
Abstract
Background:
Screening and brief intervention (SBI), effective in community health care, show inconsistent results in correctional settings (CS). We hypothesized that SBI needs adaptation for the incarcerated population. The study aimed to evaluate the effectiveness of extended SBI (X-SBI) for substance misuse in CS.
Methods:
A controlled trial was conducted in two federal CSs in India. X-SBI included coping skills training, risk behavior counseling, and acceptance-based stigma reduction, while the control group received screening, advice, and brief psychoeducation. Both groups received three sessions with 188 participants each, with a “moderate risk” of SUD. Measurements included the Alcohol, Smoking, and Substance Involvement Screening Test (ASSIST), Timeline Follow-up for drug and alcohol use frequency, Overdose Risk Information, HIV risk-taking behavior scales, Self-reporting questionnaire, and Internalized Stigma of Substance Abuse scale. Follow-ups were done at three- and six months post-intervention.
Results:
All participants were men. No initial differences in ASSIST scores or substance use frequencies were noted. ASSIST scores for all substances were significantly reduced at follow-ups. X-SBI showed better outcomes in reducing ASSIST scores for primary substances and illicit drugs, with small effect sizes (η2 = .06–.10). Reductions in drug and alcohol use were noted in both groups, with X-SBI showing a greater decrease in illicit drug use at six months. X-SBI had higher transition rates to the “action” stage of motivation and significant declines in overdose and HIV risk behaviors, mental distress, and stigma scores.
Conclusion:
Integrating three-session X-SBI into CS may effectively address substance misuse.
Trial Registration:
Clinical Trial Registry, India (Reference No. CTRI/2022/01/0391XX)
This was a controlled trial in two correctional settings (CS) The experimental group received extended screening and brief interventions (X-SBI) Participants in the X-SBI group had reduced primary substance use significantly at 3 and 6 months The X-SBI participants had improvements in mental health, HIV, and overdose risk behaviors The X-SBI might be an effective and scalable intervention for substance misuse in CSKey Messages:
Substance misuse and substance use disorders (SUDs) among incarcerated populations are alarmingly high, exceeding general population rates by more than 20 and 30 times for alcohol use disorder (AUD) and drug use disorders, respectively.1,2 The prevalence of HIV in correctional settings (CS) is 3–4 times higher than in the general population, 3 making incarcerated individuals a “key population” for HIV and hepatitis prevention. The risk of drug overdose post-release is significantly elevated for those with SUD or mental health treatment needs. 4 Effective management of substance misuse in prisons is crucial for individual health and societal implications, such as reducing recidivism and mortality and improving public safety. 5 Treatment can change attitudes, beliefs, and behaviors toward drug use and crime.5–8
Psychosocial interventions for substance misuse in prison settings have gained recognition for effectively addressing the complex needs of incarcerated individuals. Approaches such as cognitive-behavioral therapy (CBT), motivational interviewing (MI), and group therapy aim to reduce substance use and improve psychological well-being. Recent systematic reviews indicate that CBT and MI are particularly effective in reducing drug and alcohol use among prisoners9,10 (References). A study by Mitchell et al. (2012) 11 found significant reductions in substance use post-release due to CBT, suggesting enduring benefits. MI enhances inmates’ motivation for recovery and adherence to treatment, contributing to lower relapse rates. 12 Group therapy, including therapeutic communities, fosters supportive networks crucial for long-term recovery, with research by Prendergast et al. (2004) 13 showing lower drug use and recidivism rates among participants.
Implementing psychosocial interventions for substance misuse in prisons faces barriers such as limited resources, staff shortages, and the transient nature of the prison population. Overcrowding and high turnover disrupt treatment continuity, essential for long-term success. 14 Additionally, a lack of trained staff limits the effectiveness of specialized interventions like CBT. 11 In response to these challenges, brief psychosocial interventions based on screening and brief interventions (SBI) offer a viable alternative. Designed to be adaptable and delivered in a short format, they are feasible in resource-constrained environments. 15 The transient nature of incarceration highlights the need for interventions that yield meaningful results quickly. Brief interventions leverage the prison setting as a “teachable moment.” 15 SBI aligns with emerging paradigms in correctional rehabilitation that emphasize strengths-based approaches and empowerment for individuals with SUDs. By fostering self-efficacy and enhancing motivation for change, these interventions empower individuals to take ownership of their recovery journey and promote positive behavioral changes beyond prison walls.16,17 Addressing substance use early in incarceration can mitigate the cycle of misuse, criminal behavior, and recidivism. 18
However, clinical trials on the effectiveness of SBI in CS provided mixed results. A study from the US did not find differences between SBI and controls either in substance use or reduction in risk behavior and quality of life. 19 The authors advocated developing and evaluating SBI models specifically tailored to meet the unique characteristics and needs of the prison population.
We explored adapting SBI in CS through a qualitative pre-intervention inquiry to understand drug use from personal and systems perspectives. At the individual level, interventions should enhance coping strategies and address stigma. At the systems level, staff training is needed to improve attitudes and create a supportive environment for behavior change. 20 This work aimed to determine the effectiveness of X-SBI (vs. screening and education) in reducing substance use, risky use, other risk behaviors, mental health, and stigma in the CS.
Methodology
Study Design
This quasi-experimental study used a cluster design with individual prisons as clusters. This design was chosen to administer the intervention at the organizational level, minimize participant contamination, ensure blinding, and control contextual variables influencing outcomes.
Participants
The study was conducted in a North Indian State, with a network of 21 jails as clusters. Three jails were selected through cluster random sampling, with one excluded due to administrative reasons, leaving two district jails. Both jails house adult under-trial and convicted prisoners. These jails share similar provisions for educational and recreational activities, administrative structures, and healthcare facilities.
Participants were eligible if aged 18–60, of any sex, and scored at moderate risk for substance misuse on the Alcohol, Smoking, and Substance Involvement Screening Test (ASSIST). For those scoring moderate risk for multiple substances, the intervention prioritized the highest-scoring substance, ensuring a tailored treatment approach. Eligibility also required inmates to remain imprisoned for at least six months post-intervention. Under-trial prisoners’ participation was contingent on court hearing dates. The inclusion criteria also ensured that all participants must have been staying in the same prison for at least the last three months of enrollment. Participants at high or low risk per ASSIST, those with only tobacco use disorder, and those unwilling to participate in the interventions or follow-ups were excluded.
Participants were enrolled between December 2022 and May 2023.
Interventions
The experimental intervention, X-SBI, targeted substance misuse among incarcerated individuals through key components. It began with SBIs known for motivating behavioral change. 21 Integrated with the ASSIST screening tool, the intervention used the FRAMES model (Feedback, Responsibility, Advice, Menu of Options, Empathy, Self-efficacy), engaging participants through personalized feedback, encouraging responsibility, and offering advice and treatment options. Delivering the intervention with empathy and boosting self-efficacy were core elements supported by the WHO-ASSIST manual. 22 Educational sessions informed participants about substance dependence, its effects, and high-risk behaviors, empowering informed treatment choices. 23 Coping skills and resilience building were emphasized, and inmates were equipped with stress management strategies, as resilience improves treatment outcomes. 24 Acceptance-based therapy, including acceptance and commitment therapy (ACT), targets reducing internalized stigma and enhancing recovery and psychological well-being among substance users. 25
The control intervention comprised screening via ASSIST, providing feedback, education regarding substance misuse, and carrying out an open dialogue with the participants on the challenges in dealing with the CS as well as their hopes for and aspirations. The discussions were more general and free-flowing, with no theoretical orientation/objectives. Both groups received three sessions; although individual sessions for the X-SBI were up to 30 minutes, these were 15 minutes or less for the control group. All sessions were delivered in a week. Two trained psychiatric social work professionals delivered the interventions—one each in the experimental and control prisons. They had at least two years of clinical experience with persons with SUD. We checked the fidelity of the intervention. The senior research staff listened to 5% of the randomly chosen recorded sessions and rated those on a predesigned questionnaire. The questionnaire was based on the spirit and process of MI and components of BI (“FRAMES”).
Outcome(s)
The primary outcome was to determine the effect of X-SBI (vs. control) on the ASSIST score for primary substance misuse. There were several secondary outcomes- comparing the groups about the reduction in the frequency of drug and alcohol use, change in motivation, transition from moderate to low-risk category of substance use, reduction in stigma, mental distress, and high-risk behavior.
Outcome Assessment
We used the following assessment tools:
Alcohol, Smoking, Substance Involvement Screening Test (ASSIST) 3.0:22
Developed by the World Health Organization (WHO), the ASSIST is designed to identify hazardous, harmful, and dependent use of substances, including tobacco, alcohol, and drugs. It has high internal consistency (0.77–0.94) and satisfactory correlations with risk factors for substance use problems (0.48–0.76). The tool has been validated for use in the Indian context and asks participants about their substance use over the last three months, categorizing them into low-, moderate-, or high-risk groups. We focused on enrolling those categorized as “moderate” risk. 22 The “moderate risk” group was defined by a score between 4 and 26 for illicit drugs and 11–26 for alcohol.
Timeline Follow-Back (TLFB)
This tool serves both clinical and research purposes to quantify the usage of various drugs, including cannabis. It requires participants to estimate their substance use over the past three months retrospectively. The TLFB can provide reliable estimates ranging from the past seven days up to two years and will be used to assess secondary outcomes such as the frequency of illicit drug and alcohol use. 26 We calculated the frequency of use as the number of days of illicit drug/alcohol use in the last month. The heavy drinking frequency was estimated from the number of days in which the participants had six or more drinks on one occasion. 27
Readiness to Change Questionnaire (RCQ)
Based on Prochaska and DiClemente’s stages of change model, the RCQ is a 12-item questionnaire developed initially for alcohol use but was adapted to include drug use. An interviewer administers it and aims to gauge progression through stages of change, ideally advancing participants from contemplation to action through brief MI. 28
HIV Risk-Taking Behavior Scale (HRTBS)
This scale includes 11 items, each targeting specific HIV risk behaviors, scored on a 0–5 scale where higher scores indicate more significant risk. It features two subscales to assess both injecting and sexual behaviors. 29
Overdose Risk
The assessment of overdose risk was conducted using the Overdose Risk Information (ORION) tool, developed as part of an EU project for drug overdose prevention. It consists of nine questions that address both risk and protective factors for drug overdoses occurring in the last 30 days, with responses being “yes” or “no.” 30
Self-Reporting Questionnaire (SRQ)
Developed by the WHO, it is a tool designed to screen for mental health disorders, particularly in low-resource settings. Comprising 20 items, the SRQ assesses symptoms associated with anxiety, depression, and psychosomatic complaints to identify individuals in need of further psychological evaluation or treatment. 31
Internalized Stigma of Substance Abuse (ISSA) Scale
The ISSA scale quantifies the internalized stigma experienced by individuals with SUDs. It measures feelings of shame, social withdrawal, and perceived discrimination, providing insights into the psychological barriers that impact rehabilitation and recovery processes. 32
The outcomes were assessed twice- at three months and six months post-intervention. Clinical psychologists assessed the outcomes.
Sample Size
For our primary outcome, a 7-point difference in the ASSIST scores (standard deviation of 15), we required sample size of 117 participants per study arm to achieve 80% statistical power. 33 This calculation assumed a pre-post correlation coefficient of 0.2 between measurements. To account for an anticipated dropout rate of 25%, we adjusted the initial sample size to 188 participants in each study arm to ensure sufficient statistical power for detecting the intended effects.
Randomization
Although we selected three prisons via our first stage cluster random sampling, one of these prisons had to be excluded because of the lack of administrative approval. AG tossed a coin and allocated the two prisons to the X-SBI and control groups. Allocation concealment was not applicable here. Although we randomly allocated the prisons into two treatment groups, we do not present this study as a randomized trial but as a quasi-experimental study. The participants and the outcome assessors were blinded to the group status. Blinding the staff delivering the intervention was not feasible.
Statistical Analysis
Data analysis used IBM SPSS Statistics 16.0. Independent sample t-tests and Chi-square tests compared baseline demographic characteristics, ASSIST scores, and drug use frequency. A general linear model (GLM) with repeated measures assessed the main effects of time and group and their interaction on mean ASSIST scores, with age as a covariate and Bonferroni’s correction applied. Completers-only and intention-to-treat (ITT) analyses were conducted, with the last observations carried forward in ITT analyses. GLM and repeated measures assessed changes in SRQ, ORION, and ISSA scores, adjusted for baseline scores. Friedman and Mann-Whitney-U tests compared substance use frequency within and between groups, using completers-only analyses.
Results
Participant Flow
Enrollment occurred in two phases for logistical reasons: October 1, 2022 to February 28, 2023, and April 1, 2023 to May 1, 2023. All participants completed three sessions. The three- and six-month follow-ups started mid-February 2023 and ended by November 30, 2023. Of 538 assessed for eligibility, 376 met the inclusion criteria (188 per group). At three months, seven in X-SBI and 10 in control did not follow up; 22 and 32, respectively, at six months. The overall follow-up rate was ~86% at six months, with no significant differences between groups (3 months: P = .456; 6 months: P = .141). See Figure 1 for details.
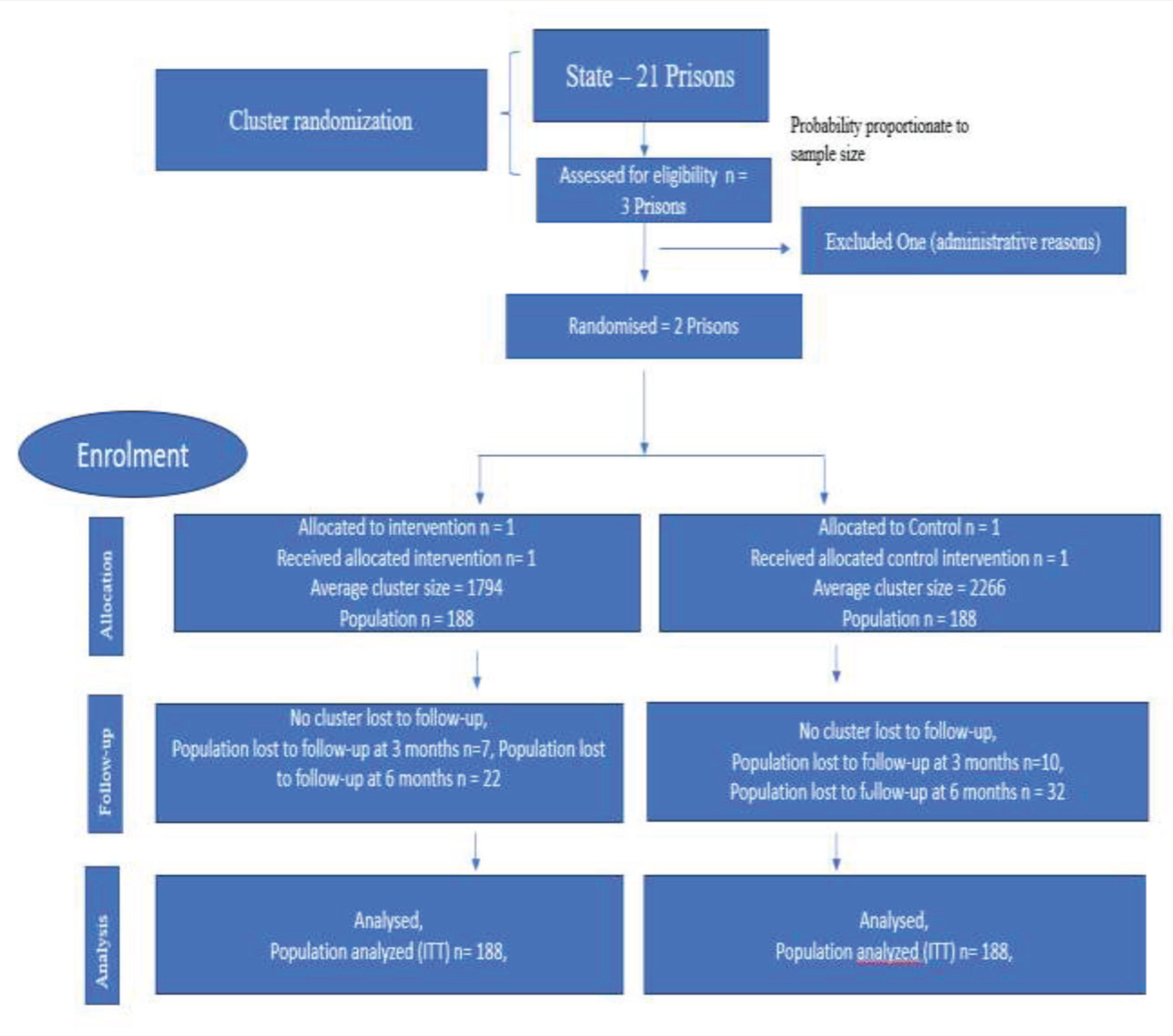
This diagram illustrates the flow of clusters (correctional facilities) and participants through each stage of the randomized trial. It details the number of clusters assessed for eligibility, randomized, allocated to each group (intervention or control), followed up, and analyzed. Additionally, it reports participant enrollment, allocation, follow-up, and analysis within each cluster. Exclusions and losses at each stage are specified along with reasons to ensure transparency in trial reporting. This structure helps in understanding the management of both clusters and individual participants throughout the study phases, from initial assessment to final analysis.
Baseline Data
There were no significant differences between the X-SBI and control groups in education level, marital status, former occupation, ASSIST scores for substances, illicit drug use, motivation, frequency of illicit drug use, heavy drinking, drinks per drinking day, and HIV risk behaviors. All participants were men. However, significant differences were observed in other characteristics. The X-SBI group was younger (t = −2.326, P = .021), had higher baseline ORION scores (t = 6.316, P < .001), better SRQ scores (t = 6.456, P < .001), and lower ISSA scores (t = 2.686, P = .008). They also had more initial drinking days (TLFB: U = 1755.500, P = .022) (Table 1).
Baseline Characteristics.
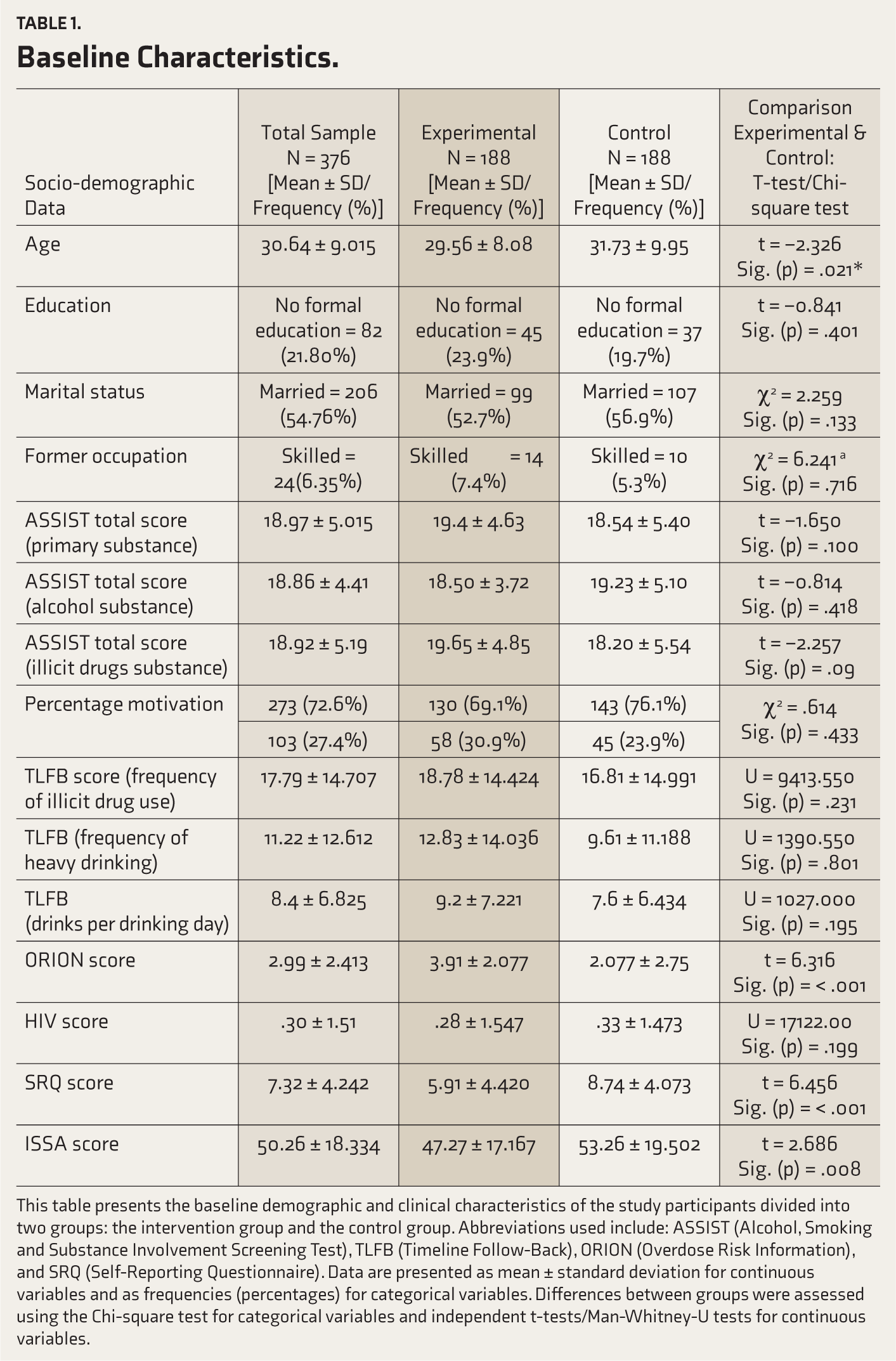
This table presents the baseline demographic and clinical characteristics of the study participants divided into two groups: the intervention group and the control group. Abbreviations used include: ASSIST (Alcohol, Smoking and Substance Involvement Screening Test), TLFB (Timeline Follow-Back), ORION (Overdose Risk Information), and SRQ (Self-Reporting Questionnaire). Data are presented as mean ± standard deviation for continuous variables and as frequencies (percentages) for categorical variables. Differences between groups were assessed using the Chi-square test for categorical variables and independent t-tests/Man-Whitney-U tests for continuous variables.
Numbers Analyzed
For the primary outcome, that is, change of primary substance ASSIST score, we performed completers-only (n = 322) and ITT (n=376) analyses. However, we ran completers-only analyses for the secondary outcome.
Outcomes and Estimations
Change in ASSIST Scores
The ITT analyses for the primary substance ASSIST score showed significant effects of time (F (2, 376) = 111.174, P < .001, partial η 2 = .373), group-by-time interaction (F (2, 376) = 12.045, P < .001, partial η 2 = .061), and a main effect of group (F (1, 188) = 11.301, P = .001, partial η 2 = .029). In the X-SBI group, the ASSIST scores for the primary substance reduced from 19.35 at baseline to 12.08 at three months, with a non-significant increase to 12.50 at six months, indicating significant initial improvements largely maintained over time. For the alcohol ASSIST score, there were significant time effects (F (2, 376) = 33.964, P < .001, partial η 2 = .391) and a main effect of group (F (1, 188) = 4.133, P = .045, partial η 2 = .037), but no significant group-by-time interaction (F (2, 376) = 1.834, P = .165, partial η 2 = .033). For illicit drugs, significant time effects (F (2, 376) = 71.948, P < .001, partial η 2 = .369), group-by-time interaction (F (2, 376) = 7.457, P = .001, partial η 2 = .057), and a trend toward significance for the main effect of group (F (1, 188) = 3.318, P = .070, partial η 2 = .013) were observed. See Supplementary Figures 1, 2, and 3.
The completers-only analyses showed similar results. Please see Table 2.
Effects of Group, Time, and Group X Time on the Primary Substance ASSIST Score.
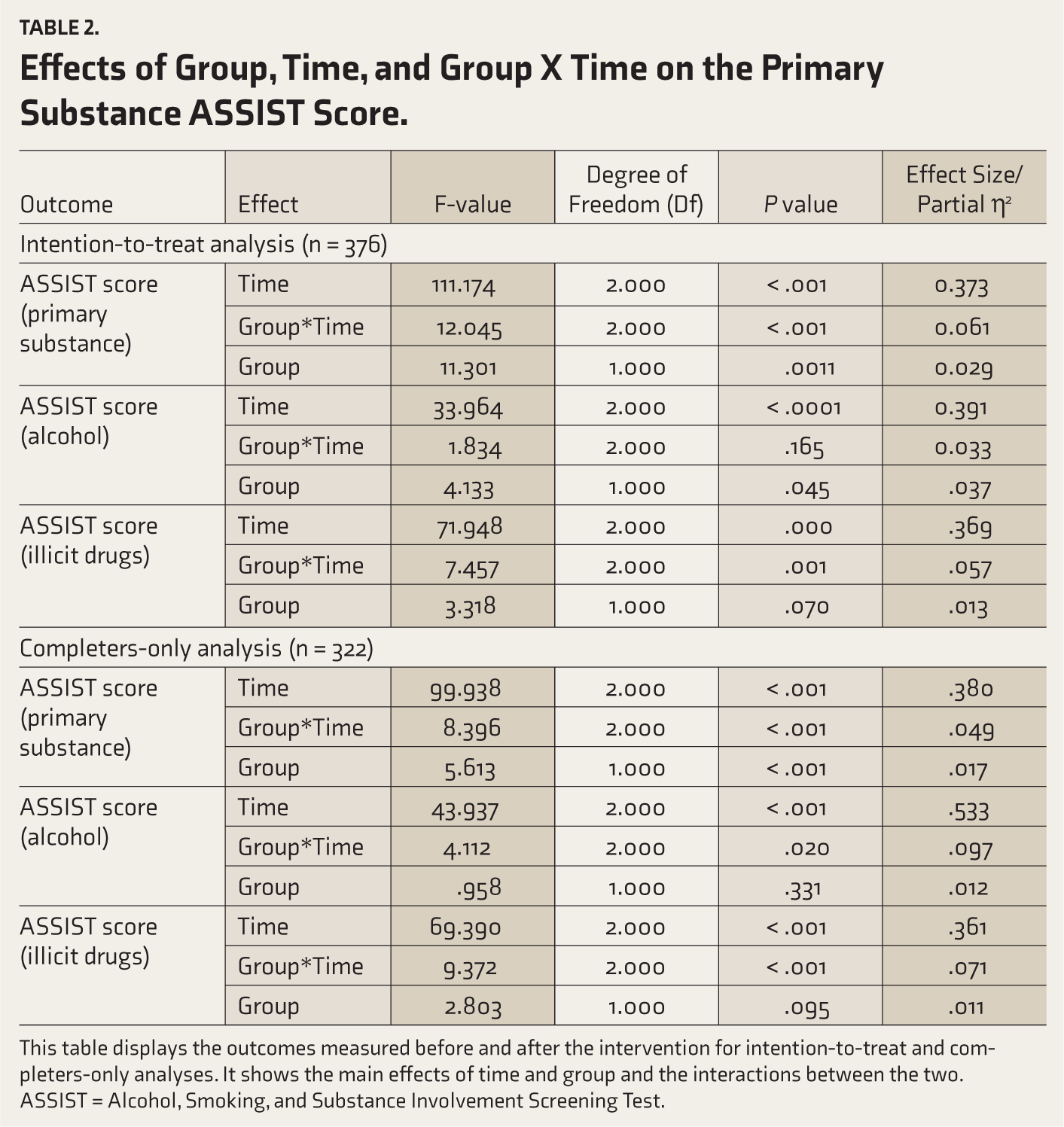
This table displays the outcomes measured before and after the intervention for intention-to-treat and completers-only analyses. It shows the main effects of time and group and the interactions between the two. ASSIST = Alcohol, Smoking, and Substance Involvement Screening Test.
Substance Use
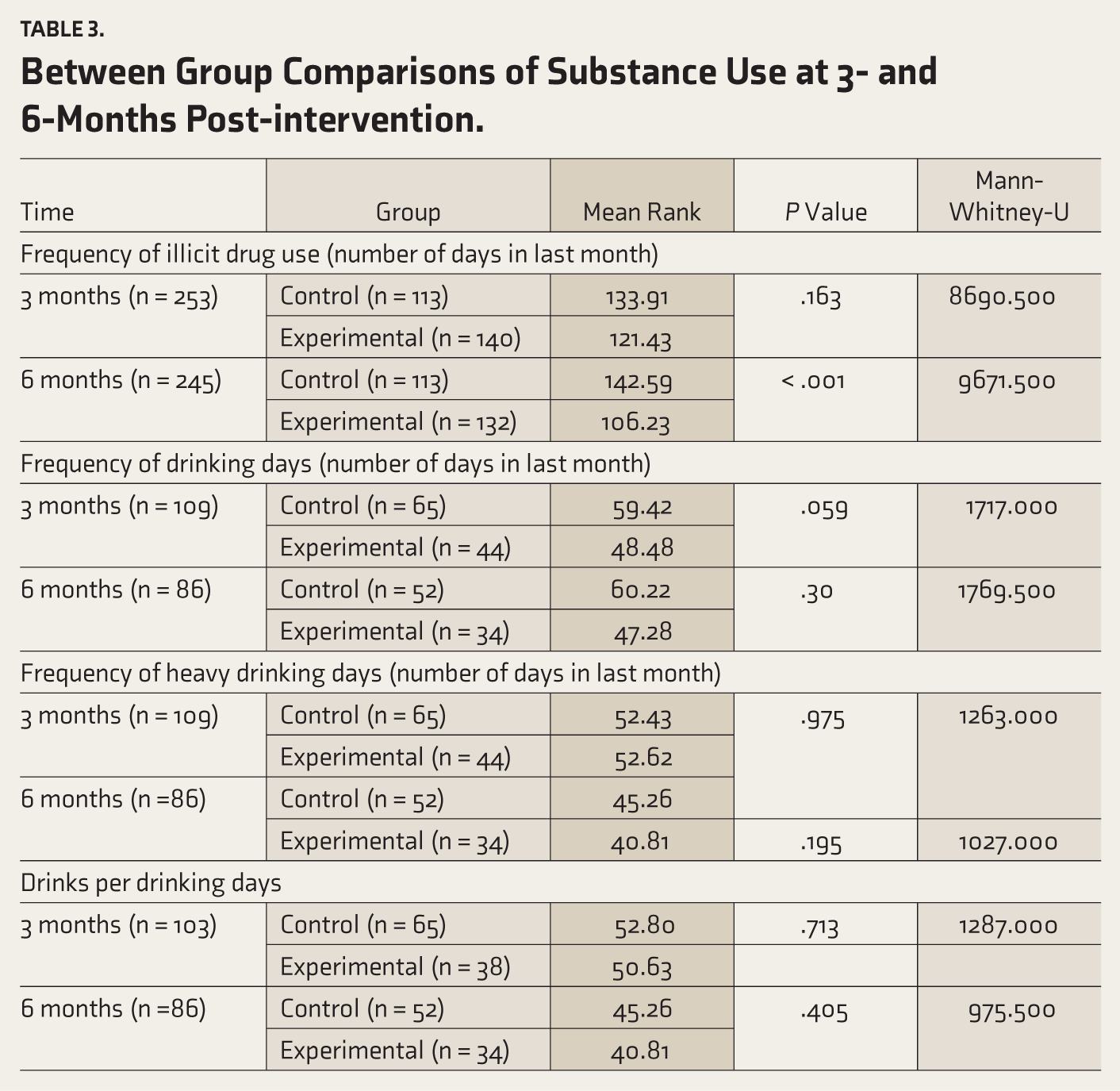
At the 6-month follow-up, the X-SBI group showed a significant reduction in the frequency of illicit drug use compared to the control group (Mean Rank = 106.23 vs. 142.59; Mann-Whitney U = 9671.500, P < .001). No other significant differences were found in drinking frequency or heavy drinking days at 3 and 6 months. Within the X-SBI group, illicit drug use significantly reduced from baseline to 6 months (Friedman = 38.885, P < .001), and drinks per drinking day decreased from 9.9 to 6.3 (Friedman = 24.96, P < .001). In the control group, drinking days significantly decreased from baseline to 6 months (Friedman = 8.735, P = .013). See Table 3 and Supplementary Table 1.
Motivation Level
Significant differences were observed between the control and X-SBI groups at three and 6-month follow-ups in the transition from pre-contemplation/contemplation to action stages. At three months, more participants in the experimental group moved to the action stage compared to the control group (χ² = 15.157, P < .001). By six months, the X-SBI group still showed a higher transition to action, although the difference decreased (χ² = 8.632, P = .003), demonstrating sustained intervention effects.
Mental Health
There was a substantial effect of time on SRQ scores (F = 232.428, P < .001, partial η 2 = .593), indicating significant reductions across different measurement periods. A reduction in SRQ scores suggests reductions in mental distress. Additionally, the interaction between group and time was also significant (F = 87.841, P < .001, partial η 2 = .355), suggesting that the changes in SRQ scores over time differed significantly between the experimental (X-SBI) group and the control group. A significant main effect of the group was also observed (F = 171.669, P < .001, partial η 2 = .349).
Overdose and HIV Risk Behaviors
Time significantly affected ORION scores (F = 301.194, P < .001, partial η 2 = .654), with significant group-by-time interaction (F = 31.878, P < .001, partial η 2 = .167) and a main effect of group (F= 61.619, P < .001, partial η 2 = .161), indicating differing reductions between X-SBI and control groups. Reductions in ORION scores meant a reduction in the overdose risk. The X-SBI group showed significant HIV Risk-Taking Behavior Scale score decreases from baseline (.32 ± 1.495) to 6 months (.00 ± 0.00; χ 2 = 20.462, P < .001), while the control group had minimal changes. No significant between-group differences in HIV risk scores were observed at six months, with a non-significant trend at three months (Mann-Whitney U = 16565.000, P = .052).
Internalized Stigma
Time significantly affected ISSA scores (F = 414.713, P < .001, partial η 2 = .565), with a significant group-time interaction (F = 39.684, P < .001, partial η 2 = .111). The X-SBI group had a greater reduction over time. A significant main effect of the group was also observed (F = 133.185, P < .001, partial η 2 = .295).
Fidelity of the Intervention
The fidelity questionnaire showed high adherence to X-SBI styles and techniques, with mean scores between 4.1 and 5.0. “Autonomy Support” and “Feedback” scored 4.9 and 5.0, respectively. See Supplementary Table 2.
Between Group Comparisons of Substance Use at 3- and 6-Months Post-intervention.
Discussion
We assessed the effectiveness of an Extended SBI (X-SBI) in reducing substance use and associated risks among incarcerated populations. The study showed significant improvements in primary substance use scores, mental health, reductions in overdose risk behaviors, and decreased internalized stigma at six months. The improvements were sustained at the six-month follow-up for alcohol but not for illicit drugs.
Previous literature on the effectiveness of MI and SBI in the CS has provided mixed results. While a large RCT from the US did not find greater effectiveness of SBI (than controls), a review of five randomized trials showed MI might be effective in reducing substance use, at least in the short term.17,34 The additional components of X-SBI, that is, coping and resilience, craving management, and drug education, might be responsible for its significant effect on substance use reduction. CBT and education-based programs have shown effectiveness in reducing drug and alcohol use in the incarcerated population. 35 The effect size of X-SBI for the reduction in ASSIST scores was tiny, suggesting X-SBI must be scaled significantly for a substantial public health impact. However, the small effect was also due to the significant ASSIST score reduction in the control group. While there was about a 7-point ASSIST reduction in the X-SBI, it was 5 points for the controls. The notable reduction in ASSIST scores within the control group suggests that even minimal interventions can have a significant impact on substance misuse among incarcerated individuals. A previous study from the UK also showed that standardized, low-threshold interventions in CS can lead to measurable improvements in substance misuse indicators. 36 The smaller difference between the X-SBI and control groups may indicate that enhancing basic interventions with additional psychosocial support could yield diminishing returns in settings where minimal support provides substantial benefits. This highlights the importance of optimizing resource allocation in correctional substance use programs, ensuring that interventions are cost-effective and appropriately scaled to the prison environment’s needs and existing support levels. Moreover, unlike alcohol (which observed a mean 6-point reduction in ASSIST score), the effects of X-SBI on illicit drugs might not be sustainable beyond three months (with nearly a 2-point increase in the mean ASSIST score). Additional psychosocial support or pharmacological interventions might help sustain the initial improvement.
One of the more distinctive aspects of our study was the marked reduction in internalized stigma. Unlike the findings of Luoma and colleagues, 37 who focused solely on ACT for stigma reduction in community settings, our intervention successfully integrated these principles within a correctional environment. This suggests that interventions tailored to the specific environmental and social pressures of incarceration may be particularly effective in reducing stigma, thereby improving overall treatment engagement and outcomes. The improved mental health outcome could also be attributed to the acceptance and mindfulness training, which was aligned with the evidence of the effectiveness of “third-wave” therapies in improving mental distress in CS. 38
Our findings of significant HIV risk behavior reduction in the X-SBI group must be highlighted. Previous studies also showed the effectiveness of the information and education programs in reducing HIV risk behaviors and changing attitudes and beliefs. 39 However, these studies examined the effectiveness of education programs as stand-alone interventions. In contrast, we demonstrated that HIV-risk reduction information could be delivered effectively with SBI for substance misuse. The reduction in overdose risk behavior was another noteworthy finding. MI-based information strategies showed effectiveness in reducing risk behaviors and overdose incidents. 40 We extended these results to the CS and illustrated the feasibility and preliminary effectiveness of combining overdose risk reduction with SBI.
Our study has several limitations. The foremost is its quasi-experimental design. Although clusters of prisons were randomized, studying only two prisons introduces cluster-specific trait confounding. The intervention’s effects may not generalize broadly due to the unique characteristics of the two prisons. However, structural and systematic differences were minimized by comparing participants’ characteristics and adjusting for baseline age differences.
Nevertheless, the baseline differences at the participants’ level in the scales for measuring overdose risk, mental distress, and internalized stigma might play an effect-modifying role in the outcomes. Including only moderate-risk inmates, excluding high and low-risk individuals, limits generalizability. Conducting the study in two prisons within a specific geographic area further constrains applicability, and men-only participants limit external validity. Follow-up periods of three and six months were too short to gauge long-term impacts like sustained behavioral changes or recidivism. The control group received basic educational interventions, potentially reducing the apparent effectiveness of the specialized intervention. Reliance on self-reported measures for substance use could introduce bias. Despite fidelity checks, variations in facilitator delivery could affect treatment consistency and reliability. The study did not address cost-effectiveness.
This study demonstrates that X-SBI is a unique and effective approach for addressing substance misuse and related risks within CS. The significant improvements in substance use scores, mental health, overdose risk behaviors, and stigma reduction underline the efficacy of X-SBI. Moving forward, future research should explore the scalability of X-SBI, assess its long-term effects on recidivism and integration post-release, and evaluate its cost-effectiveness to optimize resource allocation in correctional health interventions.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Acknowledgements
The Director General Prisons (Haryana) for granting permission to conduct the study and for providing administrative and logistical support.
Data Sharing Statement
Deidentified individual participant data (including data dictionaries) will be made available, in addition to study protocols, the statistical analysis plan, and the informed consent form. The data will be made available upon publication to researchers who provide a methodologically sound proposal for use in achieving the goals of the approved proposal. Proposals should be submitted to
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethics Approval
Extramural Ethics Committee, Postgraduate Institute of Medical Education and Research, Chandigarh, India (in April 2021). Approval from the State Prison Department: October, 2021.
Ethical Considerations
The study was approved by the Institute’s extramural ethics committee (XXX/IEC/2021/000571). Administrative approval was obtained from the State Prisons Department. A written informed consent was obtained from all study participants.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Indian Council of Medical Research (ICMR), New Delhi, India.
Informed Consent
All participants consented to participate in the study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.