
Abstract
Background:
Serotonin reuptake inhibitors (SSRIS) and cognitive behavior therapy (CBT), comprising exposure and response prevention (ERP), are the first line of treatment for obsessive compulsive disorders (OCD). However, many patients fail to achieve clinically significant symptom relief from traditional exposure-based therapies. This has led to research on strategies that can optimize the effects of ERP. Inhibitory learning theory (ILT) provides a novel foundation for understanding how exposure therapy reduces fear and has been mainly studied in the context of anxiety and phobia.
Novelty:
There is limited empirical data on applying the principles of IL, such as expectancy violation, variability, deepened extinction, labelling of affect, and removal of safety signals as mechanisms of extinction that can aid the achievement of favorable outcomes in OCD. In the absence of an existing manual, we describe the development of a novel IL-based ERP therapy intervention and the trial protocol to test its efficacy in patients with OCD.
Methods:
A quasi-experimental study design with baseline, post-treatment, and follow-up assessments will be adopted. The first phase of this study includes developing and validating an IL-based ERP intervention. A sample of 24 patients diagnosed with OCD will be recruited to receive IL-based ERP as part of the study. Measures of OCD symptom severity will be used to test efficacy.
Expected Outcome:
This study describes the development of an OCD-specific IL-based ERP intervention and an open-label trial to generate preliminary evidence for its utility in persons with OCD. The use of IL principles in ERP may potentially improve treatment outcomes for OCD.
Keywords
This is the study protocol for developing an IL-based ERP intervention and testing its efficacy in OCD, while also exploring key psychological factors, such as cognitive flexibility, psychological flexibility, and intolerance of uncertainty, which may predict therapeutic outcomes.Key Messages:
With a lifetime prevalence of 2%–3%, obsessive-compulsive disorder (OCD) is associated with significant impairment in functioning and reduced quality of life. 1 Cognitive behavior therapy (CBT), including exposure and response prevention (ERP), is the first-line psychological treatment of choice for OCD. 2 The mechanism underlying how ERP works has traditionally been based on the two-factor theory of learning 3 involves habituation, fear extinction, and emotional processing theory (EPT),4,5 which emphasize that long-term outcome in exposure therapy results from the initial activation of fear and prolonged exposure until habituation occurs. Yet, habituation alone does not reliably predict treatment outcomes.6–8 The main criticism of ERP is that a sizeable number of patients do not respond to treatment optimally (14%–31%), and among those who respond, nearly 50%–60% experience at least a partial return of fear (ROF) in follow-ups and about half of the patients endorse impairing residual symptoms. 9 The ROF 10 can occur through spontaneous recovery, renewal of conditional fear, and reinstatement of conditional fear, leading to a relapse.11,12 Obsessional fears may not be “unlearned” and may remain in memory and compete with newly learned nonthreat associations, suggesting the need for additional opportunities to enhance the long-term effects of exposure therapies to prepare for ROF. 13 Traditional exposure-based therapies may not provide clinically significant symptom relief in a substantial proportion of those with OCD, 14 possibly due to deficits in inhibitory learning (IL) and regulation. 15 Hence, there is a need to examine different ways of optimizing ERP-based CBT in OCD.
Optimizing IL as a core mechanism of extinction can enhance long-term outcomes in OCD. Inhibitory learning theory (ILT) explains the process of extinction.16,17 New nonthreat associations are formed during exposure, which inhibits the original threat association, but the memory is not erased or replaced. Instead, the conditioning stimuli (CS) become ambiguous, with two meanings that remain in memory and compete for retrieval.18,19 Exposure aims to inhibit the retrieval of older threat associations and to increase the retrieval of new nonthreat associations. 20
For instance, consider an individual with contamination obsessions, who avoids public washrooms due to the belief that doing so would result in severe illness or emotional collapse. An exposure task grounded in IL principles could involve entering a public restroom and remaining inside without engaging in safety behaviors. If the predicted outcomes (e.g., “I will feel like I can’t breathe and will have a breakdown”) do not occur, this experience would violate the individual’s threat-based expectancy. Over time, repeated and varied exposures across contexts (e.g., hospitals, schools, and public settings) may consolidate new, nonthreatening associations, making them more accessible and reducing the risk of fear renewal. This example highlights how expectancy violation and retrieval competition promote long-term change in IL-based exposure therapy.
Literature Review
Intervention strategies to enhance IL include expectancy violation, deepened extinction, contextual variability, removal of safety behaviors, and expanding the inter-session interval. In IL-based ERP, exposure tasks are created to violate expectancies regarding the frequency/intensity of aversive outcomes, immediate, long-term, and unknowable. 21 Deepened extinction, that is, combining multiple fear cues, reduces spontaneous recovery and reinstatement of fear. 22 Contextual variability, that is, practicing exposure under variable conditions, has more long-term benefits23,24 and varied phobic stimuli have resulted in better maintenance of treatment gains at follow-up.25,26 Safety cues prevent extinction learning 27 and preventing safety signals and behaviors improves outcomes. 28 Experimental studies suggest clinical strategies to optimize IL in exposure therapy for adults with anxiety disorders.29,30 These strategies can address certain limitations of the traditional ERP model. IL-based ERP aims for the longer-term extinction of fear by disconfirming threat-based expectations. 6
Additionally, understanding the factors that contribute to or predict learning in exposure therapy is important. Flexibility might be crucial for the exposure paradigm, especially with respect to willingness to experience, openness to change, and adaptation to new situations. Learning, especially through techniques like expectancy violation or variability, requires flexibility. Studies on cognitive flexibility in patients with OCD suggest deficits in executive functions,31,32 with a moderate effect size on inflexibility.33–35 Individuals with high cognitive and psychological flexibility may respond better to strategies presented in IL-based ERP tasks. Similarly, intolerance of uncertainty (IU) is a significant variable in threat extinction and safety associations, particularly in OCD. 36 Interventions such as ERP have shown lasting effects on reducing IU and OCD severity outcomes. 37 In the context of IL-based ERP, IU is highly relevant. Varying levels of fear hierarchy, stimuli, triggers, and a combination of cues will be presented during IL-based ERP. IU could be one of the factors that might play a role in how patients respond to IL-based techniques.
Novelty
Despite the robust evidence base supporting ERP as the first-line psychological treatment for OCD, a significant proportion of individuals experiences residual symptoms or relapse. Traditional models of ERP emphasize habituation, but recent literature points to the importance of optimizing IL mechanisms to enhance long-term outcomes.13,37 ILT suggests that the effectiveness of exposure therapy depends not on reducing fear in the moment, but on fostering new, nonthreat associations that compete with existing threat associations during future retrieval. While research on IL has advanced through analog and nonclinical studies, its application within clinical OCD populations remains limited. Preliminary case reports and experimental findings have shown promise, but there is a clear need for systematic translation of ILT principles into clinical interventions. Notably, there are no structured ERP interventions designed specifically to target IL processes in OCD. This study aims to fill this research gap by developing and testing an IL-based ERP intervention tailored for OCD. This study outlines the study protocol used for intervention development and evaluating its efficacy in a clinical sample.
Objectives
The primary objective of the study is to develop an IL-based ERP intervention for patients with OCD and to examine its efficacy in reducing symptoms of OCD. The study’s secondary objectives are to examine the efficacy of IL-based ERP in reducing depression, anxiety symptoms, and avoidance. Additionally, the study will also examine the role of cognitive flexibility, psychological flexibility, and IU as predictors of treatment outcomes.
We hypothesize that there will be a significant reduction in symptom severity (measured by the Yale-Brown Obsessive-Compulsive Severity Scale (YBOCS) post-treatment and at follow-up. We also expect a significant reduction in the severity of anxiety, depression, and avoidance following the intervention, and that cognitive flexibility, psychological flexibility, and IU will be significant predictors of treatment outcome.
Methodology
The study will be conducted in two phases: the intervention development phase and the main phase.
Phase 1: Development and validation of the intervention
Phase 1 focused on developing a therapeutic intervention for IL-based ERP for patients with OCD. Intervention development followed the six essential steps of quality intervention development (6SQuID). 38
The first step included defining and understanding the concerns and limitations of the existing ERP strategies. The literature review indicated that despite the evidence to support the efficacy of CBT for OCD incorporating ERP, nearly 14%–31% remain nonresponders, 9 and even responders often experience relapse.5,6 Fear can reappear due to spontaneous recovery, renewal, or reinstatement of fear associations. 10
The second step included clarifying which causal or contextual factors are malleable and have the greatest scope for change. Literature on ERP indicates the availability of additional strategies that could be adopted to optimize ERP. While research on IL mechanisms in OCD is limited, existing case studies and nonclinical research support the efficacy of IL and its various techniques.
The third and fourth steps included identifying the change mechanism and how to deliver it subsequently. IL theory has been used as the theoretical principle for developing the intervention. IL-based strategies have been identified, and an intervention has been developed. A preliminary draft of the intervention was prepared and refined in consultation with the coauthors, who have expertise in CBT for OCD and anxiety disorders.
Validation of the Intervention
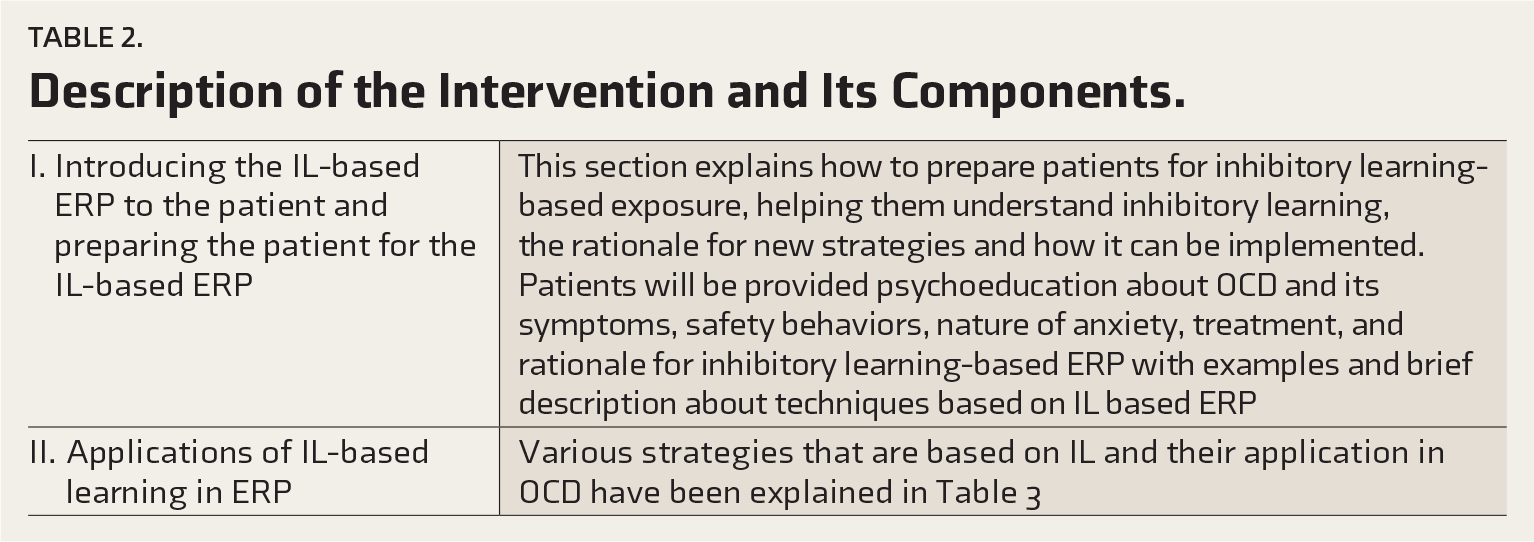
In the second round of consultation, five experts from the field of IL, OCD, and ERP were identified and consented to review the intervention. Four subject experts validated the intervention on a 5-point Likert scale for structure and length, clarity, applicability, relevance, and suitability of techniques based on IL. Changes were made based on the experts’ feedback and ratings. Suggestions by subject experts included simplifying psychoeducation using more examples suited to the cultural context of patients, including a post-briefing exposure, providing a rationale for the strategies, planning suitable homework tasks using worksheets and self-monitoring, and increasing the number of sessions, with a range of 17–20 sessions. Following this, the intervention was finalized (see Table 2 for final components).
Phase 2: Testing the efficacy of IL-based ERP therapy in patients with OCD.
This step will include gathering evidence for effectiveness to proceed to a rigorous evaluation. This step will be carried out to examine the efficacy of IL-based ERP in a sample of 24 patients with OCD, which will be done in phase 2 of the study.
Study Design
A quasi-experimental study design with baseline, post-treatment, and follow-up assessments will be adopted.
Study Participants and Setting
A sample of 24 consecutive patients with a primary diagnosis of OCD (Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, DSM-5) 49 who fulfil the study criteria and provide informed consent will be recruited from a specialty clinic for OCD and the clinical services of a tertiary mental health setting. The inclusion criteria are a primary diagnosis of OCD as per DSM-5, age between 18 years–50 years, from all genders, minimum education of Grade VII, a Y-BOCS score of ≥16, and being stabilized on medication, defined as no change in type or dosage for at least eight weeks prior to study entry and remaining stable throughout the course of the intervention. Patients with a history suggestive of organicity, schizophrenia, psychosis, schizoaffective disorder, bipolar disorder, current substance dependence (except nicotine), or clinical evidence of intellectual disability will be excluded. Patients who have undergone more than six sessions of structured CBT with ERP, mindfulness-based CBT, or metacognitive therapy in the past three months will also be excluded.
Sample Size Calculation
Assuming a power of 0.95, with an alpha value of 0.006 for an effect size f = 0.5 and an expected attrition rate of 20%, to evaluate the effect of treatment for repeated measures, a sample size of 24 is estimated. The limited number of earlier studies that compared the treatment with conventional methods reported high effect sizes (0.8–1.1) for between-subjects comparisons. We propose a sample size based on a slightly conservative effect size estimate compared to the previously reported values, given the lack of well-conducted studies using this treatment method in OCD.
Therapist Competence and Treatment Fidelity
IL-based ERP will be delivered by the first author, a qualified clinical psychologist with five years of clinical experience, following a master’s degree in clinical psychology and the practice of CBT and, in particular, ERP. Treatment fidelity will be ensured through regular case supervision from senior clinical psychologists and psychiatrists. Approximately 10% of the audio recordings of sessions, selected randomly, will be rated by independent raters using a fidelity checklist. Informed consent will be obtained from patients for audio recording of sessions. The fidelity checklist will be prepared during phase 2 of the study.
Implementation Plan
During the main phase, 24 patients with a primary diagnosis of OCD based on DSM-5 meeting specified study criteria will be recruited from a tertiary hospital outpatient and inpatient clinical services, OCD clinic, and therapy unit. Patients meeting specified study criteria will be recruited, following their consent to participate, and baseline assessments will be completed. The intervention will be delivered individually by the first author in person. Baseline, post, and follow-up assessments on primary and secondary assessments will be conducted, and the primary outcome assessment, YBOCS rating, will be conducted by an independent rater (Table 1). Weekly assessments on YBOCS will be carried out to assess symptom severity. The participant flow is depicted in Figure 1.
Measures Used in the Study.
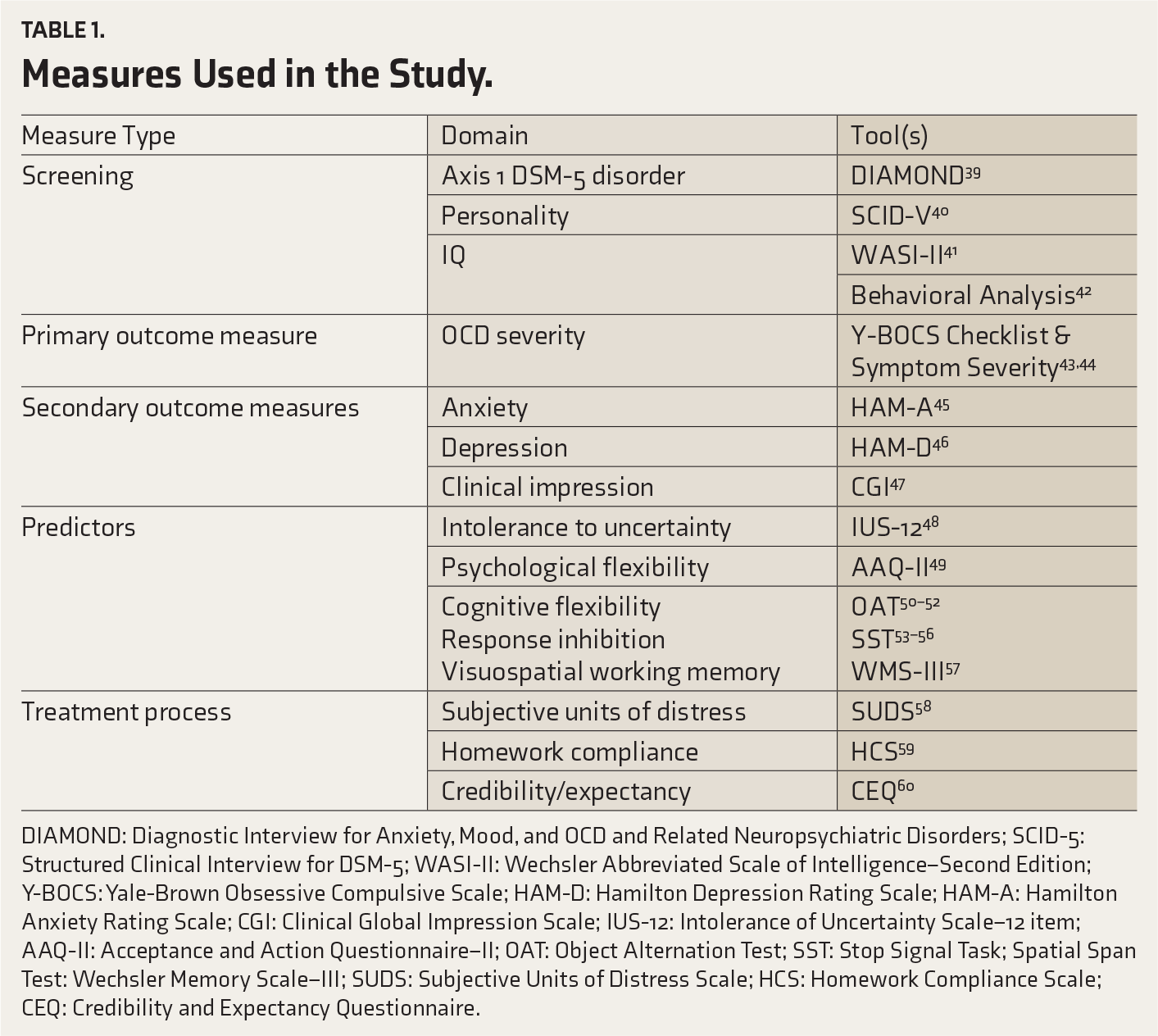
DIAMOND: Diagnostic Interview for Anxiety, Mood, and OCD and Related Neuropsychiatric Disorders; SCID-5: Structured Clinical Interview for DSM-5; WASI-II: Wechsler Abbreviated Scale of Intelligence–Second Edition; Y-BOCS: Yale-Brown Obsessive Compulsive Scale; HAM-D: Hamilton Depression Rating Scale; HAM-A: Hamilton Anxiety Rating Scale; CGI: Clinical Global Impression Scale; IUS-12: Intolerance of Uncertainty Scale–12 item; AAQ-II: Acceptance and Action Questionnaire–II; OAT: Object Alternation Test; SST: Stop Signal Task; Spatial Span Test: Wechsler Memory Scale–III; SUDS: Subjective Units of Distress Scale; HCS: Homework Compliance Scale; CEQ: Credibility and Expectancy Questionnaire.
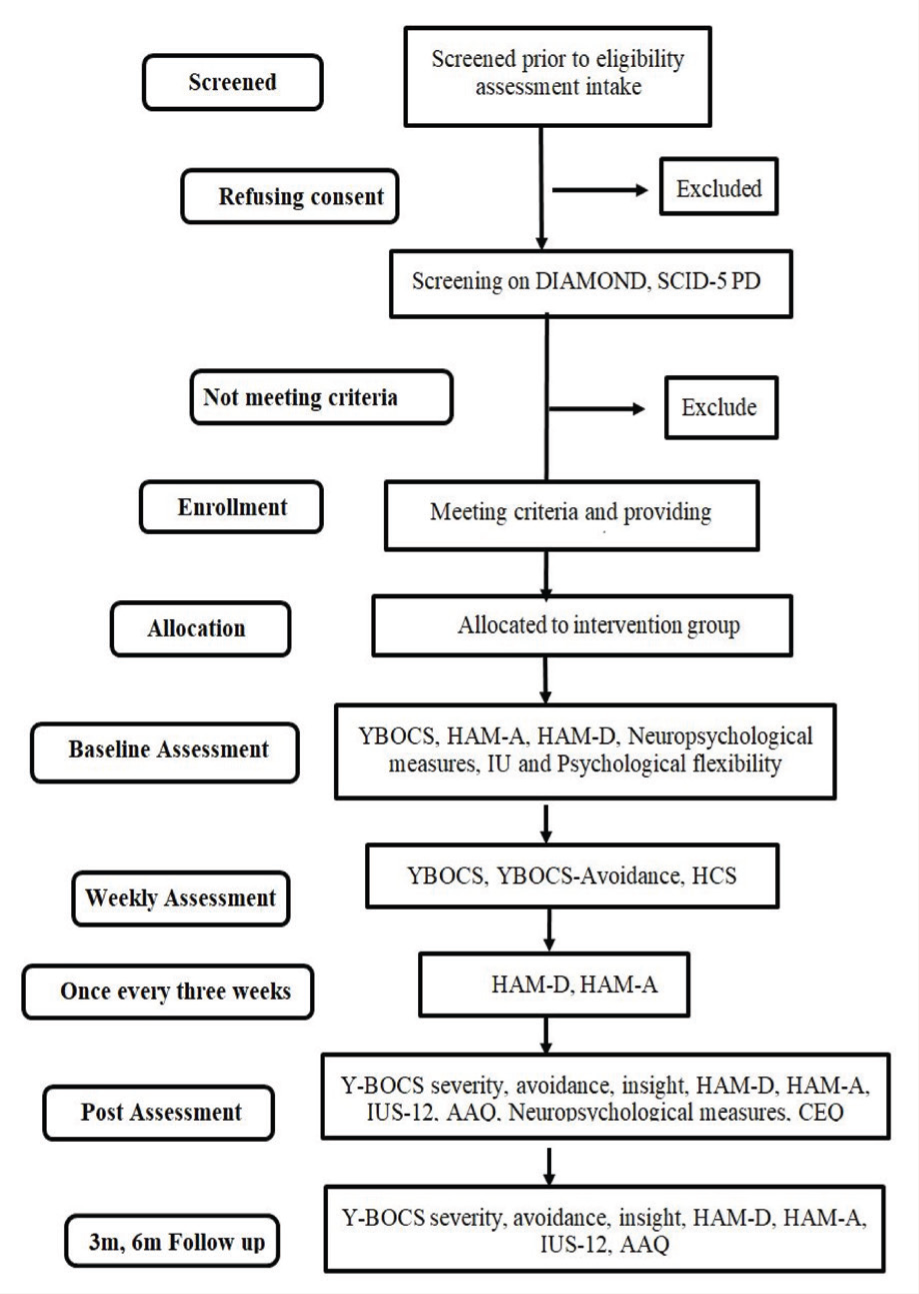
DIAMOND: Diagnostic Interview for Anxiety, Mood, and OCD and Related Neuropsychiatric Disorders; SCID-5 PD: Structured Clinical Interview for DSM-5 Personality Disorders; Y-BOCS: Yale-Brown Obsessive Compulsive Scale; HAM-D: Hamilton Depression Rating Scale; HAM-A: Hamilton Anxiety Rating Scale; IUS-12: Intolerance of Uncertainty Scale–12 item; AAQ: Acceptance and Action Questionnaire; CEO: Credibility and Expectancy Questionnaire; 3M: 3-month follow-up; 6M: 6-month follow-up.
Ethics Review
The study has been approved by the Institute Ethics Committee (NIMH/DO/BEH.Sc. Div/2021-22) and is registered with the Indian Council of Medical Research (ICMR) clinical trials registry (CTRI/2022/06/043229). Written informed consent will be sought from all participants, and all participants will be briefed about the study and their participation.
Data Analysis
Repeated measures analysis of variance (ANOVA) will be used to assess change across assessment time points. The effect size will be calculated for the completers’ sample. Regression analysis will be carried out to examine predictors of outcome (score on YBOCS). Scores on compliance with homework, IU, cognitive flexibility, and psychological flexibility will be examined as predictor variables. Clinical significance will be calculated using the Jacobson Truax method. 63
Timelines
The study protocol was developed, and institutional ethics approval was obtained between January and February 2021. Phase 1, which involved the development of therapeutic intervention and pilot testing, was conducted from March 2022 to March 2023. The main phase of the study, focusing on data collection, began in April 2023 and is ongoing until February 2025. Data analysis is scheduled to take place from March to June 2025.
The Intervention
The intervention is designed to be delivered over 17–20 weekly or biweekly individual sessions, with a longer duration of exposure (60 minutes–90 minutes). An exit interview will be conducted to understand the patient’s feedback on the intervention. Worksheets for self-monitoring and expectancy violation will be recommended to ensure between-session practice and learning.
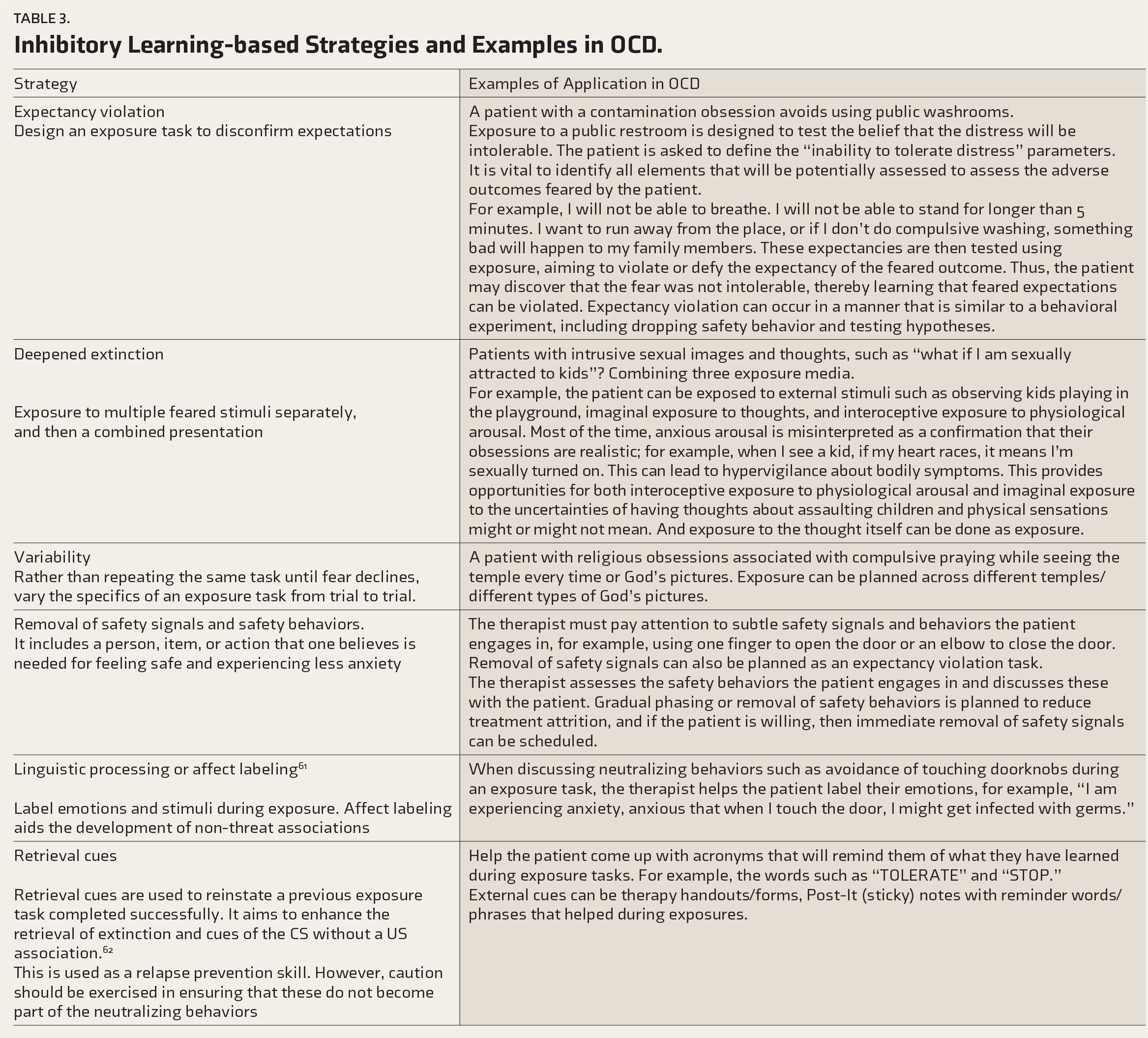
The description of the intervention and its components, as well as the strategies and selection of strategies and techniques, are provided in Tables 2 and 3, respectively. Further details of IL-based strategies, with examples applicable to OCD, are provided in Table 3.
Description of the Intervention and Its Components.
Inhibitory Learning-based Strategies and Examples in OCD.
Discussion
In this study, we describe a study protocol that includes the development of a the rapeutic intervention of IL-based ERP for patients with OCD and testing the efficacy of the IL-based ERP intervention in reducing symptoms of OCD. Conceptualizing exposure therapy by facilitating IL would help develop competing, nonthreat associations, enhancing the retrieval of new learning over time and across various contexts and aiding the generalization of learning beyond the clinical situation. While there is considerable research on IL-based exposure strategies in anxiety disorders, there is little empirical data on OCD. Therefore, in the absence of a systematic approach to incorporating IL-based principles in OCD, this study will contribute to a small but growing body of evidence on the application of IL-based exposure therapy, specifically in OCD. In addition, the study will provide an understanding of the role of cognitive and psychological flexibility and IU within a learning paradigm. For example, greater IU can interfere with strategies in IL-based exposure as the fear levels will be faced in random order, and possibly, individuals with better cognitive flexibility and psychological flexibility might show better treatment outcomes.
Expected Limitations and Strengths
The study is also likely to provide information on some of the challenges in implementing IL-based techniques in OCD, including how patients receive and tolerate treatment and which symptom dimensions would respond better to this approach of ERP. However, a significant limitation of the protocol is that this is an open-label design. Future studies should test the efficacy of IL-based exposure in patients with OCD using more robust research designs and larger samples.
Expected Outcomes
Using IL principles in ERP may potentially improve treatment outcomes for OCD. The IL-based ERP intervention is expected to demonstrate significant efficacy in reducing the severity of OCD symptoms, as measured by YBOCS. Additionally, it is anticipated that the intervention will lead to improvements in secondary outcomes, such as reductions in depression, anxiety, and avoidance behaviors. The study also explores how cognitive flexibility, psychological flexibility, and IU predict treatment outcomes. It is expected that greater psychological and cognitive flexibility and lower IU will be associated with better treatment efficacy, further supporting these factors as potential mediators of therapeutic change.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
The authors acknowledge the contributions of Vasundhra Teotia, Clinical Post-Doctoral Fellow at the Centre for Brain and Mind, NIMHANS.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
Grammarly, an artificial intelligence (AI)-based writing tool, was used to assist in grammar checking, spelling corrections, and improving the manuscript’s clarity. The authors assume full responsibility for the entire manuscript content, including the parts refined with the assistance of Grammarly.
Ethical Approval
The study has been approved by the Institute Ethics Committee and is registered with the Indian Council of Medical Research (ICMR) clinical trials registry (CTRI/2022/06/043229).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.