
Abstract
Introduction:
As compared to the general population, prison inmates have a high prevalence of mental illness and substance use disorders. The authors designed and implemented a digitally driven, one-year primary care psychiatry program for medical officers in prison and correctional settings to address this need in Bihar, India.
Aim:
The study aimed to assess the outcome of training given to prison medical officers deputed by the Government of Bihar.
Materials and Method:
Five medical officers completed training out of the seven deputed. The training contained brief onsite (three-day) training in “Clinical Schedules for Primary Care Psychiatry” and three online (one-year) modules containing tele-psychiatric on-consultation training (tele-OCT), virtual classroom (VCR) sessions, and a public health module. We measured the outcome using translational quotient (TQ) and primary care psychiatry quotient (PCPQ), which were carried out 6 and 12 months after the onset of training.
Results:
The TQ scores in the first and second tele-OCT evaluations were 64% and 75.2% at 6 and 12 months of the course, suggesting adequate skill retention. Out of 33,565 consultations over 12 months, medical officers identified 2,947 psychiatric disorders requiring treatment, resulting in a PCPQ of 8.7%.
Conclusion:
Over a year, the training demonstrated efficacy in acquiring primary care psychiatry skills, and these competencies were applied in providing care for those with psychiatric disorders.
Keywords
Prison mental health. Tele-mentoring of prison medical officers. Primary care psychiatry program in prison setting.Key Messages:
The prevalence of mental illnesses (inclusive of substance use disorders) in prisons is three to five times higher than that in the general population.1,2 Among nine million prisoners worldwide, one million suffer from mental health disorders. 3 Their prevalence in American and European prisons ranges from 11% to 31% and 62% to 71%, respectively.4,5 According to the Bangalore Prison Mental Health Study, which used a MINI plus interview schedule for psychiatric diagnosis, 79.6% of inmates suffered from either mental illness or substance use (mainly tobacco, followed by alcohol), similar to the studies in Australia and Iran.6,7 Substance use disorders, depression, and anxiety were the most common psychiatric diagnoses; 2 out of 100 people had attempted suicide before, and 7 out of 100 deliberately caused self-injuries. 8 A variety of factors complicate the situation, including overcrowding, disconnection from family, homosexual contact, prolonged detention of prisoners awaiting trials, unsatisfactory living conditions, and lack of any treatment programs.8,9
Given the above reality, it is imperative to maintain a sufficient workforce capable of identifying and promptly addressing mental health issues. However, in India, there is a dearth of working mental health professionals in prison and correctional settings. In the Bangalore prison, there was only one psychiatrist for 5,000 inmates. 8 The India Justice Report (IJR), 2022, mentions that 42,577 inmates in 64 prisons across Maharashtra had only one psychiatrist and two psychologists to attend to them and address their needs. 10 Moreover, in India, in most jails, inmates’ mental health issues are handled by medical officers (MOs), who are usually MBBS graduates. Aside from running the hectic prison clinics, these officers are also expected to handle various administrative tasks. Given the circumstances, the best solution would be to develop an effective mental health training program for MOs already working in prisons, a task-sharing approach, and a well-established concept in primary care. Primary care doctors (PCDs) are expected to manage various conditions at the primary care centers (such as prisons), including mental health issues.11,12 Research shows that PCDs consistently fail to identify 50%–75% of common mental disorders (CMD) patients in their clinical settings.13,14
The National Institute of Mental Health and Neurosciences (NIMHANS) in collaboration with state governments, is involved in scaling up mental health capacities in Karnataka, Uttarakhand, Bihar, and Chhattisgarh, where the aim is to train the PCDs, nurses, social workers, ASHAs, and others working at primary health centers (PHCs), community health centers (CHCs), and Taluk hospitals in identifying, screening, treating, and referring patients with mental health disorders.
In Bihar, particularly since 2017, 59 MBBS doctors have been trained to date with long-term digitally driven hybrid courses in primary care psychiatry, carrying out the District Mental Health Program (DMHP) work at district-level centers across the state. Further, these digitally driven programs have significantly increased their competence and skills (as measured by a progressive increase in the number of psychiatry patients detected and treated and an increase in translational quotient), owing largely to the andragogic and bottom-up approaches employed in these training programs.15,16
This article aims to evaluate the outcome of training and mentoring seven prison MOs working across various prisons in Bihar who were deputed during the years 2021–2022. To cater to the exclusive needs of prisons, a new digitally driven hybrid course titled “Diploma in Prison and Correctional Psychiatry” was designed and accredited by the Board of Studies of the NIMHANS Digital Academy. The course commenced in May 2021 and was completed in April 2022.
Materials and Methods
A point-of-care manual titled “Clinical Schedules of Primary Care Psychiatry 2.2 (CSP)”
17
guided the PCDs throughout the one-year training. It is a validated instrument designed to meet the requirements of PCDs, particularly focusing on developing clinical skills. PCDs can effectively screen, identify, prescribe first-line treatment, and provide brief counseling using CSP. Each medical officer underwent the following four modules in the course curriculum:
Basic module: Between March 24, 2021, and March 26, 2021, a three-day, onsite training was conducted for MOs at All India Institute of Medical Sciences (AIIMS), a tertiary health facility in Patna, Bihar. The prison MOs underwent an orientation program on a range of psychiatric illnesses sourced from CSP. These illnesses included tobacco addiction, alcohol use disorders, psychotic disorders, depressive disorders, anxiety disorders (panic and generalized anxiety), and somatization disorders (acronym TAP DAS). The training methods included live demonstrations of patient assessments and role plays. It also included an orientation on counseling skills as per the CSP manual. The brief counseling involves the following components: (a) educating the patient about the illness; (b) setting realistic treatment expectations; and (c) stress management techniques for applicable individuals. Finally, orientation was given on the upcoming tele on-consultation training. All seven deputed MOs attended the basic module. Module on tele-OCT: It is a hand-holding training procedure conducted in a live, real-time clinical scenario where doctors provide consultations to their patients with minimal disruption to their clinical work. A tele-psychiatrist sits at the hub, observing, correcting, and mentoring the PCDs. It is a kind of practical teaching methodology that helps in easily identifying and starting first-line treatment for common, non-complicated psychiatric disorders. Further details, advantages, and impact of the tele-OCT procedure are detailed elsewhere.11,18 Each prison MO had 2–3 tele-OCT sessions, one-on-one, each covering anywhere between 5 and 15 patients, and lasting 2–3 hours. A total of 19 tele-OCT training sessions were conducted for six prison MOs, and the total number of patients seen was 154, out of which 92 were identified and treated for psychiatric illnesses. Virtual classroom sessions (VCR): Online classroom sessions (to be attended by all MOs) typically lasted one hour and contained seminars, case conferences, and expert talks. These sessions employed a peer-learning approach, where MOs presented cases and seminars on diverse psychiatry topics in prison. These collaborative programs were previously verified by a psychiatrist who chaired these sessions. During the one-year period, one-hour sessions of 10 seminars, 10 case conferences, and 18 interactive lectures on various topics such as history, psychiatry, mental status examination, and common mental conditions such as generalized anxiety disorders, panic disorder, somatization disorder, depressive disorders, and severe mental disorders such as psychosis, alcohol disorders (harmful use and addiction), and tobacco addiction in lines of the CSP manual were conducted. Specific sessions about psychotropic medications, women’s mental health, and child and adolescent psychiatric conditions were included. Additionally, specific topics on prison mental health, identifying and managing high-risk groups (suicidal, violent), the basics of forensic psychiatry, giving expert witnesses in a court of law, prisoners, relevant provisions in the Mental Healthcare Act, 2017, the Juvenile Justice (JJ) Act, 2015, the Protection of Children from Sexual Offenses (POCSO) Act, 2012, and a session on when to refer cases that require specialist evaluation were conducted. Public health module: Each prison MO had to prepare and carry out information, education, and communication (IEC) activities related to mental health awareness. Scoring was given to each activity, which fed into the total summative assessment of the performance, culminating in the certification. Five MOs (who eventually passed the course after fulfilling the accreditation criteria) prepared and conducted one awareness activity inside their respective prisons during World Mental Health Day, covering the following topics: substance use and abuse, suicides, and mental disorders. The content of the IEC was supervised and corrected. Three weeks prior, MOs were informed to prepare the IEC drafts.
Assessments: This course had 10 formative assessment criteria that every MO had to fulfill: (a) one case conference (collaborative and verified); (b) one seminar (collaborative and verified); (c) 50 prison/correctional patients to be screened; (d) 15 psychiatric patients to be treated; (e) 10 referrals to the higher center; (f) 10 video-based case discussions; (g) submitting monthly reports of total patients and those psychiatric disorders seen in a Google form; (h) submitting a monthly audit of psychiatric medications prescribed; (i) substantial attendance for the VCR module (> 60%); and (j) conducting at least one public health initiative, designing at least one public education material (alcohol addiction, tobacco addiction, mental illness, self-harm behavior), and finally, undergoing periodic tele-OCT evaluation sessions. Subsequently, a summative evaluation comprising theoretical and practical examinations was administered online and proctored. All the above assessments were carried out by investigators who are qualified psychiatrists at NIMHANS. Five prison MOs completed all requisite modules at the end of one year. They qualified for the “Diploma in Prison and Correctional Psychiatry award for practicing Medical Officers.” NIMHANS Digital Academy, Board of Studies (BOS) has accredited the course.
Impact and Outcome Measures
Translational Quotient
Translational quotient (TQ) assesses the degree of integration of psychiatry clinical skills among PCDs in their real primary care clinical scenario. TQ is the ability of a training program to translate the learned/taught knowledge into clinical skills required for use during a routine, busy clinical practice. This quotient assesses the degree of success in early diagnosis and prescribing first-line treatment at the primary care level. In this study, TQ was assessed during the two tele-OCT evaluative sessions conducted by an independent tele-psychiatrist (meaning not the one who conducted the tele-OCT for a particular PCD) for each PCD, 6 and 12 months after the commencement of the course, over the live video streaming of their real-time consultations. Prison MOs were evaluated based on six criteria for assessing the TQ:
Elicitation of psychiatric symptoms using a CSP screener, Clinical reasoning of case-ness for psychiatric diagnosis, An appropriate decision regarding choosing psychiatric medications, Coverage of components of brief counseling for patients, Time management for psychiatric evaluation at the primary care level and Overall clinical psychiatric skills
Each criterion was scored between 1 and 5, with a minimum total score of 6 and a maximum score of 30.
Primary Care Psychiatry Quotient
PCPQ is defined as the proportion of psychiatric cases among total general patients with PCDs. It may be equated with the prevalence of psychiatric disorders in primary care.

Analysis
Descriptive statistics were reported in terms of frequency and percentage. The statistical analysis was conducted using IBM SPSS Statistics 29.0.
Results
Translational Quotient
Figure 1 depicts the translational quotient scores obtained in the 6th and 12th months, that is, 64% and 75.2%, respectively. Figure 2 depicts the improvement in different components of TQ. The observed increase in the TQ percentage after the 12-month program indicates that the skills acquired during the course were enhanced and sustained throughout the program. Among the various components of TQ (Figure 2), the difference in score was higher for decision-making regarding psychotropic medications, using elements of counseling and elicitation of psychiatric symptoms using the CSP questionnaire.
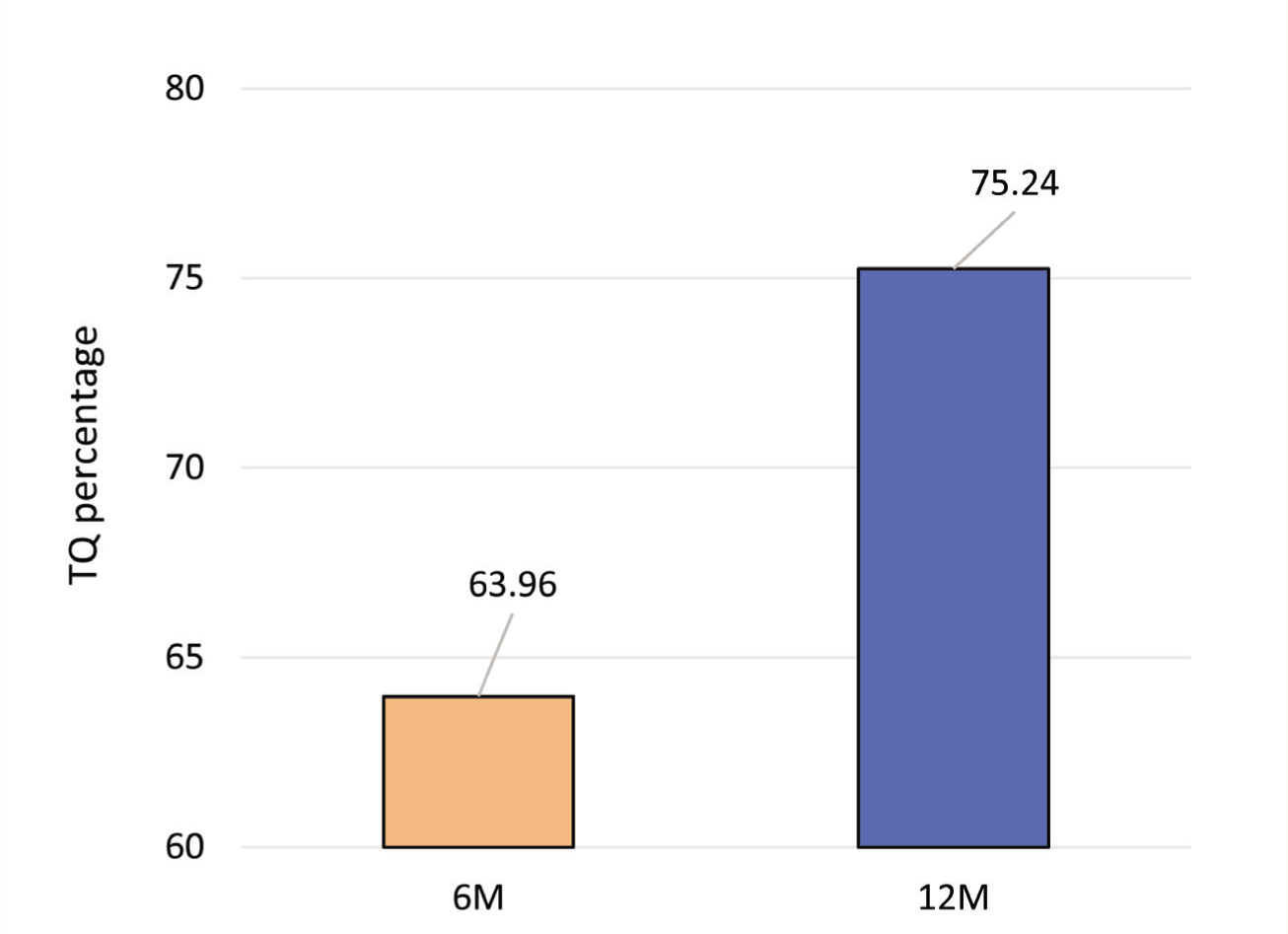
6M, at sixth months; 12M, at 12 months.
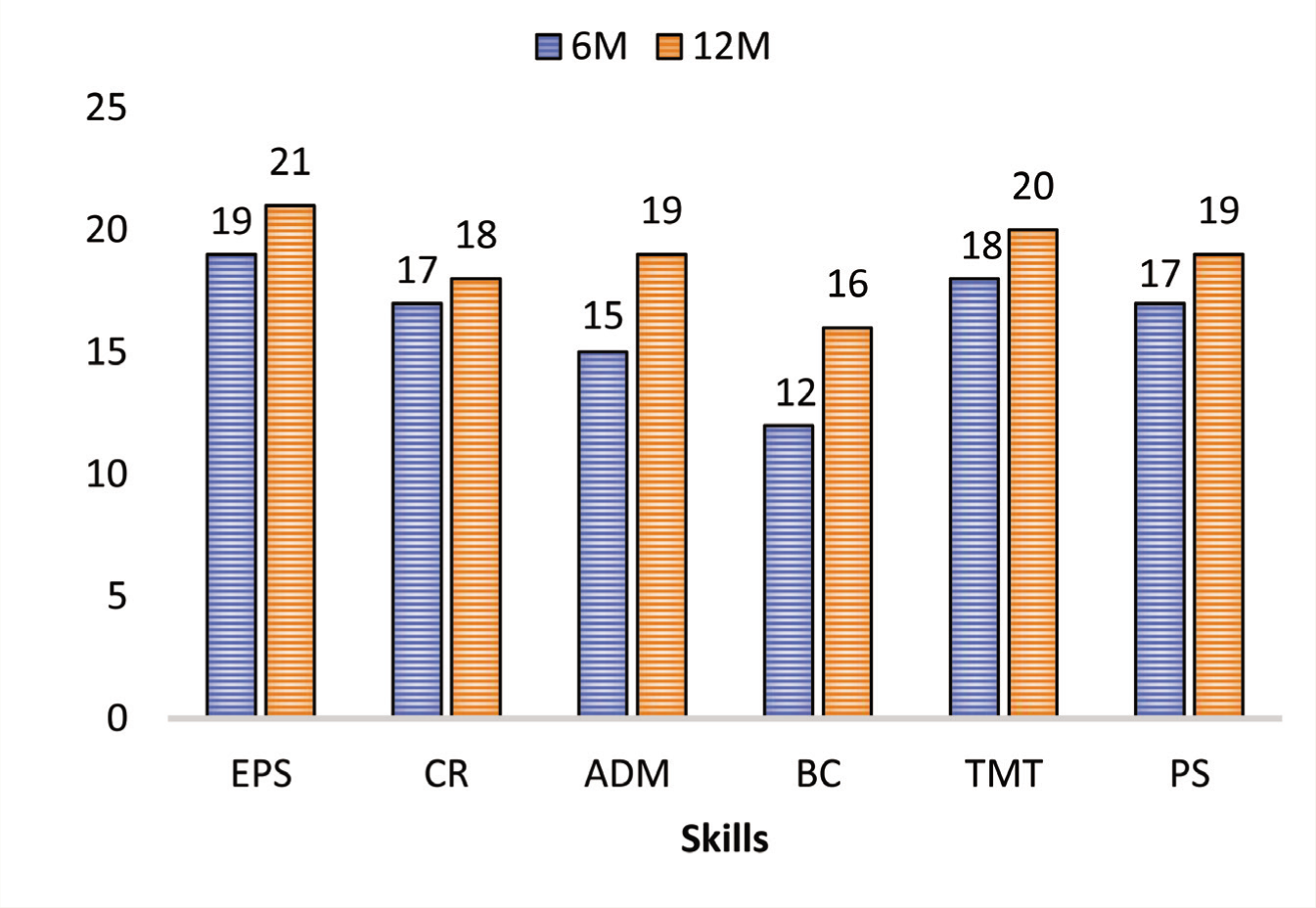
6M, at sixth months; 12M, at 12 months; EPS, elicitation of psychiatric symptoms using the screening questionnaire; CR, clinical reasoning of case-ness for psychiatric diagnosis; ADM, appropriate decision regarding choosing psychiatric medication; BC,- whether they cover components of brief counseling skills; TMT, time management for psychiatric evaluation at the primary level (5–10 min); PS, overall clinical psychiatric skills.
Primary Care Psychiatry Quotient
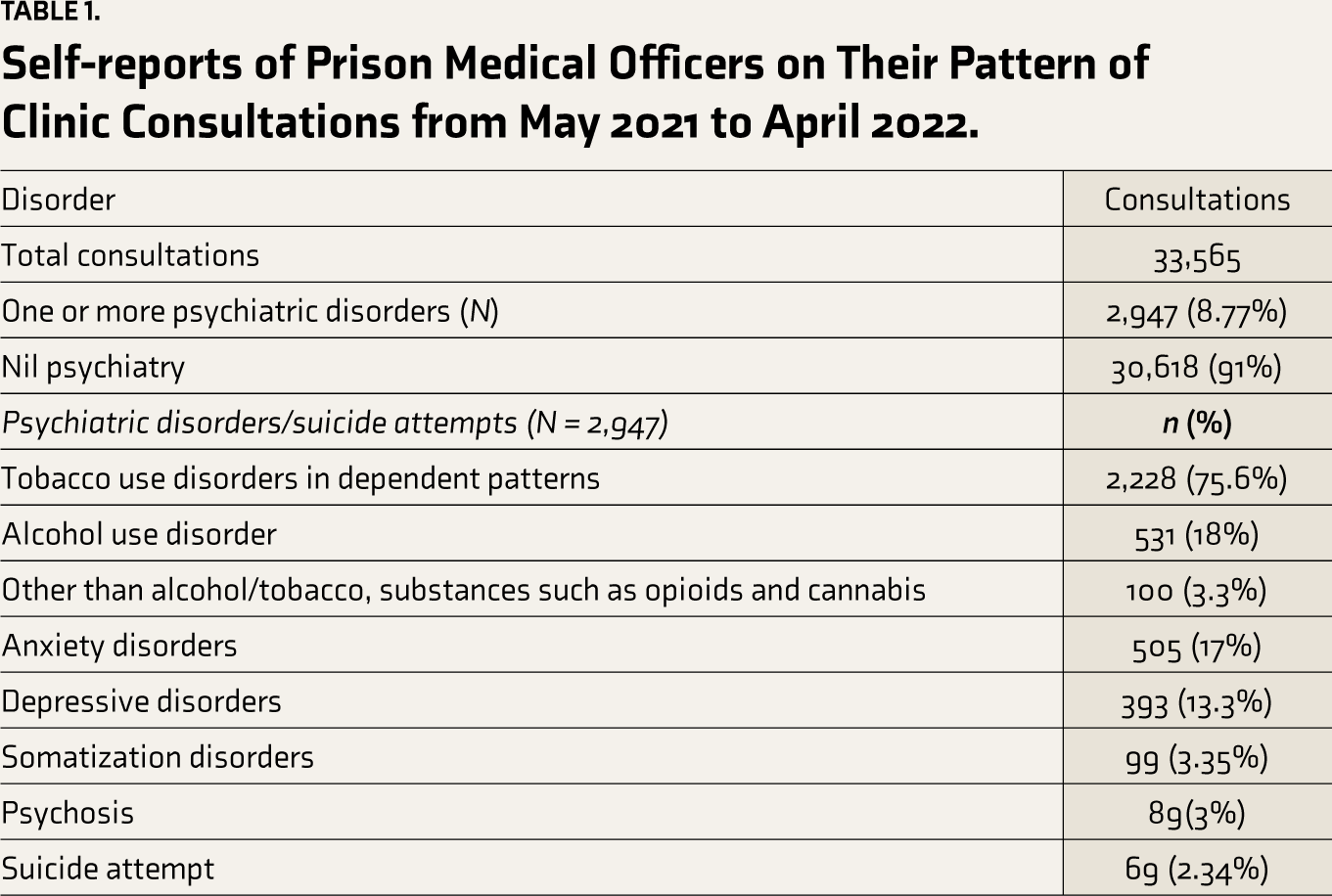
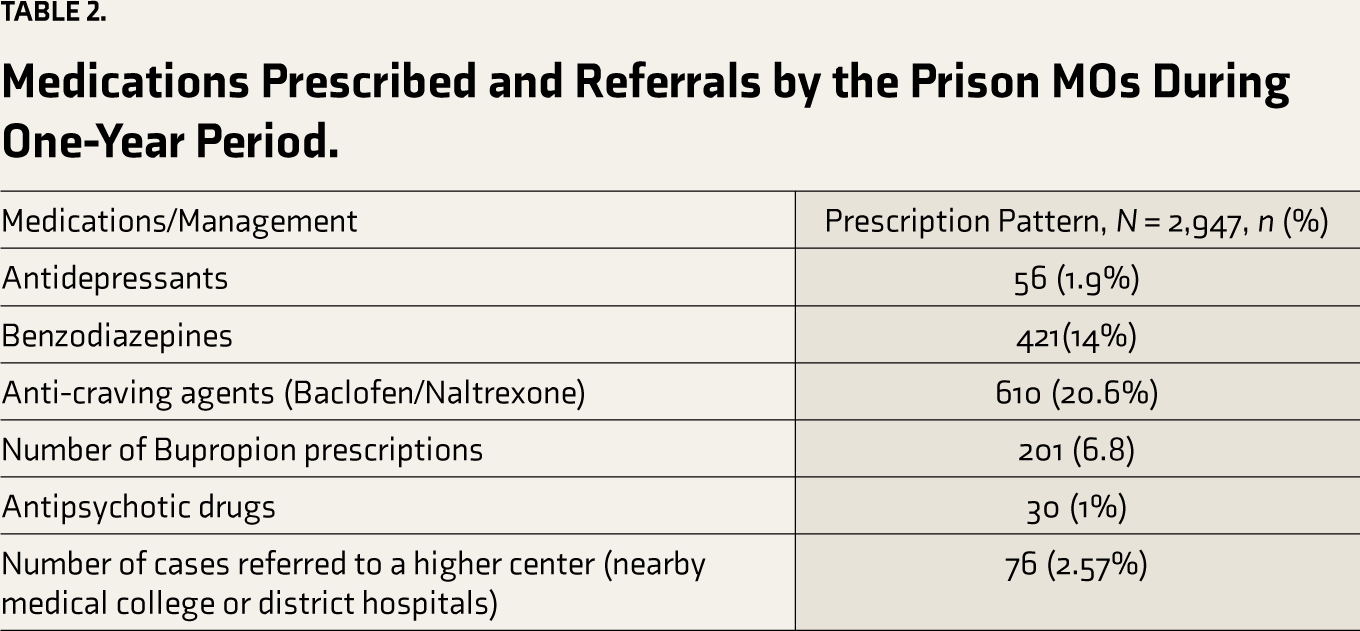
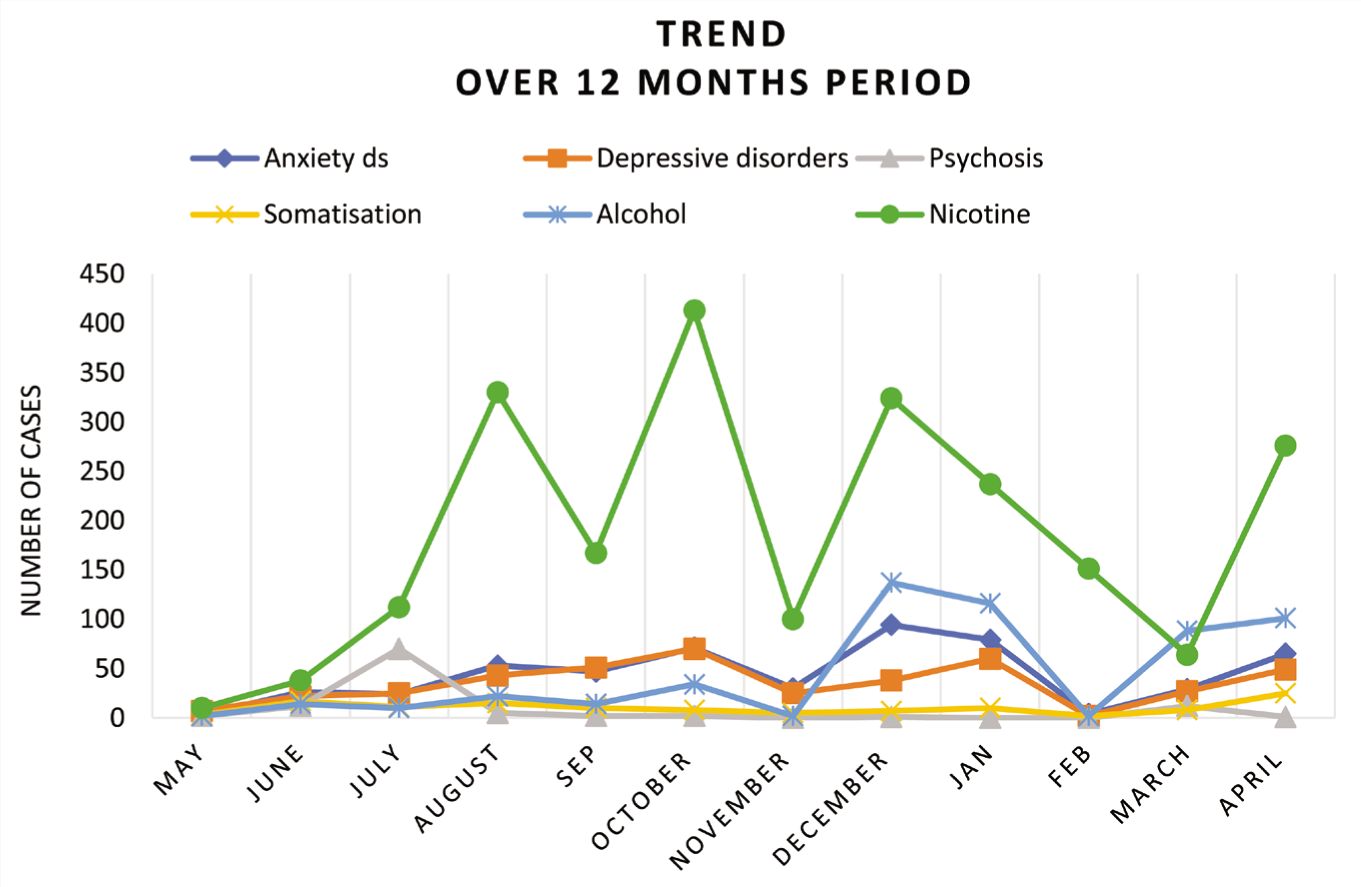
PCPQ was calculated from the monthly patient audits submitted by the prison MOs. Two thousand nine hundred forty-seven inmates with psychiatric disorders were identified and treated out of the total 33,565 medical consultations in the one year of their training. The estimation of one-year PCPQ in this study was 8.77%. Table 1 presents the distribution of various psychiatric disorders observed over one year. The highest proportion was related to tobacco and alcohol use. Anxiety and depressive disorders were the subsequent ones. Table 2 presents a comprehensive overview of the medications the prison MOs prescribed during the said one-year period and the proportion of cases referred to higher centers. All patients diagnosed with MOs were not prescribed medications at the first instance. For the initial couple of weeks, MOs were taught to watch symptoms carefully for two weeks. Patients were offered brief counseling for those with milder symptoms, if required. Only those individuals whose symptoms persisted beyond two weeks were prescribed medications. These principles were followed, as mentioned in the CSP manual. Figure 3 depicts the monthly trends in the reported cases. Table 3 depicts a progressive increase in the number of psychiatric cases identified in each quartile (three months), and the statistical significance of the quartile with consecutive quartiles reflects that the yearlong hand-holding training program remained effective and improved further as the months of training progressed. Figure 4 depicts the disorder-wise case-identification trend throughout the one-year training program.
Self-reports of Prison Medical Officers on Their Pattern of Clinic Consultations from May 2021 to April 2022.
Medications Prescribed and Referrals by the Prison MOs During One-Year Period.
Month-wise Psychiatric Cases Identified from May 2021 to April 2022.

Quartile-wise Comparison of the Number of Inmates Requiring Psychiatric Consultation.
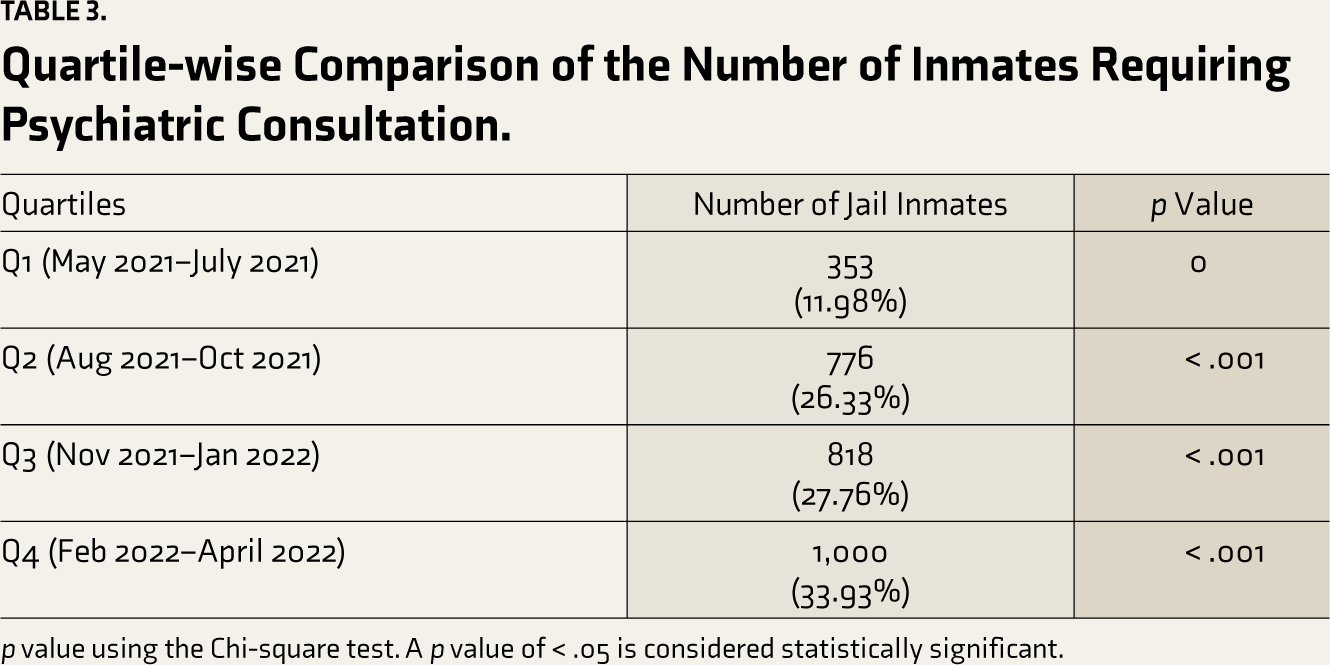
p value using the Chi-square test. A p value of < .05 is considered statistically significant.
Trend of Psychiatric Disorders over a One-year Period, that is, May 2021–April 2022.
Discussion
In this study, the TQ, denoting the degree of knowledge and skill retention, was found to be 64% in the sixth month of training and 75% upon completion. This indicates that two-thirds of the acquired skills were adequately retained in the sixth month and further improved in the subsequent six months. The upward trend in scores suggests enhanced proficiency in terms of screening, improved interpretation of signs and symptoms, accurate diagnoses of prevalent psychiatric disorders, the provision of appropriate first-line treatment, appropriate referral of patients, and collaborative management of prison inmates with mental illness. These results are consistent with the training program implemented for PCDs working in the community (as opposed to prisons) in the state of Uttarakhand, where TQ scores of 70.33% and 76.33% were achieved during the sixth and ninth months of the course. The PCPQ score of 8.7% suggests that 2,947 out of 33,565 consultations with inmates revealed the presence of mental illness. Without psychiatry training, these patients may not have received timely clinical attention, potentially exacerbating symptoms or causing further impairment in functioning. The Uttarakhand training program (2018–2019) included 10 PCDs; PCPQ was 11.09%. The restricted catchment area could be a potential reason for a lower PCPQ in this group. Additionally, only five PCDs could complete the training, as opposed to 10 PCDs in the Uttarakhand training program and 22 PCDs in the District Mental Health Program of Bihar (2020–2021).18,19
Studies done abroad showed a prevalence of any mental disorder (62.7%–92.2%), substance use disorders (5.1%–87%), severe depressive disorders (3.8%–44%), anxiety disorders (5.6%–44.4%), and psychosis (6.2%–56.7%) in the prison population.20–28 Literature from India 8 revealed that the prisoners’ lifetime use of tobacco was 67.3%, their lifetime use of alcohol was 51.5%, their lifetime prevalence of major depressive disorders was 12.7%, and their lifetime prevalence of combined anxiety disorders (including panic disorder, agoraphobia, social phobia, post-traumatic stress disorder, and generalized anxiety disorder) was 5.5%. 8 It may be noted that the denominator used to calculate the above percentages was the entire prison population of 5,200 inmates. Another study of 118 random inmates in Central Jail, Kota, Rajasthan, in 2013 showed 58.8% drug dependence/abuse prior to prison, 16.1% depressive disorder, 8.5% anxiety disorders, and 6.7% psychosis. 29 However, in the current study, we did not assess the entire prison population, and the denominator was only the population with positive psychiatric diagnoses (2,947) that had presented to prison hospitals. Even so, the proportion of substance use disorders was higher: tobacco use disorder (75.6%), followed by alcohol use disorder (18%). Depressive disorders (13.3%) and anxiety disorders (17%) followed. Further, in the present study, the proportion of those with severe mental illnesses requiring specialist care or immediate referral was much lower. Even this pattern mirrors the scenario in the outside community, that is, depression, anxiety, and substance use disorders in the order of prevalence in primary care clinics.30–32 Like in the community, even in prisons, it may be possible for trained MOs to manage most of the mental health concerns instead of having a psychiatrist. This assertion does not negate the ideally desirable scenario of a psychiatrist serving inside prisons. The study demonstrates the feasibility of leveraging digital technology in mentoring and providing long-term support for PCDs in prison. This kind of task-shifting training can be easily scaled up across the prisons in the country to improve mental health care. Further, the anecdotal feedback the trainee MOs received implied that they developed confidence in identifying and handling mental health issues compared to before the training and requested that more such training programs be conducted in the future.
The Mental Healthcare (Rights of Persons with Mental Illness) Rules, 2018, clearly state the need for prompt and proper identification of a person from mental illness among the inmates, and the schedule describes minimum standards for mental healthcare in prisons. The minimum standards as per schedule direct for (a) screening of all inmates during their entry into prison by mandatory physical and mental status examination and urine test for common substances; (b) identification of inmates with serious mental illness and preparing the treatment plan; (c) ensuring availability of minimum psychotropic medications, psychosocial interventions and suitable rehabilitation services; (d) protocols to deal with suicide risk and crises; (e) addressing substance use problems with specific interventions for various drug conditions, and finally, (f) advocating for minimum mental health human resources and in-patient facility requirements. 33
In India, MBBS graduates get very little undergraduate training in psychiatry except for an optional two-week internship with 20 one-hour lectures in the fifth semester. 34 It may also be noted that there is a dearth of psychiatrists even at the community level; in most states of India, there is less than 1 psychiatrist per 100,000 population, whereas the desirable number is 3 or more per 100,000 population. 35 Given all these circumstances, the most viable solution in the short term would be to provide primary care psychiatry training to the existing MOs working in prison and correctional settings with little disruption of their work using digital technology.
Limitations and Future Directions
Only five out of seven MOs who attended the course could complete it. The remaining two MOs could only attend some modules due to their demanding work schedules, other administrative duties, relocation to a different work location, and personal reasons. Intermittent restrictions on the use of mobile phones inside jail premises and poor telephone signals were other challenges. It would be beneficial to employ qualitative methods to get in-depth insights into the challenges, workload, feasibility of implementing, and outcome of such digitally driven training courses. Prospective studies of extended duration and involving a larger number of prison MOs might yield novel insights into mental health issues in correctional facilities and the degree of skill retention in prison MOs. This study proposes a potential alternative training model for prison MOs in primary psychiatry as a means of addressing mental health issues in hard-to-access and challenging places like prisons until a psychiatrist becomes available in resource-limited settings such as India.
Conclusion
This one-year prison and correctional psychiatry course is valuable for practicing MOs to enhance their knowledge and skills to strengthen primary mental health care in prison settings.
Footnotes
Acknowledgements
Th authors would like to acknowledge the following persons:
Prison Health Service, Home (Prison) department, Government of Bihar, India. Dr. Deepa Rani, Director of Health, Home department and Dr. Prashant Sinha, Deputy Director of Health, Home Department, Government of Bihar, India Dr. Preeti Bajpai, Consultant Mental Health, State Health Society, Government of Bihar, India Dr. Sunil Kumar, Special Program Officer, State Health Society, Government of Bihar National Health Mission, State Health Society, Bihar. Trainee medical doctors for working in prison and correctional settings for participating in study. The assistance of staff from the Tele Medicine Centre, NIMHANS, Bengaluru.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Received the Institute Ethics Committee approval (No. NIMHANS/EC( BEH.SC.DIV) MEETING/2023, 18.08.2023, NIMHANS, Bengaluru.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The anonymized monthly reports are analyzed and the researchers had no interaction with prison inmates presenting to prison clinics.