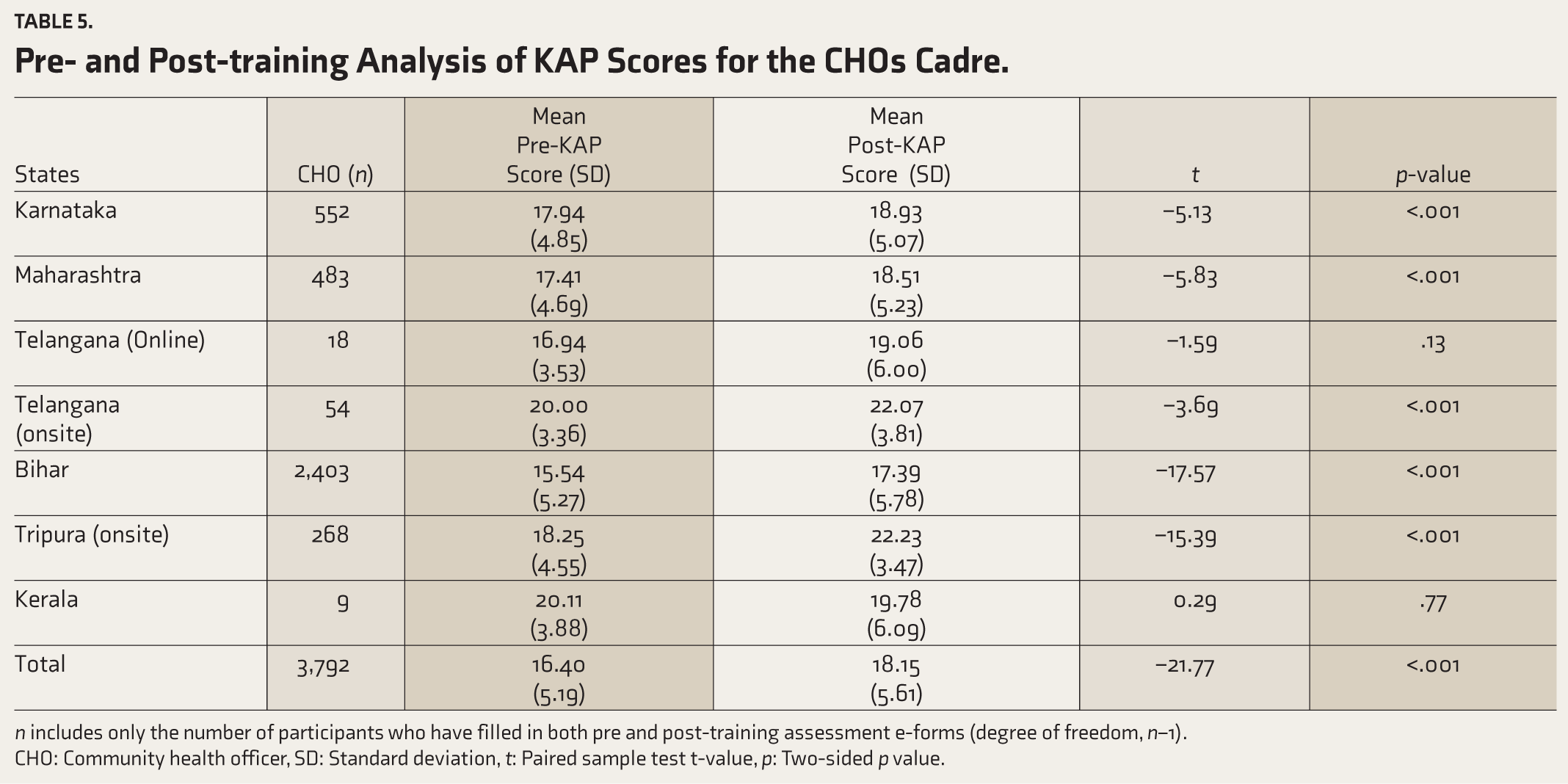
n- Includes only the number of participants who have filled in both pre and post training assessment e-forms, (Degree of freedom= n-1); CHO- community health officer, SD- Standard deviation, t- paired sample test t-value, p- two-sided p value.
Pre-and post-training analysis of KAP scoresforthe FLW cadre
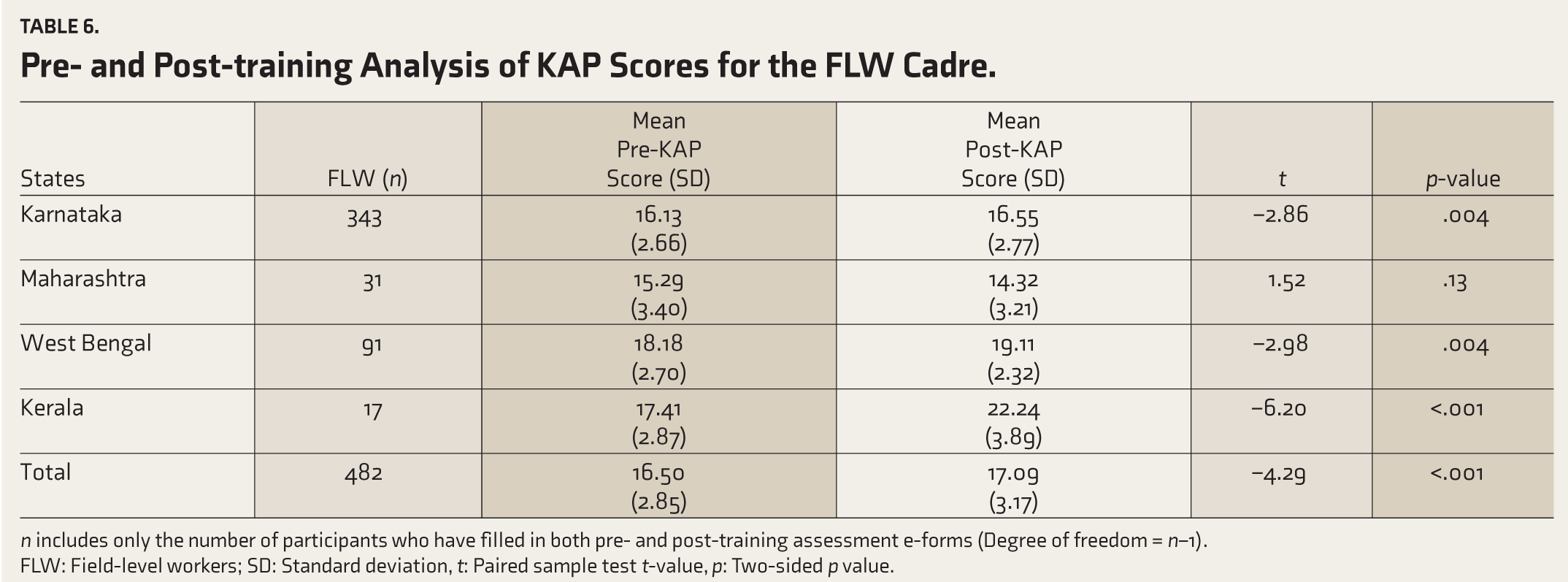
n- Includes only the number of participants who have filled in both pre and post training assessment e-forms, (Degree of freedom= n-1); FLW- field level workers, SD- Standard deviation, t- paired sample test t-value, p- two-sided p value.
Through ongoing support from CVCs, this program empowered trained frontline workers to manage 476 cases of CMDs, 219 cases of SMDs, and 200 cases of SUDs within the community (Table 7). It is important to clarify that instant CVCs were provided only for cases where the PCDs, CHOs, and FLWs had uncertainties regarding the diagnosis or management of the case. Therefore, the total number of CVCs does not reflect the cases handled during training. Sustained tracking of monthly reports remains a daunting challenge in our country, primarily due to the limitations of the existing public healthcare systems. Arguably, this area requires immediate strengthening, and “all-out” efforts should be dedicated considering the rapid developments in other domains of mental healthcare systems. Tracking the footfalls in out-patient clinics in primary care settings would be one of the sensitive indicators of the performance and success of a mental health program. To address this, digital technology should be utilized more effectively. 26 States like Chhattisgarh and Karnataka have set exemplary benchmarks in this regard, providing models that can be easily adapted by other states and Union Territories. 27 Returning to the topic of CVCs, they played a pivotal role in fostering collaboration between specialists and frontline workers following online mental health training. They provide real-time feedback on clinical applications and demonstrate the training program’s tangible impact. Continued CVC support also promoted post-training engagement.18,19 Additionally, CVCs offer a scalable and economically sustainable model for future mental healthcare delivery. 28
Summary of Collaborative Video Consultations During the Program.
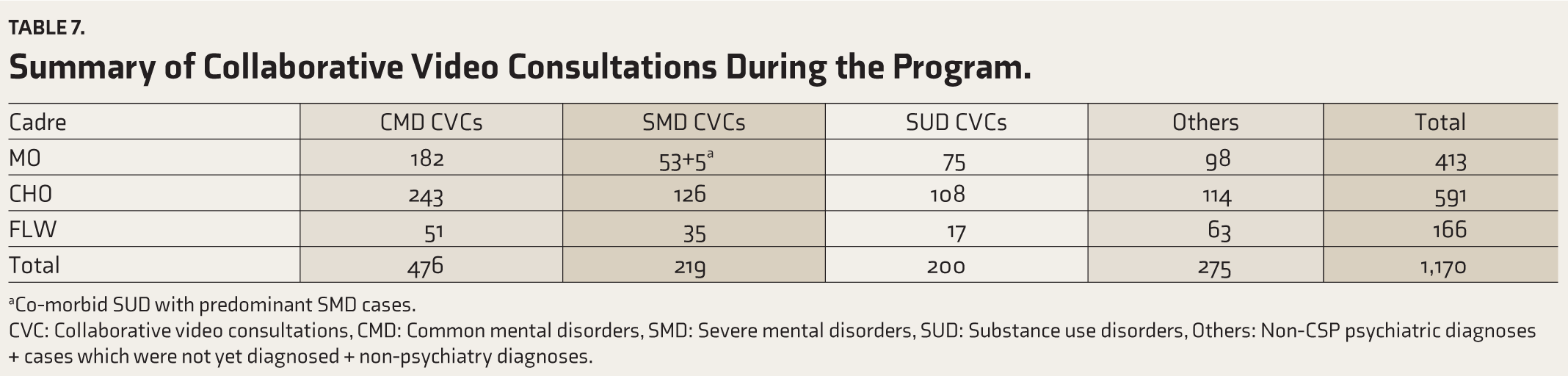
aCo-morbid SUD with predominant SMD cases.
CVC: Collaborative video consultations, CMD: Common mental disorders, SMD: Severe mental disorders, SUD: Substance use disorders, Others: Non-CSP psychiatric diagnoses + cases which were not yet diagnosed + non-psychiatry diagnoses.
Limitations
One limitation of this digital program was the absence of a structured incentivization plan for training participation. Although e-certificates initially boosted participation, this motivation waned over time. Designing an effective incentivization strategy for such a large-scale digital initiative necessitates the involvement of multiple stakeholders, which may not always be feasible in real-world scenarios. Nevertheless, when logistical challenges were effectively addressed on both ends, the program demonstrated successful participant engagement in digital training. This also calls for robust administrative strategies at the district level to enhance the feasibility of digital training, which would foster greater engagement. Another limitation of the implementation plan was the absence of an onsite training component, which, as evidenced by existing literature and our findings, could have increased participant engagement. However, incorporating onsite training for 42,192 participants would have compromised scalability, cost-effectiveness, and the overall duration of the program. Looking ahead, a hybrid training model that integrates the strengths of both in-person and online training would be ideal, maximizing engagement and enhancing the clinical translation of skills as adopted by the Chhattisgarh Community Mental Healthcare Tele-Mentoring Program (CHaMP) and Bihar primary care doctors blended training by NIMHANS.29–31
Conclusion
Viewing this digital capacity development program through a realistic lens allows for a practical, grounded assessment of its scalability and impact. It demonstrates that integrating digital technology is a viable approach to achieving meaningful outcomes in primary care in India. Digital training has significantly improved mental health knowledge and outcomes for the community, thereby reducing the treatment gap and decreasing stigma among patients, caregivers, and frontline care providers. It has also fostered healthier attitudes and practices in community mental health. Strong local administrative support, effective incentivization, and collaboration with implementation partners are key to successful large-scale digital mental health training rollout.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
Same as the “Introduction” article of this issue (Indian J Psychol Med. 2026;48(1 suppl)).
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Author Channaveerachari Naveen Kumar is the Principal Investigator of this project and supplemental issue. The author did not take part in the peer review or decision-making process for this submission and has no further conflicts to declare.
Declaration Regarding the Use of Generative AI
The authors utilized ChatGPT for only occasional writing assistance. After employing this tool, the authors carefully reviewed and edited the content as necessary and take full responsibility for the final publication.
Ethical Approval
The study was approved by the NIMHANS Institutional Ethics Committee (IEC) (Approval No. NIMHANS/43rd IEC (BEH.SC.DIV) 2023, dated 8th December 2023).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The pan India training program was funded by a multinational company's CSR grant.
Informed Consent
Informed consent from all participants to take part in the program and for publication was obtained.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.