
Abstract
Background:
Autism spectrum disorder (ASD) is a lifelong condition requiring continued rehabilitation services. However, children with ASD who seek rehabilitation services tend to drop out once they enter puberty, because of varying reasons, some of which are unknown. This study intended to explore the reasons for not availing of rehabilitation services in families of adolescents with ASD and the parental challenges in taking care of adolescents with ASD.
Method:
The study followed a descriptive qualitative research design by conducting in-depth interviews with 12 primary caregivers of adolescents with ASD (10 to 19 years; mean age 16.3 years) who were not availing of any direct rehabilitation services. All interviews were conducted by telephone, and data obtained were subjected to thematic analysis.
Results:
The results showed two major themes, viz. reasons for discontinuing the rehabilitation services and parental challenges among primary caregivers of adolescents with ASD, and their corresponding subthemes. The reasons for discontinuation of rehabilitation included financial difficulties, difficulties in handling the child, and a lack of improvement in the child. A few of the parental challenges were disruptive behaviors and associated medical conditions of the child and difficulty in managing changes during adolescence.
Conclusion:
The study revealed several reasons as well as potential barriers to avail rehabilitation services in Indian families of adolescents with ASD. The data further unveil related parenting challenges specific to the Indian context. Further, implications for service providers and policymakers are discussed.
Findings from the study reveal salient reasons for the discontinuation of rehabilitation services as well as various parenting challenges among primary caregivers of adolescents with ASD relevant to the Indian context. These findings have implications for mental health care professionals and policymakers.Key Messages:
Autism spectrum disorder (ASD) is a neurodevelopmental disorder characterized by impairments in verbal and nonverbal communication, social interactions, as well as restrictive or repetitive behaviors that persist well into adulthood. 1 Early rehabilitation services are always preferred for children with ASD; yet, the need for ongoing rehabilitation services planned explicitly for adolescents with ASD cannot be underestimated. Given the range of difficulties and issues that change over time, there is a need to provide continuous rehabilitation services to make adolescents with ASD lead independent or semi-independent lives in adulthood. 2 While several children with ASD seek rehabilitation services, many tend to drop out once they enter puberty 3 because of varying reasons that often remain unknown. It is assumed that availing of long-term support services for adolescents with ASD may be compromised because of parent- or client-related issues. 4
Families of adolescents with ASD experience significant difficulties in transitioning to adult medical care. A few barriers to accessing health or rehabilitation services are financial hardships to cover services for their children, difficulty in getting insurance reimbursement for needed services, 5 and unavailability of services. 6 Other barriers faced by families include lack of information on the transition process, difficulty finding a service provider with sufficient ASD knowledge, lack of coordination and communication between service providers, 7 and difficulty in receiving transition plan for adolescents with ASD. 5
Primary caregivers of children with ASD play a key role in facilitating continued access to various rehabilitation services to facilitate overall development. Providing intensive and adequate care to an adolescent with ASD is always an enduring task for the parents or caregivers. Many parents reported a negative impact on their recreational activities, finances, physical and mental health, marital relationships, and personal development. 8 Furthermore, parental misconceptions and guilt,9,10 behavioral problems, and social and emotional difficulties 11 in adolescents with ASD could lead to unfavorable effects on the mental and physical health and quality of life of the parents, especially the mother. 12
There is a lack of information regarding access barriers to rehabilitation services in parents of adolescents with ASD not receiving rehabilitation services. The above-presented literature is largely from the families who either never availed of or were availing of rehabilitation services for adolescents with ASD. To the best of our knowledge, none of the studies have particularly investigated the reasons for discontinuing rehabilitation services in this population. This particular gap in knowledge is more crucial in a developing nation with limited resources and health insurance facilities. This brings us to the research question, “What are the reasons for nonavailing of rehabilitation services in families of adolescents with ASD?” Given this need, this study aimed to explore the reasons for not availing of rehabilitation services and parental challenges and issues in families of adolescents with ASD within the cultural context of India.
Method
This study employed a qualitative design where data was collected using in-depth interviews and was subjected to thematic analysis. 13
Participants
Participants were recruited from an ASD (parent) support group and a special school (previous records of children with ASD who discontinued schooling) in the South-Indian state of Kerala. A purposive sampling procedure was used to recruit the participants. Participants for the study were the parents or the primary caregivers (who took care of and spent most time of the day with the patient) of adolescents (age range 10 to 19 years, as per the WHO 14 ) with ASD who had received the diagnosis of ASD from a psychiatrist and/or clinical psychologist, who were not availing of any direct rehabilitation services (i.e., speech therapy, occupational therapy, special education services at school, behavioral therapy, and vocational training) for a minimum period of two years. The details on autism severity in adolescents with ASD were obtained from the medical records. Families having adolescents with ASD having severe degenerative conditions (e.g., Rett’s disorder, childhood disintegrative disorder, or Fragile X-syndrome) and/or with vision or hearing impairment(s) were excluded. The interview was carried out in the local language, Malayalam, by the first author, a native speaker of the language.
Procedure
The study protocol was approved by the Institutional Research and the Institutional Ethics Committee (589-2020) and registered under the Clinical Trials Registry-India (CTRI/2021/01/030172). A semi-structured interview guide eliciting reasons for not availing of rehabilitation services and parental challenges experienced by primary caregivers was prepared based on the literature search and expert opinion (Appendix A, online-only supplementary material). Permissions were obtained from the respective centers for collecting data. All primary caregivers were screened as per the study criteria. After obtaining consent, the first author carried out one-to-one in-depth telephonic interviews at a time provided by individual participants as per their convenience. The interview started by explaining the purpose of the study, guaranteeing confidentiality, and seeking demographic details. As the questioning strategy was responsive to each participant, the interviewer used probes to clarify comments and elicit in-depth explanations. An android application, Cube ACR, was used to record the consent and the complete telephonic interviews. The data were collected from January to March 2021.
Coding and Analysis
All obtained samples were played back and transliterated offline to ensure the accuracy of information. All transcripts were further read and verified against the audio recordings by an external reviewer and native speaker of the language of the interview. Saturation of data was observed after the ninth participant. However, data were collected for additional three participants to ascertain the same. The verified transcripts were read systematically and analyzed using a six-phase thematic analysis. 15 These steps involved familiarizing with the data (transcripts), followed by the generation of names/initial codes that addressed respective research questions. Statements that illustrated the essence of each code were highlighted and assigned numbers to locate the codes within the transcripts. Subsequently, these initial codes were reviewed by the second author in order to retain the diversity of the initial codes. Finally, the codes were checked and discussed by all the authors.
Verification of data integrity was done with the involvement of an external reviewer. The codes from the external reviewer were compared, and discrepancies were discussed within the research team. A code list was generated after coding the entire data. For the purpose of analysis and presentation of the result, all participants were anonymized, and excerpts were identified by the notation of mother (M) and father (F) with an accompanying participant number (Appendix B, online-only supplementary material).
Results
A total of 12 primary caregivers (11 mothers and one father) of adolescents with ASD (mean age = 16.3 years; SD = 2.74 years) participated in the interview. As reported by them, the commonly availed rehabilitation services (before discontinuation) included school-based special education, speech and language therapy, occupational therapy, and physiotherapy. The average duration for each interview was approximately 45 min. Table 1 presents the demographic details of caregivers and adolescents with ASD.
Details of Primary Caregivers and Adolescents with ASD
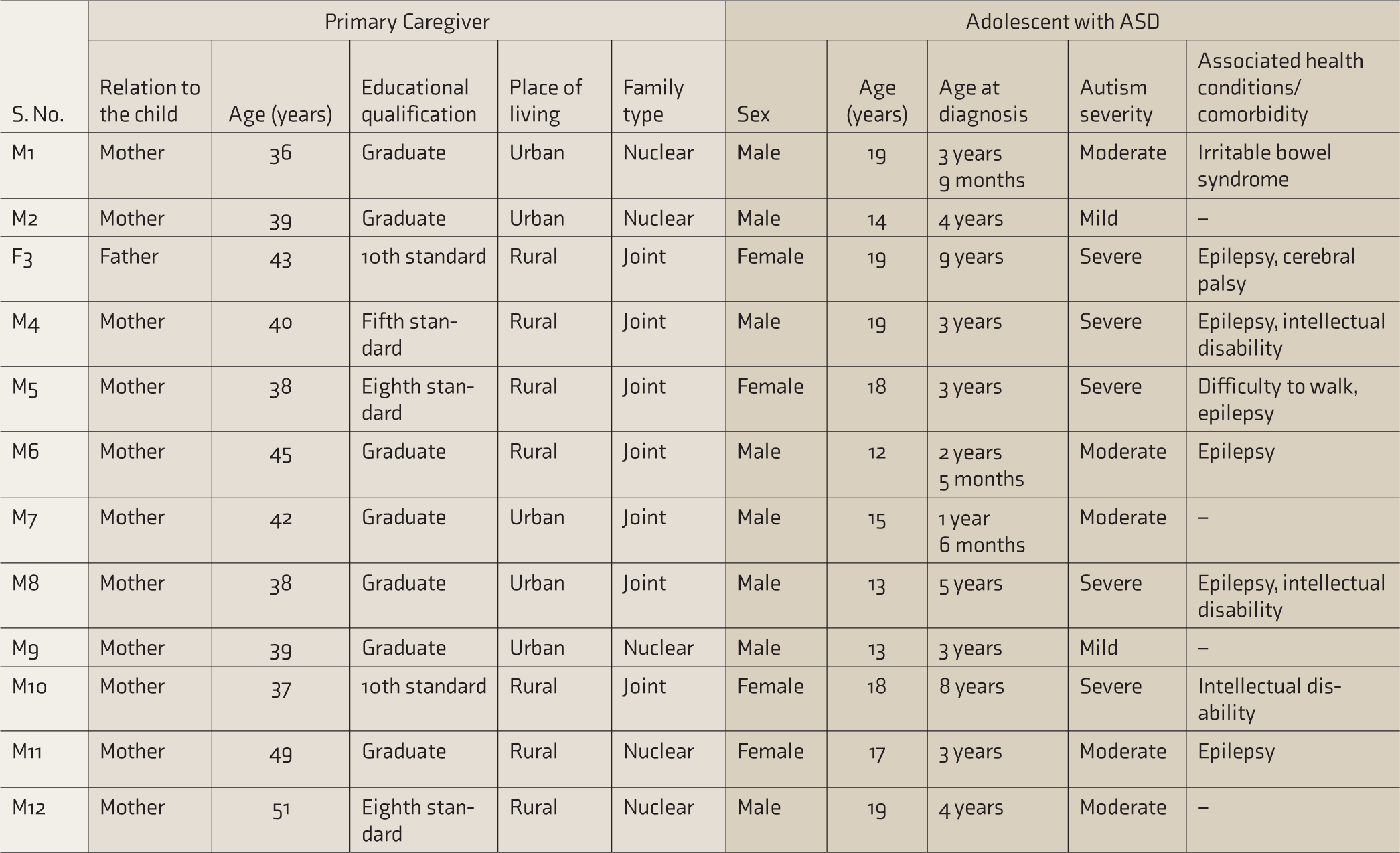
ASD, Autism Spectrum Disorders.
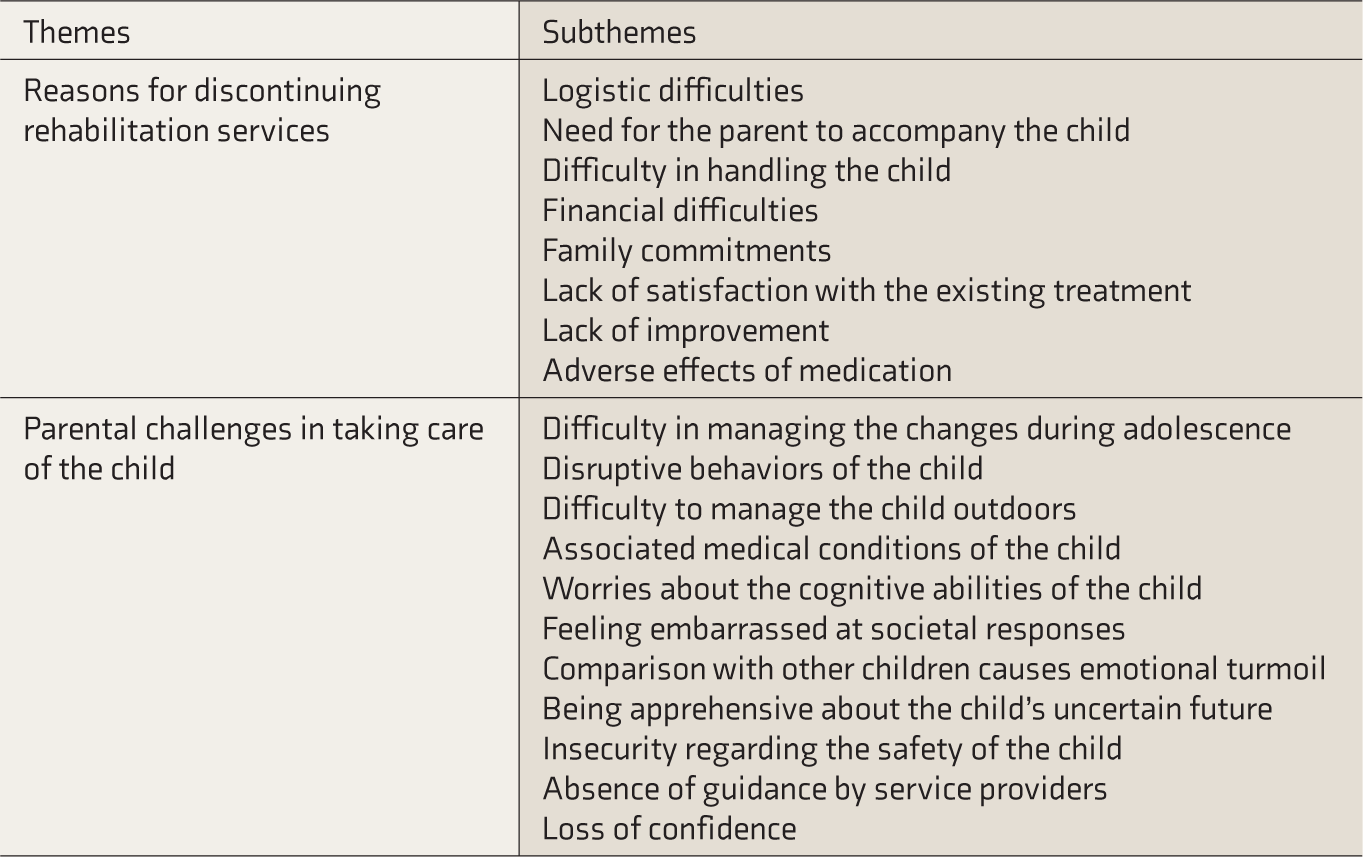
The results revealed two main themes, i.e., major reasons or barriers for not availing the rehabilitation services and challenges faced by parents in taking care of adolescents with ASD, and corresponding subthemes, as provided in Table 2.
Overview of Themes and Subthemes Identified
Reasons for Discontinuing Rehabilitation Services
Caregivers described a range of reasons for the discontinuation of the rehabilitation services, which are discussed in forthcoming sections.
Logistic Difficulties
Caregivers stated logistic reasons like distant rehabilitation center, difficulty in dropping and bringing the child back home, difficulty staying at a distant place (from home) to avail rehabilitation services, and long wait time, e.g., one of the parents had to wait for six months before starting the therapy, though they were interested in continuing the rehabilitation services.
“Because of travelling issue, I couldn’t take him to special school afterward. Reaching there and getting back on time was all difficult for me …” (M11)
Need for the Parent to Accompany the Child
Accompanying the child to the rehabilitation center was difficult for working parents and mothers with household responsibilities, who also had to attend to the needs of younger siblings or old parents. As in the case of participant M6, the child could not be sent to school unaccompanied because of repeated seizures, which the mother believed would be troublesome for the teachers to handle. The parents, too, could not accompany the child to the special school; hence, they stopped the services. Parents had to spare time in the midst of their busy schedules, as rehabilitation centers and special schools demanded the parents be with the child all the time, which was not feasible.
“To whichever school we took him, whenever we asked, they informed that the child cannot attend the therapy or the school without parent…told me to be with him throughout the school time…” (M8)
Difficulty for Parents and Service Providers in Handling the Child in Rehabilitation Centre
Many parents expressed difficulty handling a child with ASD as a major reason for discontinuing the rehabilitation services. Behavioral issues, toileting issues, health issues like irritable bowel syndrome, sleep disorder, and frequent seizures were some of the major challenges faced by the parents, making it difficult for the parents and service providers to manage the child, which ultimately led to the discontinuation of rehabilitation services.
“His condition is such that he cannot be left in the school alone because he falls down following seizure… That being the case, it might be difficult for the teachers to handle him in such situations…” (M6)
A mother explained an incident when her child with ASD became unmanageably violent on the way to the special school, after which the child was not sent to the rehabilitation center. Another parent stated that because of the sleep disorder experienced by the child, it was difficult for the mother to take him for therapy on time, which often resulted in the cancellation of the sessions and eventually led to the discontinuation of therapy. A few parents (M4 and M8) reported that the toileting and behavioral issues were unmanageable such that the child could not be sent to school or anywhere outside. A mother recollected an incident when special educators in her son’s class resigned from their job because of the child’s behavioral and toileting issues. Another parent eventually had to discontinue rehabilitation as the child’s behavior deteriorated remarkably following the relapse of epilepsy. One of the mothers was interested in restarting intervention, yet worried if the new therapist would be able to handle the child like the previous therapist.
Financial Difficulties
Financial problem was yet another reason for discontinuing the rehabilitation therapy or not enrolling children with ASD in any centers because charges for speech therapy and occupational therapy were fairly high and unaffordable for many parents (M4 and M6). It was an enormous expense for the family to meet the cost of the individual therapy session(s) with the father’s low income. Some parents expressed financial constraints to meet travel expenses and accommodation costs, in order to avail of therapy at distant places, in addition to the therapy charges.
“With father’s low-income work, it is difficult for us to meet daily therapy charges, and expenses are unaffordable for us…” (M6)
Family Commitments
Caregivers expressed their involvement with household commitments resulting in an inability to spare time for attending rehabilitation services. One of the mothers reported that she had to discontinue the child’s therapy after delivering the second child. Another mother stated that it was difficult for her to take her child to a special school as she had to care for her sick mother-in-law at home.
“I was the only one there to take care of his sick and bedridden mother… So I couldn’t manage to take him for therapy…” (M6)
Lack of Satisfaction with the Existing Treatment
Parents narrated varied experiences and levels of satisfaction with the treatment and rehabilitation team. Many parents (M1, M4, and M7) were not satisfied with the services the child received at the rehabilitation center and reported enrolling their child in the rehabilitation center as a bad decision. Parents expressed concern about the child not getting enough attention from the service providers. Another mother (M1) stated that contrary to her expectation (of the child getting individual attention), the special educator was available only once a week. One parent expressed her discontent over the treatment while expecting to have a rehabilitation professional who would be able to handle the child properly. She also had expectations of learning more about a few of the Alternative and Augmentative Communication (AAC) programs, which were not met.
“I thought he would get more attention at special school than normal school, and special educators would be more understanding and skilled to handle such children with special needs. With all these thoughts, I put him in a special school. What to say…Most of the time, he was left unattended at special school…special educators and administrators will be engaged in their work…not every child was getting individual attention. Further, there was no training provided…I used to even get phone calls from the school, complaining that he hurts other children at the special school…” (M1)
Lack of Improvement
Nearly all participants echoed the lack of improvement in the child’s condition as another concern. Many of the parents (F3, M4, M8, and M11) decided not to take the child to the rehabilitation center as they found no improvement in the child’s life skills. A caregiver (M1) concluded that enrolling the child in a special school was of no help to the child, as there was no reduction in the child’s tantrums after he was enrolled in the special school and, therefore, discontinued. Another mother (M7) felt that all therapy efforts tried for the child were in vain (after the child showed regression), so she had no desire to continue therapy for the child. Another parent (M8) felt sad as no improvements were seen for her child while treatment was beneficial for other children with ASD.
“It was so sad that there were only negative results from all the treatments.” (M8)
Adverse Effects of Medication
Many parents reported adverse effects of medications, including sleeplessness, drowsiness, aggravation of acidity issues, weight gain, and irritability, which made some parents discontinue the medications. A parent (M2) reported that instead of improving the hyperactivity in her child, the medication caused drowsiness and hindered the child’s participation at the rehabilitation center. Another parent (M11) stopped taking her child to the special school as he was not being engaged in any activities at school because of drowsiness as a result of the medication.
“There was no benefit out of medicines… while given tablets and medicines, she used to get tired, and most of the time she sleeps in special school…” (M11)
Parenting Challenges in Taking Care of the Child
This theme is about the experienced parental challenges and the need to constantly look after adolescents with ASD. The following sub-themes emerged in relation to this theme.
Difficulty in Managing the Changes During Adolescence
Parents felt anxious as the child reached adolescence, and it was difficult for the parents and children to cope with the physical and mental changes that occur during adolescence. Parents of female adolescents with ASD (F3, M5, M10, and M11), in particular, stated that their children are not capable of maintaining personal hygiene themselves during the time of menstruation. A mother (M5) mentioned that her child would not cooperate with her in maintaining personal hygiene, and she often had to change the child’s dress several times while she showed aggressive behaviors, temper tantrums, and sensory issues. Few of the parents (M1 and M8) stated that their adolescents with ASD would engage in sexual behaviors, like masturbating, in inappropriate situations, which was very embarrassing for the parents.
“She tears apart the sanitary pad into pieces and throws it somewhere…she knows nothing about it…she smears it over her face and puts in her mouth …” (M5)
Parents reported varied experiences in making their children understand the bodily changes of adolescence. A few parents tried to make the adolescent aware of bodily changes following secondary sexual development and the need to keep personal hygiene. Two of the parents (M2 and M12) reported that their children showed curiosity related to the bodily changes (like hair growth on the face and legs) while they explained it to the children.
Disruptive Behavior of the Child
Most of the parents expressed their concerns when adolescents with ASD showed disruptive behaviors like aggressiveness, temper tantrums, crying for no apparent reason, inappropriate laughter, noncooperativeness, self-injurious behaviors, and hurting others. Some of the parents (M1, M5, M7, and M8) reported that the child’s behavioral issues worsened when they reached adolescence. Another parent (M9) rather observed positive changes in the child’s behavior during adolescence, such as reduced temper tantrums and hurting others, being considerate toward the younger sibling, and even starting to control his anger and aggressiveness (M1).
“He makes the other kids at the school cry by pushing them away, hitting their head against the wall or floor, and pinching them …and he starts laughing at them when the kids cry …” (M8)
According to the parents, toileting issues were quite difficult to manage and, at times, embarrassing. The adolescents were reluctant and noncooperative to clean themselves because of sensory issues, which was a matter of worry for many parents.
Some parents (M4, M8, and M10) conveyed their anxiety over behaviors such as getting undressed in inappropriate situations and hurting others. A parent (M4) expressed her anxiety regarding planning for the next child, as her adolescent with ASD hurts other children. Two parents (M1 and M8) reported issues such as anger; increased tantrums; behaviors like jumping around, running around, screaming, and clapping hands, and showing aggression when the child feels discomfort because of acidity issues or indigestion. Another parent (M4) expressed her distress over the child’s noncooperation with grooming, such that even barbers refused to cut the child’s hair and the mother had to groom him.
When discussing aggressive and disruptive behaviors, a parent (M8) informed that the child is so violent that two or three people are required to control him and bring him to the room; else, everything within his reach would be destroyed, and the child rolls on the ground if left outside. Many parents (F3, M4, M5, M8, M10, and M12) reported that adolescents with ASD showed self-injurious behaviors like head banging, self-biting, and putting their head in between doors when frustrated and emotionally overwhelmed. Some parents (M4 and M8) reported confining adolescents with ASD in a room to control them.
Difficulty to Manage the Child Outdoors
Caregivers expressed differences in opinion in terms of handling adolescents with ASD outdoors. While most parents (M4, M6, M8, and M10) hesitated to take their children out for social gatherings, some (F3, M5, M7, M11, and M12) believed in taking adolescents with ASD as other children, in spite of the difficulty in handling. Many parents (M4, M6, M8, and M10) reported that they stopped attending family functions because of embarrassment caused by disturbance to others or difficulty in handling them. One of the parents (M1) stated that she could not take her child with ASD outside after her second child was born, and if at all she took the children out, she had to take only one at a time.
“I can’t take him to any marriage functions, as he won’t sit still. He eats others’ food… It is so embarrassing for us.” (M4)
Associated Medical Condition of the Child
Most adolescents with ASD presented with comorbid medical conditions (like constipation, irritable bowel syndrome, gastroesophageal reflux disease, indigestion and acidity issues, urinary incontinence, and seizures) that needed attention from parents. Repeated seizures were one of the major causes of concern for parents. One parent (M8) reported that her child often develops diarrhea followed by seizure attacks. Comorbid psychopathologies like hyperactivity, anxiety, mood disorders, and even sleep disorders were seen. Often, the parents had to stay awake at night, felt tired the whole day, and felt helpless as it affected the sleep of others at home.
“Sometimes he won’t sleep at night. He won’t let me sleep; he walks all around and pulls all others out of bed…” (M4)
Worries About the Cognitive Abilities of the Child
Many parents informed that adolescents with ASD remained poor in their cognitive abilities like executive functions, theory of mind, logic and reasoning skills, and comprehension. A few parents (F3 and M8) felt that, although their child appeared to understand a few things, was ignorant at times. A parent (M9) felt anxious that her child could not understand what was right and wrong. Another mother worried that she could not identify any skills her child was good at.
“Sometimes, she answers our questions in 4-5 words utterance. After that, she starts speaking something else. Sometimes I feel that she has no difficulty understanding, but at some other times … she can’t understand….” (F3)
Parent Feels Embarrassed at Societal Responses
The parents believed that many people around were less understanding, showed unwarranted sympathy, and stared at their children. A parent (M4) reported that she was hesitant to take her child even to a relative’s house, as she felt embarrassed about the response from relatives toward the child’s behavioral issues. Furthermore, questions from others who are unaware of ASD were distressing for the parents (M1 and M11). Some people even believed that children with ASD are incapable of doing anything of their own. A mother (M10) recollected an incident where she felt miserable that her own family members accused her of being careless and unresponsive to her child’s injurious behaviors toward other children.
“I take my child only to my relatives’ house. No one seems pleased. Everyone used to stare at children like this and show sympathy. Not every parent might feel good at others’ sympathy…” (M8)
Comparison with Other Children Causes Emotional Turmoil
A parent (M9) expressed her sadness when she saw other children of her child’s age having fun and wished her child to be like them. A few parents (M4, M6, and M8) stated that they felt bad that, while most of the children with ASD at special school were able to do toileting with minimal support, their child could not. Another parent (M9) stated that she felt upset when other children did not involve her child with ASD while playing.
“Other children say… go away from here…you don’t have to come with us to play…I feel sad that if my child had been like them, he could have played with them…” (M9)
Parent Apprehensive About Child’s Uncertain Future
Parents reported that they were worried about the future of their child. Parents were anxious about what would happen to their children in their absence and how long they would remain healthy enough to look after their children with ASD. Some parents worried about the safety issues as the children with ASD grew as adolescents. One of the mothers (M2) pointed out that she felt anxious when she thought about her child’s future, marriage, employment, and independent life. Another parent (M1) said that she became more apprehensive about her child’s future when she understood more about autism.
“After a period of time…gradually I could understand that this is such a condition due to which most probably his future would be lost …”
Insecurity Regarding the Safety of the Child
Many parents feared about the child’s security in public and hence would not leave their child alone. A few of the parents (M4, M7, M8, M9, and M10) mentioned that they never left their child with ASD with anyone and used to accompany the child always, as they worried about the child’s safety. Two of the parents (M4 and M7) shared their fear about the child’s obsessiveness with vehicles and that the child would run toward the road whenever he heard the sound of any vehicle, with little regard for safety.
“He likes to travel in vehicles. He sits in an autorickshaw although it is someone else’s. He will go with anyone…that’s what I’m afraid of…” (M4)
Absence of Guidance by Service Providers
Nearly all parents in the study reported not having received any guidance from the rehabilitation centers regarding strategies to cope with the physical and psychological changes in adolescents with ASD. A few parents (M4 and M11) had not received any sort of guidance from service providers regarding the diagnosis of autism in their child. Other parents (M1 and M10) came to know about the diagnosis of ASD very late because of the delay in receiving a referral from the consulting medical doctor. In the case of another parent (M8), although the doctor had diagnosed the child at the age of three years, neither of the parents was informed.
Two parents (M11 and M12) got to know about the availability of rehabilitation for children with ASD very late. A few others (M1 and M4) had no clue as to what could be done to improve the child’s communication skills, as they were misguided by the consulting doctor that there was no treatment to improve the child’s condition. Another parent (M4) expressed her surprise when she got to know about speech and language therapy during the study and the difference it can cause in a child’s communication skills.
“Although regular consultation by the doctor was done from 2-3 years of age, it was only at the age of eight years that the doctor told that the child requires training…” (M10)
Parent Losing Confidence
A few parents (M1 and M8) reported feeling apprehensive because of the increase in the child’s aggressive behavior as the child reached adolescence. A parent (M4) indicated that she felt hopeless as the adolescent with ASD could not carry out basic life skills like dressing on his own. One of the parents (M6) expressed her helplessness regarding the lack of improvement in the child’s condition. Another parent (M10) stated that, unlike earlier, her confidence in dressing and taking the child out has come down because of the child’s physical appearance.
“Isn’t the disorder of autism a special disease which is very difficult to handle?” (M6)
Discussion
This study provided a descriptive account of primary parental perspectives on reasons for not availing of rehabilitation services for adolescents with ASD and potential access barriers to rehabilitation services. The results also revealed several challenges in the parenting of adolescents with ASD.
Results on reasons for discontinuing rehabilitation services provided a broader understanding of various reasons why families of adolescents with ASD failed to continue rehabilitation services. The financial difficulties as one reason to discontinue rehabilitation services showed convergence with the literature on financial constraints as an access barrier to avail rehabilitation services.2,6 Specific financial difficulties faced by the parents in this study included difficulty to meet the daily therapy charges, travel/accommodation expenses as they are forced to hire a private vehicle owing to the child’s behavioral issues, the cost to avail rehabilitation at distant places, and being unable to go for work in order to look after the child. The financial difficulties reported in the literature, however, were difficulty in getting insurance reimbursement, absence of a transition plan for adolescents with ASD, 5 and inability to afford the payments for services and debts. 5 The difference in the nature of financial difficulties could be attributed to the lack of insurance schemes covering rehabilitation services for children with ASD in India. The government schemes on monthly financial assistance, aids, and devices are not sufficient enough to cover the regular expenses of the rehabilitation services. Further, there are only a few government-run schools for children with special needs to avail of free services. Other barriers to avail of medical and rehabilitation services for adolescents with ASD, as documented in the literature, are remaining on a waiting list for a long time and unavailability of services. 6 This was also the case for one of the participants in our study, where the parents were asked to wait and start therapy after six months. This particular factor reflects the lack of available rehabilitation services and personnel for children with special needs. Unawareness about the condition of ASD and its rehabilitation, along with lack of guidance (as apparent from the responses of a few caregivers), was another reason for not availing of rehabilitation services among families of adolescents with ASD. 16 Evidence-based intervention models17,18 exist for children and families of ASD in the Indian context, yet there is a gap between research and practice.
Other reasons that emerged from this study included logistic difficulties, difficulty in handling the child, the need for the parent to accompany the child, and family commitments. These issues restricted the caregivers from attending rehabilitation services for their children even though they wished to. Dissatisfaction with the existing treatment, lack of improvement, and adverse effects of medications were other factors reported by some of the parents as reasons to discontinue rehabilitation. While these findings reflect the quality of services provided to adolescents with ASD, it also reveals insufficient knowledge in caregivers, thereby leading to unrealistic expectations.
Findings on the parenting challenges theme indicated difficulty in managing the changes during adolescence along with disruptive behaviors, in the absence of availability of proper guidance by service providers. Apprehension about the child’s uncertain future, constant worry about the child’s insecurity, disruptive behaviors, and associated medical conditions of the children were a few enduring challenges faced by the parents of adolescents with ASD. For some parents, comparison with children of a similar age group caused emotional turmoil. Some parents reported feeling embarrassed at societal responses, indicating the public’s lack of awareness and acceptance of the special children. A few parents reported losing confidence, revealing their anxiety and mental status. Our findings were in agreement with the literature reporting perceived burden, depression, and stress in families of children with ASD.11,19–22
Our findings provide a first-hand, in-depth account of parental perspectives on reasons for discontinuing medical and rehabilitation services in the cultural context of India. It has several implications for authorities and professionals in the educational and mental health rehabilitation service sector. There is a need for the rehabilitation sector to address these issues by improving the training facilities for adolescents with ASD, training professionals to address the needs of families with ASD, conducting awareness programs for parents and health care professionals about the available rehabilitation services, and addressing the physical and mental health of caregivers. Additionally, these results help policymakers identify the needs and plan for the welfare of adolescents with ASD. Our results further emphasize the need for scaling up mental health services for the families of adolescents with ASD. 22
One of the limitations of this study was that the diagnosis and severity of ASD were based on secondary data. Likewise, the diagnosis of comorbid psychopathology was parent-reported. The direct assessment was, however, not feasible, given the pandemic and lockdown during the study period. The findings of the study are applicable to the Indian context. However, differences may be noticeable based on the geographical area and socioeconomic status of the sample.
Conclusion
This study provided a range of reasons for the discontinuation of rehabilitation services (such as logistic difficulties, financial difficulties, family commitments, difficulty handling the child, lack of satisfaction with the existing treatment, and lack of improvement) and potential barriers to avail rehabilitation services and parenting challenges (viz. difficulty in managing the changes during adolescence, disruptive behaviors of the child, difficulty to manage the child outdoors, associated medical conditions of the child, and worries about the cognitive abilities of the child) relevant to the Indian context. These findings have implications for professionals in the educational and mental health rehabilitation sector as well as policymakers to support rehabilitation services and improve the quality of life for families of adolescents with ASD.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.