
Abstract
Background:
Inflammation may play an important role in the pathogenesis of schizophrenia and related psychotic disorders. This study aimed to measure the inflammatory marker (serum prolactin, serum cortisol, C-reactive protein [CRP], erythrocyte sedimentation rate (ESR), total leucocyte count, and differential leucocyte count) in drug naïve patients of the first episode of acute and transient psychotic disorder (ATPD) at baseline and their alterations after three months of antipsychotic treatment.
Methods:
This prospective study estimated the change of inflammatory biomarkers in patients with ATPD over three months, along with the change in psychopathology and global functioning. Attempts were taken to compare the trend of change in inflammatory biomarkers with clinical improvement.
Result:
A total of 157 patients with ATPD were screened to recruit 78 patients, of which only 33 patients were followed up till three months from the point of recruitment. More than three-fourths of the patients improved significantly during the brief follow-up period. Patients who improved substantially with antipsychotic drug treatment had a significantly lower age and age at the onset of psychiatric illness. The patients who improved also had a significant reduction in total leucocyte count, absolute neutrophil count, and neutrophil-to-lymphocyte ratio from baseline to three-month follow-up. Duration of untreated illness had a significant positive correlation (P = .042; r = 0.401) with the ESR.
Conclusion:
Inflammatory biomarkers are raised in drug naïve patients with ATPD, which improves with antipsychotic drug treatment, indicating a possible role of inflammation in the pathogenesis of ATPD.
Improvement of psychosis in the short term was associated with a significant reduction in total leucocyte count, absolute neutrophil count, and neutrophil-to-lymphocyte ratio. Duration of untreated illness had a significant positive correlation with the erythrocyte sedimentation rate. Response to antipsychotic drug treatment in ATPD was associated with corrections in the alterations in the inflammatory markers.Key Messages
Over the past few decades, research evidence regarding the role of inflammation in psychiatric disorders has been accumulated. Studies evaluated the role of inflammatory reactions in patients with schizophrenia and related psychotic disorders.1–4 Evidence supports that inflammation has a determining role in the onset as well as the progression of schizophrenia and related psychotic disorders, and the inflammatory process is mostly mediated by stress and infection. 5 These inflammatory processes are capable of activating the microglial activity, which subsequently produces alterations in the neuro-circuitry in the brain, resulting in the onset and progression of psychosis. 6 The chronic inflammatory changes in schizophrenia are hypothesized to impair cerebral blood flow by compromising the micro-vascular system. 4 In comparison to healthy controls, patients with first-episode psychosis have increased levels of pro-inflammatory cytokines and increased peripheral inflammatory cells. Simultaneously, there is a decrement in the anti-inflammatory mechanisms in the body. 7 In the first episode of psychosis, it was found that the inflammatory and pro-inflammatory mediators determine the expression of an active form of brain-derived neurotrophic factor (BDNF) receptor in peripheral blood cells. As there is improvement in psychosis following antipsychotic treatment, there is a reduction in inflammation and decreased expression of the active BDNF receptors (TrkB-FL). 8 C-reactive protein (CRP) is considered to be a sensitive immune marker of schizophrenia. 4
The neutrophil-to-lymphocyte ratio is considered a proxy marker of inflammation. 1 In the symptomatic phase of psychosis, the neutrophil-to-lymphocyte ratio remains elevated, which gradually reduces as the patients approach remission. This ratio was found to be significantly associated with psychosis as a biomarker even after controlling the confounders like—body mass index, age, antipsychotic medications used, and smoking status. 1 Like neutrophil-to-lymphocyte ratio, monocyte to lymphocyte ratio is also a sensitive marker of inflammation. These two ratios also determine endothelial function and are considered predictors of cardiovascular mortality in schizophrenia. 9 Higher monocytes were significantly associated with higher pulse pressure and rate pressure product. 9 Abnormality in the hypothalamic-pituitary-adrenal axis has been reported in psychosis. Evidence supports that there is an abnormality in the level of cortisol in drug naïve patients with first-episode psychosis. 10
Some evidence supports that even drug-naive patients with schizophrenia and related psychotic disorders have elevated levels of serum prolactin in comparison to healthy controls. 11 Hyperprolactinemia is also a side effect of antipsychotic medications used in the management of schizophrenia and related psychotic disorders, which are attributed to sexual dysfunction, menstrual irregularities, and galactorrhoea. 11 Both cortisol and prolactin determine the pathogenesis and clinical manifestation of psychotic disorders. 12
Here, we attempted to see changes in inflammatory markers (serum prolactin, serum cortisol, CRP, erythrocyte sedimentation rate (ESR), total leucocyte count, and differential leucocyte count) in drug naïve patients of the first episode of acute and transient psychotic disorder (ATPD) at baseline and their alterations after three months of antipsychotic treatment. We hypothesized that drug-naive patients with acute transient psychotic disorders have decreased levels of serum prolactin and increased levels of inflammatory markers (CRP and Serum Cortisol), which normalizes with antipsychotic treatment.
Methods
A prospective study designed to assess blood biomarkers in acute transient psychotic disorders during illness over a three-month follow-up period. Ethical approval was obtained from the institutional ethics committee, and the study was conducted between November 2018 and September 2019. Patients attending the Psychiatry outpatient department of a tertiary care hospital in Northern India were enrolled in the study and met the inclusion criteria. Adult drug naïve patients (age more than 18 years) with a diagnosis of acute transient psychotic disorders (ATPD) as per ICD-10 DCR, who were cooperative for assessment and consented to participate in the study, were recruited to the study. Patients having any other psychiatric illness (both current and past), except tobacco use disorder, pregnancy, and lactation, were excluded from the study.
Additionally, patients with any acute inflammatory medical condition or medical morbidity that requires immediate attention were excluded from the study. Patients were regularly followed up for a period of three months from the point of recruitment. The monthly follow-up was done to look for the evolution of psychopathology, which may indicate any other diagnosis and development of any medical abnormalities. Assessment of inflammatory markers was done at two points (baseline and three months) only. Any patient who was non-adherent to the prescribed psychiatric treatment or who developed a medical illness during the follow-up period (at least within one month before the second assessment) or received some medications that may alter inflammatory biomarkers were removed from the final analysis as they were potential confounding factors. The sample size estimation was done using the G power software. The following parameters are taken into account while estimating the sample size:
Analysis: A priori: Compute required sample size
Input:
Effect size f
=
0.25
α err prob
=
0.05
Power (1−β err prob)
=
0.80
Number of groups
=
1
Number of measurements
=
2
Corr among rep measures
=
0.5
Nonsphericity correction ε
=
1
Output:
Noncentrality parameter λ
=
8.5000000
Critical F
=
4.1392525
Numerator df
=
1.0000000
Denominator df
=
33.0000000
Total sample size
=
34
Actual power
=
0.80777
Considering a dropout of 10%, the final sample calculated was 38.
A semi-structured proforma was used to collect socio-demographic data and clinical history. Mini international neuropsychiatric interview [M.I.N.I. 6.0] 13 was used to screen other psychiatric illnesses. The brief psychiatric rating scale (BPRS) was used to assess the severity of psychotic episodes.14,15 The Clinical Global Impression-severity (CGI-S) and Clinical Global Impression-improvement (CGI-I) were used to measure the disease severity and clinical improvement, respectively.16–18 The blood sample was taken to estimate serum cortisol, serum prolactin, serum CRP, ESR, total leucocyte count, and differential leucocyte count. After the baseline investigations, patients were started on antipsychotic medications (olanzapine 10–20 mg/day or risperidone 4–6 mg/day) and benzodiazepine (lorazepam 1–2 mg/day) as per the need. Re-estimation of blood biomarkers was done after three months, along with the administration of the tools that were applied at baseline to evaluate the psychopathology. The method used for the estimation of serum prolactin and serum cortisol was chemiluminescence immunoassay. CRP-turbilatex is the quantitative turbidimetric test for the measurement of CRP. Wintrobe’s method was used to estimate the ESR.
Statistical Analysis
Statistical analysis was done by using Statistical Package for the Social Sciences (SPSS) version 18.0. The Shapiro–Wilk test was applied to check whether the data was parametric or non-parametric. The baseline parameters and the three-month follow-up parameters were compared by using a paired t-test. Mann–Whitney U test was applied to compare the parameters of patients who improved at three months versus patients who remained symptomatic. Wilcoxon signed-rank test was used to compare the baseline parameters with a three-month follow-up. Spearman’s rank correlation test was used for the correlational analysis. A P value of <.05 was considered statistically significant.
Result
A total of 157 patients with a diagnosis of ATPD as per ICD-10 DCR diagnostic criteria were screened. A total of 79 patients were excluded, of which the major reason for exclusion was a history of ATPD (n = 54). The other reasons for exclusion were already on antipsychotic medication treatment (n = 17), the presence of medical morbidity (n = 5), and pregnancy (n = 3). Additionally, 45 patients dropped out from the final analysis due to being lost to follow-up, withdrawing consent, or being non-adherent to medications, making the final sample of 33 patients. At the end of the three-month follow-up, 26 patients improved clinically with antipsychotic drug treatment.
In contrast, seven remained symptomatic, and their diagnosis changed to either affective psychosis (n = 5, Severe depressive episode with psychotic symptoms) or non-affective psychosis (n = 2, Other non-organic-psychotic-disorder). There was no difference in the type and dose of antipsychotic medication used between the two groups. None of the patients developed any major side effects of the medications. However, the commonly reported minor side effects were increased sedation, weight gain, and increased appetite (in 10 out of 33 patients). Those who improved with antipsychotic drug treatment retained the diagnosis of ATPD.
In contrast, for those who remained symptomatic at the end of three months, their diagnosis was changed as the ICD-10 DCR diagnostic criteria consider the diagnosis of ATPD if the symptoms are less than three months for most sub-categories of ATPD (diagnosis of ATPD with schizophrenia-like symptoms, changes to schizophrenia, if the symptoms persist beyond one month). 19 Table 1 summarizes the socio-demographic and clinical characteristics of the patients of ATPD who improved at three months versus those who remained symptomatic. Table 2 summarizes the change in symptom severity and blood inflammatory markers between the time of enrollment into the study and the three-month follow-up period. Table 3 summarizes the association of clinical variables with mean change of blood biomarkers.
Socio-demographic and Clinical Characteristics of Patients Who Retained the Diagnosis of ATPD (n = 26) and Whose Diagnosis Changed (n = 7) at Three Months Follow-up.
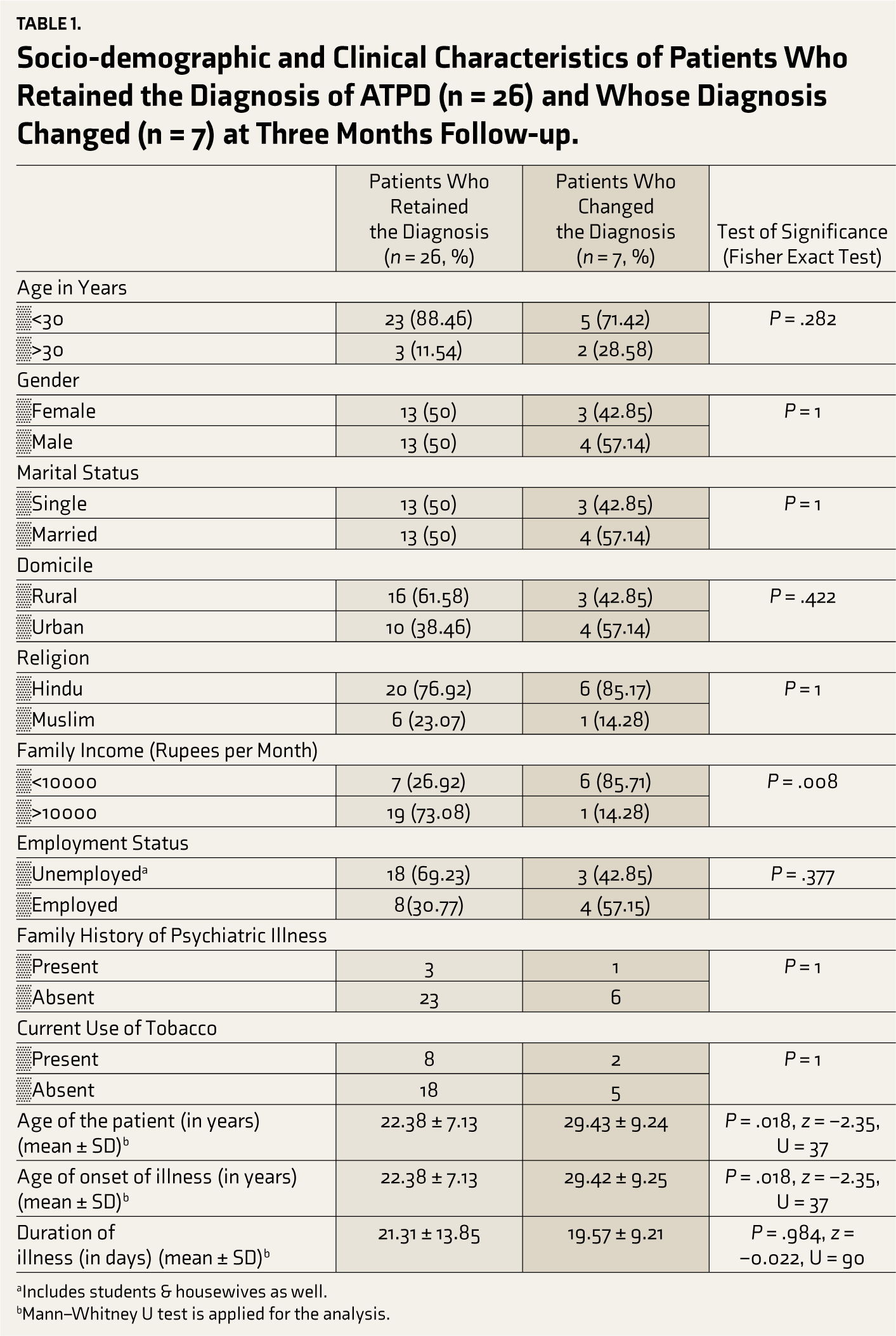
aIncludes students & housewives as well.
bMann–Whitney U test is applied for the analysis.
Comparison of Symptom Severity and Blood Markers at Baseline Versus Three Months in Patients Who Retained the Diagnosis of ATPD (n = 26).
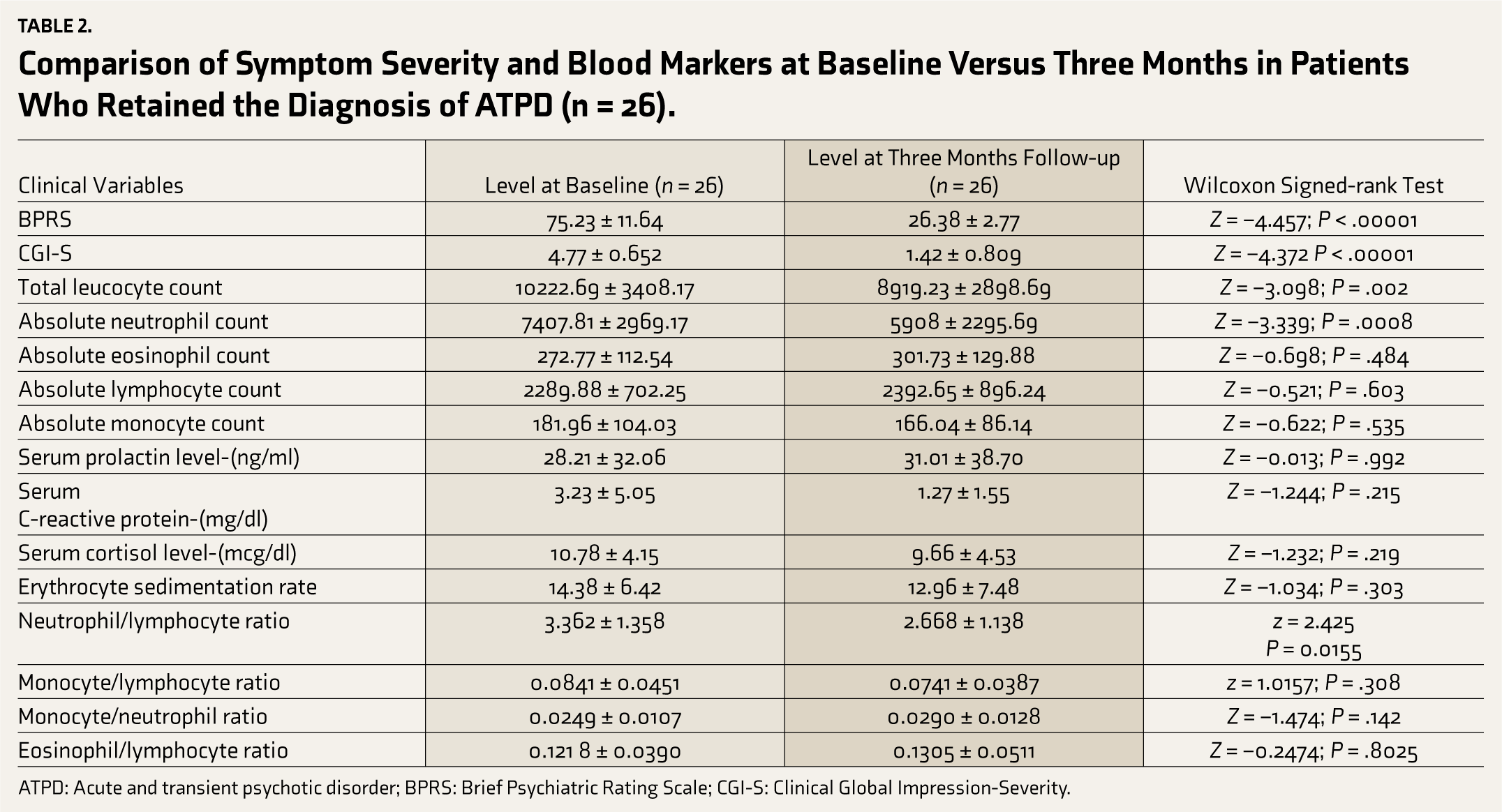
ATPD: Acute and transient psychotic disorder; BPRS: Brief Psychiatric Rating Scale; CGI-S: Clinical Global Impression-Severity.
Correlationa Between Clinical Variables with Mean Change of Blood Biomarkers (n = 26).
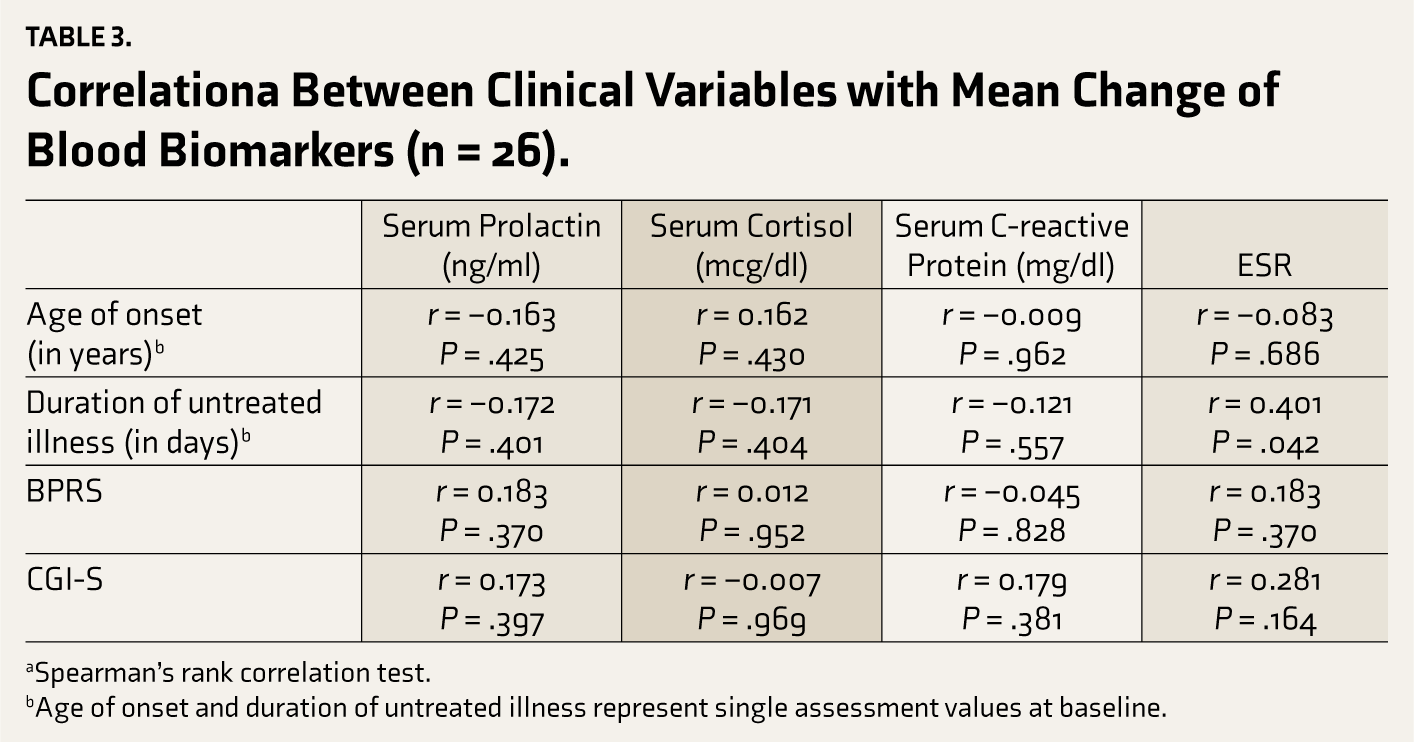
aSpearman’s rank correlation test.
bAge of onset and duration of untreated illness represent single assessment values at baseline.
Discussion
This study gives a brief overview of basic markers of inflammation over a short follow-up of patients with ATPD. Additionally, it gives insight into changes in the parameters of inflammation in recovery from ATPD. In our study, among the 157 screened patients, 54 (34.4%) were excluded due to having a past history of ATPD. It indicates that nearly one-third of patients diagnosed with ATPD in the index episode had a history of ATPD. Similarly, in short-term follow-up in the longitudinal course of the first episode of ATPD, 78.8% (n = 26) recovered, retaining the diagnosis of ATPD, whereas the remaining 21.2% remained symptomatic with the change of diagnosis to affective psychosis or schizophrenia-like psychotic disorders. An earlier study from India reported that about 14.28% of patients with ATPD had a past history of ATPD, and nearly 66.3% retained the diagnosis of ATPD at the end of three three-month follow-ups. 20 During long-term follow-up, the recurrence rate of ATPD may reach as high as 45.2%, as reported by a study on the Hong Kong population. 21 The latest systematic review and meta-analysis supports the diagnostic shift and risk of recurrence in ATPD, 22 with the majority of recurrences in the first two years following the initial episode. 23
The age of onset of illness among patients with ATPD who recovered completely was significantly lower than that of those who remained symptomatic at the end of three months of follow-up. However, other similar studies report contrary findings, mentioning an early age of onset associated with poor or slow response. 24 Our findings could be due to the small sample in the comparator group (those who remained symptomatic over the three-month follow-up period).
Inflammation may be associated with psychosis. It has been reported that fever is a common precipitating factor associated with the onset of ATPD.24–26 Several research studies reported an increase in pro-inflammatory and inflammatory cytokines like interleukins, tumor necrosis factor-alpha, and tumor growth factor in patients with ATPD and schizophrenia in comparison to healthy controls.25,27,28
Improvement in inflammatory markers has been reported in patients with schizophrenia and ATPD, with improvement in psychotic symptoms. 29 A recent systematic review reported that inflammatory markers like interleukin 6 (IL-6), interleukin 10 (IL-10), and CRP predict the outcome of psychosis. 30 Persistent high levels of IL-6 and CRP are associated with the persistence of symptoms of psychosis and poor outcome, whereas the increased level of IL-10 is associated with better improvement of symptoms of psychosis. 30 In our study, we found no significant improvement in the level of CRP from baseline to three-month follow-up. However, there is a significant improvement in symptoms of psychosis.
Additionally, we did not find any significant correlation between the mean reduction of symptoms and severity of psychosis and the mean reduction in the level of CRP. It might be possibly due to the differential relationship of inflammatory markers with ATPD and schizophrenia. The ATPD being an acute form of psychosis, and schizophrenia, being a chronic form of psychosis, may have different immunological underpinnings. Evidence supports that the neutrophil-lymphocyte ratio in first-episode psychosis who are drug naïve is significantly higher than healthy controls. 31 An earlier Indian study reported that the neutrophil-lymphocyte ratio is a sensitive marker for understanding the clinical progression of ATPD. 32 A high neutrophil-lymphocyte ratio is related to higher severity of symptoms and late recovery.32,33 Stefanovic et al. (2015) reported that treatment with antipsychotic drugs improves most of the non-specific inflammatory reactions (total leucocyte count, CRP) in first-episode schizophrenia. However, ESR remained unchanged in about 50% of the patients. 34 In our study, there was a significant reduction in the total leucocyte count, absolute neutrophil count, and neutrophil-to-lymphocyte ratio from baseline level to a three-month follow-up period among patients of ATPD who recovered completely. A significant positive correlation was found between the duration of untreated psychosis and ESR, which indicates that the longer the duration of untreated psychosis, the higher the ESR. It might be due to the persistence of inflammatory reactions when psychosis remains untreated, giving rise to an elevated ESR.
The small sample size is a major limitation of the study. Again, the follow-up period was short, and non-specific inflammatory markers were evaluated in the study. In a recent study, after controlling confounders inflammation like smoking, it was found that the drug naïve patients of first-episode psychosis have significantly higher total WBC count and neutrophil count in comparison to healthy controls. 35 Such confounders also could not be eliminated in our study. We were not able to exclude tobacco use disorder in our study due to its commonness, and it may alter the level of inflammatory markers. The comparison group (who remained symptomatic at the end of three months of follow-ups) was very small, so we avoided the comparison with the patients who recovered completely to eliminate arbitrary or random interpretations.
Despite its limitations, the study gives a clue that non-specific markers of peripheral inflammation can be used as biomarkers in ATPD. They can predict the symptom severity, recovery, and response to antipsychotic drug treatment. As the specific markers of inflammation like IL-2, IL-6, and IL-10 are very costly and not routinely performed in clinical settings to measure clinical improvements, one may consider the cost-effective non-specific peripheral markers to evaluate outcomes. Though tobacco use disorder could not be excluded, the distribution of tobacco use disorder in patients who retained the diagnosis and whose diagnosis changed at the end of follow-up was not statistically different. In the present study, it may not be possible to establish a causal link between specific antipsychotic medication and change in inflammatory markers as several other confounders may influence the change of the inflammatory markers. For example, concomitant use of other medications, nutritional factors, body immunity, and severity of psychopathology may influence the immune response and inflammatory marker levels. Future research may consider specific immune mediators (like IL-2, IL-6, IL-10) in a larger sample addressing all possible confounders with a long-term follow-up period to understand the intricate association of inflammatory biomarkers with the outcome of ATPD.
Conclusion
The ATPD is associated with alterations in inflammatory mediators, which may predict the outcome of ATPD, at least in the short term. Response to antipsychotic drug treatment in ATPD is associated with corrections in the alterations in the inflammatory markers.
Supplementary Material
The supplementary material for this article is available online.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethical Approval
The project was approved by the institutional ethics committee of King George's Medical University, Lucknow. Ethical approval reference number was: 93rd ECM II B-Thesis/P47, dated on 15-11-2018.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Informed consent was taken from all the patients or their caregivers.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.