
Abstract
Background:
Children with autism spectrum disorder (ASD) exhibit atypical responses to sensory stimuli. These sensory and perceptual issues persist as hyper-, hypo-, or atypical sensory reactivity that impacts their daily activities. The present protocol describes a method for developing a locally relevant and simple instrument for identifying and estimating the severity of sensory reactivity in children with ASD.
Novelty:
Employing a consultative approach, the authors aim to develop and validate an Indian instrument to assess sensory reactivity in children with ASD.
Objectives:
To gather insights from parents and experts about sensory reactivity patterns in children with ASD and to use this information to create and validate a culturally relevant tool for measuring the severity of sensory reactivity in these children.
Methods:
This study will be conducted in two phases following an exploratory sequential mixed-method design. In the first phase, data will be collected through in-depth interviews of parents of children with ASD and focused group discussions with the experts. The collected data will be used to identify different themes and domains related to sensory reactivity. A questionnaire will be developed based on their inputs. In the second phase, the instrument will be analyzed further using exploratory factor analysis to obtain the factor structure and confirmatory factor analysis to test the factor structure of the developed instrument.
Expected Outcome:
A simple, reliable, and validated severity instrument will be developed for children with ASD and made accessible to all for convenient use.
In children with ASD, sensory reactivity is a persistent trait that frequently remains unnoticed due to communication challenges. The study aims to develop a valid and reliable instrument for the assessment of the severity of sensory reactivity in children with ASD. A two-phase, exploratory sequential mixed-method study design will be utilized. We expect to design a simple, precise, easy-to-administer instrument for identifying and assessing the severity of sensory reactivity in children with ASD.Key Messages:
Autism spectrum disorder (ASD) is a neurodevelopmental condition manifested in childhood, marked by significant difficulties in social interactions, inability to relate to people and their surroundings, repetitive verbal and nonverbal behaviors, and stereotypical patterns. These stereotypical or repetitive behavior patterns result from sensory processing deficits. 1 India’s huge population and the degree of genetic, socioeconomic, and environmental diversity places it in a unique position to influence the global prevalence of autism. Considering that 95% of children with ASD (CwASD) live in low-middle-income countries and India’s huge population, its burden of autism may be one of the highest in the world. 2
Sensory reactivity pertains to the brain’s ability to detect, process, and interpret sensory information. This neurological function integrates both internal bodily sensations and external environmental stimuli, facilitating adaptive and efficient interaction with one’s surroundings. While sensory reactivity is common in CwASD, it can be frequently observed in children with other developmental disabilities and may also be present in typically developing children. 3 Atypical reactions to sensory stimuli, such as increased sensitivity or decreased responsiveness to noise, textures, lights, or other sensory inputs, are prominent sensory reactivities in CwASD. Although there are many different sensory and perceptual impairments, patterns of sensory reactivities across modalities are typically described as hyper- and hypo-reactivity. 4 Due to these sensory deficiencies, CwASD may find their sensory surroundings to be either overwhelming or under-stimulating, which can cause problems with everyday functioning and interpersonal relationships.
The Diagnostic and Statistical Manual of Mental Disorders, 4th edition, text revision (DSM-IV-TR) 5 did not include sensory reactivity as a diagnostic criterion. However, the DSM-5, 1 empirically introduced sensory “hyper-” and “hypo-”reactivity as subcriteria for ASD, defined as over and under-responsiveness. Hyperactivity refers to heightened or exaggerated responses to specific sensory stimuli, such as sounds and textures, or an intense preoccupation with certain stimuli, including lights, sounds, or spinning objects. In contrast, hypo-reactivity is characterized by a reduced or absent response to sensory inputs, such as pain, heat, or cold.1,6
While the precise origins of these variations in sensory reactivity remain unclear, they are thought to be associated with differences in the brain’s integration and processing of sensory information or other sensory processing impairments.1,7 Numerous theoretical explanations have been proposed for a shared element responsible for atypical sensory reactivity. However, no theoretical model completely articulates the reasons for sensory impairments in autism. The initial frame of reference for studies on sensory reactivity is Ayres’ theory of sensory integration (1972). 8 It broadly defined “sensory integration” as a behavioral reaction to sensory stimuli. Dunn 9 further established an innovative model that addressed a person’s behavioral reactions and neurological thresholds to sensory input and identified four subtypes of sensory reactivity deficits. These thresholds, whether high or low, impact people’s reactions actively or passively by dictating the quantity of sensory information needed for a reaction. While seekers actively interact with their surroundings despite presumably missing sensory input, those with poor registration have a high threshold and passive reactions, frequently failing to react to inputs. Sensory avoidants also have low thresholds and active responses and respond strongly to overwhelming stimuli. Miller’s model of sensory reactivity includes three aspects of sensory integration, namely sensory modulation, sensory–motor integration, and sensory discrimination. 10 Therefore, we will utilize both models for our theoretical framework for sensory reactivity, which will include Dunn’s model as well as Miller’s model.
Different assessment tools have been developed globally to measure sensory reactivity in CwASD. The most used among them are the Sensory Profile
Current sensory reactivity assessment measures lack indigenous relevance in the Indian context. Items in these instruments are difficult to apply in our population, and the language of the items is not relatable to Indian parents. Most of the tools used are so extensive, take too much time to administer, and hence lack precision. The existing (e.g., Sensory Profile 2 by Winnie Dunn) 11 scoring system is complex and involves individual scoring of quadrants, sensory sections, and behavioral sections used by occupational therapists. It does not provide an overall score of sensory reactivity construct. Most of the existing instruments measure sensory issues across diverse neurodevelopmental disorders in children, whereas our instrument will be more specific for children with autism and sensory issues. Further items are not covered under the theoretical construct of sensory reactivity (e.g., sensory overresponsive, sensory under-responsive, and sensory seeking); it is covered under dimensions of sensory systems (e.g., auditory, visual, and tactile) in Sensory Profile 2. 11 Existing instruments are caregiver-rated, not clinician- or therapist-rated.
Items are generic without relevant examples (e.g., seem unaware of temperature changes). Most of the parents interpreted it to be a hot and cold sensation or fever in response to this item, while it denotes awareness of weather changes in the surroundings. Therefore, the items are not user-friendly or relatable. Till now, we have two tools developed for the assessment, diagnosis, and severity of autism in India. INCLEN Diagnostic Tool for ASD (INDT-ASD) by Juneja et al. (2014)15 is the diagnostic tool for ASD according to the DSM-IV criterion. Indian Scale for Assessment of Autism (ISAA) 16 is a severity and diagnostic instrument that holistically focuses on all the aspects of autism, including the sensory aspects, as one of the subdomains. It does not give much emphasis on the sensory aspect, though. This study aims to address a significant gap in the assessment of sensory reactivity in children CwASD in India, as existing tools available are not suitable in the Indian context. The research seeks to develop a culturally appropriate assessment instrument by incorporating perspectives from parents and professionals through both qualitative and quantitative methodologies. The anticipated outcome is a user-friendly, reliable, and publicly accessible tool that delivers accurate information to facilitate personalized intervention strategies. By incorporating cultural considerations, this study will not only improve interventions for ASD but also establish a standard for contextually relevant research in neurodevelopmental disorders. Therefore, it is crucial to investigate sensory reactivity as a specific attribute or construct in CwASD within an Indian framework. Hence, we aim to capture parental experiences and expert perspectives on patterns of sensory reactivity among CwASD to develop further and validate a culturally relevant instrument for assessing the severity of sensory reactivity in CwASD.
Methodology
Ethical Procedures
The institutional ethics committee has approved the study, and the research will be conducted following the ethical guidelines for biomedical research on human subjects, as outlined by the ICMR, 2017. Children will be selected based on the clearly defined inclusion and exclusion criteria of the participants to ensure the relevance and appropriateness of the participants for the study. Verbal assent will be obtained from the CwASD, written informed consent will be obtained from their parents. The data collected from the participants will be anonymized or coded to protect their identity, and the anonymity of the participants will be preserved while reporting the findings of the study. Parents will have the right to revoke their consent and withdraw from the study at any point. This study is prospectively registered with the Clinical Trial Registry of India (CTRI/2024/09/074306).
Proposed Study Design, Participants, Setting
The study will be carried out in two phases using a sequential mixed-method research design (Figure 1). The findings from the initial phase will inform the development and validation of the instrument in the subsequent phase. Parents of children with ASD aged 2–6 years clinically diagnosed with DSM-5 1 and confirmed by the ISAA, 16 visiting our tertiary care psychiatric center, will be eligible to participate after taking due informed consent from parents. Children with known genetic syndromes, comorbid neurological disorders, and psychiatric illnesses such as intellectual disability, attention-deficit/hyperactivity disorder, anxiety disorders, and mood disorders will be excluded from our study.
A schematic representation of the implementation plan of the study.
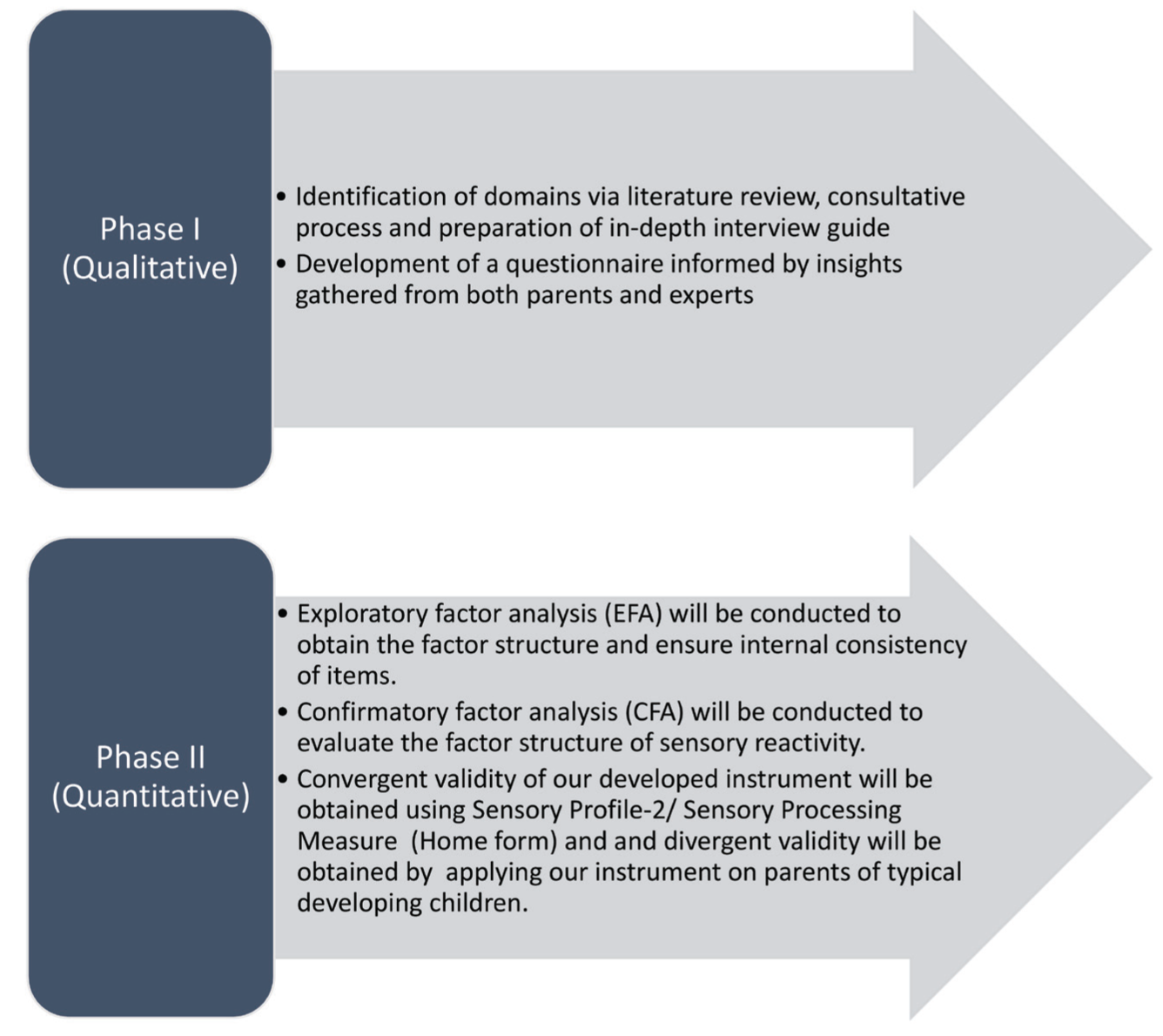
Phase 1 (Qualitative): Development of the Questionnaire
Preparation of an In-depth Interview Guide from the Literature Review and Consultative Process
This step will focus on gathering and examining tools and questionnaires assessing sensory impairments across sensory systems (such as vision, auditory, and tactile) and their associated dimensions through an exhaustive literature review. The psychometric properties and conceptual framework underlying each instrument will be reviewed to compare existing methods. Based on the literature review, an in-depth interview guide with a few proposed questions or items will be developed and refined based on inputs from experts and parents.
Development of a Questionnaire Based on Inputs from Parents and Experts
To ensure accuracy, we will observe CwASD, as well as gather insights from their caregivers or parents of CwASD diagnosed as per DSM-5 (aged 2–6 years), with a sample size of at least 15. In-depth interviews will be conducted with parents of CwASD in the language that the parents are most comfortable with, ensuring effective communication. Each session is expected to last around 45–50 minutes, during which one or both parents may participate. One researcher will lead the interview, guide the conversation, and ask questions, while the other will take detailed notes. With prior consent, the interviews will be audio-recorded, transcribed, and translated from Hindi to English in accordance with qualitative translation methodology guidelines. 17 The objective is to continue data collection until saturation is achieved, meaning no new information or themes emerge from subsequent interviews.
Focused group discussions will be conducted with professionals who are well versed in ASD (including psychiatrists, clinical psychologists, occupational therapists, speech-language pathologists, and pediatricians). A consultative process will be conducted with experts who are well versed in early intervention for CwASD to guide key aspects of the instrument preparation, including item length, response formats (self-reported or interviewer administered), types of questions (dichotomous or open-ended), scoring methods (Likert scale), complexity, relevant domains, and language. To facilitate this process, other experts from various institutions, from outside or of our own, will be invited to participate in virtual meetings, if required.
Reviewing of the Questionnaire by Experts for Content Validity
We would further aim to refine a questionnaire for assessing sensory reactivity in CwASD through an iterative process to ensure its applicability in real-world settings. Items of the domains that will be created based on initial interviews will be reviewed by at least five different professionals for content validity to evaluate their relevance, importance, and clarity.
Phase 2 (Quantitative): Validation of the Questionnaire
The primary objective of the second quantitative phase is to validate the factor structure of the sensory reactivity instrument using a large sample and to assess the reliability and validity of the obtained scores. Exploratory factor analysis (EFA) will be performed to obtain the internal consistency and factor structure. Confirmatory factor analysis (CFA) will be performed to test the factor structure of sensory reactivity by applying the developed instrument to parents of CwASD. The convergent validity of our developed instrument will be checked using existing standard instruments. The divergent validity of our developed instrument will be checked by applying a questionnaire to parents of typically developing children.
Sampling Technique and Sample Size Estimation
A non-probability, purposive sampling technique will be used for our study for both phases. The initially developed, proposed instrument will be applied to a purposively selected sample of parents of CwASD of 2–6 years, with comparison participants drawn from typically developing children from play schools and pediatrics outpatient departments. Stratification by age will ensure comparability between groups. The sample size for in-depth interviews (Phase 1) will be a minimum of 15 parents of CwASD, depending upon the variability and richness of qualitative data. The sample size for Phase 2 (EFA and CFA) will be preliminary estimated based on a respondent-to-item ratio of 5–10:1 to allow for sufficient statistical power and factor analysis. However, the exact number of items will be decided after the first phase. 18
Instruments
Semi-structured Proforma for CwASD and Their Parents
A specifically designed proforma will be utilized to collect sociodemographic information, including age in months, sex, toddler versus preschooler, locality, and relationship of the primary therapist to the child, the informant’s educational background and occupation, as well as the duration of daily contact with the child. Additionally, clinical profile data will be gathered, encompassing gestational duration, mode of delivery, family history of late language development or genetic disorders, family structure, prerequisite learning skills components, the current mode of communication, and the presence of sensory issues.
Indian Scale for Assessment of Autism
The ISAA is designed for the diagnosis and severity assessment of autism, categorizing severity levels as mild (70–106), moderate (107–153), and severe (above 153). It comprises 40 items distributed across six domains and employs a Likert scale ranging from 1 to 5 for scoring. A higher total score indicates greater severity, with a maximum possible score of 200 and a cut-off score of 70. 16
Proposed Tool for Sensory Reactivity in CwASD
Based upon our previous work and exhaustive literature review, our proposed tool tentatively will have four major domains (hyper-responsive, hypo-responsive, sensory seeker, and socio-emotional aspects) of sensory reactivity in CwASD. 19 Moreover, we will explore domains of sensory reactivity across sensory systems such as visual, auditory, tactile, vestibular, proprioceptive, and oro-sensory (gustatory, olfactory).
Sensory Profile 2 (SP-2)
The SP-2 is a standard 86-item tool for ages ranging from 3 to 14 years. It consists of several quadrants of items (registration, seeking, sensitivity, and avoiding) and associated sensory systems (e.g., Tactile, proprioceptive, visual, auditory, vestibular, oro-sensory). This tool will be utilized to assess the convergent validity of our newly developed scale. 11
Sensory Processing Measure Home Form (SPM-Home Form)
The Sensory Processing Measure (SPM) is a tool designed to assess children aged 5–12 years. The SPM Home Form consists of 75 items and is completed by the child’s parent or caregiver. The items cover a wide range of behaviors and characteristics related to sensory processing, social participation, and praxis. The Home Form yields scoring on eight domains, namely social participation (SOC), vision (VIS), hearing (HEA), touch (TOU), body awareness (BOD), balance and motion (BAL), planning and ideas (PLA), and total sensory systems (TOT). Scoring consists of a 4-point Likert scale in which 1 refers to “Never,” 2 indicates “Occasionally,” 3 implies “Frequently,” and 4 indicates “Always.” This tool will be incorporated to measure the convergent validity of our developed scale(Parham et al., 2007). 20
Implementation Plan
The study will be conducted in two phases over a three-year period. The first phase will consist of identifying domains of sensory reactivity through an exhaustive literature review and consultative iterations. Following this, a questionnaire will be developed based on input from the parents and experts. The second phase will consist of validating the questionnaire. The phase-wise description is given in Figure 1.
A Schematic Representation of the Study Design.
Phase 1
The data will be analyzed by thematic analysis. The researchers will transcribe and translate the audio recording of the interview. Guidelines about qualitative research will be followed. The transcribed data from each interview will be thoroughly reviewed to ensure familiarity with the raw information. During this familiarization process, the experts (e.g., speech therapists and occupational therapists) will highlight the emerging codes and identify new themes. The coding index will organize the emerging codes into superordinate themes, superordinate themes, and subthemes. We will use supporting data in the form of excerpts to analyze the themes and final dimensions, and items will be narrated (see Figure 2 for Phase I statistical analysis plan).
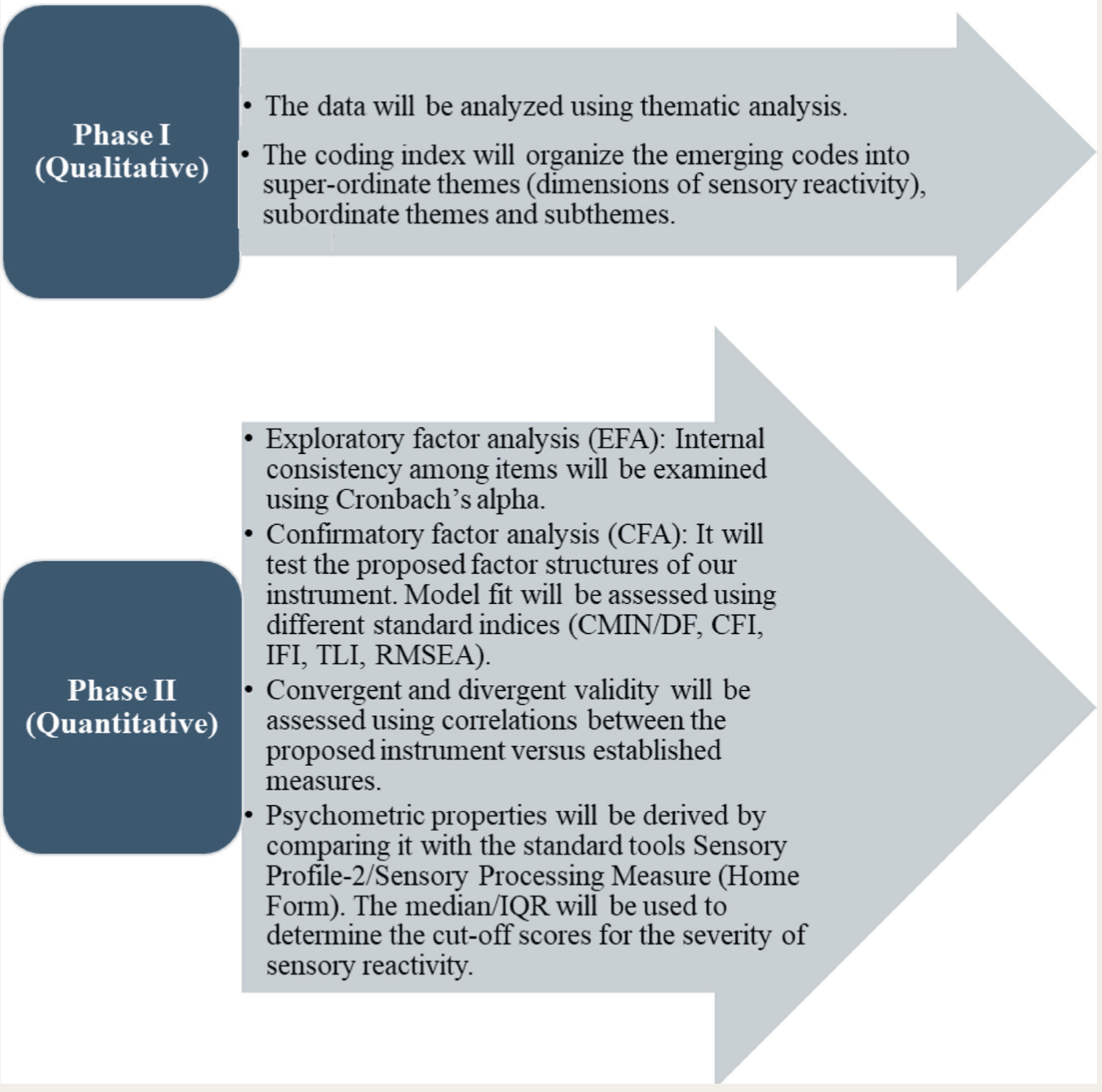
CMIN/DF: Chi-square minimum/degree of freedom; CFI: Comparative fit index; IFI: Incremental Fit Indices; TLI: Tucker–Lewis Index; RMSEA: Root mean square error of approximation; IQR: Inter-quartile range.
Phase 2
Descriptive statistics will be used to represent frequencies and means of participants and items. An exploratory factor analysis will be performed to explore and obtain the underlying factor structure of our instrument for sensory reactivity in ASD. A principal component analysis with promax rotation will be conducted on the items related to dimensions. To assess the suitability of factor structure, the Kaiser–Meyer–Olkin 21 measure of sampling adequacy and Bartlett’s test for sphericity 22 will be applied. Cronbach’s alpha and intraclass correlation coefficient will be applied to evaluate the internal consistency and reliability of the items of the developed instrument. Confirmatory factor analysis will be performed to compare the one-factor model with the proposed factor structure of the instrument. In CFA, model-fit indices will be utilized by recommended fit indices, including the chi-square divided by its degree of freedom (CMIN/DF < 3), comparative fit index (CFI ≥ 0.90), Tucker–Lewis index (TLI ≥ 0.95), and root mean square error of approximation (RMSEA ≤ 0.08) for the suitability of factor structure recommended by established guidelines. 23 Bivariate correlations will be utilized for the convergent and divergent validity between the proposed instrument scores versus existing measures (SP-2 11 SPM Home Form 20 , and our instrument scores on parents of typical developing children). Our sensory reactivity instrument will be translated into Hindi following the procedure recommended by the World Health Organization, 2013. 24 The psychometric properties of our instrument will be derived by comparing it with the standard tools, SP-2 and SPM-Home Form. The median and interquartile range will be used to determine the cut-off scores for severity. In the second phase, statistical analysis will be conducted using SPSS AMOS version 27.0.0 (SPSS Inc., Chicago, IL, USA) (see Figure 2 for Phase II statistical analysis plan).
Timelines
The activities to be undertaken, along with their corresponding timelines, for the preparatory phase, data collection, analysis, and report writing are outlined. Table 1 depicts a phase-wise breakdown of the tasks.
Timeline of the Study.
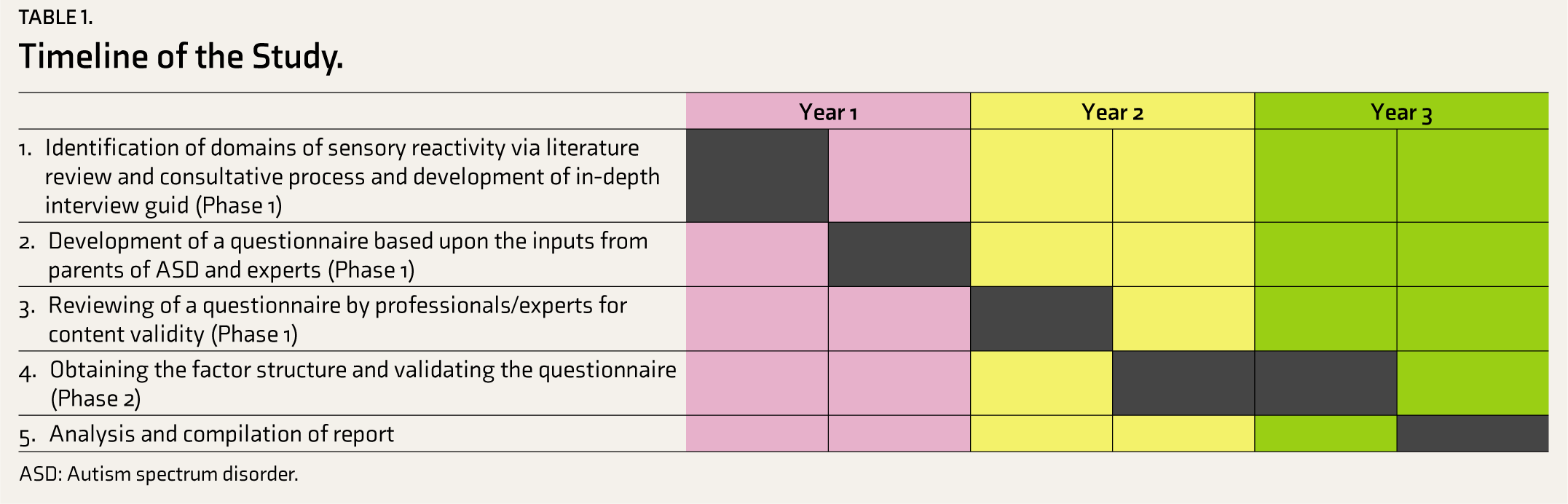
ASD: Autism spectrum disorder.
Discussion
The proposed study aims to develop an Indian instrument to measure the severity of sensory reactivity in CwASD, validate it among parents of CwASD, and compare it with typically growing children for appropriate use in the general population. We will employ a two-phase, exploratory sequential mixed-method study design to investigate, develop, and validate the domains of the newly developed scale for assessing the severity of sensory reactivity in CwASD. The insights obtained from the initial qualitative phase will inform the development of the dimensions of our tool. Subsequently, the tool will be validated using a sample of parents of CwASD and typically growing children through exploratory and confirmatory factor analyses, which will further provide a factor structure for the scale.
Over the past three years, our clinical experience has highlighted a significant gap in community resources for children diagnosed with ASD, particularly regarding their sensory issues. The majority of CwASD experience sensory issues that remain unaddressed in the absence of a tailored approach to assessment and treatment. The literature revealed a high prevalence of sensory dysfunction, resulting in the impaired modulation of the central nervous system in CwASD. 25 In one study, CwASD experience sensory difficulties up to 78%, more particularly in three areas, namely tactile sensitivity (86%), hypo-responsive (86%), and auditory discrimination (64%). 26 This makes it important to explore and identify tools and plan therapeutic management to facilitate the assessment of the severity of sensory reactivity. There is a need for a culture-specific tool that can evaluate the sensory processing abilities of CwASD. Sensory reactivity seems to be a more complex process than captured in DSM-5. 1 Therefore, this sensory tool will be designed to serve as a clinical tool for identifying sensory reactivity in CwASD.
Implications of the Study
No factor analysis has been conducted on sensory reactivity in children diagnosed with ASD in our population. Thus, there is a pressing need to create a culturally attuned assessment tool that better reflects the specific sensory experiences of CwASD in the Indian context. Our sensory reactivity tool for CwASD will be easily accessible and will provide information regarding sensory reactivity to support individualized treatment strategies in these children.
Expected Challenges
The study anticipates some challenges that might be faced during the study’s conduction. First, some of the children included might be undergoing therapy at the time of the study, making it challenging for parents to accurately recall sensory issues that existed before the initiation of therapy. Additionally, due to logistical constraints, it might not be possible to interview both parents for all children, which will limit the richness of the data collected. Furthermore, the study will focus exclusively on children aged 2–6 years, thus excluding other age groups, which might not provide a comprehensive representation of sensory reactivity in older CwASD. Moreover, we plan for a multicenter study of different age groups of children and adolescents with autism. Given that the study will be conducted in a single tertiary care referral hospital in East India, its findings may limit the generalizability to other regions of the country.
Expected Outcome
We expect to develop a robust tool to assess the severity of sensory reactivity in CwASD, which can be validated in other centers. The tool will be user-friendly, comprehensible, and accessible to healthcare providers, facilitating the identification and assessment of sensory reactivity severity in CwASD. It will be precise and more focused and will provide accurate information about sensory reactivity in CwASD to enable an individualized treatment strategy.
Supplemental Material
Supplemental material for this article is available online.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
The authors thank Dr. Ashoo Gover, Dr. Neha Dahiya, Dr. Ravinder Singh, and Dr. Harpreet Singh from the ICMR, Professor V. L. Nimgaonkar, Dr. Mary Hawk, Dr. Triptish Bhatia, and the Psychiatric Research Infrastructure for Intervention and Implementation in India (PRIIIA) faculty. The authors also thank project staff members and clinical and child psychologist of Department of Psychiatry, AIIMS, Patna.
Author’s Note
The content of this manuscript is solely the responsibility of the authors and does not necessarily represent the official views of NIH or FIC who had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Declaration of Conflict of Interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None Used.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received financial support for the research from Indian Council of Medical Research, Government of India (ICMR Grant- File No. GRANTATHON2/MH-13/2023-NCD-II; 2022-17781) and the training “Psychiatric Research Infrastructure for Intervention and Implementation in India (PRIIIA)” (D43 TW009114, HMSC File No 2019-7623 dated January 6, 2020, funded by Fogarty International Centre, NIH).
Ethical Approval
Ethical approval for this work was obtained from Institutional Ethics Committee, AIIMS, Patna, India (AIIMS /Pat/IEC/2022/1022). This study is prospectively registered with the Clinical Trial Registry of India (CTRI/2024/09/074306).
Informed Consent
The authors certify that they will obtain written informed consent from the parents and verbal assent from CwASD.
Reporting Guideline
The SPIRIT 2013 Checklist (reporting guideline) is uploaded as a supplementary online material file.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.