
Abstract
Background:
Individuals with bipolar disorder (BD) experience considerable difficulty in functioning during remission as well. The actual lived experience of individuals with BD with respect to their functioning is not understood in the cultural context.
Methods:
A qualitative approach in the form of interviews was taken from 11 participants who were diagnosed with BD in remission from a tertiary care hospital. The interviews were audio recorded and coded. Thematic analysis was carried out using a grounded theory approach to bring out relevant themes surrounding their inter-episodic functional limitations.
Results:
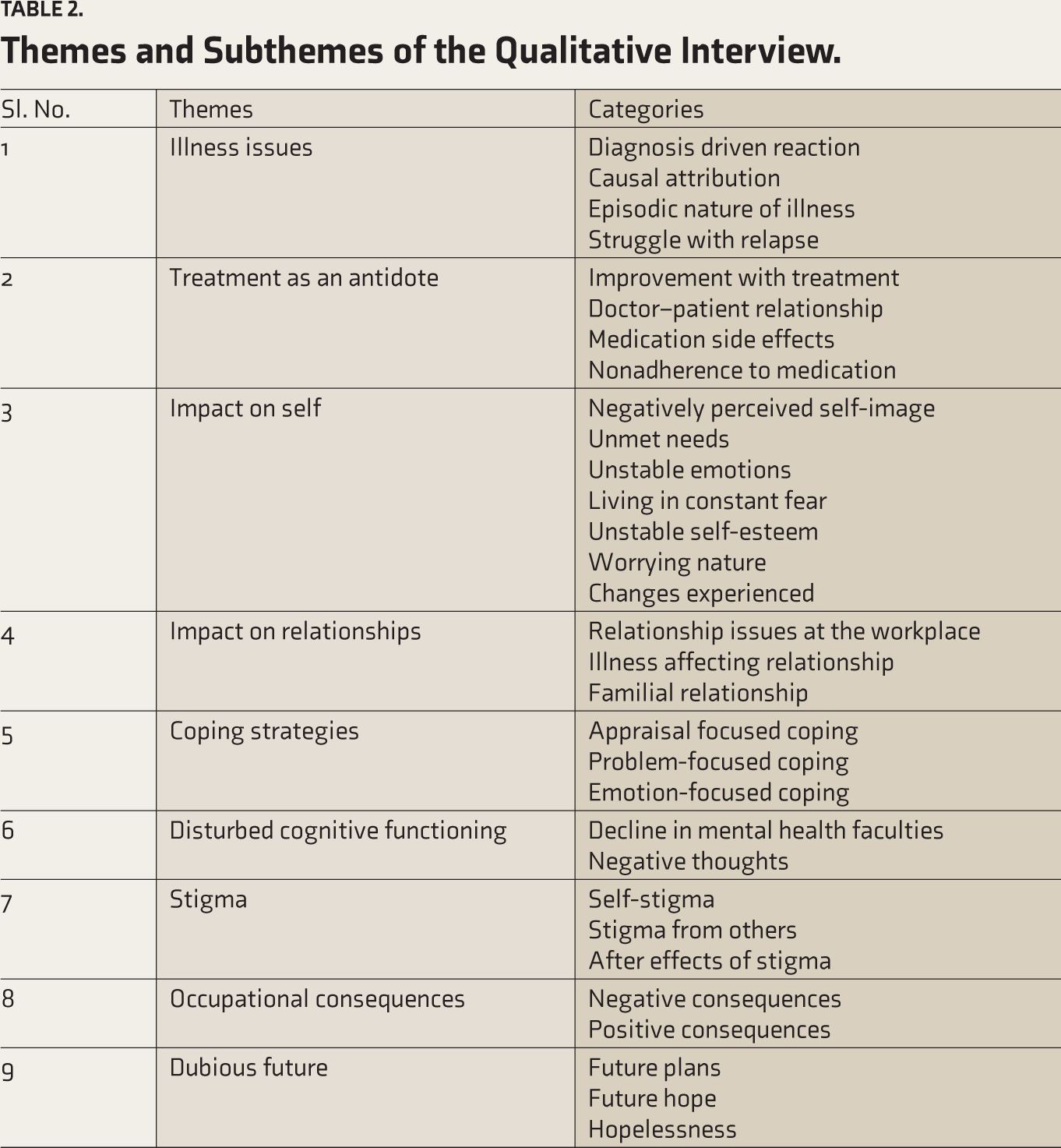
The thematic analysis resulted in nine themes associated with the functioning, namely illness issues, treatment as an antidote, impact on self, relationship issues, coping strategies, disturbed cognitive functioning, stigma, occupational consequences, and dubious future.
Conclusions:
The qualitative interview analysis provides a comprehensive picture of the experiences undergone by patients with BD. The themes and the sub-themes that came up in the analysis are reflective of the experiences of these individuals. The findings of the study can be utilized in planning effective interventions for remitted patients in the future so that functional limitations can be effectively addressed.
Even in remission, individuals with BD experience disturbances in self-image, relationships, and functioning. Past episodes have a lasting effect on self-confidence, self-stigma, and social interactions. Negative thinking patterns and the use of emotional coping strategies are commonly reported.Key Messages:
The percentage of total disability-adjusted life years, a measure of the burden of disease due to bipolar disorder (BD) in India, is 6.9%, which is considerably high and reveals the burden because of BD. 1 Multiple recurrences and incomplete remission result in functional impairment in many patients with BD.2–3 Despite the clinical focus on acute episodes, the periods of remission are crucial yet understudied, where patients navigate the complexities of maintaining stability and preventing relapse. The factors associated with functional outcomes vary from study to study and have been difficult to replicate because of different methodologies and the use of other measures to assess functional outcomes. A meta-synthesis of 24 qualitative studies revealed that diagnosis, loss, uncertainty, threat, relationships, stigma, and fear of relapse were distressing elements in BD. 4 Patients with BD in the Indian context were found to have a different profile with respect to the symptoms and clinical course, psychosocial functioning, comorbid rapid cycling affective disorder/seasonal affective disorder, suicidal behavior and the treatment received in the form of mood stabilizers, antidepressants, and electroconvulsive therapy (ECT). 5
Most studies have focused on the quantitative aspects of functional recovery using various psychometric tools. Although quantitative studies provide information regarding functioning, there seem to be several personal and cultural factors that might influence inter-episodic functioning. To understand these individual unique factors, an in-depth interview would be a better approach. The qualitative findings throw light on the fact that living with BD is never an easy task. Poor understanding in society, shortcomings of the health care system, and inefficient involvement of the caregivers in the treatment, discontinuation of treatment (medical and psychological) seem to worsen the social, interpersonal, and economic costs of BD. 6 Women with BD reported negative illness consequences because of stigma, loss of self-determination/feeling powerless, and changes to relationships (being victimized, power imbalance, dependence). They reported using certain strategies to cope with illness, such as focusing on children, seeking social support, seeking help from professionals, and trying to be normal. 7 One study showed that BD seems to impact self and identity development because it tends to cause confused experiences, contradictions, and self-doubt, which could cumulatively affect the proper sense of self. People with BD often face disruption and discontinuity and external definitions of self-based on their illness. 8
The qualitative literature thus can provide important contextual, individual, and illness-related factors that contribute to functioning during remission. Therefore, it helps to develop an individual’s stay-well plan based on the difficulties experienced, facilitating a sense of personal agency through strategies to manage the symptoms, address social stigma, and promote active involvement in treatment. However, very few qualitative research studies have been conducted in India to describe patients’ experiences of how the disorder impacts their quality of life, personal life and relationships, self-esteem, and acceptance. Hence, this study employs a grounded theory approach to delve into the experiential accounts of individuals with BD in remission to understand the nuanced ways these individuals manage their condition and maintain functionality during remission.
Method
The study aimed at an in-depth exploration of the subjective experiences of individuals diagnosed with BD who are currently in remission. For this purpose, a qualitative research design of grounded theory with a thematic analysis approach was adopted. Ethical clearance for the study was obtained from Institute Ethics Committee.
Subjects
The participants (n = 11 complete interviews out of 14) were selected from 150 patients who were part of a quantitative study carried out by the authors. For the quantitative research, those with a primary diagnosis of bipolar affective disorder in remission as per International Classification of Diseases-10 (ICD-10) criteria F 31.7, within an age range of 18–50 years and who scored 7 or less on both the Hamilton Depression Rating Scale 9 and the Young Mania Rating Scale 10 were included. Patients with a history of organic and neurological illness or having a primary diagnosis of a unipolar disorder and other psychotic disorders or mental retardation were excluded from the study. Among the 150 participants, a subsample was selected based on their availability (convenience sampling), consent for recording the interview, proficiency in English, and ability to describe their experiences. Fourteen interviews were carried out; however, due to incomplete interviews and poor content, three were discarded. The interviews were continued till theme saturation and on a first-come, first-served basis.
The qualitative study was carried out in the form of face-to-face interviews where patient’s narration about their experiences after having the illness was recorded. The data collection was done from September 2013 to March 2014 in a tertiary care hospital setting. The researcher developed the semi-structured interview schedule based on a literature review. The prepared semi-structured interview schedule was validated by three mental health professionals with at least 12 years of experience in this field. Their suggestions were incorporated, and the experts approved the modified schedule. The sociodemographic details were recorded before initiating the interview. The semi-structured interview schedule consisted of 15 open-ended questions focusing on specific areas like their understanding of the BD, stigma, personal and family adjustment, and functioning concerning personal, occupational, societal, and family roles. All the interviews were carried out by the first author with the patient alone and were audio recorded. The duration of these interviews ranged from two to three hours, and they were conducted in one sitting with breaks when needed.
The findings were verified by adhering to Guba’s four criteria for ensuring rigor in qualitative studies- credibility, transferability, dependability, and confirmability. 11 Credibility was ensured by using a well-established grounded theory methodology; the researcher was trained in working with the psychiatric population during her M. Phil in Clinical Psychology training, and the research was carried out as part of her PhD thesis. Methodological triangulation was achieved using a mixed methods design, and theoretical triangulation was achieved through a review of the literature. Discussions were conducted with the supervisor/guide (second author at each stage). Though the findings supplement the quantitative results as well as the literature on qualitative studies, more future studies will establish the transferability. The methods used and the validation process involved ensure the dependability and conformability of the results.
Participants were informed about the nature of the study (part of PhD research), and written informed consent was obtained for participation and audio recording of interviews. Confidentiality of the information given by the participants was ensured, and the data was solely used for research purposes. The immediate concerns of the participants and the family members were addressed by the researcher or referred to another mental health professional if required. Psychoeducation on the areas recognized during the assessment phase was provided.
Qualitative Analysis
The data obtained from the interviews were analyzed for recurrent or significant themes using the thematic analytic approach by Braun et al. 12 An inductive thematic analysis was used to develop themes from the interview data using ATLAS ti-7 software. Initial coding based on grounded theory was adopted to break down interview transcripts into initial codes, identifying key concepts related to remission experiences. The interview transcripts were read and reread by the first author to come up with initial ideas and codes based on interesting features of the data selected systematically across the entire data set. The data was grouped according to each code. After generating 800 initial codes, they were collated into potential themes, and a thematic map was generated. Focused coding was used to refine significant codes and develop categories. With the input of the second author, these themes were defined and named to produce the final report of nine themes. Axial coding was used to explore relationships between categories, linking them to form a cohesive understanding of functioning correlates. Theoretical integration was used to develop a grounded theory that explains a nuanced understanding of the experiences of patients with BD in remission.
Results
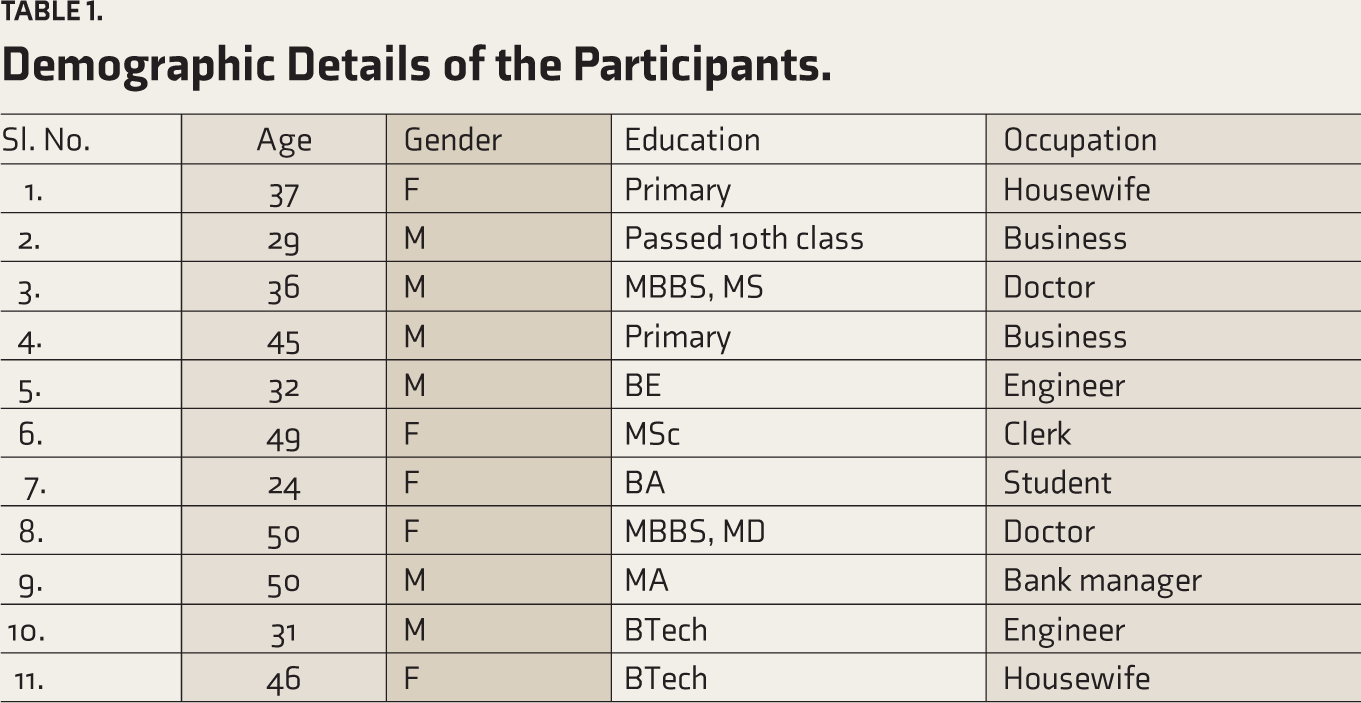
Findings from the 11 interviews are presented under each theme. Out of the 11 participants, 5 were females and 6 were males. The mean age of the sample was 39 years; 80% of the participants were employed, and the remaining were homemakers and students (Table 1).
Demographic Details of the Participants.
The analysis found that patients were affected psychologically concerning their self-functioning and their socio-occupational functioning. The thematic analysis resulted in nine themes, namely issues related to illness, treatment as an antidote, impact on self, relationship issues, coping strategies, disturbed cognitive functioning, stigma, occupational consequences, and dubious future (Table 2).
Themes and Subthemes of the Qualitative Interview.
Illness Issues
Most of the patients reported going through shock, anger, anxiety, denial, sadness, and finally acceptance of the diagnosis (“I was shocked when they told me the diagnosis and that I required medication. The fact that this is lifelong was my major worry, the financial constraints, the side effects after taking medications … I had to study and work. I was also apprehensive that the puffiness and other changes in my body might lead others to find out that I have this illness”). Patients attributed the illness to a variety of factors, including childhood trauma, neurobiological causes, stress, and fate (God). Variations in the mood affected functioning as reported by many (e.g., “before leaving for office I have laziness to start for work, I will sleep till 10:15 am and then I suddenly jump up from the bed and once I go I will be better.”). The sudden shifts and uncertainty created anxiety in patients (“Suddenly everything changes, everything from white it turns to black. I do not feel like doing anything in the whole world. It’s just me. I can’t imagine.… I could not attend class … very hard”). Relapses resulted in a reduction in efficiency and financial loss/burden (“during the time of relapse I ran through a very tough time…, I gave away a lot of money, had a debt of 10 lakhs”). Patients also reported anticipatory anxiety about the next episode; one said, “I have the fear that this illness may come again … whether it is going to start now … which illness will come now … it is mania or depression.”
Treatment as an Antidote
Treatment had a lot of positive effects on the patients. Many reported that their mood could be under control with treatment (“after prolonged treatment what I have noticed is that it is not going extreme. My mood was going out of control before, now I can control it”) and have better quality of life (“What I understand is I need lifelong medication and I can have good quality of life with medication … for the past 3 years I have been on medication and my quality of life is pretty good.”) Several side effects of medicines were bothering the patients. Most of them were associated with sleep issues such as drowsiness, early morning awakening, and weight gain (“I am double the weight now! These tablets have caused the weight gain … that keeps worrying
me, and my personality has changed too”). Some of the reasons for nonadherence to medication are sleep-related problems, stigma, and absence of mood symptoms.
Impact on Self
The majority of the sample perceived their self-image negatively. They considered themselves a burden and felt that they were less than others (“I have the thought that I am a patient always … sometimes when I am happy, I have a fear that I may have a loss … always I am not in a same level you know I am a patient”). Several needs emerged during the interview. The need for love and affiliation was the most predominant among them. (“I want to feel loved … nobody is there … nobody”). The need for independence was observed in another patient (“I want to live without depending on others … without causing trouble to others”). Contrary to this, some had dependency needs: “I get a feeling that I won’t be able to write, so I have difficulty in conducting this business alone, and I need someone to depend on.” The responses indicate a lack of confidence and a need for dependency even though they wanted to be independent.
The interplay of several emotions was seen among the patients, and emotional regulation seemed difficult even during the remission phase. Anger outbursts and irritability, difficulty balancing sadness and happiness, and fear of mood switching during happiness were notable (“The illness manifested in the beginning as anger then it was more of sadness … after that both started”). A lot of responses by the patients indicated that the self was in danger; they seemed to live a life of constant fear. One of them reported fear of others knowing about their illness, while another patient feared having another episode. Some shared the fear of not meeting others’ expectations. Patients showed varied responses concerning self-esteem (“I always look down on myself. I want to be a lot better, but I am not able to do anything, and I am frustrated”). Most of them had fluctuations between low and high self-esteem. Their self-esteem seems to be related to their faith in religion (a patient who was a doctor by profession reported that his self-esteem remained unaffected due to his faith in God) or their work performance. However, most tend to worry about family, work problems, and the future. They also experienced changes within themselves due to the impact of the illness. Bodily changes such as poor posture, weight gain, and dull facial expressions were reported after having this illness (“my body language is also kind of less confident … earlier I used to walk straight now it is sloppy”). Attitude toward other patients had also changed (“my approach towards other mentally ill patients changed, I became more empathetic”). Behavioral changes, such as laziness, avoidance of social gatherings, and disinterest in daily activities, were reported (“I avoid social functions so nobody has seen me in a very bad condition”).
Impact on Relationships
Patients with BD tend to have significant adjustment problems concerning their relationships. Primarily, suspiciousness during the episode ruined the trust, which was difficult to gain after remission. Several patients also reported poor interpersonal skills and criticism by their colleagues for their previous symptoms.
Even in remission, many reported poor social and familial interaction (“After relapse, I withdrew more, and my interaction has decreased be it socially or within the family. I don’t want to talk … I do not know what to talk”). Insecurity feelings also seem to affect the relationship. Patients perceived poor understanding by others about their problems and felt that their actions caused hatred in others. This might have led them to withdraw and isolate themselves from others in society (“I isolated myself from others and that led to further depression, it affected my academic life. I was poor in relationship with people I never knew how to adjust in life”). Patients have learned to keep a safe distance during their episodes. On a positive note, some patients reported being more empathetic after having the illness.
Familial relationships were impacted, too. Even though the patient’s family members were aware of their illness, many helped the patient improve. (“My in-laws are very cooperative; they consider it only a physical illness”). Some of the positive aspects were acceptance, motivation, and support from relatives. (“My husband initially had problems because I was always sleeping, … this was only an initial problem afterward he understood it”). They also helped the patient in accepting the diagnosis. The parent–child relationship also enabled them to adapt to the illness; one patient considers her father as her best friend. Coming to the negative side of a familial relationship, one patient reported being abandoned by his wife due to his illness. Marital infidelity also was found to worsen their symptoms.
Coping Strategies
Appraisal-focused strategies are those coping mechanisms that involve a change of mindset or a revision of thoughts. Denial was relatively less utilized compared to other coping mechanisms in this sample. One patient reported, “I kept the thought that the diagnosis might be wrong. I decided to respect the analysis and conclusion that the doctor might have had. On my side, I kept myself as a patient just to show the doctor.” Many patients tried to rationalize their thinking: “Understanding why it happened and what happened … thinking rationally and observing own behavior as a third person helped me.”
Problem-focused strategies modify the behavior of the person. Planning was utilized by a few patients to reduce stress (“Due to tension, now I have started planning things … whatever I need to do, in the morning I write it down”). Some also resorted to keeping themselves fit through exercise. One of the most common coping strategies was acceptance (“whatever happens, I need to accept it, whether good or bad”). To reduce stress, many have brought down their demands (“It’s not labor when I bring my demands down, I don’t study for long hours … I am satisfied with studying for half an hour.” ). A few others reduced their workload. Active coping, where the patients actively did something to come out of their problems, was also observed. Emotion-focused strategies include altering one’s emotions to tolerate or eliminate stress. Distractions like listening to music and doing more work also were used by many to prevent stress. Ventilation, seeking support (from family, friends, spouse), journalling, and tearing it were the methods adopted to cope (“I call one of my sisters to whom I am very close and talk”). Religious or spiritual coping helped most of the patients. It also prevented acting upon death wishes (“Several times I have felt to die … but I don’t do it because I know the Bible,” “in the very extreme negative situation I feel what is the point in living like this being of no use to myself and others,… since my religion is against it and God may punish me,… I am not committing suicide”).
Disturbance in Cognitive Functioning
Poor concentration, forgetting, poor decision making, difficulty with reading and writing, difficulty learning new things, and experiencing a mental block. (“I am not able to read books or newspapers or general knowledge as I am unable to concentrate and grasp
I just keep reading”). Another patient also responded along similar lines: “It’s my concentration defect. I cannot concentrate even if I like a book; the maximum I can concentrate on is half an hour … more than that, reading, watching a movie, or involving in any other activities will lead to lethargy, due to which I need to lie down or it may lead me to go to a maniac phase.” Thoughts about suicide, the future, medication, and self-blame predominated in the patients (“I think my skill of doing surgery has decreased, making decisions are a little difficult, and problem-solving is difficult too”).
Some of the patients reported that they were unable to think positively, while some tried to avoid thinking about their illness. Death wishes and suicidal thoughts were found in a few patients.
Perceived Stigma
The remitted patients identified shame, self-blame, self-doubt, self-judgment, and self-loathing as part of their daily experience of living with BD. Internalized negative attitudes influenced activities, relationships, and decisions, thereby affecting the quality of life. They mostly look down on themselves (“I am always a patient, what to do”). Some feel hurt and perceive hatred from others.
They reported stigma from others as well. Discrimination was present even in the family, among spouses, parents, and children. Several responses implying stigmatizing attitudes emerged during the interview. Society also was found to discriminate by name calling, segregation, talking behind their back, etc. (“I understood that my subordinates misbehaved with me, people started criticizing me … I saw a huge difference in others’ reactions towards me.”)
As an after-effect of stigma, many patients reported that they try their best to conceal their illness, especially from society (“Not out of fear but husband says we have a daughter if we say that mom has depression, it will be difficult for her marriage so I have not told others and it is not right to tell others”). Many of them became insecure, and they refused to come out of their houses, fearing rejection. Some even withdrew from all social activities and reported having an inferiority complex (“Really, I didn’t want to go back to the previous job where I got fired”).
Occupational Consequences
Occupation is one area where the patients were worst hit regarding their functioning. Absenteeism from work was one of the most common consequences in the remission period, the reasons being lack of initiative, depression, and low self-esteem. Interpersonal relationship issues with colleagues, not being assigned much work, frequent job transfers, job loss, and inability to rejoin after the illness were very clearly seen among the sample. (“In the office, I won’t be able to handle the work pressure now. Interpersonal relationships are now difficult.” Some of the patients consider work to be a burden (“If somebody asks me to do something, I feel sad … I have to put a lot of effort into doing something”). Even small work assigned seemed like an arduous task for them. Morning blues before going to work were reported. Due to all these issues, a few found jobs to be a source of unhappiness and tension.
Even though most reported negative experiences, few had positive experiences at the workplace, too. Few were able to work beyond their capability, and this has been attributed to “God’s intervention.” Few enjoyed doing work and were satisfied; some even improved, as work provided them with an engagement rather than being idle (“If I didn’t have this job, I would be laying on the bed … I will not go out anywhere”).
Even though positive experiences were present, they were overshadowed by negative experiences. Severe and sudden changes in their moods and symptoms often overwhelm their capacity to cope with work stress and their environment, leading to absenteeism, irregularity, and sometimes termination from work.
Dubious Future
Remitted patients with bipolar illness had several big plans in their minds, and many seemed to be optimistic about their plans. Patients were hopeful about getting well. For some, their hope was on medication. Many entrusted their hope to God. This might be because all other sources might have failed to provide meaning (“As the days pass I am growing more in Christ and definitely I will be in tune with God and definitely I will be doing god’s will more.… So I’m seeing a bright future”). Many patients were also pessimistic about their future and owed it to the uncertainty and unpredictability of the episodic illness (“It’s very difficult, so I am not thinking much about my future … I am uncertain about my future”).
Discussion
The study aimed to explore the subjective experiences related to BD in a sub-sample of patients with BD. Concerning the impact on self, stigma contributed significantly to the self-esteem of the patients (“Even though I have a feeling that I have achieved something in my life, I intermittently have the feeling that it is because I have this illness that many hate me”). The patients’ reactions are consistent with the modified labeling theory proposed by Link et al. 13 According to the theory, a mental illness label can impair one’s self-efficacy as one begins to fear uncontrollable negative reactions. The patients tend to become more secretive, withdrawn, and inactive. The label of mental illness is likened to hearing a death sentence in another qualitative study. 14
Improvement with medications such as lithium is consistent with the literature. 15 Similarly, side effects of medication were also an important contributor to their distress. 16 However, adherence to medications is reported to be associated with fewer health problems, better coping with stress, and a stronger belief in the controllability of their health. 17
Negatively perceived self-image, unmet needs of self, feeling like a patient, unstable emotions, living in constant fear, unstable self-esteem, worrying nature, and changes experienced during the remission phase tend to have a significant impact on the patient and their functioning. Most of these subthemes, except self-esteem, have not been identified in other qualitative studies. One important meta-analytic study has found fluctuating self-esteem in remitted patients with BD, 18 while another study has pointed out their low self-esteem. 19 Contrary to the expectations that remission might improve the perception of self, this study sheds light on the vulnerability they experience, which might impact all other areas.
Patients with BD tend to have significant adjustment problems concerning their relationships (“My life started changing. I started getting irritated, and that led to adjustment problems.… In the mornings, when I get up, I have no enthusiasm or energy for anything”). They tend to have greater difficulties in adjustment, specifically in leisure and work activities, than controls. 20 The relationship issues stemmed from suspiciousness, poor interpersonal skills, being subject to criticism, and denial of the patient’s illness by others. These results align with previous research 21 reporting BD to cause significant impairment of instrumental and interpersonal functioning. This study also reveals the impact of BD on the family (“if I go for a work conference, my husband would come and help me in typing and other aspects of my life, he would appreciate me especially when I am weak and lethargic”). Family support has been reported to influence the remitted patient positively in most interviews. It is already seen in past studies that empathy and understanding from another person can make it easier to cope with BD. 22 The support provided by family members in a collectivistic culture like India 23 might contribute as a protective factor. Previous studies have focused on the negative impact on the family; the relationship with the family was severely and adversely affected due to stigmatization and rejection within the family. 24 An Indian study also found that patients with BD were dissatisfied and discontented with their jobs, friends, and finances. They either did not participate in any recreational activities or derived little enjoyment from such activities if involved in them. 25 This highlights the importance of targeting relationships and expressed emotions during intervention for longer remission and preventing relapse. Most patients also used adaptive coping strategies, which are consistent with the previous qualitative studies.7,17,26
The presence of cognitive deficits such as poor concentration, memory, decision making, difficulty with reading and writing, learning new things, mind block, and negative thoughts in the sample might be due to the impact of either BD or the medications used. These findings are consistent with several neuropsychiatric studies.27–28 Robinson et al. 29 reported relatively marked impairment in aspects of executive function and verbal memory, resulting in functional disability. 30 Thoughts about suicide, the future, medication, and self-blame predominated in the patients. This confirms the findings from the previous studies that BD not only affects higher-order thinking but also causes negative ruminations.31–32
Stigma is a “dynamic, multifaceted social process” that has been consistently implicated as a key contributor to poor outcomes for many people who live with stigmatized health conditions, such as mental illnesses.33–34 The patients identified shame, self-blame, self-doubt, self-judgment, and self-loathing as part of their daily experience of living with BD. Internalized negative attitudes influenced activities, relationships, and decisions, thereby affecting the quality of life. Previous studies have also found numerous negative consequences due to the stigmatization of people with mental illness, such as reduced self-esteem,35–36 hurt and anger, 35 social rejection 13 , avoidance, delayed healthcare seeking, 37 unemployment and reduced income, 38 poorer quality of life, 39 and less social support. 40 This shows that despite awareness, the presence of stigma concerning mental disorders is a universal phenomenon.
Although BD had positive and negative consequences at work, the negative repercussions outweighed the positives in the sample. The cognitive decline, subsyndromal depression or manic symptoms, and other residual symptoms might be to blame for this. A previous qualitative study on the impact of BD on work functioning also identified similar themes, such as lack of continuity in work, illness management strategies in the workplace, stigma and disclosure in the workplace, and interpersonal problems at work. 41 These results also confirm the results found in the quantitative analysis. 2
In this sample, we can see that the participants have many uncertainties about their future due to the episodic nature of the illness. Yet, many of them are still in remission due to their coping abilities, realistic plans, and hope. A study by Jönsson et al. 42 also confirms this finding; they revealed that the daily life of those with BD was characterized by insecurity and challenges of accepting, understanding, and managing the illness. The nine identified themes provide a deeper understanding, which underscores the need for culturally sensitive interventions that address these multifaceted issues.
The study has certain strengths. This research explored in depth the subjective experiences of patients with BD, thereby obtaining a rich knowledge of factors that tend to affect functioning. The study comprised a widely representative sample drawn from diverse education, age, and occupational statuses, thus increasing the generalizability of the findings. Both a priori codes and codes developed through the study were used for data analysis, therefore ensuring the groundedness and density of the data.
A few limitations of the study include the probability of self-selection bias, the stringent criteria for remission used in the study, which led to the exclusion of cases who were remitted for less than six months, and the exclusion of patients who did not have any education.
In terms of implications, the study is one of the first to focus on an in-depth understanding of the functional correlates and experiences of remitted patients with BD in the Indian context. This helps to understand the psychopathology of BD in the cultural setting of India, with issues that are different from those in Western studies. This could broaden the theoretical understanding of determinants of functioning in remitted BD, thus helping the healthcare professionals to develop more targeted support strategies that acknowledge these individuals’ ongoing struggles, fostering a more holistic approach to their care and well-being. The study highlights that even with effective therapeutic and pharmacological interventions to treat BD, overlooking psychosocial variables can contribute to disability even in the absence of acute symptoms.
Supplemental Material
Supplemental material for this article available online.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The article being submitted has not been published, simultaneously submitted, or already accepted for publication elsewhere. The manuscript has been read and approved by all the authors, and the requirements for authorship, as stated earlier in this document, have been met. Each author believes that the manuscript represents honest work. We declare that, to the best of our knowledge, the manuscript does not infringe upon any copyright or property right of any third party.
Declaration Regarding the Use of Generative AI
We declare that we have not used any AI tools in the writing of this manuscript, and we assume full responsibility for the entire content of the manuscript.
Ethical Statements
Ethics committee of National Institute of Mental Health and Neuro Sciences, Bangalore.
Approval Number: No. NIMH/DO/SUB-COMMITTEE/2013 dated: 24 October 2013.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.