
Abstract
Background:
Duration of untreated psychosis (DUP) is an important modifiable factor affecting schizophrenia outcomes. A dearth of research in India on untreated versus treated schizophrenia warrants further research.
Methods:
This was a longitudinal study in a tertiary hospital over 2 years. Inpatients diagnosed with schizophrenia (N = 116), aged 18–45, were divided into untreated and treated groups. Diagnostic confirmation, severity assessment, and clinical outcome were done using ICD-10 criteria, Positive and Negative Syndrome Scale (PANSS), and Clinical Global Impression (CGI) scale. Follow-up was done at 12 and 24 weeks. DUP was measured, and its association with the outcome was assessed.
Results:
Final analysis included 100 patients, 50 each of previously untreated and treated. Untreated patients had lower age and duration of illness (DOI), but higher DUP (p < .001). Treated patients showed much improvement on CGI-I at 12 weeks (p = .029), with no difference at 24 weeks. PANSS severity comparison showed no difference, and both groups followed a declining trend. In untreated patients, age of onset (AoO) was negatively correlated with severity (except general symptoms at baseline) at all follow-ups (‘r’ range = −0.32 to –0.49, p < .05), while DOI showed a positive correlation with negative and general symptoms at 12 weeks (r ~ 0.3, p < .05). Treated patients showed inconsistent and lower negative correlation between AoO and PANSS, with no correlation between severity and DOI. The mean sample DUP was 17.9 ± 31.6 weeks; it negatively correlated with education (r = –0.25, p = .01) and positively with PANSS severity (‘r’ range = 0.22 to 0.30, p < .05) at all follow-ups, especially negative symptoms. Patients with no or minimal improvement on CGI at 24 weeks had higher DUP (Quade’s ANOVA F[1,98] = 6.24, p = .014).
Conclusion:
Illness variables in untreated schizophrenia affect severity, which has delayed improvement than treated schizophrenia. Higher DUP is associated with negative symptoms of schizophrenia.
Illness variables in untreated schizophrenia significantly affect severity. Untreated psychosis has delayed improvement on short follow-up. DUP is associated with negative symptoms.Key Message:
Countless studies have been conducted on the outcome of schizophrenia. Factors affecting clinical outcome include socio-demographic profile, genetics, environment, antenatal CNS insults, premorbid personality, co-morbid physical conditions, duration of illness (DOI), duration of untreated psychosis (DUP), and caregiver attitude toward the illness.1–3 Among these, DUP stands as an important modifiable factor affecting outcome and social functioning, both short- and long-term. 4 This single factor has been sought for a reduction in remnant psychopathology via early intervention. 5 Despite advances in the field of mental health, numerous schizophrenia patients remain untreated for long. The World Health Organization found a treatment gap of 69%, which was even larger among low-income countries (89%). 6 Indian National Mental Health Survey 2015–2016 found a gap of 75.5% for schizophrenia and psychotic disorders. 7 Most previous research emphasizes untreated psychosis/schizophrenia, with only countable studies aiming at differences between previously treated and untreated patients. 8 Moreover, data from India is scarce. 9 Hence, the current research aimed to compare illness characteristics in previously untreated versus treated schizophrenia patients and assess the association between DUP and clinical outcomes in total patients and within groups.
Material and Methods
Study Setting and Design
This longitudinal study was done in the department of Psychiatry, Guru Gobind Singh Medical College and Hospital, a tertiary care government facility in Faridkot, Punjab, India. The catchment area includes urban and rural backgrounds, from within or nearby districts in south-western region of the state. Few patients present from other regions or states.
Study Population and Duration
The study was conducted on inpatients of the psychiatry ward, diagnosed with schizophrenia (F20). Patient enrolment was done from August 2017 to July 2019 (two years), and each patient was followed up for 6 months. The Institutional Ethics committee approved the study protocol.
Sample Size
Before commencement of the study, 30 consecutive patients (15 each of previously untreated and treated) presenting to psychiatry OPD, aged 18–45, diagnosed with schizophrenia (F20) were assessed for crude estimates of relevant illness variables. Along with routine evaluation (history and general physical and mental status examination), patients and/or their primary caregivers were enquired about DUP and clinical improvement after 4 weeks of treatment. Sample sizes were calculated:-

Taking confidence level of 95% and power of 80%,


where
taking
α
= 0.05 and
β
= 0.20,

Values were also put in g*power software v3.1, and Wilcoxon–Mann–Whitney tests (two groups) were conducted. The two-tailed sample size calculated was 49 each.
Hence, the final sample size was 102 (51 patients in each group). Convenient sampling was employed.
Inclusion Criteria
Psychiatric inpatients meeting the International Classification of Diseases (ICD-10) diagnostic criteria for schizophrenia (F20).
Subjects aged 18–45 years.
Subjects and/or caregivers who have given a written informed consent for the study.
Exclusion Criteria
Subjects with intellectual disability.
Subjects with a history of head injury.
Subjects with neurological, severe cardio-pulmonary, or other medical illnesses.
Operational Definitions
Untreated psychosis: Defined as never or still not having received any antipsychotic medication before the investigation. 8
Treated psychosis: Defined as once having received any antipsychotic medication before the investigation. 8
DUP: Duration in weeks from the emergence of the first psychotic symptom (hallucinations, delusions, or thought disorder) to the start of adequate antipsychotic treatment. 10
Study Procedure
At the start of study, a written informed consent was obtained from patients and/or their caregivers. Caregivers’ consent was sought only if the patient at the time of presentation did not have the capacity to consent. Following treatment, restoration of insight, and improvement in symptoms, patients’ consent was sought for the use of previous data and further participation in the study. They were selected as per the inclusion and exclusion criteria and evaluated for socio-demographic and illness-related variables. Diagnosis of schizophrenia (F20) was made as per ICD-10 diagnostic guidelines and confirmed by a consultant in the department. Further confirmation and assessment of the severity of psychosis was done using the Positive and Negative Syndrome Scale (PANSS), 11 a reliable and valid instrument. The patients were subjected to appropriate investigations justifying inclusion/exclusion criteria (complete blood counts, liver and renal functions, blood sugar, serum electrolytes, viral markers, electrocardiography, and chest X-ray; specific investigations like electroencephalography or computed tomography head, wherever required). Based on previous treatment received, patients were divided into two groups of previously untreated and treated. Relevant items from Nottingham Onset Schedule 12 were used to measure DUP, based on patient/caregiver interviews and old case records. Appropriate antipsychotic medication chosen as per the clinician’s assessment was started in all patients at baseline. The outcome of illness and treatment given were assessed using Clinical Global Impression (CGI) scale, including CGI-S and CGI-I sub-scales, measuring symptom severity and treatment response, respectively. 13 Depending upon feasibility, enrolled patients were followed up on a weekly to monthly basis to ensure treatment adherence. A reminder phone call was made to patients who missed their designated follow-up date, the next day. Patients who failed to follow up for more than a month were considered dropouts. Periods 12 and 24 weeks were designated follow-up periods when re-assessment on PANSS, CGI-S, and CGI-I scales was done.
Statistical Analysis
Data were entered in Microsoft Excel and analyzed using software IBM SPSS v23. Descriptive data are presented as frequencies and means ± standard deviations (μ ± SD) for categorical and continuous variables, respectively. Comparison of categorical variables was done using Pearson’s Chi Square test, with Bonferroni correction for multiple comparisons. Fisher’s exact test was used where the expected cell count (≥20% cells) was <5. Continuous variables were compared using the Mann–Whitney U and Quade’s ANOVA. Wilcoxon Signed Rank test was used for related samples. Correlation analysis was done using Kendall’s tau b test. p values of significance were determined, and values <.05 were considered significant.
Results
During the study period, 116 inpatients were diagnosed with schizophrenia (F20), all of whom were enrolled. Out of these, 64 and 52 were previously untreated and treated, respectively. After screening as per inclusion/exclusion criteria, five were excluded. Eleven patients dropped out. The final analysis was conducted on 100 patients, with 50 each of previously untreated and treated patients, at baseline, 12 and 24 weeks.
Untreated Versus Treated Schizophrenia
Socio-demographic comparison (Table 1) showed that previously untreated patients had a significantly lower age of presentation, lower total DOI, and higher DUP than previously treated patients (p < .001). No differences were found for other socio- demographic characteristics between the groups.
Socio-demographic Comparison of Previously Untreated Versus Treated Patients.
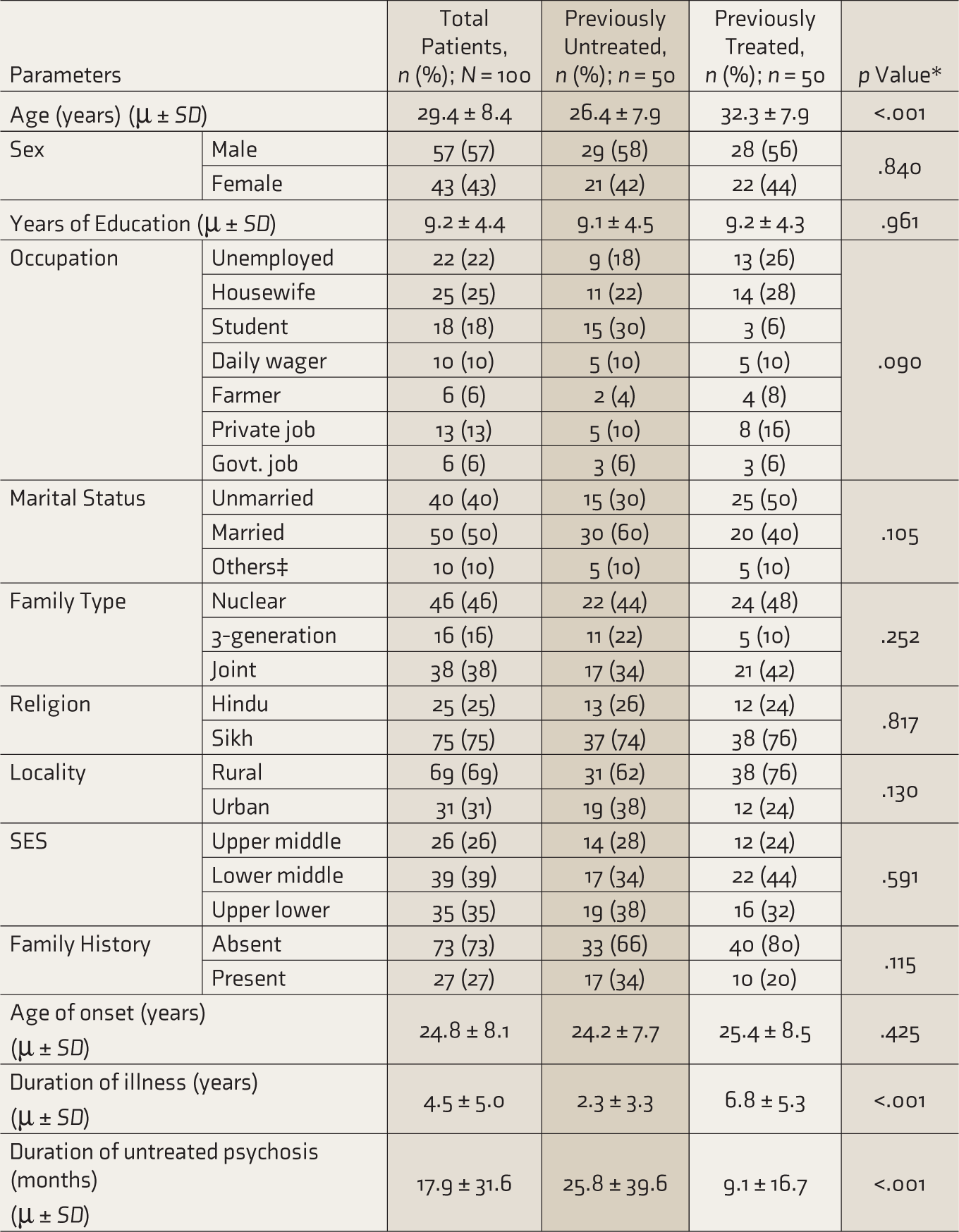
*Chi-square test used for categorical variables.
Fisher’s exact test used when expected cell count was <5.
Mann–Whitney U test used for continuous variables.
p values ≤ .05 considered significant.
Govt.: Government; SES: Socioeconomic status (as per modified Kuppuswamy socioeconomic scale).
‡Others include separated/divorced/widowed.
Comparison of illness variables of PANSS total, positive, negative, and general scores and CGI-S scores between the groups at baseline, 12 and 24 weeks (Table 2) showed no significant differences. However, significant improvement on CGI-I scale was found at 12 weeks, previously untreated patients being less improved (p = .029). A comparison of antipsychotics used at baseline showed that second generation antipsychotics (SGAs) were more used among untreated patients, while a combination of first generation antipsychotics (FGAs) and SGAs were more used in treated patients (p = .038). At 12 and 24 weeks, however, there was no difference. There was no difference in Olanzapine (OLA) equivalent dose at any follow-up (median ~ 9.5mg–10.0mg).
Comparison of Illness-related Variables among Previously Untreated Versus Treated Patients at Baseline and Follow-ups.
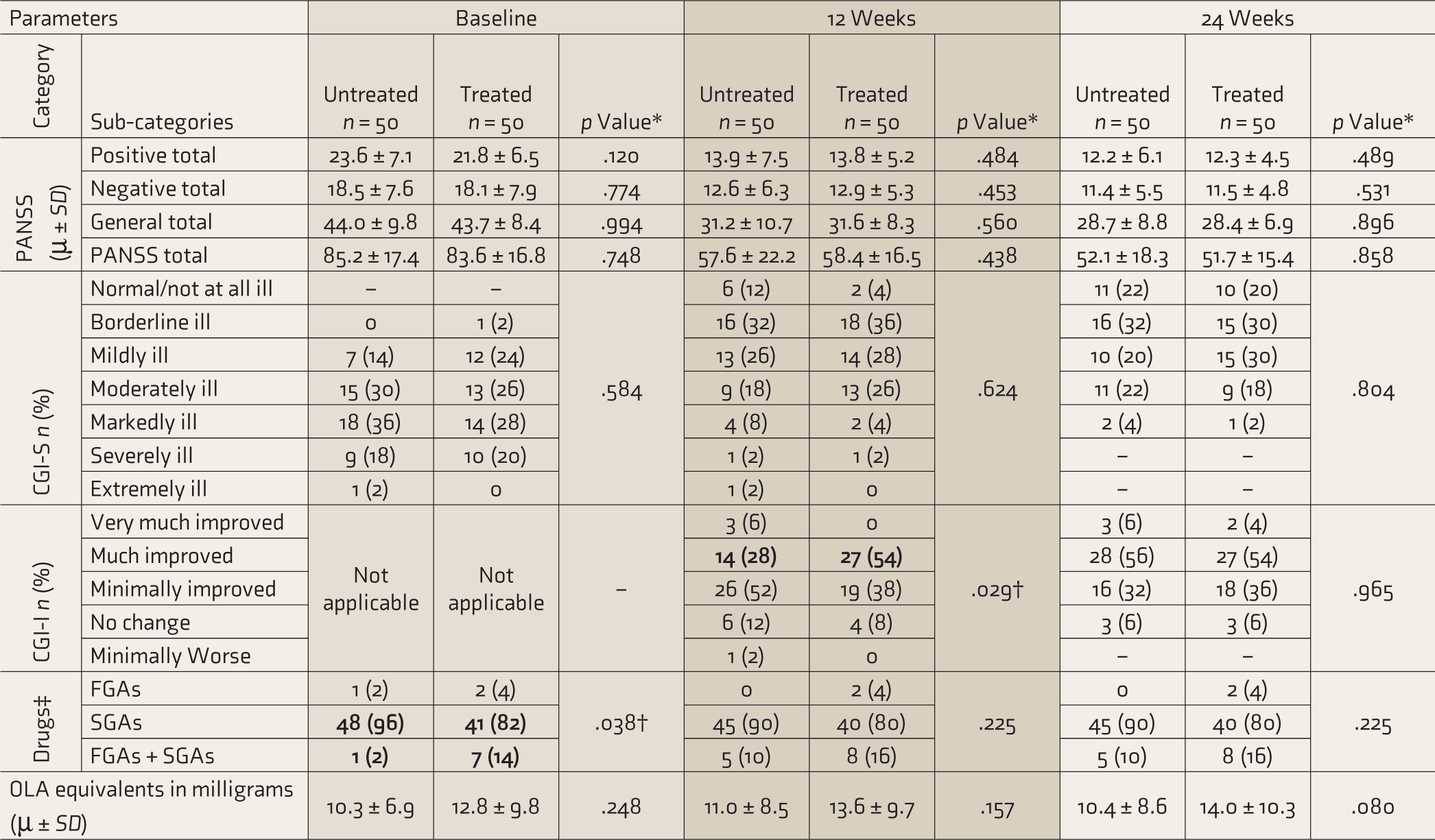
*Fischer’s exact test used for categorical variables.
Mann–Whitney U test used for continuous variables.
p values ≤ .05 considered significant.
†Adjusted p value as per Bonferroni correction showed significant difference for the categories made ‘bold’.
‡FGAs: First generation antipsychotics; SGAs: second generation antipsychotics; PANSS: Positive and Negative Syndrome Scale; CGI: Clinical Global Impression; OLA: Olanzapine equivalents of antipsychotics calculated by the minimal effective dose method. 14
Correlation analysis of severity with illness variables (Table 3) showed that in previously untreated patients, except for general symptom scores at baseline, lower age of onset (AoO) of psychotic symptoms was associated with higher total, positive, negative, and general symptoms at all follow-ups (p < .05). PANSS total, negative, and general symptom scores also showed a weak-moderate positive correlation with DOI at 12 weeks. In comparison, previously treated patients showed a moderate, but relatively lower, negative correlation between AoO and PANSS total, negative, and general symptom severity at 12 weeks and weak negative correlation with negative symptoms at 24 weeks. DOI was not correlated with severity in treated patients. Antipsychotic dose was negatively correlated with AoO at 12 and 24 weeks in untreated patients (p < .05) but not in treated patients.
Medians (50th percentile) of PANSS total and positive, negative, and general symptom sub-scores were plotted for all assessment periods. In both groups individually, severity scores showed a decreasing trend, with more fall in scores at 12 weeks than at 24 weeks (p < .001 for all comparisons on the Wilcoxon Signed Ranks test). However, comparatively, both groups followed a similar trend, with no difference on visualization. Details are provided as online-only supplementary material.
Correlation Analysis of Illness Variables.
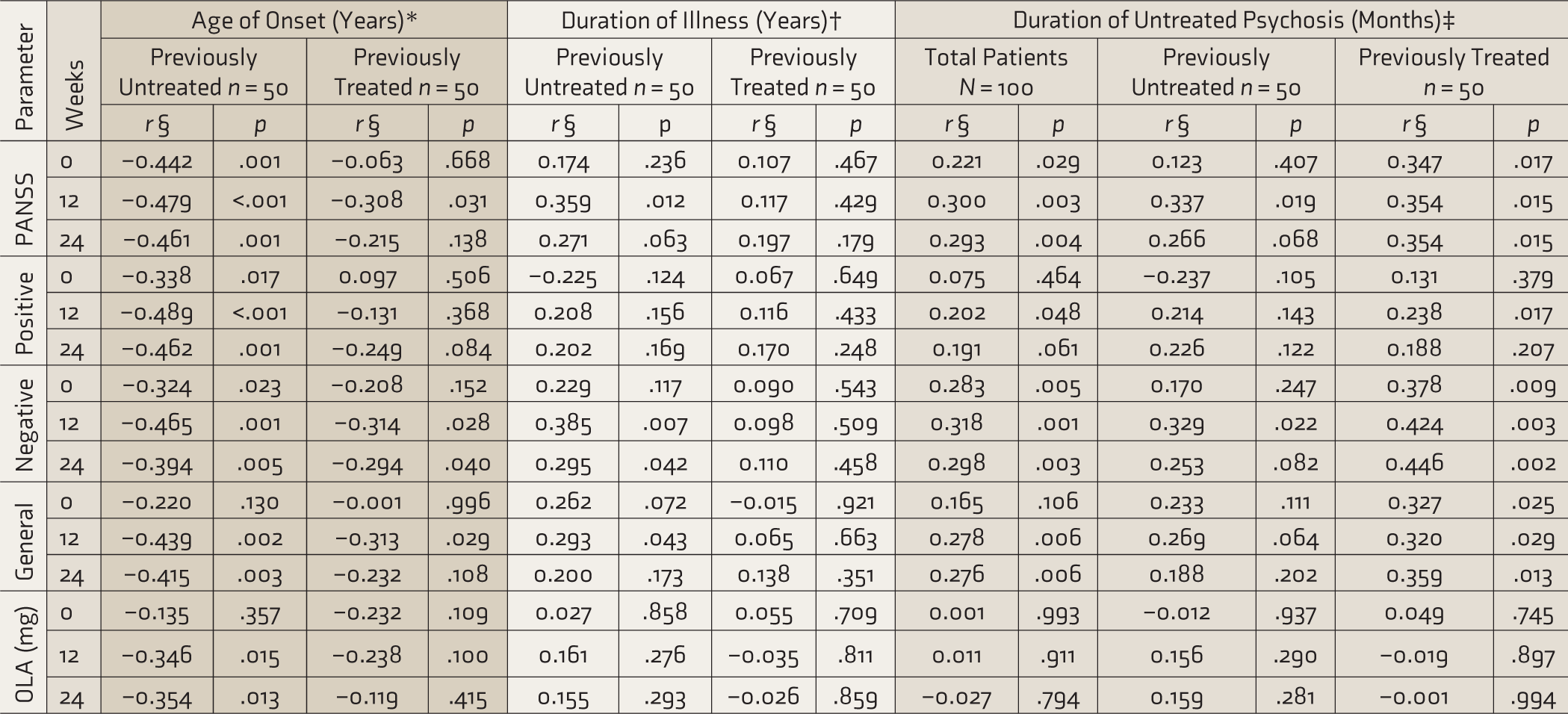
*Controlled for age.
†Controlled for age and age of onset.
‡Controlled for age, age of onset, and duration of illness; duration of illness was highly correlated (r > 0.9) with duration of untreated psychosis in previously untreated patients, so these were controlled for age and age of onset only.
§Partial non-parametric correlations.
PANSS: Positive and Negative Syndrome Scale; OLA: Olanzapine equivalents of antipsychotics calculated by the minimal effective dose method.
DUP
The mean DUP of total patients was 17.9 ± 31.6 months, with a median of 3.0 months. DUP showed no association with age (Kendall’s tau b = 0.09, p = .225), gender (Mann–Whitney U = 1077.50, p = .302), occupation (Kruskal–Wallis H = 5.02, p = .541), marital status (Kruskal–Wallis H = 0.98, p = .613), religion (Mann–Whitney U = 776.50, p = .199), type of family (Kruskal–Wallis H = 0.43, p = .807), locality (Mann–Whitney U = 989.50, p = .550), socio-economic status (Kruskal–Wallis H = 2.00, p = .367), or family history of psychiatric illness (Mann–Whitney U = 805.00, p = .160). However, DUP had a significant negative correlation with years of education (partial non-parametric correlation, controlling for age; r = –0.25, p = .011).
Correlation analysis of DUP with illness severity (Table 3) showed a weak-moderate positive correlation with PANSS total and negative symptoms at all follow-ups, positive and general symptoms at 12 weeks, and general symptoms at 24 weeks, after controlling for age, AoO, and DOI (p < .05). Considering groups individually, DUP in untreated patients showed a moderate positive correlation with PANSS total and negative symptoms at 12 weeks, while in treated patients, it showed a moderate correlation with PANSS total, negative, and general symptoms at all follow-ups.
Impact of DUP on CGI-S measures (Table 4) was that, at all follow-ups, moderately to extremely ill patients had significantly higher DUP than patients with a normal to mild illness. On CGI-I measures post-treatment, DUP was significantly higher in those patients who did not improve at all or those who had minimal change.
Comparison of CGI Measures Based on DUP in Total Sample (N = 100).
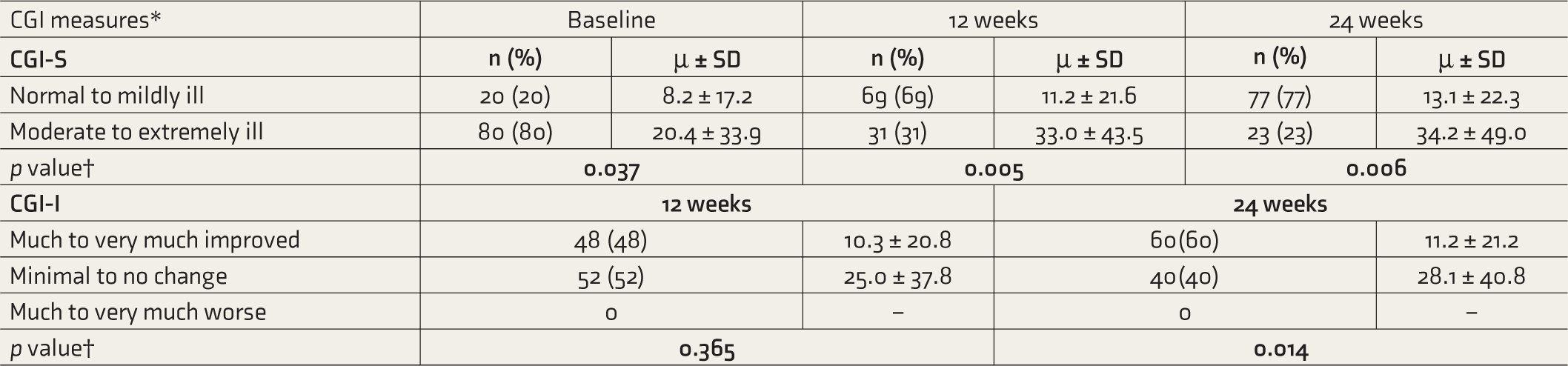
*Some CGI categories were combined for ease of comparison.
†Quade’s ANOVA test used, controlling for Age, Age of Onset, and Duration of Illness.
CGI: Clinical Global Impression; DUP: Duration of untreated psychosis.
Discussion
Previously Untreated versus Treated Schizophrenia
Socio-demographic Variables
Compared to previously treated patients, untreated schizophrenia patients had a lower age of presentation and lower total DOI. Similar AoO between both groups and higher DOI in treated patients explain their higher age of presentation. Lower DOI in untreated patients may be multifactorial. Factors like easy availability of services or mental health awareness leading to early presentation in hospitals seem less likely due to high prevalence of untreated patients in the area. Considering no group differences in terms of severity, untreated patients may have progressed at a faster rate to warrant hospitalization than treated patients, hence a lower DOI. However, further research into factors leading to admission is required to pinpoint the same. No significant differences were found based on gender, education, occupation, marital status, family type, religion, locality, socioeconomic status, or family history of psychiatric illnesses. In contrast, Ran et al. showed that the never-treated patients had a higher mean age, had a lower family economic status, had obtained lower education (at least primary), lived alone, and had higher AoO of psychosis than treated patients, but with no difference in the DOI. These may be due to sample differences in the current study. Similar to our study, however, no differences were found based on gender, marital status, or ability to do work. 8
Illness Severity
Comparing the illness severity using the PANSS and CGI-S scores, no difference was found between the two groups at baseline or 12 or 24 weeks, although a declining trend was seen in both. Ran et al. found that after a 10-year follow-up, PANSS total, positive, negative, and general scores were higher among untreated patients than treated patients with schizophrenia. 8 This might be due to the difference in study duration, which was considerably short in the current study. In contrast, Harrow et al. found that more treated patients presented with moderate to severe psychotic symptoms, which was explained based on internal characteristics of untreated patients, that is, being less vulnerable and more resilient. 15
Illness Improvement
Assessing improvement using the CGI-I scale, more of the previously treated patients were much improved at first follow-up. This difference, however, was not seen at 24 weeks. Thus, although end-point recovery was similar between the groups, the rate of improvement was better in previously treated patients. Similarly, Ran et al. found that Global Assessment of Function scores were higher for treated patients than for untreated patients at 10-year follow-up. 8 In contrast, a study found that at the end of 25 years, of the 46 treated schizophrenia patients, most had only intermediate (52%) or poor outcomes (19%). A better outcome was associated with favorable course and severity of illness, rather than a ‘previously treated’ status. 16 Another research based on long-term assessments (ranging from 2 to 20 years) had found that treated psychotic patients did not show remarkable improvement in terms of severity than the ones not prescribed antipsychotics at all on previous assessments. 15 Haddad et al. found that antipsychotic naive patients had better treatment response (≥50% PANSS score reduction) than pre-treated patients (66% and 47%, respectively). 17 The explanation they provided was that either the treated patients got more resistant over the illness course or the untreated patients had a better response due to shorter DOI and lesser adverse effects of antipsychotics. This was not the case in the current study; though the total DOI was lower in untreated patients, the similar equivalent dosage required in both groups potentially ruled out treatment resistance in the short term.
AoO and DOI
In previously untreated patients, controlling for age, AoO was negatively correlated with positive, negative, and general psychopathological symptoms on most assessments, including baseline. However, in treated patients, AoO was negatively correlated with negative (both follow-ups) and general (second follow-up) symptoms only. It might be that in treated patients, factors like antipsychotics dose, adverse effects, and treatment adherence may have played major roles rather than AoO, especially for positive symptoms. Because treatment adherence was ensured and adverse effects were kept in check during follow-ups, AoO might have re-emerged as a factor for negative and general symptoms.
Considering DOI after controlling for age and AoO, untreated patients showed a positive correlation with negative (both follow-ups) and general (first follow-up) symptoms, while it was not correlated with severity in treated patients. For untreated psychosis, it may be said that after initiating treatment, DOI plays a major role in delaying response to treatment in terms of negative and general symptoms. In treated patients, however, other factors like the number of episodes, treatment adherence, and adverse effects may play a role rather than DOI.
Based on previous studies on AoO and DOI, Immonen et al. found that an earlier AoO was correlated with more negative symptoms (N = 7, r = 0.14, p < .05), independent of DOI. They inferred that DOI partly explains the connection between AoO and poor outcomes, especially in non-first-episode previously treated patients. Similar to the current study, 18 Boonstra et al. found that longer illness duration in previously untreated first-episode patients was associated with higher PANSS scores from baseline to follow-ups. Though they did not differentiate between untreated and treated patients, 19 Altamura et al. also stated that in acute schizophrenia, longer DOI was predictive of poor treatment response. 20
Antipsychotics and OLA Equivalents
The comparison of antipsychotics used showed that at presentation, SGAs and combination FGAs+SGAs were used more among untreated and treated patients, respectively. This may be because SGAs have largely replaced FGAs as the usual initial treatment for psychosis. The treated patients might have been on combination drugs on the previous treatment itself. In any case, since both groups did not differ much on CGI and PANSS measures at presentation, this difference may be a part of clinician’s practice rather than presenting symptoms. No difference in terms of OLA equivalents was found in both groups; however, correlation analysis in untreated patients showed that it was negatively correlated with AoO at follow-ups. Since no correlation was found at baseline, it may be said that in first-time-treated patients with lower AoO, a higher dose is required for the desired improvement over time. While in treated patients, treatment-related factors might have played a role rather than AoO. No recent studies had compared antipsychotic types and OLA equivalents among untreated and treated patients. Only in terms of dosage, Harrow et al. 15 found that among treated patients, a median dose of 575mg Chlorpromazine (CPZ) equivalent dose was prescribed. However, in the current study, a lower median dose (10mg OLA equivalent = 360mg CPZ equivalent) 14 was prescribed at baseline, with minor variation at follow-ups, which may be due to clinical or demographic characteristics of our sample.
Trends in the Illness Pattern
Trajectories of PANSS total, positive, negative, and general scores were similar in both groups, depicting a falling trend. The fall was steep from baseline to 12 weeks and gentle from 12 to 24 weeks. Abdin et al., over a 2-year follow-up, described two trajectories (early response and stable trajectory and delayed response trajectory) for positive symptoms and four trajectories (early response and stable trajectory, early response and relapse trajectory, slower response and no response trajectory, and delayed response trajectory) for negative and general symptoms. 21 In this sense, the current study followed an early response and stable trajectory for both groups. Another study found mixed trends in patients with untreated psychosis, whereas for psychosis in general, they found a decline followed by a plateau for positive symptoms, similar to the current study. However, not much change was found in negative symptoms over the long term. 22
DUP
The current study found a mean DUP of 17.9 ± 31.6 months in total patients (median 3.0 months). In contrast, it was variable in previous studies; Norman et al. reported a DUP of 14.6 months (58.4 weeks), 23 Boonstra et al. reported 61.4 ± 132.7 weeks (median~3.0 months), 24 and Thrithalli et al. reported 90.2 ± 121.9 weeks. 25 Variations in the study sample and duration can account for such differences.
Based on socio-demographic characteristics, previous studies found both similarities and differences in comparison to the current study, which only found a negative correlation with education. The findings by Kaymak et al. were in line with the current study. 26 Ran et al. found an association of longer DUP with higher age, being unmarried, living alone, and having lower educational achievements (p < .01). 8 Other studies found that untreated patients were more among 15–29 year olds (84%) than higher age groups; 27 were mostly males; 28 were artisans, followed by students and unemployed; 29 belonged to urban areas; 30 had more positive family psychiatric history (53.8%–55.1%),29,30 and had an AoO of 26.0 ± 8.9 years. 24 The differences may be due to demographic and sample variations.
The current study reflected that longer DUP in the total sample was correlated with more negative symptoms consistently at presentation and follow-ups, and with general symptoms at follow- ups only. It was inconsistent for positive symptoms. However, overall se- verity (PANSS total) was correlated with longer DUP. Considering DUP in un- treated versus treated patients, the former showed an inconsistent positive correlation of DUP with negative symptoms at 12 weeks, while the latter had a consistent correlation with negative and general symptoms at presentation and follow-ups. This result was unexpected, and factors causing this remain unknown. However, overall, DUP seems to affect the negative and general psychopathological symptoms more than the positive symptoms. Similarly, Thrithalli et al. found that DUP had a weak positive correlation with symptom severity at baseline (r = 0.25, p < .01) and at follow-ups (r = 0.23, p = .03). 25 Boonstra et al. found a positive correlation between DUP and negative symptoms throughout the course from baseline (Fisher’s z = 0.117, 95% confidence interval [CI] 0.064–0.17), to short-term (Fisher’s z = 0.18, 95% CI 0.086–0.274) and long-term follow-up (Fisher’s z = 0.202, 95% CI 0.137–0.267). 24 In contrast, Cavalcante et al. found that in addition to PANSS total and negative symptoms, DUP was also correlated with positive symptoms (p < .05). 31
The CGI measures had findings similar to the PANSS scores, with higher DUP associated with moderate to extreme illness (CGI-S) and minimal to no improvement (CGI-I). Cavalcante et al. supported the same that higher DUP was positively correlated with severity on CGI at all follow-ups. 31 Harrow et al. noted that on severity scales, more patients at follow-ups, presented with moderate to severe psychotic symptoms compared to mild symptoms (p < .05). 15 Long-term studies had maintained that DUP negatively affects the outcome in clinical, functional, and psychosocial domains. 32 A recent study found that DUP was not associated with baseline clinical parameters but with worse outcomes following a short treatment. 33 Research also found that patients with longer DUP had a worse pharmacological response. 33 The current study, however, did not find an independent correlation of DUP with antipsychotic dosage.
Strengths and Limitations
Strengths include a comparison of un- treated versus treated psychosis, studies of which, especially from India, are scarce. Rigorous inclusion criteria were set beforehand to reduce selection bias, data were corroborated from reliable informants and old case records to reduce information bias, and confirmation of diagnosis and review of severity were done by a consultant in the department to address interviewer bias. Regular follow-ups were done to ensure treatment adherence. Limitations of the study include the small sample studied. Also, a longer follow-up period may have provided more robust results. The use of a blinded evaluator to assess outcomes would have avoided inadvertent bias. The pattern of illness (e.g., episodic or continuous, partial, or complete remission) was not analyzed, which might have impacted clinical outcomes in both groups.
Conclusion
In previously untreated schizophrenia, illness variables like AoO and DOI significantly affect severity. End-point recoveries being similar, untreated patients have delayed improvement. Higher DUP is more consistently associated with negative symptoms of schizophrenia.
Footnotes
Acknowledgements
We express sincerest gratitude to the department of Psychiatry, Guru Gobind Singh Medical College & Hospital, Faridkot.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.